
Abstract
Objectives:
To gather perspectives on childhood vaccination and vaccine hesitancy, the Saint Louis County Department of Public Health (DPH) surveyed parents seeking nonmedical exemptions, conducted focus groups of school nurses, and interviewed pediatricians.
Methods:
We distributed exemption forms and voluntary questionnaires to parents in St Louis County who were seeking nonmedical exemptions for their school-aged children at any DPH clinic from August 2019 through December 2022. We conducted and recorded four 75- to 90-minute focus groups of 11 school nurses in groups of 2 or 3 nurses in September 2022. We conducted and recorded interviews of 8 pediatricians in March 2023. We calculated descriptive statistics, transcribed focus group discussions and interviews, and performed qualitative coding.
Results:
We collected 1871 exemption forms. The median age of children (n = 1854) was 6 years. Of the 10 vaccines included in the exemption list, the percentage of exclusions ranged from 91.2% for meningococcal conjugate to 88.7% for hepatitis A. We identified 4 themes in the focus groups: recent changes in vaccine compliance, hesitancy and barriers, services addressing hesitancy and barriers, and future requests for DPH. Analysis of pediatrician interviews revealed themes relating to vaccine information, community efforts, and physician decision-making.
Conclusions:
This study highlights the need for a multidisciplinary approach to vaccine hesitancy in St Louis County. Future interventions need to focus on beliefs and behavioral change related to vaccines and not just the economics and accessibility of vaccines.
Vaccinations are among the greatest public health achievements of the 20th century, saving millions of lives and billions of dollars annually. 1 Yet, in recent years, vaccine providers and programs have faced challenges, such as mistrust of health care providers, parents creating their own vaccine schedules, and misinformation, leading to resurgences of diseases in countries close to eradicating them.2,3 The growing opposition to vaccines has necessitated definition by the Strategic Advisory Group of Experts, which defines vaccine hesitancy as the “delay in acceptance or refusal of vaccination despite availability of vaccination services.” 2 Childhood vaccines, in conjunction with school immunization requirements, which are important methods of perpetuating herd immunity, are a flashpoint for antivaccine efforts. 4 In Missouri, school immunization rates declined during the past decade across all required vaccines, although a corresponding increase in vaccine-preventable diseases has not yet been observed.5,6 Simultaneously, requests for religious exemptions have increased; Missouri allows religious and philosophical exemptions.5,7 This increase in requests reflects national trends. 8 It is unclear whether rising exemption rates result from increased opposition to vaccination or from families seeking exemptions because of barriers to vaccination or convenience. 8 In Missouri, seeking an exemption can be more convenient than obtaining a vaccination, with exemption cards available online through the Missouri Department of Health and Senior Services, at local health departments, and at physicians’ offices. 7
Studies addressing socioeconomic factors and social determinants of undervaccinated or nonvaccinated children have found that hesitant families may have financial difficulties, have vaccine safety concerns, are influenced by misinformation, seek alternative care, or have a low perceived risk of the disease.9,10 Additionally, vaccination services were disrupted during the COVID-19 pandemic, creating new challenges for parents and health care providers. 11 School nurses and pediatricians play a pivotal role in addressing social determinants and educating parents about the severity of disease and the safety of vaccines.9,12 Qualitative studies have also explored health care provider attitudes, protocols, and strategies used to discuss vaccinations in clinical settings.13 -15
This project conducted formative research on nonmedical exemptions, laying the groundwork for the Saint Louis County Department of Public Health (DPH) to devise interventions to improve vaccine uptake among pediatric patients. This multimethod study included quantitative survey data from parents in St Louis County seeking nonmedical exemptions and qualitative data from school nurse focus groups and pediatrician interviews. The aim was to gather perspectives from these groups on current vaccination practices and trends in schools, barriers among students, challenges faced by school nurses in getting students up-to-date on vaccinations, and pediatricians’ current vaccine practices, as well as how DPH can aid parents, school nurses, and pediatricians in improving vaccine uptake.
Methods
This multimethod study was approved by the DPH Internal Research Review Committee as a public health practice endeavor.
We collected quantitative data through exemption forms and questionnaires distributed to parents seeking nonmedical exemptions for their school-aged children at DPH’s 3 clinics. The exemption form lists 10 vaccines; DPH exemption policies mandate completion of the exemption form. Completion of the parent questionnaire was voluntary (eAppendix A in the Supplement). We used the initial voluntary questionnaire (n = 889) from August 2019 through June 2022 and an updated voluntary questionnaire (n = 300) from July 2022 through December 2022. The updated questionnaire added questions on attitudes toward vaccines, socioeconomic characteristics, and religious and philosophical beliefs (eAppendix B in the Supplement).
