
Abstract
Wastewater monitoring is a useful tool to complement case-based surveillance. A hepatitis A virus (HAV) investigation in North Carolina demonstrated that wastewater monitoring detections preceded identification of 2 clinical cases by 12 days. State and local health officials used a preestablished decision tree to respond to wastewater detections of HAV and implement public health actions. The investigation determined that HAV detected in wastewater was likely from 2 people who had not yet developed symptoms or sought testing at the time of detection, providing early information for public health response, including vaccination of family members. Targeted outreach to hospitals as well as medically or socially vulnerable groups at high risk of HAV infection could be recommended in response to consistent HAV detections in wastewater.
Wastewater monitoring was initiated in North Carolina during the COVID-19 pandemic as a complementary public health tool for community disease surveillance.1,2 Wastewater monitoring programs are expanding to include pathogens beyond COVID-19, such as polio and respiratory syncytial virus.3,4 Wastewater monitoring can inform public health action across multiple pathogens, but public health uses vary widely because of differences in laboratory sensitivity, viral shedding patterns, and disease incidence and prevalence. 5 For example, New York used wastewater monitoring in response to identification of a polio case to track possible spread and guide vaccination outreach in 5 counties. 3 Polio had previously been eradicated from the United States, so immediate public health action was needed, which prompted the expansion of immunization efforts. In Wisconsin, public health officials tested for influenza and respiratory syncytial virus and found that wastewater provided an early warning and longer duration of viral signal than emergency department (ED) visits did, demonstrating wastewater’s complementary utility. 4 Incidence, along with disease virulence, pathogenicity, and transmissibility, must be assessed to determine the appropriate public health action in response to wastewater detections. Because hepatitis A virus (HAV) is shed in feces, potential has been shown for improving public health surveillance and response using wastewater.
