
Abstract
Objectives:
Despite recent decreases in overdose deaths in the United States, an opportunity remains to connect with people who have had a nonfatal overdose. We analyzed data collected from the Maricopa County Department of Public Health (MCDPH) nonfatal opioid overdose case investigations program, highlighted findings from investigations conducted during the first 2 years of the program (September 1, 2021–August 31, 2023), and compared findings across the 2 years.
Materials and Methods:
We reviewed data collected through the MCDPH nonfatal opioid overdose case investigations program, wherein MCDPH staff members conduct telephone interviews with a sample of case patients with a recent nonfatal opioid overdose. During interviews, MCDPH staff asked questions about overdose event circumstances, knowledge and practice of harm reduction strategies, substances used, and interest in treatment. MCDPH staff offered harm reduction kits to all case patients and transferred case patients interested in treatment to the Arizona Opioid Assistance and Referral Line.
Results:
MCDPH interviewed 529 of 2029 case patients (29.5%) who met sampling criteria. Among 354 case patients who self-reported recreational drug use, the number of cases reporting recreational fentanyl use increased from 117 of 179 (62.6%) in year 1 to 129 of 175 (73.7%) in year 2. Of 352 case patients, 187 (53.1%) reported access to naloxone. Smoking (208 of 295 case patients; 70.5%) was the most commonly reported route of consumption.
Practice Implications:
MCDPH’s novel nonfatal opioid overdose surveillance program identified trends in drug use and harm reduction among people who use drugs who are at the highest risk of a subsequent overdose. The program continues to operate, and survey questions are routinely evaluated to ensure data collected inform overdose prevention strategies.
Opioid overdose deaths in Maricopa County, Arizona, reached a record death rate of 28.8 deaths per 100 000 population in 2021. 1 In 2017, Arizona issued a statute requiring all health professionals to report suspected opioid overdoses to the local public health department. 2 Seeing the mandated reporting as an opportunity to collect risk factor information not typically available in other public health data sources used for overdose surveillance, in March 2021, the Maricopa County Department of Public Health (MCDPH) launched a novel program to investigate nonfatal opioid overdose cases, mirroring the public health response for most other mandated disease reports. Although case investigations of nonfatal opioid overdoses began in March 2021, the first several months were considered a pilot period, wherein processes and survey questions were tested and improvements were made. By September 2021, the program was fully operational and standardized.
In this article, we aimed to (1) describe the methodology of a nonfatal opioid overdose surveillance program, (2) highlight findings from nonfatal opioid overdose case investigations conducted among Maricopa County residents during the first 2 years of the program, and (3) compare findings of the case investigations program from year 1 (September 1, 2021–August 31, 2022) with findings from year 2 (September 1, 2022–August 31, 2023) to guide prevention strategies.
Materials and Methods
Arizona medical facilities are required by Arizona Administrative Code R9-4 Article 6 to report suspected opioid overdoses to the health department through the statewide Medical Electronic Disease Surveillance Intelligence System (MEDSIS), which is the same system used for communicable disease reporting. 2 Per Arizona Administrative Code R9-1, MCDPH services include assisting individuals and populations to improve health and prevent disease by performing epidemiologic investigations, providing health education, and evaluating the effects of activities and services provided by the local health department. 3 MCDPH established this surveillance initiative as part of its public health services, where a team of epidemiology investigators (1) collects data that help MCDPH better understand the circumstances of overdoses locally to inform and support local opioid overdose prevention programs and (2) promotes mitigating health risks associated with drug use and high-risk behaviors based on scientific evidence. 4 With a limited team capacity to investigate all reported cases, MCDPH samples a subset of reported cases to conduct telephone interviews. This project aligns with Arizona Revised Statutes and Administrative Code for local health department services and was executed as an approved surveillance activity for the Overdose Data to Action Grant; therefore, an institutional review board assessment was not pursued for this public health practice activity.2-4
For sampling of case patients, MCDPH uses the following inclusion criteria: (1) case patients seen at 2 of the major hospital systems that have facilities across Maricopa County, (2) case patients aged ≥18 years, and (3) case patients with confirmed or probable nonfatal opioid overdose. 5 MCDPH excludes (1) cases with fatal outcomes and (2) intentional overdose cases, unless documentation showed prior substance use. Investigators abstract information on overdose circumstances from hospital medical records for all cases, including case patients lost to follow-up (defined as 3 unsuccessful contact attempts).
