
Abstract
Objectives:
Studies have demonstrated that people with disabilities are more likely to use cannabis than people without disabilities. However, less is known about novel forms of use, such as cannabis vaping, in this population. We examined the correlates of cannabis vaping among people with disabilities and the association between cannabis vaping and the frequency of cannabis use in any form.
Methods:
We used data from the 2022 Behavioral Risk Factor Surveillance System to examine the association between disabilities and past-month cannabis vaping, as well as the number of days that cannabis was used in the past month, among US adults. We used weighted multivariable logistic and modified Poisson regression models with incidence rate ratios to examine the associations.
Results:
The prevalence of cannabis vaping was higher among adults with any disability (4.6%) than among adults without disabilities (2.8%); adults with only cognitive disabilities had the highest prevalence (8.2%). Daily nicotine vaping (adjusted odds ratio [AOR] = 6.04; 95% CI, 4.14-8.80), former cigarette smoking status (AOR = 1.67; 95% CI, 1.25-2.25), and being aged 18-24 years (vs ≥65 y) (AOR = 11.07; 95% CI, 7.05-17.38) were associated with higher odds of cannabis vaping among adults with any disability. Disability status modified the relationship between cigarette smoking and cannabis vaping (P < .001). Additionally, among adults with disabilities, the rate of cannabis-use days was higher among adults who vaped cannabis (adjusted incidence rate ratio = 1.28; 95% CI, 1.19-1.36) than among adults who did not vape cannabis.
Conclusions:
Among adults with disabilities, nicotine consumption by vaping was associated with cannabis vaping. Our findings highlight the need for interventions that reduce the risk of polysubstance use (ie, nicotine and cannabis) in this population.
Cannabis is one of the most commonly used substances among adults in the United States1-3 and has seen a substantial shift in public perception and legal status during the past 2 decades.4-6 As of May 2024, in the United States, >24 states and the District of Columbia had legalized adult recreational and medical cannabis use, while 14 states had legalized only medical cannabis use.4-8 The legalization of cannabis and more positive attitudes toward cannabis have been linked to cannabis use.9-12 These trends, along with cannabis legalization, coincide with the rise of electronic nicotine delivery systems, 13 growing interest in cannabis for therapeutic and recreational purposes, and an increasing prevalence of depressive disorders, which are associated with cannabis use in the United States.14-16
The main psychoactive component of cannabis, tetrahydrocannabinol (THC), can be administered through various routes. 17 Studies show that smoking and vaporized routes exert more rapid albeit shorter effects than oral routes.18,19 While cannabis has been shown to have health benefits, such as pain and anxiety relief,20-22 it can have a negative effect on short-term memory and could be a gateway to the use of other substances.23-25 Also, the co-use of THCs with nicotine can heighten the intoxicating properties of both substances when inhaled.26,27 Additionally, cannabis vaping is especially notable in its link with lung injury associated with the use of electronic cigarettes (e-cigarettes) or vaping, 28 although vitamin E acetate was eventually identified as one of the causal agents, 28 thus highlighting the potential harm of unsupervised vaporized cannabis consumption.