We interviewed 11 school nurses in four 75- to 90-minute focus groups of 2 or 3 nurses each and recorded groups via Webex in September 2022. We recruited participants via email. Eligibility included nurses actively working for public or private schools and districts. We provided participants a $50 Visa gift card at the end of the focus groups. DPH epidemiologists developed focus group questions based on parents’ answers from the parent questionnaire (eAppendix C in the Supplement). We created the codebook for qualitative analysis (eAppendix D in the Supplement) inductively and deductively based on preconceived notions and new themes emerging from the focus groups.
We conducted and recorded via Webex 8 pediatrician interviews in March 2023. Eligible participants included currently practicing physicians (doctor of medicine or doctor of osteopathic medicine) and nurse practitioners working in pediatrics or family medicine in St Louis (the city) or St Louis County, Missouri. We used purposive sampling, seeking out health care providers named in parent questionnaires. We sent recruitment letters to health care provider offices via fax and email. We provided participants a $150 Visa gift card at the end of their interview. We created a codebook (eAppendix E in the Supplement) inductively while reviewing transcripts.
We calculated descriptive statistics by using Excel for Office 365 (Microsoft Corp) and R version 4.2.2 (R Foundation for Statistical Computing). We ensured privacy by storing data on secure DPH servers and redacting participants’ names. We transcribed focus groups and interviews through otter.ai’s transcription program. We completed qualitative coding by using MAXQDA 2022 (VERBI GmbH) and examined codes thematically to identify major and minor themes.
Results
We collected 1871 exemption forms among DPH’s 3 clinics. Of the children’s ages provided (n = 1854), the median age was 6 years. Of the 1871 forms, 1739 had 1 or more vaccines selected (132 were left blank). Parents sought exemptions for the 10 vaccines on the exemption list at rates ranging from 88.7% (1542 of 1739) for hepatitis A to 91.2% (1586 of 1739) for meningococcal conjugate (Table 1). Of the 1848 parents who provided reasons for asking for an exemption, the majority selected religious reasons (81.8%; 1512 of 1848), followed by personal or philosophical beliefs (44.2%; 817 of 1848).
Types of vaccines for which parents and guardians sought nonmedical exemptions (N = 1739), St Louis County, Missouri, August 2019–December 2022 a
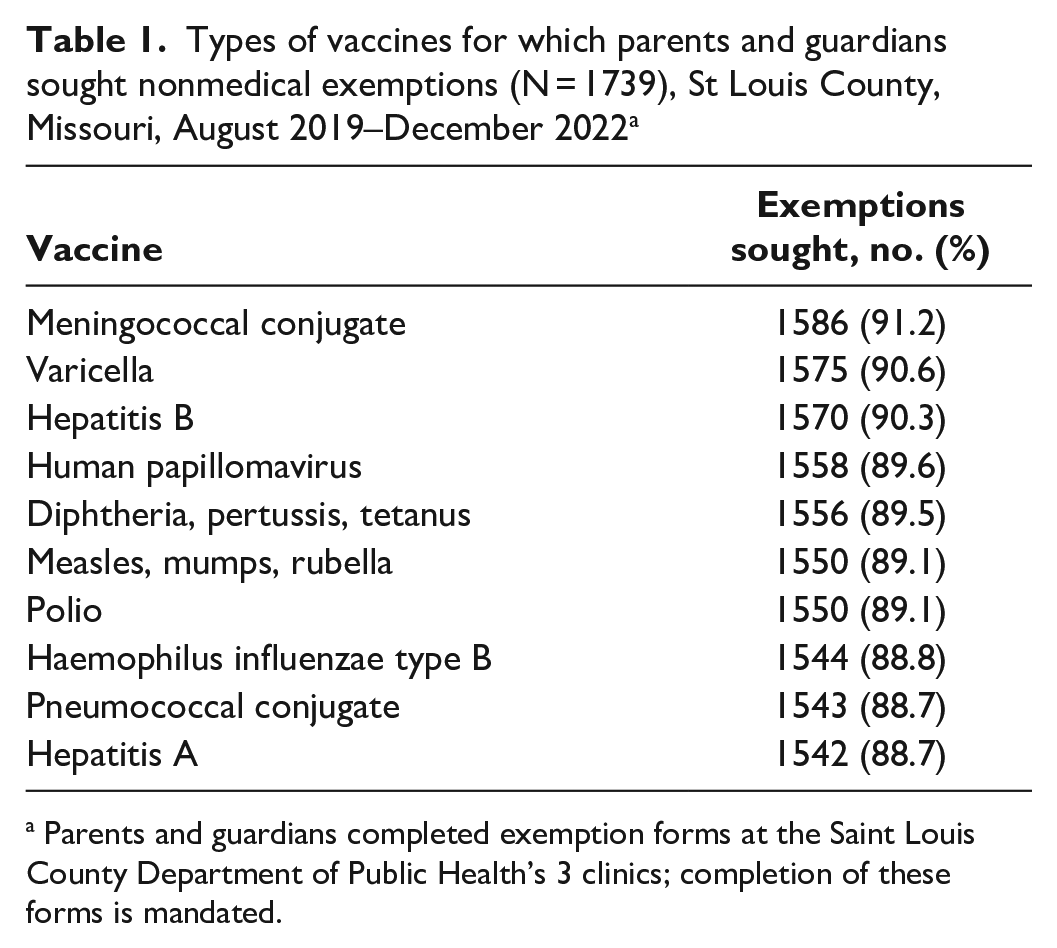
Parents and guardians completed exemption forms at the Saint Louis County Department of Public Health’s 3 clinics; completion of these forms is mandated.