MCDPH staff members conduct interviews by telephone and use a standard electronic questionnaire. MCDPH staff ask questions on overdose event circumstances, knowledge and practice of harm reduction strategies, substances used, and interest in substance use treatment. MCDPH defined recreational drug use as self-reported use of drugs for a nonmedical purpose within the past 12 months, excluding cannabis, such as socially, to cope, or to feel better. MCDPH defined intentional fentanyl use as the case patient either reporting that they intended to use fentanyl on the day of the overdose or reporting fentanyl as a drug that they use recreationally.
MCDPH employed 3 investigators to conduct interviews; MCDPH required investigators to have a bachelor’s degree in health promotion, public health, medical technology, health sciences, or a health-related field or to have an equivalent combination of education and experience. Investigators completed training classes hosted by external partners in motivational interviewing techniques and harm reduction principles. Investigators then completed outreach under supervision to ensure compliance and comfort with standardized processes. Throughout the interview, investigators provide harm reduction education, including the use of and access to naloxone. If the patient is interested in substance use treatment, the investigator can also conduct a direct transfer to Arizona’s Opioid Assistance and Referral Line, a 24/7 hotline that, among many services offered, can schedule an appointment and arrange transportation for the patient to receive substance use treatment. 6 In August 2022, MCDPH began offering patients a mailed harm reduction kit, which includes intranasal naloxone and fentanyl test strips (FTSs).
We used SAS Enterprise Guide version 8.2 (SAS Institute, Inc) to analyze case investigation data. We calculated frequencies stratified by year 1 and year 2 and by total years. To compare results between years 1 and 2, we used the Pearson χ2 test to calculate P values (using α = .05 to indicate significance). We suppressed demographic information where counts were <5. We calculated percentages for nonmissing responses.
Results
Results Across 2 Years of Data
During year 1 and year 2 of the case investigations, MCDPH received 7209 suspected nonfatal opioid overdose case reports in MEDSIS. About two-thirds (67.1%) of all reports were men, and the median (IQR) age was 36 (28-51) years. Among reports that showed data on race and ethnicity (n = 5819), 24.9% of the case patients were Hispanic and 58.1% were non-Hispanic White. Among the 7209 case reports, 2392 (33.2%) met internal sampling criteria and were eligible for investigation. Investigators contacted 2029 case patients; 592 (29.2%) were interviewed and 1437 (70.8%) were lost to follow-up.
