
Abstract
Amid a resurgence of measles in the United States, public health practitioners must respond to emergent cases and closing gaps in population immunity, while preserving continuity of other essential health services.1,2 Among the world’s most contagious diseases, measles can cause brain damage and pneumonia and leave survivors with immune system amnesia, placing them at increased risk of illness from other diseases.3,4 Recent large-scale outbreaks in the United States, which eliminated measles in 2000, underscore the need for continued vigilance, especially with risks posed by travel, case importation, and pockets of under- and nonvaccination among socially and medically vulnerable populations and in congregate settings.5,6
Impact on Public Health Agencies
Measles imposes operational burdens on state and local public health agencies (PHAs). Contact tracing, laboratory testing, postexposure prophylaxis, isolation and quarantine, and community engagement are time- and labor-intensive components of the outbreak response and often divert limited resources from other essential public programs and services. 6 Mitigation measures such as closures of schools, childcare centers, and workplaces may impose additional burden on the community. 7 Steep costs also accompany measles outbreaks: one analysis estimated median response costs of $223 per contact, $32 805 per case, and $152 308 per outbreak during 2001-2018. 8 Similarly, a single 2019 outbreak of 72 confirmed measles cases in Clark County, Washington, resulted in more than $3 million in societal costs, including $1 million in lost productivity and $2.3 million in public health response costs. 9 Finally, dwindling PHA budgets, eroding public trust in government institutions, health workforce burnout and attrition, and rising vaccine hesitancy due to mis- and disinformation amplify the threat of measles, even as the United States approaches the 25th year of its postelimination era.9 -11
A Theory of Change for Optimizing Measles Response
We propose a theory of change describing how PHAs could harness actionable metrics and strengthen operational learning capacities to reduce the measles-associated incidence and morbidity in their jurisdictions. Theory-of-change models are the basis of robust monitoring, evaluation, and learning (MEL) frameworks, processes, and metrics. Such models are ubiquitous in public health research and practice and can be used to articulate programmatic goals, design interventions, explore causal relationships, and assess the fidelity of program or policy implementation. A logic model (Figure) highlights pathways for PHAs to implement an effective measles response. Linking measurable inputs, processes, outputs, outcomes, and effects via a cohesive theory of change is an important prerequisite to measuring the performance of public health systems. 12 The analysis presented in this article was approved by the Johns Hopkins Bloomberg School of Public Health Institutional Review Board (#00028357).
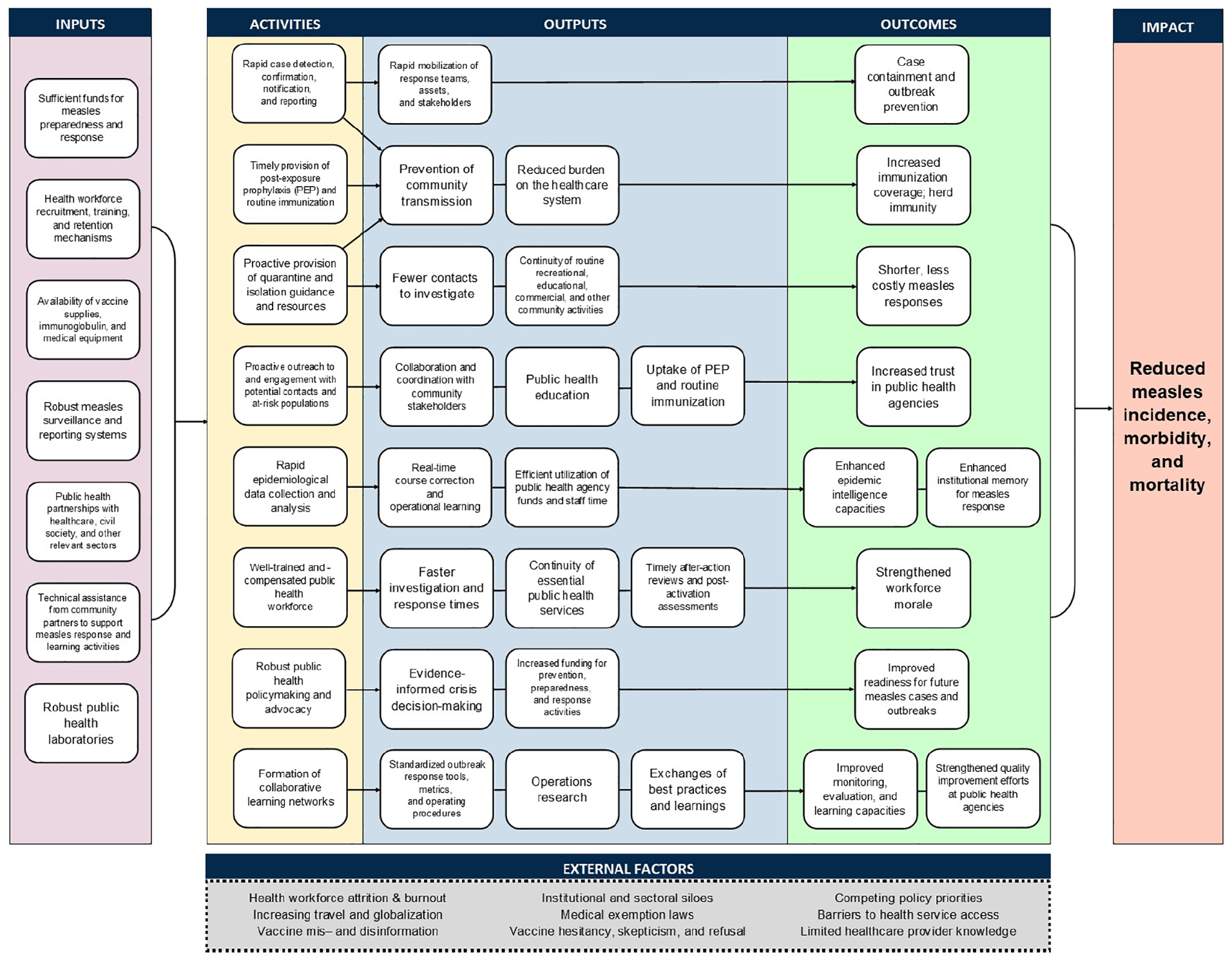
Logic model for reducing measles-associated morbidity and incidence through enhanced public health measles response efforts. Abbreviation: PEP, postexposure prophylaxis.
PHAs as Learning Organizations
