
Abstract
Introduction:
Eating fish before and during pregnancy is important but care must be taken to choose fish which maximize developmental outcomes. Physicians, a trusted health information source, could provide this nuanced communication. This cross-sectional survey of a representative sample of 400 family medicine and obstetrics and gynecology (OB-GYN) physicians in Minnesota was designed to understand physician behaviors and beliefs about safe fish consumption, describe barriers to physician-patient conversations about safe fish consumption generally and as part of prenatal care and to identify resources to help facilitate conversations on this topic.
Methods:
Data was collected January to April 2020. Two hundred nineteen surveys were completed (55% response rate) with 194 reporting seeing patients at least 1 day a week. Descriptive survey results from all were summarized and analyzed overall and by physician specialty. Responses to 3 open-ended questions were thematically coded to enrich the quantitative results.
Results:
While 62% of these reported discussing nutrition topics, only about one-third reported discussing with patients the benefits and about one-quarter the risks of eating fish. Despite the relative infrequency of fish discussions, almost all (>90%) respondents agreed that it is important to discuss fish consumption with people who are or may become pregnant. The largest reported barrier to these conversations was time (82%), and the most endorsed resource to overcome identified barriers was talking points (72%).
Conclusions:
Because physicians report limited time, resources that facilitate fish consumption should be succinct while serving to both nudge the message and direct clinicians and their patients to robust information.
Introduction
Nutrition for pregnancy is important among reproductive age people and medical professionals. 1 Eating foods consistent with the Mediterranean diet, including fish, is associated with reduced risk of pregnancy complications such as gestational diabetes mellitus. 2 Fish is a uniquely good source of fatty acids required for brain and retinal development and is recommended by the American College of Obstetricians and Gynecologists and the Academy of Nutrition and Dietetics. 3 As such, it is recommended women consume 8 to 12 oz of fish per week. However, due to the sensitivity of the developing fetus to mercury, people who are or may become pregnant should consume lower-mercury fish such as cod, salmon, herring, or tilapia.4,5
Generally patients want to engage in nutritional discussions with physicians. 6 While evidence indicates that physicians can positively influence patients’ diets,7,8 barriers to nutrition conversations include lack of time and lack of training on nutritional topics.9,10 Despite potential patient receptivity to advice before and during pregnancy, barriers exist. Providers perceive “a low level of (their own) engagement with pregnancy nutrition issues, in particular fish consumption.” 11 One convenience sample survey of physicians found that while physicians report understanding fish consumption benefits and risks for pregnant patients, they lacked a strong positive attitude and accurate knowledge about the topic. 12
A representative survey was designed to understand (1) physician behaviors and beliefs related to safe fish consumption conversations, (2) barriers to physician-patient conversations about safe fish consumption, and (3) resources to facilitate conversations. Responses were compared by physician specialty, average days per week working in clinic, years in practice, or region of practice. So as not to impact physician selection into the survey based on topic salience, the survey was framed as one about physician-patient nutrition conversations. Results will inform the development of resources to assist physicians in promoting safe fish consumption among persons who are or could become pregnant across Minnesota and beyond.
Methods
Population and Survey Methods
This cross-sectional representative survey used a listed frame of Minnesota physicians available from the state licensing board. Two hundred family medicine and 200 OB-GYN physicians were randomly sampled. With an a priori estimated response rate of 50%, this sample size was selected to produce estimates by specialty with a 10% margin of error. Physicians were emailed an invitation describing the survey with an opportunity to opt-out and a personalized survey URL. Emails included logos from Minnesota Department of Health, the host health system and the Minnesota section of the American College of Obstetricians and Gynecologists [MN ACOG] or the Minnesota Academy of Family Physicians [MAFP] and were signed by leaders representing the health system and the professional organization. Up to 2 reminder emails were sent to non-responders. Physicians without an email address or who did not respond were mailed a paper survey and a cover letter with the same logos. A coffee shop gift card was sent with the mailing or as an incentive after web survey completion. Surveys were fielded January to April 2020.
This was reviewed by the HealthPartners institutional review board (IRB) and deemed non-human subjects research (11/26/2018) due to its primary use toward project-specific improvement related to the ChooseYourFish initiative (HealthPartners Institute, 2022). Due to this waiver of approval, informed consent was not required so survey completion implied consent.
