
Abstract
Introduction:
While public health measures including physical distancing and stay-at-home orders have clear benefits in COVID-19 mitigation and prevention, they have provided unique challenges for individuals with substance use disorder (SUD), including Treatment Court (TC) participants.
Methods:
This study involved a qualitative evaluation of TC Family Nights; one series of Family Nights was conducted before the COVID-19 pandemic and the second series was adapted and held remotely due to COVID-19 distancing requirements.
Results:
Several important themes emerged, including general positive experiences, accessible session logistics, naloxone training, attention to stigma, building recovery capital, group engagement, social interaction, and community action. These themes will help inform future SUD recovery education.
Conclusion:
Online recovery support events provide a new model for courts and recovery organizations that seek multiple ways to provide connection and support for their participants and families during times when accessibility is prioritized, in-person activities are discouraged, and in resource-sparse and geographically isolated communities.
Introduction
The effect of the coronavirus disease 2019 (COVID-19) pandemic continues, and is associated with mental health and substance use challenges that persist. 1 The pandemic has disproportionately impacted people with substance use disorder (SUD) for a variety of reasons, primarily centering on the overlapping risk environments for SUD and COVID-19, in addition to the diminishing of resources that individuals with SUD need in order to initiate or maintain recovery.2-4 Individuals with SUD have experienced disrupted access to services that they need to remain healthy, as well as decreased access to medications and treatment services.2,3 Individuals in recovery from a SUD have likewise struggled to access services and resources that promote recovery; as a result, relapse rates have risen.2,5
Drug Courts (DC) are a specialized court program that generally target non-violent offenders with substance use problems or SUD. 6 These programs provide participants with intensive court supervision, treatment for their substance use problem, mandatory drug testing, and other needed social services as an alternative to incarceration, along with expedited case processing.6,7 The goal of DC is to break the cycle of SUD and crime by supporting the participant to change their behavior and providing them with necessary resources to do so. 6 DCs benefit the legal system by allowing judges, state attorneys and public defenders who specialize in drug cases to become more proficient and efficient in their work while also eliminating inordinate delays in addressing drug cases. 8 The narrow focus of the DC team allows for greater fairness and equity in sentencing as well as a reduction in the time needed to adjudicate each case. 9
Research has shown that family members of individuals with SUD report struggling with stigma, identifying and securing treatment for their loved one’s SUD, obtaining training on naloxone, caring for minor children, and accessing self-care resources. 10 In recognition of the impact of SUD on the family system as well as the influence that the family system can make in treatment of an individual’s SUD, 11 the Adult Drug Court Best Practice Standards stress the importance of family and interpersonal counseling and interventions. 12 Although the widespread impact of SUD on the entire family system is well known,10,11 there are currently no published studies that describe innovative approaches to engaging DC participants’ family members to increase their knowledge of harm reduction and improve relationships between participants and loved ones as a part of the DC program. In addition, there is no data describing how educational approaches for treatment court participants have been modified and adapted to allow remote participation. This study involved analysis of DC Family Nights conducted for 3 neighboring DCs; one series of Family Nights was conducted before the COVID-19 pandemic and the second series was adapted and held remotely due to COVID-19 distancing requirements, both included DC participants and their families or support systems. The purpose of the study was to determine what DC participants found most useful about in-person and virtual Family Nights, as well as ways that both events could be improved or adapted to better serve DC participant and their families in the future.