Among the 592 case patients who were interviewed, 354 case patients (59.8%) self-reported recreational drug use and 238 (40.2%) did not. To better interpret the findings, subsequent results summarized here were limited to the 354 case patients who were interviewed and reported recreational drug use.
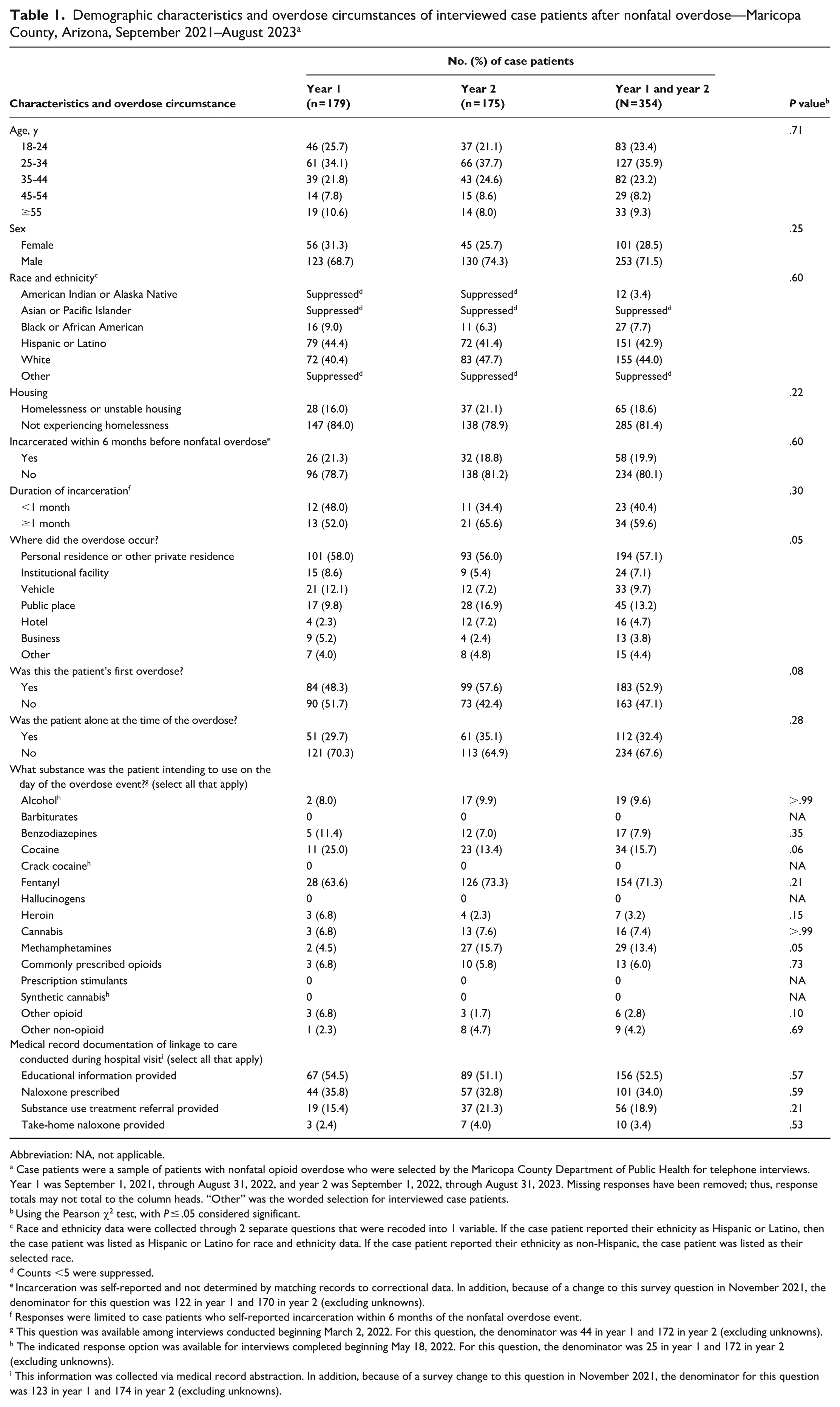
Among the 354 case patients with self-reported recreational drug use, 253 (71.5%) were men, and the median (IQR) age was 31 (25-40) years (Table 1). Most case patients identified as non-Hispanic White (44.0%) followed by Hispanic or Latino (42.9%). Of 350 case patients who responded, 65 (18.6%) reported currently experiencing homelessness or unstable housing. Of 292 case patients who responded, 58 (19.9%) reported being incarcerated at some point in the 6 months before the overdose event.
Demographic characteristics and overdose circumstances of interviewed case patients after nonfatal overdose—Maricopa County, Arizona, September 2021–August 2023 a
Abbreviation: NA, not applicable.
Case patients were a sample of patients with nonfatal opioid overdose who were selected by the Maricopa County Department of Public Health for telephone interviews. Year 1 was September 1, 2021, through August 31, 2022, and year 2 was September 1, 2022, through August 31, 2023. Missing responses have been removed; thus, response totals may not total to the column heads. “Other” was the worded selection for interviewed case patients.
Using the Pearson χ2 test, with P ≤ .05 considered significant.
Race and ethnicity data were collected through 2 separate questions that were recoded into 1 variable. If the case patient reported their ethnicity as Hispanic or Latino, then the case patient was listed as Hispanic or Latino for race and ethnicity data. If the case patient reported their ethnicity as non-Hispanic, the case patient was listed as their selected race.
Counts <5 were suppressed.
Incarceration was self-reported and not determined by matching records to correctional data. In addition, because of a change to this survey question in November 2021, the denominator for this question was 122 in year 1 and 170 in year 2 (excluding unknowns).
Responses were limited to case patients who self-reported incarceration within 6 months of the nonfatal overdose event.
This question was available among interviews conducted beginning March 2, 2022. For this question, the denominator was 44 in year 1 and 172 in year 2 (excluding unknowns).
The indicated response option was available for interviews completed beginning May 18, 2022. For this question, the denominator was 25 in year 1 and 172 in year 2 (excluding unknowns).