Questionnaire Design
Behaviors, beliefs, barriers and facilitators aligned with the COM-B model were used to guide survey construct development. 13 As no validated instruments exist for the specific constructs of interest, the questionnaire was developed using best practices for question writing, where possible adapting questions with known psychometric properties. 14 Before fielding, the survey was reviewed for face validity by content experts, survey methodologists, and OB-GYN and Family Medicine physicians from the focus population. Unclear or confusing items were iteratively revised by survey methodologists until consensus was reached. The survey, designed to take 8 min to complete, asked 18 questions nested under the 3 study aims.
Analysis
Descriptive results were summarized for differences by physician specialty. Except for population descriptions, results are reported only for physicians who see patients at least 1 day a week. Missing data, where present, are noted and removed from the denominator of calculations. Differences by days per week seeing patients, years in practice, and geographic region were tested using Pearson’s chi-square or Fisher’s exact test when there were small values. Associations were considered statistically significant if P < .05. Analyses were performed using SAS (version 9.4, Cary, NC).
Open-ended responses were coded to enrich quantitative results. A single analyst (JD) coded responses using an inductive content analysis approach. The coder first read all responses for a given item to understand the gestalt and scope of responses. Then, each response was re-read and analyzed into emergent codes. A second coder reviewed the coding for accuracy and suggested additional codes. Coders met to adjudicate the final coding schema. Representative quotes were selected and lightly edited to deepen understanding and provide respondent voice. 15
Results
Respondent Characteristics
Two hundred nineteen physicians responded, for a 55% response rate (AAPOR response rate 6). 16 There were no differences in response rates by specialty or region (data not shown). Respondents included 52% from family medicine and 48% from OB-GYN. Most were from the Twin Cities metropolitan area, worked at least 4 days a week in clinic, and had over 15 years in practice. Behaviors and beliefs, barriers, and desired resources are reported below for the 194 physicians who see patients in clinic at least 1 day a week. Over two-thirds reported seeing pregnant patients. See Table 1.
Demographic and Practice Information for Survey Respondents.

N = 219. Missing values vary by question; the most excluded for any given question is 2% due to intentional branching.
Behaviors and Beliefs
Most physicians (62%) report that nutrition is typically discussed in office visits (Table 2). When asked from whom patients should ideally receive nutrition information, 91% indicated “definitely” dietitians and 65% indicated “definitely” doctors. Information made available from the clinic, health plan, and nurses was also endorsed. Of the physicians and care teams who discuss nutrition some or all of the time, weight management and balanced diet are the most prevalent nutrition-related topics covered in non-emergent appointments, discussed by over 80% of respondents. This compares to about one-third reporting discussing benefits of fish and slightly fewer discussing related risks. This behavior differs by physician type, with more OB-GYN than family practice physicians talking about fish risks (43% vs 14%, P < .0001). Of physicians who discuss fish, most report that they have the conversation rather than a nurse or someone else; this behavior is more common among family medicine than OB-GYN physicians (93% vs 73%, P = .014). Most agreed it is somewhat or very important to discuss fish with both pregnant patients and those who may become pregnant. Of specific fish topics, “mercury” was discussed most of the time by 23% of physicians, followed by “which types of fish to eat,” “how much fish to eat,” and “limiting fish consumption” being discussed most of the time by less than one-fourth of physicians. These frequencies differ by physician type, with more OB-GYNs discussing each topic most of the time (Figure 1). Most physicians (72%) strongly agree that some fish should be avoided by pregnant people. However, only one-third strongly agree that it is important for pregnant individuals to consume fish, a belief endorsed more strongly by OB-GYNs (44% vs 14%, P = .0006).
Select Physician Survey Questions and Responses Related to Fish Consumption Conversations and Resources.