Ansell et al 13 described 4 key capacities of public organizations that are especially vulnerable to erosion and neglect: (1) rapid response to emergent events; (2) anticipation of future events, demands, and needs; (3) monitoring, or the ability to systematically collect information; (4) and learning, or the ability to harness information and draw inferences from past events to improve institutional effectiveness. Measles outbreaks function as proverbial “canaries in the coal mine,” highlighting PHA vulnerabilities, deficiencies in institutional and systems-level learning, and gaps in immunization coverage that portend the incidence of other vaccine-preventable infections.14,15 Furthermore, because the transmissibility and clinical severity of measles demand targeted approaches to case and outbreak management, PHAs possessing the aforementioned key capacities are likely better prepared to prevent and mitigate other infectious disease outbreaks than PHAs that do not have these key capacities.6,16
During measles responses, PHAs are the connective tissue between partners across health care systems, laboratories, and communities at risk of experiencing measles outbreaks, performing vital integrative, coordinating, and outreach roles. As such, they are well-positioned to identify lessons learned and best practices from previous responses, which provide learning opportunities for strengthening PHA capacities and improving operational efficiency. PHAs that proactively monitor, evaluate, and learn from previous responses to notifiable diseases such as measles may also be better equipped to collaborate with partners to implement swifter, more cohesive responses to future events. Learning enables health systems to improve performance, adapt to complex operating environments, foster innovation, and build cultures of strong governance and accountability.17-19 Previous studies have also demonstrated that evaluations performed during measles response activations can support real-time operational learning and decision-making; yet, many PHAs lack standardized, actionable performance metrics for assessing outbreak management and disaster response activities.20,21 Furthermore, few PHAs have formally codified practices for evaluating response activities, identifying bottlenecks, or enabling real-time, operational learning during a measles response.22-24
Elements of an Effective Measles Response
The Centers for Disease Control and Prevention (CDC) defines a measles outbreak as a chain of transmission including 3 or more cases linked in time and space. 25 We define an effective measles response as the timely containment of emergent cases before escalation to an outbreak, as made possible by rapid case detection, reporting, and confirmation; timely provision of postexposure prophylaxis and routine measles immunizations to susceptible community members; proactive provision of quarantine and isolation guidance and resources; proactive outreach to and engagement with potential contacts and populations at risk of experiencing measles cases and outbreaks; rapid dissemination of risk messaging and health information; robust epidemiologic data collection and analysis; and a well-prepared public health workforce that makes efficient use of PHA resources (eg, staff time, funding). Where emergent measles cases cascade into an outbreak, we further define an effective response as the rapid reduction of disease incidence to zero, with minimal disruption to routine educational, commercial, recreational, and other community activities.