This information was collected via medical record abstraction. In addition, because of a survey change to this question in November 2021, the denominator for this question was 123 in year 1 and 174 in year 2 (excluding unknowns).
Most nonfatal overdoses (194 of 340; 57.1%) were reported to occur at home or another private residence; 52.9% (183 of 346) reported this to be their first overdose, and 32.4% (112 of 346) reported that they were alone at the time of the overdose. The 3 most common drugs that were intended for use on the day of the overdose were fentanyl (71.3%), cocaine (15.7%), and methamphetamines (13.4%). This question was revised in March 2022; thus, the total was limited to the 216 case patients who were asked the revised version of the question, excluding unknowns.
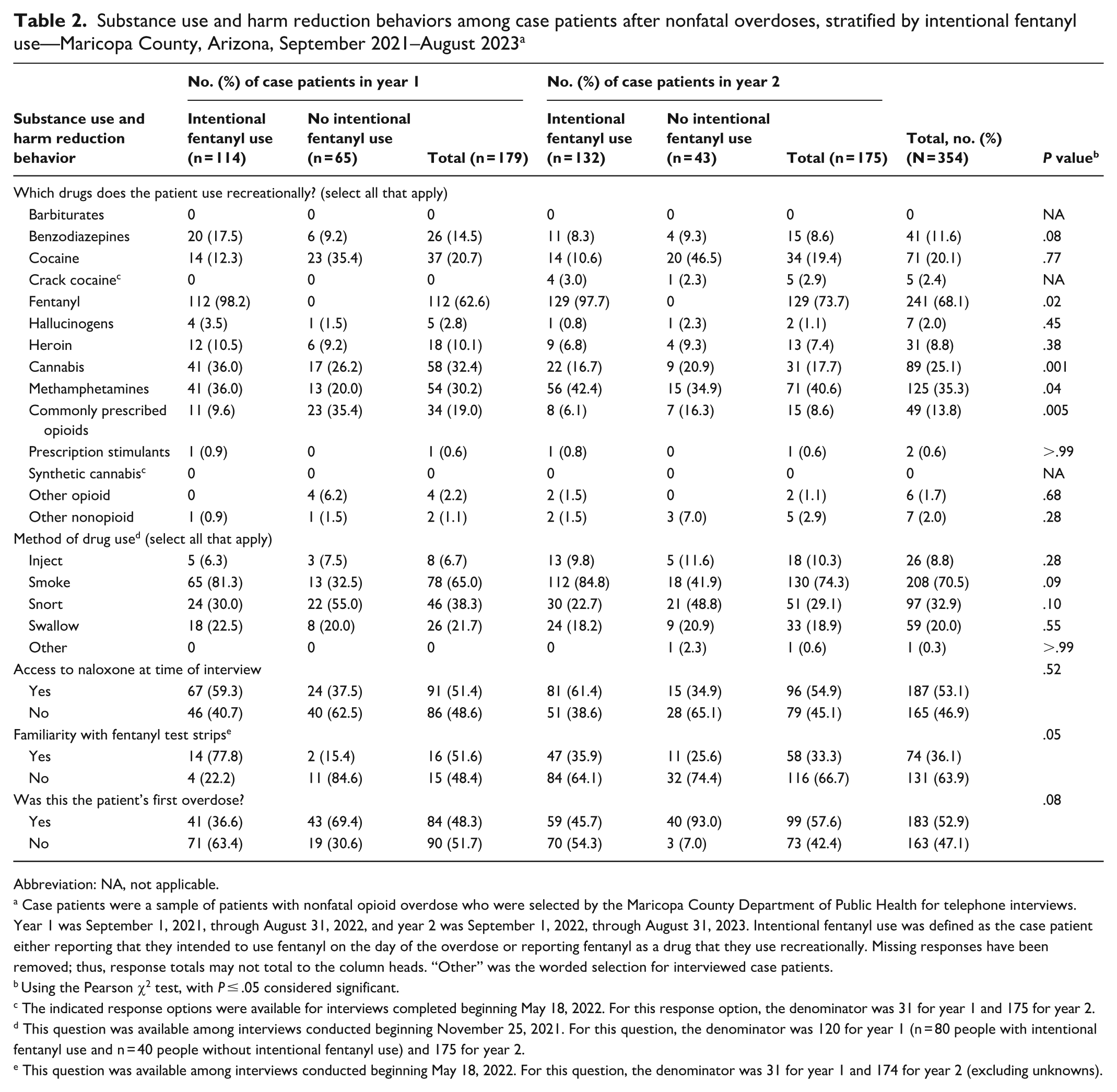
Among 354 case patients, fentanyl was the most common drug reported to be used recreationally (n = 241; 68.1%) (Table 2). Other commonly used drugs were methamphetamines (n = 125; 35.3%), cocaine (n = 71; 20.1%), commonly prescribed opioids (n = 49; 13.8%), and benzodiazepines (n = 41; 11.6%). Among 108 case patients who did not report using fentanyl intentionally, 39.8% (n = 43) and 27.8% (n = 30) were more likely to use cocaine and commonly prescribed opioids compared with those who reported intentional fentanyl use (n = 246). Rates of cocaine and commonly prescribed opioid use among 246 case patients with intentional fentanyl use were 11.4% (n = 28) and 7.7% (n = 19), respectively (P < .001 for both). Methamphetamines were more commonly used among those who reported intentional fentanyl use (39.4% [97 of 246]) than among those who did not (25.9% [28 of 108]; P = .01).