Most parents (63.5%; 1189 of 1871) completed the voluntary questionnaire. Of the parents who completed the questionnaire, 76.5% were non-Hispanic White, 8.6% were Black or African American, and 1.9% were Hispanic or Latino (Table 2). Race and ethnicity were unknown for 8.0% of respondents (n = 95). Of 300 parents who answered the additional questions on the updated questionnaire, 71.0% were in 2-parent households, and 62.0% had an annual household income ≥$85 000. Of 1189 respondents, 78% (n = 928) indicated that their child had a primary care physician, 92.3% (n = 1097) reported talking to a medical professional about vaccines, and 83.0% (n = 997) reported getting vaccine information from a medical professional.
Demographic characteristics of children and households of guardians seeking nonmedical exemptions for vaccines, St Louis County, Missouri, August 2019–December 2022 a
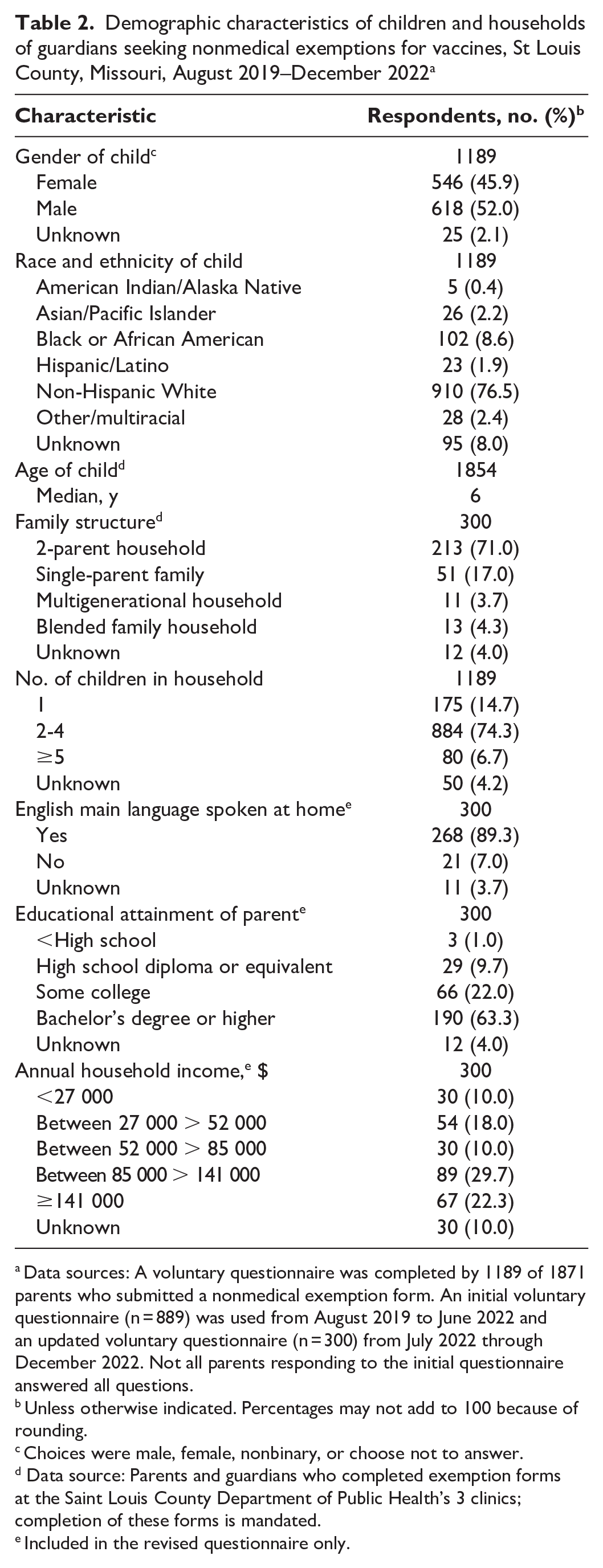
Data sources: A voluntary questionnaire was completed by 1189 of 1871 parents who submitted a nonmedical exemption form. An initial voluntary questionnaire (n = 889) was used from August 2019 to June 2022 and an updated voluntary questionnaire (n = 300) from July 2022 through December 2022. Not all parents responding to the initial questionnaire answered all questions.