HAV has been detected in wastewater by the Wastewater SCAN project, where wastewater is tested across the country for multiple pathogens and results are made publicly available to inform public health decision-making.2,5 Hepatitis A is a highly contagious, vaccine-preventable liver infection that can cause mild to severe disease. 6 People infected with HAV often go undetected and can transmit infection if asymptomatic as well as during the presymptomatic infectious period, 2 weeks prior to symptom onset. 6 Wastewater monitoring could be used to detect viral particles during asymptomatic or presymptomatic periods. Beginning in March 2024, the North Carolina Department of Health and Human Services (NCDHHS) followed a preestablished public health action decision tree to respond to a series of HAV detections at a wastewater site measured by WastewaterSCAN (Figure 1).
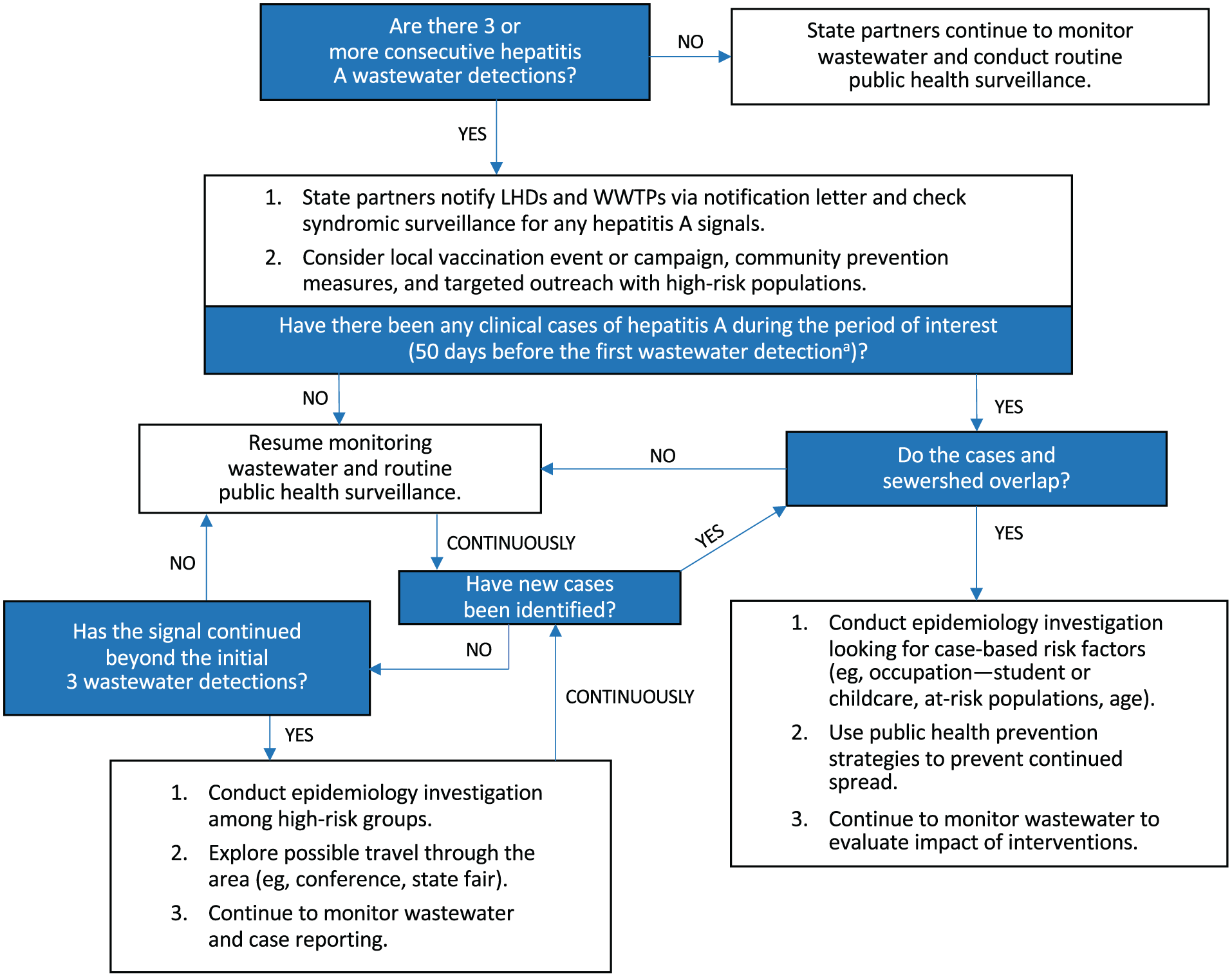
Public health action decision tree for integrating wastewater-monitoring results with other public health data sources for detection of hepatitis A virus, North Carolina Wastewater Monitoring Network. Abbreviations: LHD, local health department; WWTP, wastewater treatment plant.
Methods
Three wastewater sites in North Carolina participate in the WastewaterSCAN/SCAN project, a partnership among Stanford University, Emory University, and Verily funded philanthropically through a gift to Stanford University. 7 NCDHHS routinely monitors the public dashboard and subsequently created public health action decision trees for multiple pathogen targets measured by WastewaterSCAN in the event that state and local public health officials needed to respond to a wastewater detection. Infectious disease experts and wastewater program staff at NCDHHS collaborated to design a decision-making tree to inform a public health response for HAV. This process integrated wastewater detections with other surveillance data sources, including the Council of State and Territorial Epidemiologists (CSTE) case definition. 8 The sample collection date is usually 3 to 6 days before a detection is reported on the public-facing dashboard, so there may be a lag in public health action. A single detection was considered either a false positive or someone traveling through the sewershed, whereas 3 consistent detections were considered evidence of at least 1 case patient actively shedding HAV in the sewershed. NCDHHS used a decision-making tree to guide public health recommendations after observing 2 series of HAV wastewater detections via WastewaterSCAN (Figure 1). NCDHHS determined this study was exempt because it used publicly available data without personal identifiers.
Results
In spring 2024, NCDHHS observed 2 separate series of wastewater detections. Series 1 had 6 consecutive detections from March 18 through April 1, and series 2 had 7 consecutive detections from April 15 through April 29 (Figure 2). Both series of wastewater detections triggered state public health officials to follow a preestablished public health action decision tree for hepatitis A (Figure 1).