Methods
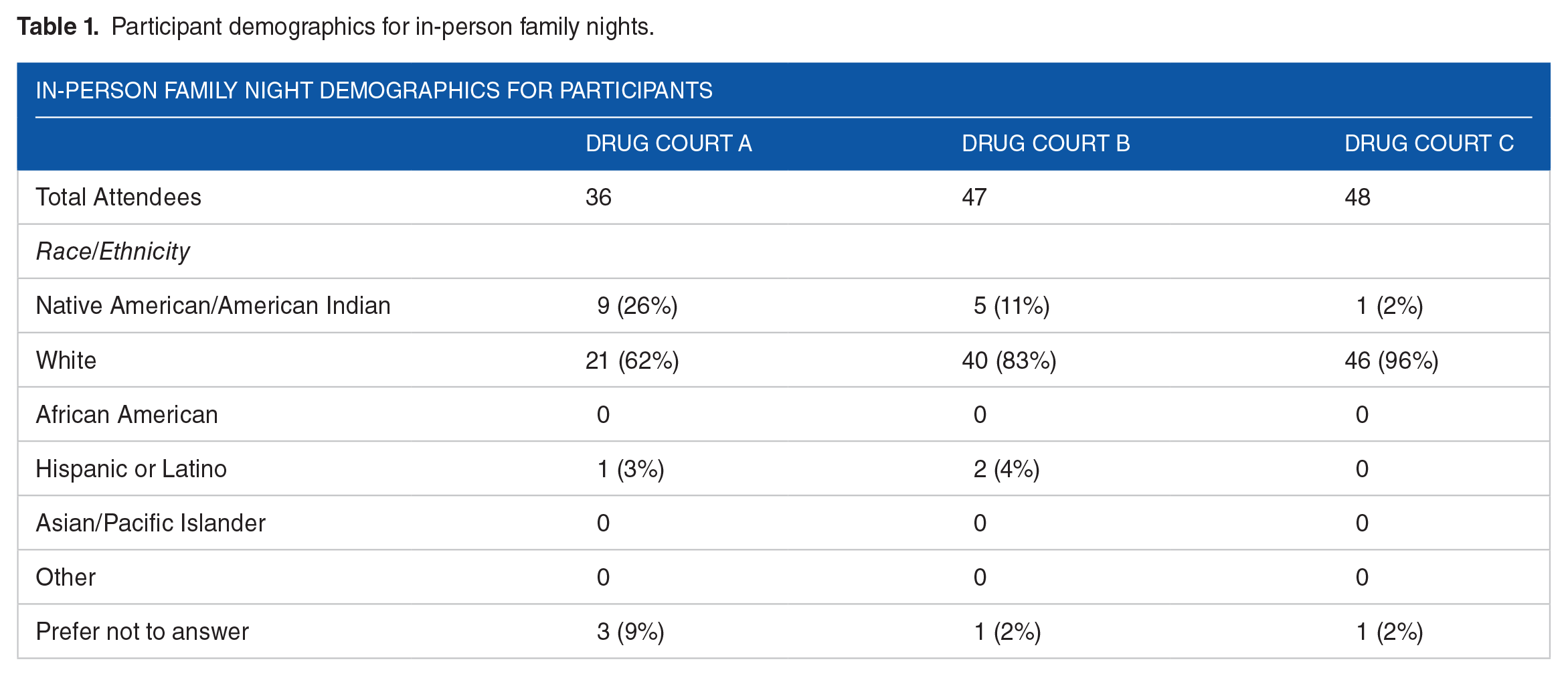
In-person TC Family Nights were held for 3 separate DCs in February and March of 2018. These sessions began with a time of fellowship and a shared meal with DC team members, participants, and their families or supporters, followed by break-out sessions for: (1) DC participants, (2) children of participants, and (3) supportive friends and family members of participants. DC participants had a private session with the local harm reduction organizations where they learned about naloxone administration and had the opportunity to be tested for HIV and hepatitis C. The training was offered to all participants regardless of their drug of choice or past use of opioids. Children were offered age-appropriate games and activities, and friends and family members attended a special session led by SUD professional who shared experience with having a family member with an SUD and resources. Participant demographics of adults from the 3 participating Treatment Courts who attended the in-person Family Nights are illustrated in Table 1.
Participant demographics for in-person family nights.