Unless otherwise indicated. Percentages may not add to 100 because of rounding.
Choices were male, female, nonbinary, or choose not to answer.
Data source: Parents and guardians who completed exemption forms at the Saint Louis County Department of Public Health’s 3 clinics; completion of these forms is mandated.
Included in the revised questionnaire only.
Approximately half of respondents (53.6%; n = 637) indicated that their child had received at least 1 vaccine, with diphtheria, tetanus, and pertussis being the most common (66.6%; n = 424) and human papillomavirus being the least common (7.7%; n = 49). Among parents, 61% (184 of 300) reported that if DPH stopped providing nonmedical exemptions, they would go to a different health department instead of vaccinating their child.
On the revised questionnaire, of the 181 parents who responded to the statement “Children get more vaccines than are good for them,” the largest proportion (43.1%; n = 78) strongly agreed. Similarly, of the 167 parents who responded to the statement “It is better for children to get fewer vaccines at the same time,” the largest proportion (44.9%; n = 75) strongly agreed (Figure 1). A large proportion of respondents were extremely concerned about the serious side effects of routine childhood vaccines immediately after or within 1 or 2 days of receiving them (117 of 170; 68.8%), the long-term safety of vaccines (105 of 169; 62.1%), and vaccine effectiveness (77 of 158; 48.7%) (Figure 2).
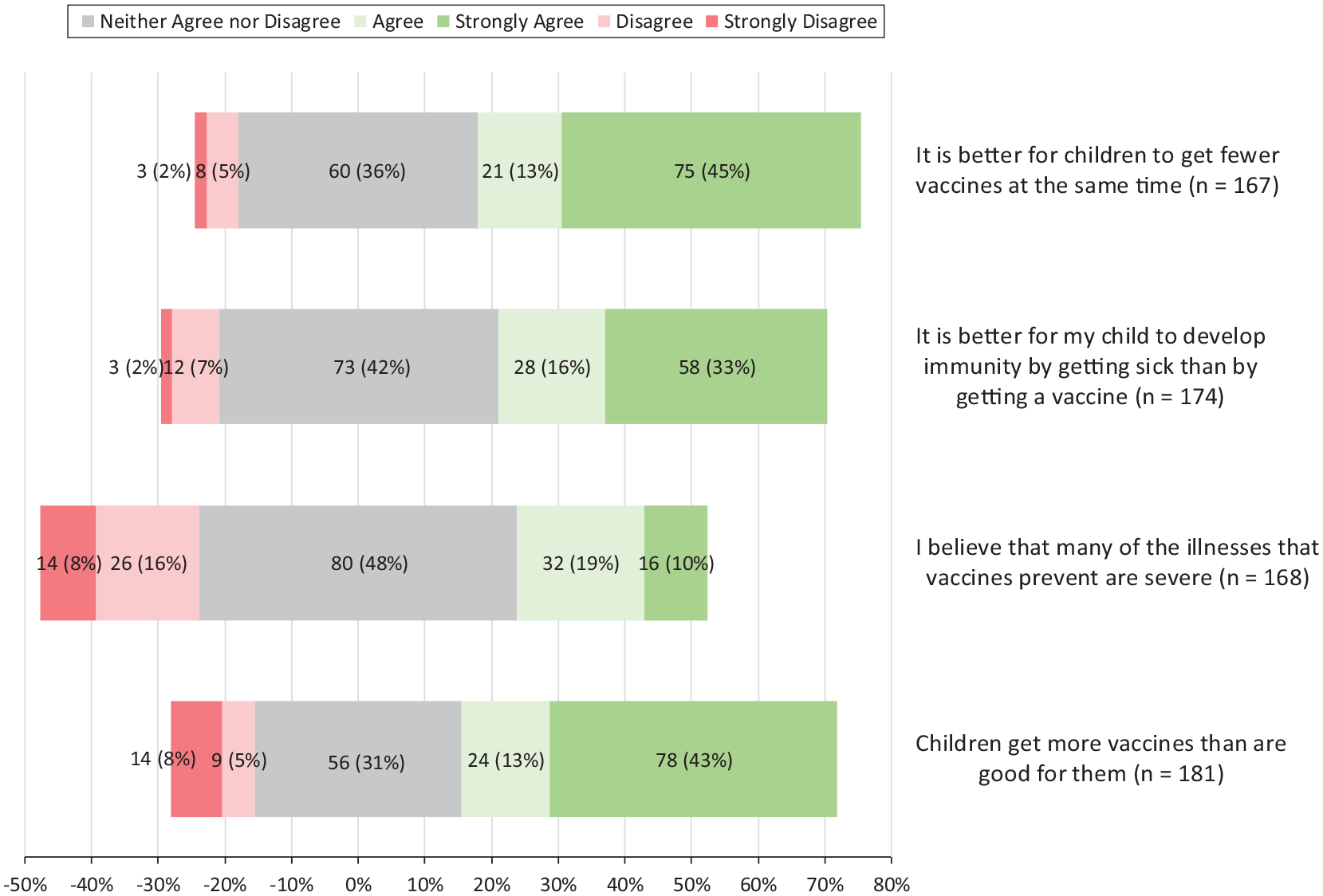
Opinions on vaccinations among those seeking nonmedical exemptions through the Saint Louis County Department of Public Health, St Louis County, Missouri, July through December 2022. Respondents completed voluntary questionnaires that indicated their levels of agreement with statements on vaccines, their effectiveness, and their safety.
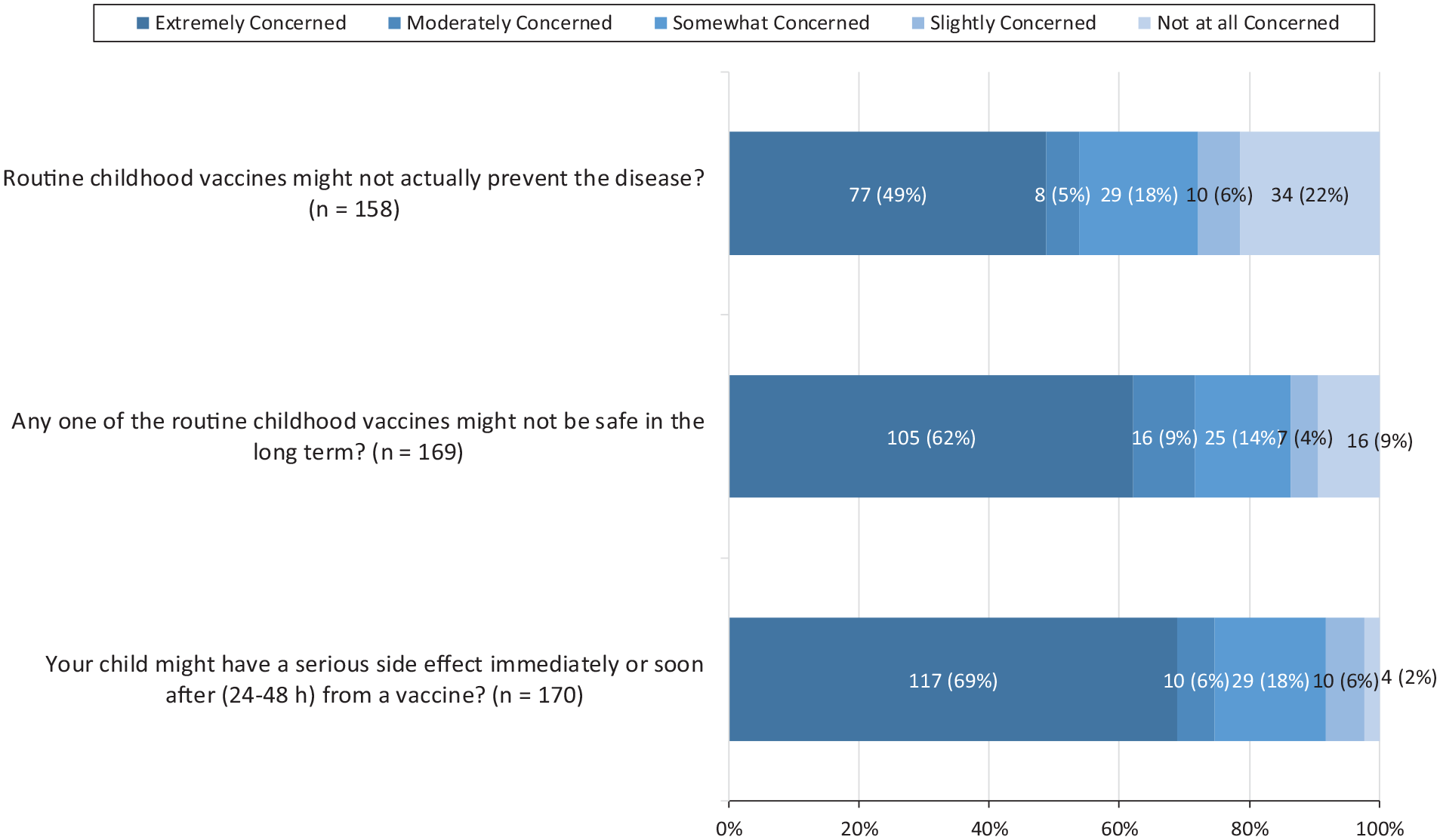
Levels of concern reported by parents seeking nonmedical exemptions through the Saint Louis County Department of Public Health, St Louis County, Missouri, July 2022 through December 2022. Respondents completed voluntary questionnaires that ranked their levels of concern about vaccines, their effectiveness, and their safety.