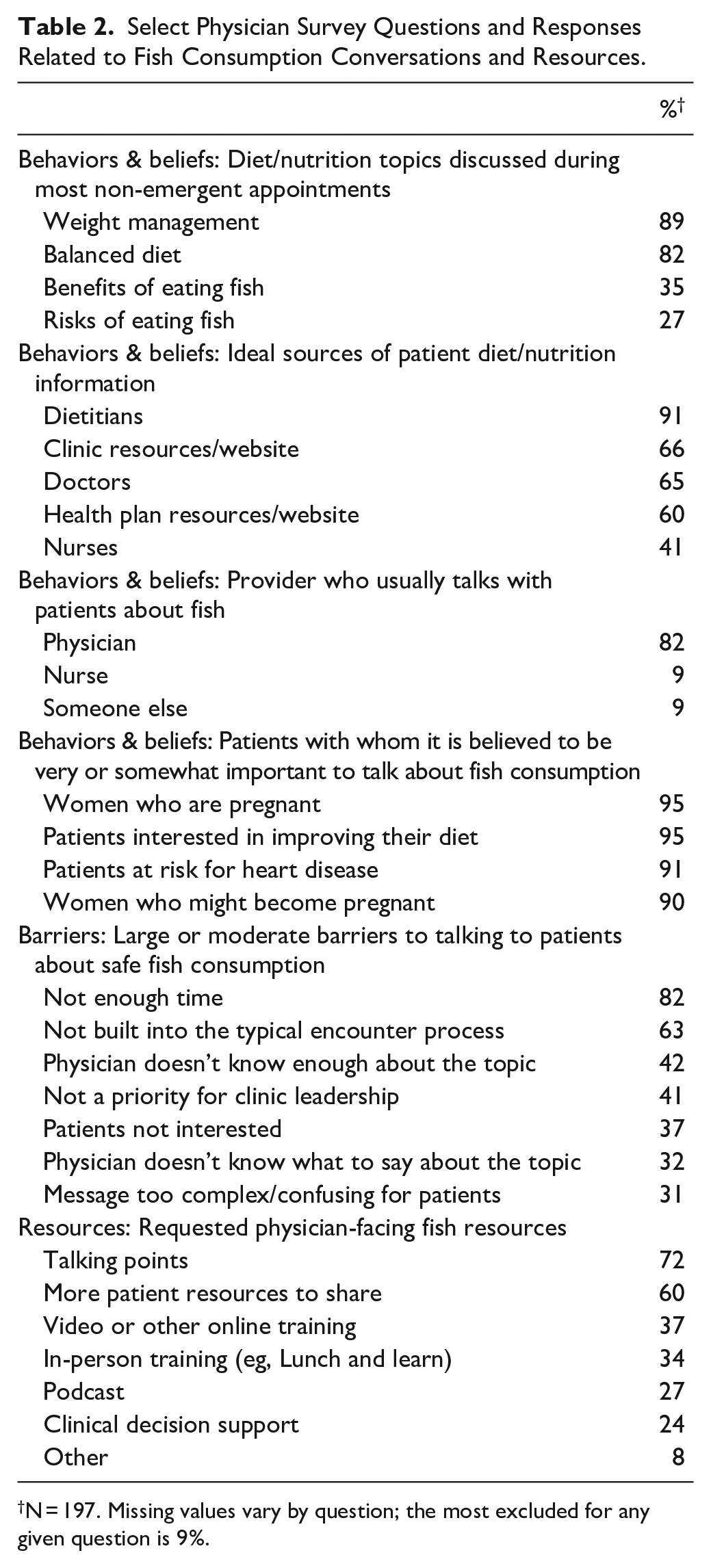
N = 197. Missing values vary by question; the most excluded for any given question is 9%.

Percent of providers talking about fish topics some or most of the time.
Perceived Barriers
Physicians reported barriers to engaging with patients about safe fish consumption, with lack of time reported most frequently (Table 2). Open-ended comments reiterated the barriers of time and other competing topic priorities:
“Almost every day I spend in clinic is rushed because of demands to see patients and general tasks. Topics like nutrition and fish consumption are rarely discussed unless they are directly connected to the problem being evaluated.”
Another identified barrier was that the topic is not seen as a priority for clinic leadership:
“It’s not prioritized by my employer, perhaps because it is not related to compensation from insurance companies.”
Patient-related factors were reported less frequently with some physicians reporting that their patients are not interested in the fish topic or that it is too complex and confusing for patients.
One additional barrier volunteered by physicians was that the topic was not a part of their practice or professional role:
“It is a personal choice, not part of acute problem consultation.”
Desired Resources
Most endorsed talking points as a resource to aid in fish conversations with patients, followed by additional patient resources. Fewer endorsed trainings, but both online and in-person trainings were favored by family medicine over OB-GYN physicians (online 44% vs 29%, P = .029; in-person 45% vs 21%, P = .0005). A few suggested standardized electronic medical record (EMR) phrases could help deliver messages:
“I created a “dot phrase” in Epic EMR that summarizes the Monterey Aquarium guidelines for mercury and overfishing various fish species - that I use daily.”