Substance use and harm reduction behaviors among case patients after nonfatal overdoses, stratified by intentional fentanyl use—Maricopa County, Arizona, September 2021–August 2023 a
Abbreviation: NA, not applicable.
Case patients were a sample of patients with nonfatal opioid overdose who were selected by the Maricopa County Department of Public Health for telephone interviews. Year 1 was September 1, 2021, through August 31, 2022, and year 2 was September 1, 2022, through August 31, 2023. Intentional fentanyl use was defined as the case patient either reporting that they intended to use fentanyl on the day of the overdose or reporting fentanyl as a drug that they use recreationally. Missing responses have been removed; thus, response totals may not total to the column heads. “Other” was the worded selection for interviewed case patients.
Using the Pearson χ2 test, with P ≤ .05 considered significant.
The indicated response options were available for interviews completed beginning May 18, 2022. For this response option, the denominator was 31 for year 1 and 175 for year 2.
This question was available among interviews conducted beginning November 25, 2021. For this question, the denominator was 120 for year 1 (n = 80 people with intentional fentanyl use and n = 40 people without intentional fentanyl use) and 175 for year 2.
This question was available among interviews conducted beginning May 18, 2022. For this question, the denominator was 31 for year 1 and 174 for year 2 (excluding unknowns).
Smoking (70.5%) and snorting (32.9%) were the most common routes of drug use. Smoking was more common among those who reported intentional fentanyl use (83.5%) than among those who did not report intentional fentanyl use (37.3%; P < .001). Snorting was more common among those who did not report intentional fentanyl use (51.8%) than among those who did (25.5%; P < .001). Approximately 10% of respondents reported injection drug use (IDU). Among those who reported IDU, 76.9% reported that they had injected with equipment that had been used by someone else.
Of 352 case patients, 187 (53.1%) reported having access to naloxone at the time of the interview. Naloxone access was less frequent among those who did not use fentanyl intentionally (36.4%; 39 of 107) than among those who reported intentional fentanyl use (60.4%; 148 of 245) (P < .001). Less than one-quarter (23.2%; n = 13) of case patients who did not use fentanyl intentionally were familiar with FTSs. This question was added to interviews in May 2022; the total was limited to the 56 case patients who did not report intentional fentanyl use and were asked this question. Case patients who did not use fentanyl intentionally were also more likely to report this as their first overdose compared with those who reported using fentanyl intentionally (79.0% [83 of 105] vs 41.5% [100 of 241], respectively) (P < .001).
According to hospital medical records, 3.4% of interviewed case patients had documentation of take-home naloxone being provided on discharge from the hospital, 34.0% had documentation of naloxone being prescribed, and 18.9% had documentation of a substance use treatment referral from the hospital.
Results Comparing Both Years
The proportion of case patients who reported experiencing homelessness or unstable housing increased slightly between year 1 and year 2 of case investigations, from 16.0% (28 of 175) to 21.1% (37 of 175) (P = .22).
The proportion of case patients who reported the event as their first overdose increased from 48.3% (84 of 174) in year 1 to 57.6% in year 2 (99 of 172) (P = .08). The proportion of case patients who reported being alone at the time of the overdose increased from 29.7% (51 of 172) in year 1 to 35.1% (61 of 174) in year 2 (P = .28).