Efforts to enhance measles responses create valuable opportunities for PHAs to engage in operational learning during and after outbreaks, especially by forming communities of practice with civil society partners, health care organizations, community leaders and members, and other relevant partners involved in mitigating communicable disease. Such collaborative learning networks could also support after-action review activities and facilitate exchanges of best practices in measles response as well as support long-term knowledge management within and across PHAs.
Metrics: Building Blocks for Operational and Organizational Learning
In its Public Health 3.0 model, the US Department of Health and Human Services underscores the importance of collecting actionable data and delineating metrics to assess public health initiatives and monitor progress toward equitable health outcomes, with a focus on addressing social determinants of health. 26 By integrating formal metrics that target these considerations into routine measles planning, response, and MEL activities, PHAs can track progress toward improving outbreak management and ultimately reducing the measles-associated incidence and morbidity in their jurisdictions. Robust metrics could also help improve public understanding of measles response operations, strengthen accountability between PHAs and their constituents, and facilitate evidence-informed policy formulation and decision-making in measles preparedness and response. 27
Although metrics are a cornerstone of effective MEL, developing, validating, collecting, and monitoring metrics may prove to be time- and labor-intensive for resource-constrained PHAs. 28 Therefore, to enhance performance assessment and learning while minimizing operational and administrative burdens, we advocate for PHAs to adopt a core set of priority metrics for measles response. Like the Centers for Medicare & Medicaid Services’ “Universal Foundation” and the National Public Health Performance Standards28 -31—which aim to align measures nationally, across health system programs, institutions, and settings—core metrics for measles response could enable practitioners to compare response efforts across space, time, and institutions; identify quality improvement priorities; and improve response operations across diverse implementation contexts.28 -31 Core metrics could also provide multisectoral partners with a common language for evaluating progress toward shared population health goals. Finally, when combined with corresponding tools and resources as part of a robust technical package for measles response, core metrics could guide progress toward alleviating pain points and support innovation in outbreak mitigation.
Drawing from a purposive literature review, we present illustrative examples of core measles response–focused metrics (Table) to support MEL activities at PHAs.7,31 -40 Core metrics adopted by PHAs need not remain static; rather, they may be adjusted over time in alignment with evolving PHA capacities and population health priorities in a given jurisdiction. However, we posit that a selection of the metrics could comprise a solid foundation for informing quality improvement efforts, optimizing response operations, and comparing measles response activities across PHAs nationally.