The prevalence of cannabis use among adults with disabilities is higher than among adults without disabilities,29-33 emphasizing the need to understand the nuances of this trend, specifically the use of vaping as an emerging route of administration among cannabis consumers. Disability can be defined as the consequence of complex interactions between environmental factors and personal or health conditions that preclude full social and functional participation in daily activities and the community.34-36 This concept of disability is multifaceted, extending beyond medical conditions (ie, visual or hearing impairments) to include psychosocial factors that influence the experience of disability. 35 People with disabilities experience barriers to opportunities that enhance the quality of life, and they are susceptible to lifestyles and behaviors with the potential for negative health effects. 37 Thus, research and surveillance are important to support evidence-based interventions in this population. For example, adults with disabilities, particularly those with visual, cognitive, or physical disabilities, have higher odds of cannabis use than adults without disabilities.30-33 This heightened use is partly attributed to the medical use of cannabis, whereby individuals with disabilities might seek relief from chronic conditions and pain,20-22 highlighting a shift toward acceptance of cannabis as a therapeutic option. Also, the perception that cannabis may be less addictive than other drugs with high potential for abuse, such as opioids for relieving chronic pain, particularly in adults with disabilities, has been explored in several studies and might support reasons for cannabis use.38-42 Thus, if cannabis is considered by many as a safer alternative to opioids with a lower potential for dependency, 38 this belief might encourage the use of cannabis rather than opioids to manage chronic pain in this population.39,42
Furthermore, the relationship among cannabis vaping, conventional cigarettes, and nicotine e-cigarette use sheds light on changing consumption patterns.23,43,44 Adults who vape nicotine e-cigarettes are more likely to engage in cannabis vaping than those who do not vape nicotine,23,43 suggesting a crossover in vaping behaviors. 45 This trend underscores the importance of considering the broader implications of vaping technologies and their effect on public health, especially among socially and medically vulnerable populations such as people with disabilities. In addition, given that nicotine vaping can facilitate increased use of nicotine, 46 less is known about how cannabis vaping might affect the frequency of cannabis use generally regardless of administration routes (ie, smoking, eating, dabbing). Exploring the associations among cannabis vaping, past-month frequency of cannabis use in all forms, and the potential influence of disability can offer insights into the vaping dynamics of people with disabilities. Furthermore, identifying modifying factors can inform targeted interventions and policies that are inclusive and sensitive to the unique needs of this population.