Virtual DC Family Nights were held in August of 2020 utilizing Zoom, after collaboration with area Treatment Court coordinators to determine how to best adapt Family Nights to conform to physical distancing requirements. These virtual Family Nights were focused on 6 different topics of interest to DC participants: Parenting Education, Financial Capability, taught by Extension educators, Birth Control Education, Family Non-violence Education, and a Naloxone Training taught by a licensed pharmacist. Each topic was discussed on a different night and was led by experts in each field, and was shorter in length (1 hour) compared to the pre-COVID family nights (3 or more hours). Family-engaged events such as home-based and timed scavenger hunts with prizes were added to the virtual family nights to encourage participation of family members. Participant demographics of adults who attended the virtual Family Nights are illustrated in Table 2.
Participant demographics for virtual family nights.

Data collection
Participants at the in-person Family Night were asked by DC coordinators to fill out a paper survey that took a mixed-methods approach with open- and closed-ended questions at the end of the event; adult family members in attendance were also encouraged to fill out the survey but were not required to do so. Participants in the virtual Family Nights were asked by their DC coordinator to complete an online survey at the end of the Family Night series that also included qualitative and quantitative questions; adult family members were also encouraged to fill out the survey but were not required to do so. Both surveys asked participants what they found to be the most meaningful part of Family Night and how Family Night could be improved in the future; they were also asked to rate how useful they found each component of the evening/session and how likely they were to use the information they learned. Each survey also included an open text option where participants could share any additional thoughts and suggestions they may have pertaining to Family Night.
Qualitative analysis
A Consensual Qualitative Research (CQR) approach was used to analyze survey results. 13 Using this method, 3 qualitative researchers with prior CQR experience reached consensus among domains and categories based on the study aims. The CQR process started with holistic coding in the first round to identify themes in larger sections of text. Initial domain themes were then independently identified for segments of raw data; larger segments of data were coded as a whole where applicable rather than coding line by line to address the research questions. Domain names were then cross-analyzed and used as the first iteration list for the next step in code mapping, where coding subdivisions were identified. The auditor reviewed and approved the domains and descriptions prior to the second round of coding. In second-cycle coding, themes became more descriptive, and codes were identified in a line-by-line fashion; this descriptive coding process allowed for the organization of domains around the goals of the event. During the second team meeting, consensus was reached and the coders discussed what codes might be combined.
Results
A total of 131 adults attended 1 of the 3 pre-COVID, in-person DC family nights that were held in 3 different communities. Attendance was much lower for the virtual family nights that were held during the COVID-19 pandemic, with a total of 55 adults attending a virtual DC family night event; some of the same individuals attended more than 1 virtual event. Attendees at the virtual family night events were unlikely to have attended an in-person event previously, as those events were held 2 years prior. While children attended both in-person and virtual family nights, with 50% to 75% of DC participants bringing at least 1 child to a Family Night event, children were not surveyed.
The most common theme noted across both in-person and virtual Family Nights included a general feeling that Family Nights were a
“The skills discussed were skills anybody from any walk of life could use.” “I found it very beneficial.”
The second most common themes noted across both types of Family Nights were focused on
“Loved that it had childcare.” “I’m glad it was on Zoom, I never would have gone in-person.” “I loved the food and free stuff!”
The third most common theme noted across both types of Family Nights was an appreciation for
“I liked how [the presenter] showed us exactly how to use the Narcan.” “I really appreciated the Narcan training.”
Of note, participants in the virtual events largely focused feedback on factors pertaining to the online platform, such as facilitator engagement, length, and the value of discussion time amongst participants. Of these 3 elements of online Family Nights, participants deemed discussion time most important. The topics presented at the online Family Nights that were determined to be most useful were naloxone education and parenting education, followed by financial capability, advocates for peace, and then birth control education.