Examples of core input, process, output, outcome, and impact metrics for assessing measles response activities at public health agencies identified from the literature a
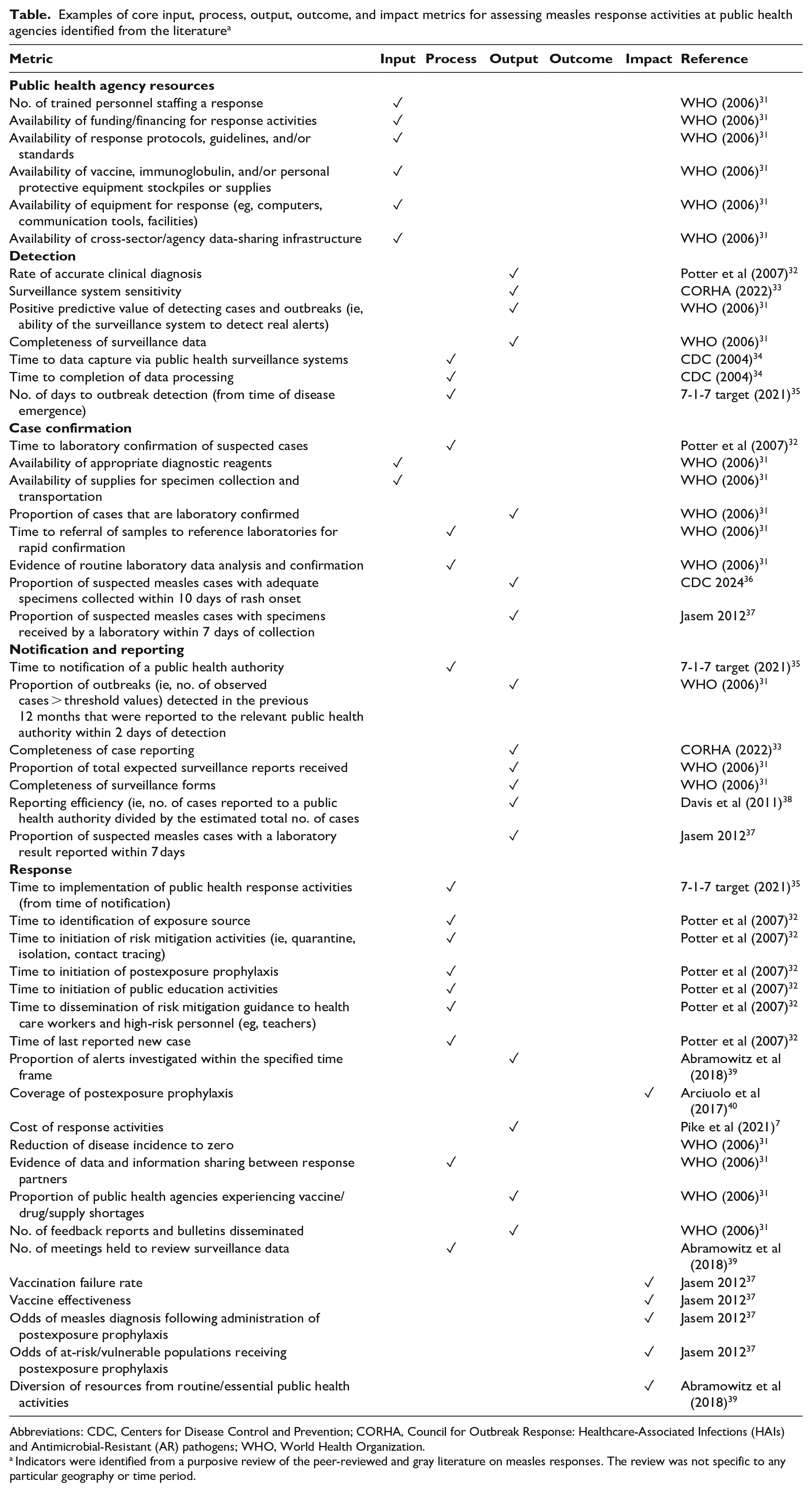
Abbreviations: CDC, Centers for Disease Control and Prevention; CORHA, Council for Outbreak Response: Healthcare-Associated Infections (HAIs) and Antimicrobial-Resistant (AR) pathogens; WHO, World Health Organization.
Indicators were identified from a purposive review of the peer-reviewed and gray literature on measles responses. The review was not specific to any particular geography or time period.
Metrics Considerations for Research, Policy, and Practice
PHAs seeking to strengthen adaptive learning capacities for measles response should consider several factors relating to metric development, selection, uptake, and operationalization. First, the theory of change and metrics presented herein are largely setting agnostic; as such, PHAs may need to modify metrics to account for their jurisdictions’ unique implementation contexts. Furthermore, despite recent surges in measles incidence across the United States, cases and outbreaks remain relatively rare in many jurisdictions; thus, PHAs may have limited opportunities to test potential response metrics. Nevertheless, broad adoption of a core set of standardized, actionable metrics could enable comparison across PHAs that do respond to measles; highlight opportunities for intraresponse course correction, learning, and quality improvement; and support longer-term advocacy activities for outbreak readiness. 41 Concurrently, localization (ie, gathering evidence relating to local contexts and needs) and tailoring (ie, transforming data into actionable messages for decision makers) should also be priorities for improving measles response performance and enhancing resilience to future public health threats.41 -43
When designing measles interventions, PHAs should also consider which metrics are both meaningful and feasible to monitor. These considerations may be especially relevant to PHAs with limited human and financial resources to respond to measles or undertake intensive MEL activities. Indicators that are not readily available, obtainable, or computable, for example, will prove challenging to monitor over time. Conversely, while purely mechanistic indicators of response performance, such as number of vaccines administered and contacts investigated, may be convenient to track, they do not account for institutional norms, practices, and values that also shape outbreak response efforts. Thus, when localizing metrics for measles response, practitioners should consider PHA governance structures, community health priorities and demographic characteristics, power dynamics, relationships between responding entities and community partners, and engagement with socially and medically vulnerable populations in their jurisdictions. Calibrating metrics to these factors could also guide PHAs toward implementing equitable responses to measles cases and outbreaks.44 -46 To avoid duplicating efforts or overburdening workforces, resource-constrained PHAs might also consider focusing on metrics that align with existing community health assessments, routine data collection activities, or strategic plans for public health improvement.