School Nurse Focus Groups
Findings from the school nurse focus groups identified 4 major themes: recent changes in vaccine compliance, vaccine hesitancy and barriers, services addressing hesitancy and barriers, and future requests for DPH.
Vaccine compliance changed over time and among districts and students but not by vaccine. Most nurses stated that students were typically fully compliant or had few or no vaccines completed. Some nurses reported greater compliance among elementary school students than among high school students in obtaining their age-appropriate required vaccines. Most nurses noted an increase in vaccine exemptions during the 2022-2023 school year relative to prior years. Some nurses noticed that parents of some previously compliant students began asking for exemptions after the COVID-19 pandemic.
I’ve seen a little bit more of religious exemptions, or kids that were . . . well on their way through all those required vaccines, and then they just stopped partway through the pandemic. And then parents were like, “Well, we’re going to get a religious exemption for the rest of them.”
Nurses from larger public school districts reported receiving a great deal of support for enforcing compliance from school administrators: [R]eally the only time my administrators . . . are involved in those [vaccine] conversations [is] when it comes to exclusions. Otherwise, they just kind of leave it to me to figure out what needs to get done, when it needs to get done.
Nurses from smaller districts described some administrative support for enforcing compliance, but their administrations were more lenient in allowing noncompliant students to continue attending school. One nurse from a private school described being frequently overruled by the school pastor about health-related education and policy.
Most nurses reported not keeping blank exemption cards on hand. Nurses who have blank exemption cards on hand do not publicize their availability; they offer them only upon request. Every nurse but one said that making the exemption cards harder to obtain led to parents vaccinating their child.
Nurses identified numerous socioeconomic barriers to obtaining vaccinations among families, including lack of transportation, vaccine cost, limited supply of vaccines at public health clinics, parents’ inability to take time off work for appointments, unstable housing, and immigration and language barriers.
A shortage of available pediatricians’ appointment slots was noted as a barrier, as was some pediatricians’ practice of not providing all recommended vaccines during a single office visit. Some nurses expressed feeling undermined by pediatricians who contradicted their guidance.
Nurses noted that misinformation from unreputable internet sources and peers has become a greater barrier since the COVID-19 pandemic. Nurses attempted to counter this barrier by educating parents about vaccination via mass email, telephone calls, and text messages but reported few responses.
School nurses have developed multiple ways to overcome vaccine hesitancy and barriers. To address barriers, schools used social workers to provide transportation to appointments, held special registration days with interpreters available for families with limited English proficiency, and notified parents in the spring about vaccines due in the fall. One high school withheld the parking passes of seniors until they submitted vaccination records. Nurses had mixed experiences with on-site vaccine clinics. Only some school districts saw a need for them, and those who used them reported results ranging from total success to “not worth the effort” to complete failure.
School nurses felt that DPH could help by providing DPH clinic information to school nurses, assisting with school vaccine clinics, extending DPH vaccine clinic hours, creating mobile-friendly messaging and printable fliers, and holding vaccination clinics at local libraries.
Pediatrician Interviews
Findings from the pediatrician interviews revealed themes relating to vaccine information, community efforts, and physician decision-making. Pediatricians identified multiple resources that they used for vaccine information. All pediatricians identified the Centers for Disease Control and Prevention (CDC), the American Academy of Pediatrics, or UpToDate as trustworthy sources for vaccine information. Several participants intentionally avoided mentioning CDC when speaking with families, with 1 participant noting, “If I just say CDC, people put their guard up.”