This study had 3 objectives: (1) identify the prevalence of cannabis vaping among adults by disability type; (2) investigate the correlates of cannabis vaping, stratified by disability status; and (3) examine the association between cannabis vaping and frequency of past-month cannabis use across all forms of consumption (ie, smoking, eating, dabbing) and explore the effect of disability on this relationship.
Methods
We obtained study data from the 2022 Behavioral Risk Factor Surveillance System (BRFSS), an annual US survey conducted by the Centers for Disease Control and Prevention. 47 The survey collects information on chronic disease conditions, risk behaviors related to health, and the use of preventive health services. The unweighted raw sample collected in 2022 among adults aged ≥18 years was 445 132, and the overall survey response rate was 45%. The question on cannabis use and vaping appeared in the optional module section of the BRFSS survey. Our analyses focused on the 18 jurisdictions (states and territories) that provided data on cannabis use in 2022. 47 These jurisdictions and their legal status of medical and/or recreational cannabis as of November 2022 are noted with the study’s dependent, independent, and covariate variables and response options (Table 1). The University of Nevada, Reno, exempted this study from institutional review board review because we used deidentified publicly available data.
Description of study measures from the BRFSS 2022 US adult dataset a
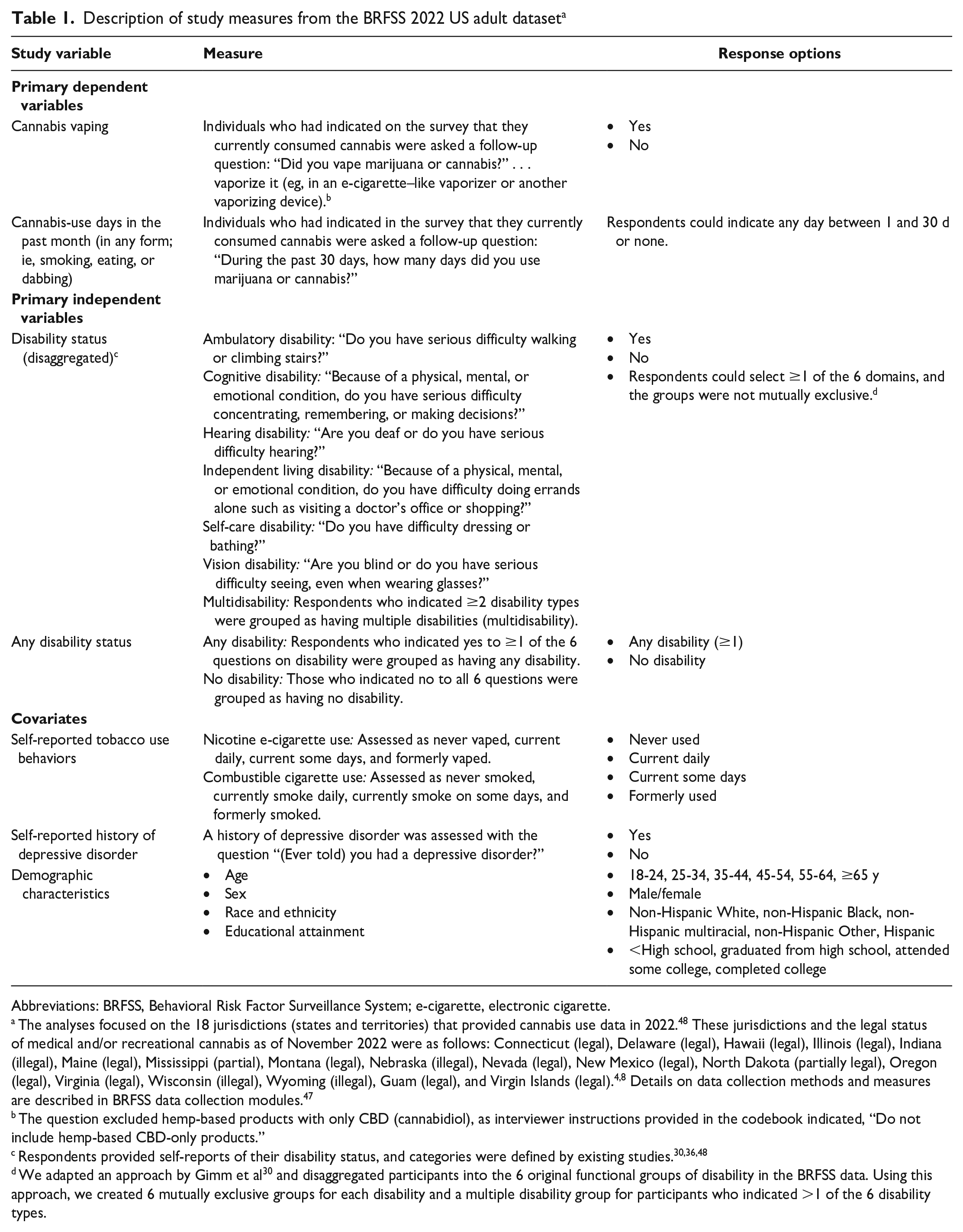
Abbreviations: BRFSS, Behavioral Risk Factor Surveillance System; e-cigarette, electronic cigarette.
The analyses focused on the 18 jurisdictions (states and territories) that provided cannabis use data in 2022. 48 These jurisdictions and the legal status of medical and/or recreational cannabis as of November 2022 were as follows: Connecticut (legal), Delaware (legal), Hawaii (legal), Illinois (legal), Indiana (illegal), Maine (legal), Mississippi (partial), Montana (legal), Nebraska (illegal), Nevada (legal), New Mexico (legal), North Dakota (partially legal), Oregon (legal), Virginia (legal), Wisconsin (illegal), Wyoming (illegal), Guam (legal), and Virgin Islands (legal).4,8 Details on data collection methods and measures are described in BRFSS data collection modules. 47
The question excluded hemp-based products with only CBD (cannabidiol), as interviewer instructions provided in the codebook indicated, “Do not include hemp-based CBD-only products.”
Respondents provided self-reports of their disability status, and categories were defined by existing studies.30,36,48
We adapted an approach by Gimm et al 30 and disaggregated participants into the 6 original functional groups of disability in the BRFSS data. Using this approach, we created 6 mutually exclusive groups for each disability and a multiple disability group for participants who indicated >1 of the 6 disability types.