Identifying appropriate leading indicators that are modifiable in the near term could facilitate course correction during an ongoing response (eg, time to identification of an exposure source; evidence of data and information sharing between response partners). By contrast, an overt focus on distal health outcomes and impacts (ie, lagging indicators that change very slowly at the population level) could divert PHAs from eliminating tractable bottlenecks in their measles response protocols. 47 Given the wide-ranging public health, economic, and social burdens associated with measles, PHAs may also wish to prioritize metrics that capture system failures (eg, numbers of un-/misdiagnosed measles infections, unreached contacts, missed opportunities for vaccination) as well as programmatic successes. 48 Linking these outputs to proximal outcome indicators (eg, number of measles exposures, cost of response) could better support decision-making during a measles response and identify urgent priorities for learning and quality improvement. 49 Finally, PHAs should consider indicator relevance for different audiences: process indicators (eg, time to notification of a measles case), for example, may be more relevant for internal quality improvement purposes than output and outcome indicators are (eg, number of outreach activities performed, immunization coverage). Conversely, output and outcome indicators may be more salient than input indicators to funders, policy makers, and community members affected by measles cases and/or outbreaks.
PHAs can take several approaches to balance these competing considerations. For example, practitioners might consider building what Saha et al 19 described as a “living library of measures” that features both core leading indicators for measles response and “flexible” metrics that are iteratively tested and refined over time. PHAs could also collaborate with academic partners and other multisectoral partners to design pilot studies to validate candidate indicators. Potential methods include performing Delphi studies or applying other nominal group techniques to generate expert consensus on priority metrics to operationalize within jurisdictional contexts.50,51 Balanced scorecard frameworks, which have previously been used to evaluate and improve foodborne disease surveillance systems, could further enable PHAs to integrate community input into their MEL practices for measles response.52,53 Finally, PHAs could explore technological solutions to indicator monitoring and management, such as by developing dashboards to support measles surveillance and response activities.54,55 This approach comports with a recent report that more than 50% of local health departments in the United States are currently undertaking data modernization initiatives, with many already using public health informatics to drive quality improvement and assurance (43%), surveillance (59%), laboratory (47%), and program improvement (43%) activities. 56
Upon designating a set of priority metrics for measles response, PHAs must also consider how to link these measures to ongoing knowledge management activities. Knowledge management is a vital function of learning health systems and refers to the creation, sharing, translation, and application of knowledge (including metrics) to create value, improve organizational effectiveness, and enhance public health service delivery. 57 Given the high rates of workforce attrition at many PHAs, robust knowledge management practices could help preserve institutional memory and ensure that effective strategies from past measles responses are not forgotten. 58 PHAs should also consider how best to harness measles response metrics in support of longer-term programmatic, policy, and advocacy efforts. Metrics are useful constructs for communicating with policymakers about the public health importance of measles and other communicable diseases and could build a compelling case for increased funding for outbreak preparedness, response, and health workforce development and additional resources for vaccine promotion and community outreach efforts. 59
Conclusion
Measles continues to pose serious operational challenges to PHAs in the United States. While prevention remains the best strategy for averting the public health burdens of this disease, targeted approaches to case management and outbreak containment are still urgently needed in the postelimination era. A core set of priority, evidence-based performance metrics rooted in a sound theory of change could pave the way for more agile responses to emergent cases and outbreaks and help catalyze long-term policy changes to enhance outbreak readiness. Collaboration with relevant partners could further support continuous learning, innovation, and quality improvement efforts at PHAs. National bodies, such as CDC, the National Association of County and City Health Officials, and the Association of State and Territorial Health Officials, could play important roles in convening PHA partners to identify and validate relevant metrics. Ultimately, PHAs that build robust adaptive and operational learning capacities during measles responses will be well equipped to safeguard population health from measles and other known, emerging, and evolving communicable disease threats.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This analysis was supported by the Centers for Disease Control and Prevention (cooperative agreement no. NU38FT000004).