Results were largely consistent across other physician characteristics. One difference in item response was observed based on the number of days per week a physician is in clinic; those in the office fewer days were less likely to know about quality assurance programs in place (P = .042). There were few differences by years in practice: physicians with 11 to 20 years of practice were more likely to want more patient resources to share (P = .008) and those with 21+ years were less likely to endorse time as a barrier (P = .016) and less likely to talk about limiting fish consumption (P = .049). Finally, physicians in the metro area were more likely to discuss the benefits of fish (P = .024; data not shown).
Discussion
ACOG encourages pregnant women, women who may become pregnant, and breastfeeding mothers to follow the FDA and EPA’s revised advice to eat 2 to 3 servings a week (8 -12 oz in total) of a variety of fish 17 and the American Academy of Family Physicians recommends that women who are pregnant, nursing, or contemplating pregnancy should limit their consumption of albacore tuna to 6 oz per week but should consume at least 12 oz of other fish weekly for adequate benefits. 18 Consistent with these recommendations, most Minnesota OB-GYN and family medicine physicians who responded to our survey say they believe it is important to talk about fish consumption with patients who are or may become pregnant.
However, not all physicians report talking about this topic most or even some of the time. Top barriers to giving advice to patients are lack of time and belief that it is not priority for leadership, 2 factors that should be considered in parallel. It should not be surprising that physicians report that lack of time is the biggest barrier to providing nutrition advice. 19
Physicians asked for talking points and patient-facing resources, which aligns with literature that emphasizes brevity. 12 Given the constraint of time, talking points that nudge pregnant people toward existing resources may hold more promise than those that signal a lengthy conversation. One strategy would be to integrate the information into the clinical encounter through an EMR smartphrase, as called for by a few respondents.
While lack of knowledge was not frequently reported in our survey, whereas it has been in others,12,20,21 differences by specialty suggest family practice physicians are less likely to discuss fish consumption, possibly due to lack of topic knowledge or comfort. While the differences between specialties could be due to fewer physicians in family medicine seeing the primary focus population, this cannot be accounted for with our data. However, OB-GYNs have the advantage of milestone events (ie, pregnancies) that trigger the conversation.
Our findings must be considered in light of important limitations. We conducted the survey before the onset of COVID-19, and we did not validate the psychometric properties of the survey beyond face validity. Surveys are subject to social desirability bias and other forms of measurement error in which context these results should be considered. The survey was conducted in multiple modes, so there could have been differences in measurement or selection. However, these concerns are assuaged by similar response patterns across modes. There were 2 marginally significant differences by mode and one significant difference (mail responders more likely than email responders to have clinics with quality assurance processes in place to make sure diet and nutrition messages are being delivered). While the 55% response rate is relatively high, in any survey nonresponse bias is a potential limitation. Here this concern is mitigated in that we had no observable differences in survey responder and non-responder characteristics. 22
This work was not designed to generalize to other states; however, lessons may extend to other Great Lakes areas where similar risks and benefits exist. Future work will use these findings to create concise talking points for physicians and integrate patient messages into the EMR.
Conclusions
While OB-GYNs and family physicians report that recommending fish to their patients is important and within scope of their practice (objective 1), they also report that lack of time is a barrier (objective 2). They also report that they would appreciate talking points to facilitate their advice (objective 3). These findings suggest that resources for physicians should be succinct with the goal of nudging patients and clinicians to access more definitive information.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319221126980 – Supplemental material for Behaviors, Beliefs, and Recommendations to Optimize Promotion of Safe Fish Consumption Before and During Pregnancy: A Physician Survey
Supplemental material, sj-docx-1-jpc-10.1177_21501319221126980 for Behaviors, Beliefs, and Recommendations to Optimize Promotion of Safe Fish Consumption Before and During Pregnancy: A Physician Survey by Jeanette Y. Ziegenfuss, Jennifer M. Dinh, Patricia McCann, Abigail S. Katz, Meghan M. JaKa, Jacob Haapala, Cresta Jones, Abbey Mello, Jeremy Springer and Thomas E. Kottke in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
We thank Casey Easterday and Erik Peterson for their assistance coordinating survey administration. We also thank our respondents for taking the time to complete the survey.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding from the Environmental Protection Agency’s Great Lakes Restoration Initiative (GL00E01161) awarded to the Minnesota Department of Health was used for this work.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.