Physicians identified other internet sources, social media, and pharmaceutical representatives as untrustworthy sources but noted that many parents and families believe the opposite, as observed in parent questionnaires and mentioned in the focus groups. Most participants remarked on the power of social media, with 1 mentioning, “I feel very weakened by social media.”
Most physicians believed that they play an important role in vaccination efforts. However, 2 of 8 participants did not view themselves as having a role in public health at all. One physician said, “There’s only so many patients I can serve. And frankly, I don’t have to serve everyone.”
Pediatricians mentioned other practices in the community working against vaccination efforts, with 4 pediatricians saying that chiropractors play an adverse role. Chiropractic influence was noted as being particularly strong due to the presence of a local chiropractic college. Some participants lamented that vaccination efforts were being undermined by physicians who exclude unvaccinated patients from their practices, driving patients toward chiropractors.
When asked about their decision to accept vaccine-hesitant patients into their practices, many physicians felt a sense of duty to care for unvaccinated children. One physician said, “I don’t feel like the child should suffer because of the parent’s choice.”
Participants frequently felt a responsibility to continue vaccination efforts, even after repeated refusals from families. One participant noted, “If all they’re hearing is what they’re Googling, then we’re never gonna make any progress. If I can get just a little bit of some information in there, with each visit, I think it helps a little bit.” Another participant said, “I’ll take one vaccine against no vaccines.”
However, several factors were reported as negatively influencing health care provider decisions to accept vaccine-hesitant patients into their practices. One participant expressed concern about the risk of exposing clinic staff, other patients, and their families to infectious diseases. One participant affiliated with a hospital system stated that accepting unvaccinated patients adversely affected their system’s quality care metrics, discouraging health care providers from working with vaccine-hesitant families. Physicians also identified time as a constraint, stating that short visit times limit their ability to establish trust with patients and families but longer visits caused them to see fewer patients. When working with parents who were perceived as being strongly antivaccine, a participant noted that time was especially precious, saying, “I don’t know how much time I should really—I would say waste, they might say spend—trying to change their mind.”
Lastly, reimbursement rates and health insurance coverage were concerns independently and as a cofactor to time. One participant remarked that vaccine-hesitant patients “fill up a lot of my schedule, and my reimbursement goes down because I’m taking the time spinning my wheels trying to educate these people.”
Discussion
One common theme in the vaccine hesitancy literature is the demographic characteristics of parents seeking nonmedical exemptions—typically White, college educated, and with high incomes. 16 Our study found similar results: parents wanting a nonmedical exemption typically were non-Hispanic White, had a bachelor’s degree or higher, and had an annual household income >$85 000. Another common theme in the literature is the time constraint on physicians to educate parents, even though taking the time to counsel has been shown to increase the likelihood of vaccination.3,17,18 Our physician interviews mirrored sentiments expressed in a study by Mohanty et al, 17 with several of our participants discussing the time required to educate and address vaccine concerns, as well as the emotional and financial cost, which are compounded when many patients are vaccine hesitant. Dinleyici et al 11 assert that the effect of disinformation surrounding the COVID-19 pandemic could increase future vaccine hesitancy. 11 While further research is needed to determine the effects of the COVID-19 pandemic on routine childhood vaccination, our school nurse participants reported that prior to the pandemic, children typically received either all or none of their required vaccinations, whereas after the pandemic, parents began opting for nonmedical exemptions for vaccine series that were already underway or opting out of some vaccines (eg, meningococcal conjugate vaccine) recommended only for older children.
One strength of this project was its multifaceted approach: we examined vaccine hesitancy from 3 very different perspectives. Misinformation was a unifying theme across all 3 perspectives. Most parents said that they received vaccine information from medical providers, but some cited social media, friends, family, or their own research as sources of their information. School nurses and pediatricians identified these as sources of misinformation that they encountered. Apart from the theme of misinformation, the 3 groups’ perspectives were distinct. The parent exemption forms and questionnaire described the population seeking exemptions, identified common pediatricians servicing this population, and provided parents’ reasons for not vaccinating. The semistructured focus groups with school nurses identified their methods for contacting and educating parents about their child’s vaccines and described the barriers to vaccination and the hesitancy trends that they observed. Finally, the physician interviews provided researchers with an understanding that some health care providers were named frequently, not necessarily because they had antivaccine sentiments themselves, but because few physicians in the St Louis metropolitan area are willing to accept unvaccinated or vaccine-hesitant patients. Those physicians have become well-known in the vaccine-hesitant population of St Louis, drawing more hesitant families into their practices. Pediatricians discussed their ethical dilemma: excluding unvaccinated or vaccine-hesitant patients from their practices limits access to care and could drive patients toward chiropractors and/or holistic practitioners. However, accepting and continuing to engage them risks exposing other patients to infectious diseases and reduces the overall number of patients that a health care provider can see.