Responses focused on the naloxone (Narcan) training, provided in all 3 of the in-person Treatment Court Family Nights and 1 of the 5 virtual Treatment Court Family Nights, were consistently rated positively. These responses were subjective answers to the question: “What was the best part about Family Night?” Specific responses included: “Learning how to save someone’s life” and “taught me what to do when a friend/family member overdoses.” Treatment Court participants in recovery and their families were able to learn information about reversing opioid overdoses 10 and obtain Narcan kits from treatment court coordinators when they had required appointments or court visits.
Responses from participants calling for increased community awareness and education made up another frequently mentioned theme. Within that category, participants called for bringing the Family Night activities to a wider audience, “Continue putting information out there for families to use,” and reducing stigma to support recovery efforts, “By helping or hiring people in the community and understanding that everyone needs help and support, no matter what they have done in the past.”
Discussion
Virtual DC Family Nights may serve as a viable way to connect the DC team with participants and their families when online participation and accessibility is a priority, while also remaining consistent with CDC recommendations to expand the distribution and use of naloxone and overdose prevention education, expand awareness about and access to and availability of treatment for SUD, and intervene early with individuals at high risk for overdose. 14 The increase in online treatment, recovery, and harm reduction programing that was necessitated by the COVID-19 pandemic was seen as a positive for some individuals in treatment and recovery, with some participants in this study reporting that they preferred online to in-person and would not have attended an in-person event.
DC participant’s appreciation for naloxone training was not surprising, given that these DC family nights were held in northeastern Minnesota, which has one of the highest rates of opioid overdose in the state along with low access to harm reduction resources. The vast majority of individuals who use drugs in this geographical region have lost a friend or loved one to opioid overdose, or have themselves had an overdose reversed with naloxone. 15 In previously published research, injection drug users (IDUs) reported a high prevalence of witnessing overdose events. 16 In one Bay Area survey, for example, 89% of participants reported witnessing an overdose event. 17 Qualitative research with IDUs indicates that fear of police is a significant barrier to calling emergency medical services (EMS) during an overdose event.16,18 Training DC participants and their family members in naloxone indication, use, and laws will allow this group to educate friends and family members, advocate for naloxone availability, and potentially save a life.
The ability to engage participants online during the COVID-19 pandemic provided a unique opportunity to increase accessibility and connect participants through virtual features such as the chat function, making the experience more individualized. While there were fewer participants in virtual DC Family Nights, the online engagement with conversation and the chat function far exceeded DC Coordinator expectations. This innovative model for engaging DC participants and their families has been continued even after the pandemic, and is especially useful for geographically isolated communities that have difficulty in recruiting expert speakers to provide education.
Conclusion
Online support events may serve as a model for other programs that seek ways to increase accessibility, promote inclusion, and remain connected to individuals with SUD or in recovery and their families. Online Family Nights successfully engaged DC participants that would not otherwise participate in in-person programing, and should be offered alongside in-person social support events for greater inclusion. This model may also be of interest for DC in resource-sparse and geographically isolated, rural communities that seek ways to provide connection and support for their participants who have barriers to attending in-person events.
Topics for discussion and education at DC Family Nights are best chosen by consulting participants and their supporters. While future research is needed, the results of this data provide support for a multi-pronged, multi-disciplinary and adaptable approach to recovery and stigma reduction that respects and honors the “voice” and lived experience of the individuals in recovery.
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The in-person Treatment Court Family Nights were supported by a Statewide Targeted Response to the Opioid Crisis grant (Minnesota DHS, 2017) and the virtual Treatment Court Family Nights were supported by a SAMHSA Rural Opioid Technical Assistance grant (1H79T108900-01).
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Laura Palombi supported the funding of the project, conceived and designed the analysis, collected the data, oversaw the analysis, and wrote the paper. Anna Van Deelen analyzed the data and wrote the paper. Andrew Hawn analyzed the data and wrote the paper. Lucas Kosobuski analyzed the data and wrote the paper. Mary Jo Katras supported the funding of the projects, analyzed the data and wrote the paper.