A larger proportion of case patients reported that they were intending to use fentanyl on the day of the overdose in year 2 (73.3%) versus year 1 (63.6%) (P = .21).
Smoking drugs increased from 65.0% in year 1 to 74.3% in year 2 (P = .09). IDU increased slightly from 6.7% in year 1 to 10.3% in year 2 (P = .28). Increases in the recreational use of fentanyl (62.6% [112 of 179] vs 73.7% [129 of 175]; P = .02) and methamphetamines (30.2% [54 of 179] vs 40.6% [71 of 175]; P = .04) were also observed between year 1 and year 2, during which there was also a simultaneous decrease in the recreational use of commonly prescribed opioids (19.0% [34 of 179] vs 8.6% [15 of 175]; P = .005).
Discussion
This novel surveillance program, which samples nonfatal opioid overdoses in Maricopa County, allows public health to identify drug use and harm reduction trends among people who use drugs and who are at the highest risk of subsequent overdose. Although differences were not significant, the proportion of patients who reported intentional use of fentanyl increased, as did the proportion who experienced their first overdose and the proportion who were alone at the time of overdose. Despite increases in fentanyl use, the proportion of people who had naloxone access after a nonfatal overdose did not change.
Compared with all suspected nonfatal opioid overdose reports in MEDSIS during the study period, the proportion of interviewed case patients who reported recreational drug use was higher among male (vs female), younger (vs older), and Hispanic (vs non-Hispanic) case patients. Answers to questions about race and ethnicity asked during interviews may be more accurate than information obtained via electronic case reporting in MEDSIS.
Nonfatal overdose is one of the strongest predictors of a future fatal overdose,7,8 making the hospital an ideal setting for intervention. Only about half of case patients reported having naloxone access at the time of the interview, and documentation of take-home naloxone from the hospital was infrequent (3.4%). This finding highlights important gaps in harm reduction, particularly in the context of rising fentanyl-related overdoses, 9 which are more likely to cause a more rapid overdose onset than overdoses from other opioids. 10 Hospitals can be effective sites for harm reduction and should increase their efforts to distribute naloxone.11,12 Throughout our investigation period, health care facilities had initiated naloxone distribution programs at varying time points, including programs that distributed but did not dispense via a pharmacy, potentially increasing the likelihood that the distribution was not documented. With most overdoses occurring at a residence and most individuals reporting not being alone at the time of the overdose, take-home naloxone for friends or family who pick up patients from the hospital, education on how to identify the signs of an overdose, and messaging for regularly checking on those who are using drugs are recommended. 13 Knowledge of FTS among people who did not report using fentanyl intentionally was low in both years. Expanding FTS education and availability among people who do not use fentanyl intentionally is vital, and hospitals may be effective distribution points. 14 Because documentation of substance use referrals at the hospital was also infrequent (18.9%), hospitals should consider bolstering their activities to link patients to substance use treatment. 15
Most case patients had reported not being alone during the overdose event; however, the percentage of case patients who reported being alone during year 2 of the case investigations increased. Increasing education about the risks associated with using drugs alone and increasing awareness of virtual overdose monitoring services such as “Never Use Alone” 16 may reduce mortality. 17 With the high proportion of individuals reporting intentional fentanyl use, harm reduction messaging should also stress the importance of using drugs with others nearby and to use less drugs or to use drugs more slowly. 18 Supervised drug consumption sites for all people who use drugs, regardless of drug use route, should also be considered as a method to mitigate overdose-related harms. 19
Smoking and snorting drugs were the most commonly reported routes of drug use, which is consistent with patterns observed in fatal overdose data in the western United States. 20 Although IDU was the least reported route of drug use, a slight increase in IDU occurred in year 2, a trend that will need to be monitored. Use of nonsterile equipment was common among those who reported IDU. These findings underscore the importance of distributing sterile equipment that targets all routes of drug use. Syringe service programs are an effective strategy for reducing the transmission of infections associated with IDU, including HIV. 21
Because of the high proportion of case patients reporting unstable housing and known susceptibility of fatal overdoses in this group, overdose prevention strategies that better reach people who are experiencing homelessness, such as providing low-barrier care in nontraditional settings, are critical. 22 With 20% of patients reporting justice involvement, prevention strategies should also offer both harm reduction and access to substance use treatment in correctional facilities. 23
Although most comparisons of findings between year 1 and year 2 were not significant, our analysis allowed for the potential identification of changes in drug use behaviors, which would be responsive to rapid changes in the drug market. 24 In addition, conducting this analysis established the process for our routine surveillance reporting to present yearly on our website.