Statistical Analysis
We used a descriptive analysis with frequencies and weighted percentages to describe the characteristics of the analytic sample. We determined the prevalence of cannabis vaping and grouped cannabis vaping by respondent characteristics with 95% CIs. We used the Pearson χ2 test to determine the bivariate association between respondent characteristics and cannabis vaping. We used multivariable logistic regression models, stratified by disability status (any disability vs no disability), to identify the correlates of cannabis vaping (dependent variable) among people with disabilities and without disabilities, adjusting for depressive disorder, tobacco product use (cigarettes and nicotine e-cigarettes), and demographic characteristics (age, sex, race, and education). We selected the independent variables based on current evidence of their link with cannabis vaping.27,43,45 We used a separate multivariable logistic regression model to examine the association between cannabis vaping (independent variable) across 6 disaggregated categories of disability30,36,48 and cannabis vaping, adjusting for depressive disorder, tobacco product use (cigarettes and nicotine e-cigarettes), and demographic characteristics (age, sex, race, and education).
We used modified Poisson regression models to obtain the incidence rate ratios for the number of days that cannabis was used in the past month (dependent variable) among cannabis vapers as compared with non–cannabis vapers (primary independent variable). We also investigated the modifying role of disability on the relationship by stratifying the models by disability status (any disability and no disability). We adjusted for depressive disorder, tobacco product use, and demographic characteristics in both models. We weighted all analyses to account for the complex survey design methods. We used listwise deletion to handle missing data, assuming that data were missing completely at random. The rate of missingness was <5% for all variables. We considered P < .05 to be significant. We analyzed data using Stata version 18.0 (StataCorp).
Results
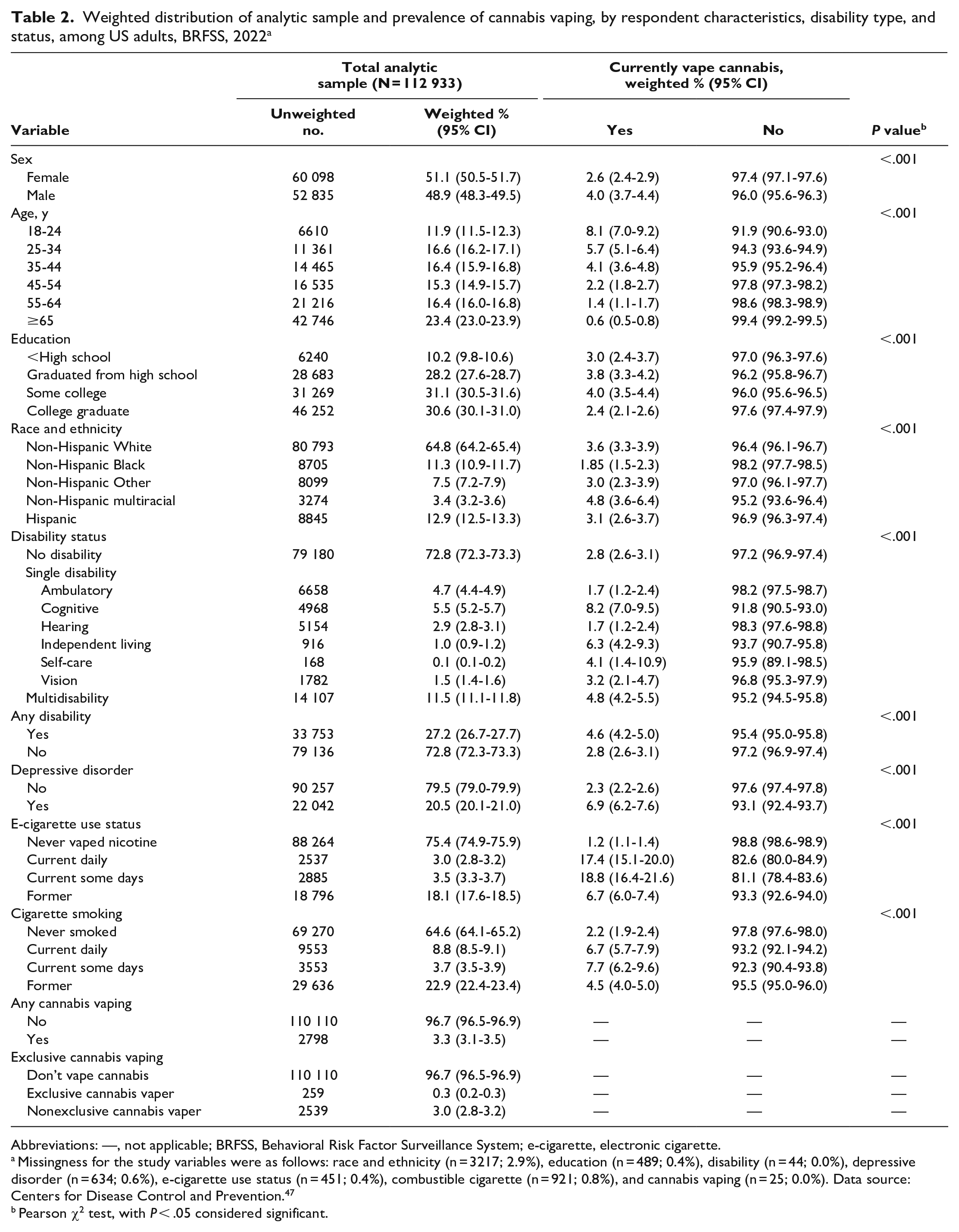