Limitations
Our study had several limitations. First, the distribution of the voluntary questionnaires was not universally promoted despite it being a required systematic process, potentially skewing our results to appear stronger in 1 demographic group versus the true distribution. Additionally, the area served by the clinic that most faithfully distributed the questionnaire was likely not representative of the overall, more diverse St Louis County population. For example, our respondents were largely non-Hispanic White, educated, and living in regions of higher socioeconomic status. While some literature indicates that parents seeking exemptions skew toward this same population, we cannot know how representative our sample was relative to the county’s entire exemption-seeking population. 16 Second, a small sample of nurses and physicians participated in our project. This small sample may not be representative of all St Louis County school nurses or health care providers. Several nurses came from a single district, and most districts and private schools did not participate. We were not able to estimate the proportion of school nurses who were reached by our invitation to participate in the focus groups. We reached out to all 23 public school district lead nurses, but it was unclear how many of them distributed the message to their individual nurses. For private schools, we did not know how many schools had a nurse, so estimating our reach was not possible. Third, the physician most frequently cited (10% of the time) by parents completing exemption questionnaires declined to participate in our project. Without this person—and a larger sample of physicians—we could not evaluate how representative our participants were with respect to local medical practitioners. Fourth, our study may have been subject to recall or reporting bias because of parents self-reporting information on the exemption forms and questionnaires. Fifth, school nurses who participated in focus groups were part of a DPH distribution list and may have worked with members of DPH during the pandemic. These nurses may have had different viewpoints than nurses who have not previously interacted with DPH. Additionally, we did not test intercoder reliability before beginning the coding process. Reflexivity was limited to weekly meetings and discussions that took place after the interviews and focus groups; it was not practiced through individual journaling.
Conclusions
This project highlights the need for a multidisciplinary approach to address vaccine hesitancy. A systematic review observed that state exemption rates seemed to be correlated with the ease with which exemptions could be obtained: the simpler the nonmedical exemption process, the higher the exemption rates, and vice versa. 16 Because of the simplicity of the nonmedical exemption process in Missouri, if DPH were to stop providing exemption cards, parents would likely find other avenues to obtain them. We recommend that local health departments facilitate discussions with their front-line partners (ie, school nurses and pediatricians) to learn how they could help reduce vaccine hesitancy. DPH plans to collect district- or school-level immunization data for St Louis County to assess trends over time and identify schools that may need additional resources, particularly schools whose nurses were not included in the convenience sample for this study. While our results may not be generalizable to all jurisdictions (eg, those with stricter nonmedical exemption processes), partnering with school nurses and/or pediatricians can benefit all parties, as stated in a policy statement by Kuo et al. 19 To cultivate its relationship with child-health partners, DPH used sentiments from this project to create a school nurse liaison to disperse educational material on childhood vaccines and information about DPH’s vaccine clinics for parents, schools, and pediatricians. This position has strengthened DPH’s relationship with school nurses and, hopefully, pediatricians and parents. Future interventions need to focus on beliefs and behavioral change surrounding vaccines and not just the economics and accessibility of vaccines.
Supplemental Material
sj-docx-1-phr-10.1177_00333549241297685 – Supplemental material for Perspectives of Parents, School Nurses, and Pediatricians on Vaccine Hesitancy in St Louis County, Missouri
Supplemental material, sj-docx-1-phr-10.1177_00333549241297685 for Perspectives of Parents, School Nurses, and Pediatricians on Vaccine Hesitancy in St Louis County, Missouri by Jennifer Bradshaw, Amanda Brzozowski, Priya Katti, Olivia Chapman, Audrey Pham, Andrew Torgerson, Ethan Wankum, Aimee Snavely and Carole R. Baskin in Public Health Reports®
Footnotes
Acknowledgements
The authors thank the parents, school nurses, and pediatricians for participating in this project.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Saint Louis University Peiper and Wang Institute for Vaccine Science and Policy Collaborative Fund.
Supplemental Material
Supplemental material for this article is available online. The authors have provided these supplemental materials to give readers additional information about their work. These materials have not been edited or formatted by Public Health Reports’s scientific editors and, thus, may not conform to the guidelines of the AMA Manual of Style, 11th Edition.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.