Our study had some limitations. First, because of the sampling criteria, the high number of people lost to follow-up, and the use of telephone interviews, our data are not generalizable. Individuals who experience a nonfatal overdose may be more inclined to practice behaviors that increase their risk of overdose, such as using fentanyl intentionally. Second, the collection of data on behaviors that are often stigmatized is susceptible to social desirability bias, which may lead to an underreporting of recreational drug use. Third, the completeness of information abstracted from medical records depends on the completeness of documentation by hospital staff. For example, if take-home naloxone is provided on discharge but not documented in the medical record, the number of people who are discharged with take-home naloxone will appear lower than in actuality.
Practical Implications
Case investigations of suspected nonfatal opioid overdoses have allowed MCDPH to collect overdose risk factor information not found in traditional public health surveillance sources, which has simultaneously allowed MCDPH an opportunity to provide harm reduction education and to link individuals to care and resources. Collecting data on overdose circumstances and harm reduction behaviors through case investigations can guide and help inform overdose prevention strategies. Data from MCDPH case investigations support 5 main strategies for overdose prevention: (1) improving naloxone access, especially among people who are not intentionally using fentanyl; (2) leveraging the role of hospitals as a point of care for people who use drugs by facilitating linkage to care and harm reduction services; (3) increasing harm reduction messaging, specifically around intentional fentanyl use, not using drugs alone, and using FTSs for those not intentionally using fentanyl; (4) increasing harm reduction services addressing all routes of drug administration, particularly noninjection; and (5) improving engagement with people experiencing homelessness and recently justice-involved populations.
This program can be adapted and scaled according to staff capacity by other public health agencies by either expanding or narrowing the investigation sampling criteria. MCDPH serves a population of about 4.5 million people and currently receives more than 3000 reports of suspected nonfatal opioid overdose each year. Smaller jurisdictions with a smaller volume of reports may be able to investigate a substantial proportion of their cases with fewer staff members. Jurisdictions with fewer resources may shorten the questionnaire or reduce the number of contact attempts to reduce the time needed to investigate a single case. Because the program does not operate as a case management service, instead providing education on existing community resources, the program operates similarly to the communicable disease investigations that public health departments routinely conduct, reducing the resources needed to operate and the specialization required of staff. Funding may be an additional challenge for jurisdictions wishing to adopt a similar program. During this time frame, MCDPH used funding through the Centers for Disease Control and Prevention’s Overdose Data to Action grant to launch and operate this program. 25
Since this program launched in 2021, MCDPH has made workflow changes to reduce inefficiencies, such as changing to a survey platform that had more straightforward features for revising survey entries for cases that require multiple contact attempts. In addition, survey questions were modified either based on investigator input or to collect more robust information for overdose prevention partners interested in making service enhancements. For example, in 2024, questions were added to gauge potential interest in peer navigation services.
Footnotes
Acknowledgements
The authors acknowledge the Maricopa County residents who participated in public health surveillance efforts of the Maricopa County Department of Public Health (MCDPH); Rebecca Sunenshine, MD (MCDPH; Career Epidemiology Field Officer Program, Centers for Disease Control and Prevention); and our clinical partners.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: A.P.D. declares participation in the Arizona Department of Health Services Human Subjects Review Board and support for traveling to the InFORM Western Regional Epidemiology Meeting in 2023 as well as the Arizona Infectious Diseases Society of America in 2021.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Centers for Disease Control and Prevention’s Overdose Data to Action grant (specifically for C.M., M.H.W., D.M., E.B.G., S.V., and M.C.).
Ethical Considerations
Arizona Administrative Code R9-4 Article 6 requires a public health authority, in this case Maricopa County Department of Public Health, to collect reports of suspected opioid overdoses within our jurisdiction. Therefore, data collection and analysis were completed for the purposes of public health practice to guide opioid overdose prevention strategies and did not require review by an institutional review board.