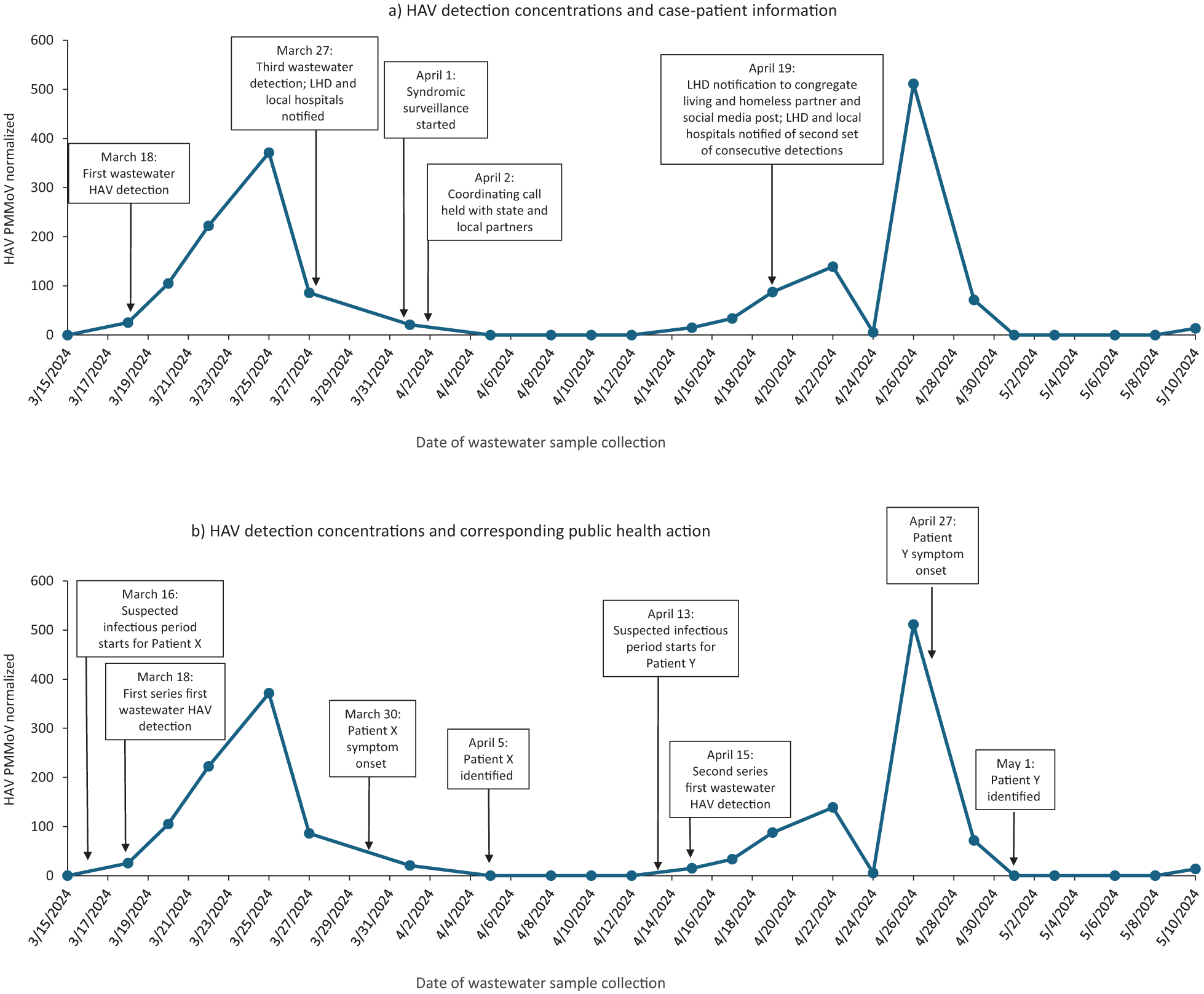
Timeline of hepatitis A virus (HAV) wastewater concentrations, public health actions, and case patient information, Forsyth County, North Carolina, 2024. Concentration is normalized by the Pepper Mild mottle virus, a control virus that helps validate the sample. Abbreviation: LHD, local health department.
On March 27, after the third consecutive hepatitis A wastewater detection in series 1, the local health department (LHD) issued an email blast to health care providers, emergency services, and surveillance partners to monitor for potential hepatitis A cases.
On April 2, after the fourth consecutive detection, state and local partners held a coordinating call to discuss notifying the public of potential disease risk and to assess the need to implement community vaccination efforts per the public health action decision tree. On April 5, the LHD was notified of acute hepatitis A in a pediatric patient, hospitalized with symptoms consistent with the CSTE case definition. The initial wastewater detection was on March 18, 12 days before symptom onset and 18 days before case identification (Figure 2). From March 18 through April 1, 6 consecutive wastewater detections occurred, with a peak concentration 5 days before symptom onset. Routine case investigation was conducted with the case patient, including vaccination of family members on April 17.
On April 15, after 4 nondetections, series 2 began at the same site. Again, after 3 consecutive detections, the LHD and wastewater treatment plant were notified, following the public health action decision tree. The LHD sent an email notification to congregate living facilities, long-term care facilities, and homeless shelters with information about wastewater detections, signs and symptoms of hepatitis A infection, and recommendations for immunization and precautions for individuals at high risk of HAV infection (Figure 2). In addition, a social media release appeared on the LHD Facebook page that included hepatitis A educational information and an infographic.
On May 1, the LHD was notified of a second acute hepatitis A case in another pediatric patient presenting with symptoms consistent with the CSTE case definition. The initial wastewater detection was 12 days before symptom onset and 16 days before case identification (Figure 2). From April 15 through April 29, 7 consecutive wastewater detections aligned with the case patient’s presentation, with a peak concentration 1 day before symptom onset. This patient was the sibling of the first case patient.
Discussion
This response outlines the potential public health utility of HAV wastewater monitoring for state and local public health officials. We recommend several considerations for programs considering similar application of wastewater monitoring.
First, when implementing a new pathogen in wastewater, it is helpful to plan what potential actions could be considered in response to detections. The preestablished public health decision-making tree for HAV provided a framework for public health action based on wastewater monitoring results. A coordinated communication strategy among the LHD, wastewater treatment plant, and state public health officials is recommended to ensure clear messaging to health care professionals and the general public. Wastewater treatment plant staff work closely with the communities they serve and may receive questions about wastewater monitoring results and safety, especially if results are available on a public dashboard.
Second, it was not known initially if the concentrations detected in wastewater were attributable to only 1 or multiple hepatitis A cases. When the wastewater detections began, the case patients were presymptomatic, so it is unclear what additional public health actions could be taken beyond early notifications to health care providers as outlined in the decision tree. Although the identified cases were not in settings or among populations at high risk of HAV infection, wastewater detection before symptom onset or medical care highlights the potential for earlier identification among groups at elevated risk of HAV infection, such as people who use injection drugs, people experiencing homelessness, people seeking refuge, and occupational exposures such as food handlers.6,9,10 Given that the second series of detections began shortly after the initial case patient was identified, further transmission of HAV can be tracked using wastewater monitoring. The timeline of wastewater detections and clinical identification provides evidence that tracking clusters and outbreaks of HAV infection via wastewater is possible and could provide context as to whether public health action is warranted. We recommend using community partnerships to provide communication and education.
In this situation, we were able to detect both hepatitis A case patients in wastewater 12 days before symptom onset, based on when the case patients sought medical care. This context provides the potential for early action if transmission was occurring presymptomatically among populations at increased risk of HAV infection. For both case patients, wastewater detections provided an early notification 16 and 18 days, respectively, before standard case-based surveillance identified the case patients. Remarkably, the first wastewater detection aligned with the start of the infectious period and wastewater concentrations peaked at 5 days and 1 day, respectively, before symptom onset. Both case patients were children, which could have contributed to high wastewater concentrations and prolonged gastrointestinal shedding. Most children aged <6 years (70%) present asymptomatically with hepatitis A infection, which could lead to wastewater detection without case identification. 6 Severity of illness and duration of symptoms can affect viral shedding time and viral load, which may result in more consecutive or higher concentration detections. 11 In the event of a similar series of hepatitis A detections in wastewater, we would consider the concentrations relative to this initial use case as added context to the decision tree.
Hepatitis A is effectively preventable with vaccines. It may be beneficial to consider community vaccination rates as well as where un- and undervaccinated populations may reside within a sewershed. Vaccination is also an important public health action for pathogens such as polio or measles, given the transmissibility and rarity of those viruses in the United States.
Conclusion
This investigation provided evidence of how the integration of wastewater monitoring into an overall response strategy can complement traditional public health surveillance and provide a comprehensive approach for HAV surveillance. The use of the described public health decision-making tree provides a method to incorporate wastewater detection with other clinical data sources that public health practitioners can use as a resource. This example provides a unique use case of this decision-making tree being used in real time to inform public health HAV response. As wastewater programs expand to additional pathogens, it is important for state and local public health officials to discuss and proactively decide what public health actions could be implemented in the event of a single detection or series of detections for a given pathogen.
Footnotes
Acknowledgements
The authors acknowledge Alexandra Boehm, PhD, with Stanford University and WastewaterSCAN; Bill Brewer, BS, with the Winston Salem Wastewater Treatment Plant; and the North Carolina Division of Public Health staff who provided critical assistance and consultation during this response.
Editors’ Note
Ariel Christensen and Ty Lautenschlager were co–first authors.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the Centers for Disease Control and Prevention’s Epidemiology and Laboratory Capacity Cooperative Agreement and the National Wastewater Surveillance System.