The analytic sample of our study comprised adults from 18 US states and territories and included questions on cannabis use in the optional module of the 2022 BRFSS dataset (N = 112 933). Most participants were female (51.1%; 95% CI, 50.5%-51.7%) and non-Hispanic White (64.8%; 95% CI, 64.2%-65.4%), and nearly one-quarter of adult participants were aged ≥65 years (23.4%; 95% CI, 23.0%-23.9%). More than one-quarter of participants (27.2%; 95% CI, 26.7%-27.7%) reported ≥1 disability. Of the 6 disaggregated disability categories, most participants had a cognitive disability only (5.5%; 95% CI, 5.2%-5.7%), but overall most participants reported multiple disabilities (11.5%; 95% CI, 11.1%-11.8%). Of all respondents, 0.3% (95% CI, 0.2%-0.3%) vaped cannabis exclusively and did not use it in any other form, while 3.0% (95% CI, 2.8%-3.2%) vaped cannabis along with other routes of consumption (ie, smoking, eating, dabbing) (Table 2).
Weighted distribution of analytic sample and prevalence of cannabis vaping, by respondent characteristics, disability type, and status, among US adults, BRFSS, 2022 a
Abbreviations: —, not applicable; BRFSS, Behavioral Risk Factor Surveillance System; e-cigarette, electronic cigarette.
Missingness for the study variables were as follows: race and ethnicity (n = 3217; 2.9%), education (n = 489; 0.4%), disability (n = 44; 0.0%), depressive disorder (n = 634; 0.6%), e-cigarette use status (n = 451; 0.4%), combustible cigarette (n = 921; 0.8%), and cannabis vaping (n = 25; 0.0%). Data source: Centers for Disease Control and Prevention. 47
Pearson χ2 test, with P < .05 considered significant.
Prevalence of Cannabis Vaping by Respondent Characteristics
Participants with only cognitive disabilities (8.2%; 95% CI, 7.0%-9.5%), only independent living disabilities (6.3%; 95% CI, 4.2%-9.3%), and multiple disabilities (4.8%; 95% CI, 4.2%-5.5%) had the highest proportion of cannabis vaping (Table 2). The prevalence of cannabis vaping was significantly higher among people with any disability (4.6%; 95% CI, 4.2%-5.0%) than among people with no disability (2.8%; 95% CI, 2.6%-3.1%). A higher prevalence of people who currently smoke combustible cigarettes daily (6.7%; 95% CI, 5.7%-7.9%) and some days (7.7%; 95% CI, 6.2%-9.6%) vaped cannabis as compared with those who have never smoked cigarettes (2.2%; 95% CI, 1.9%-2.4%). Likewise, the prevalence of cannabis vaping was higher among people who vaped nicotine daily (17.4%; 95% CI, 15.1%-20.0%) and some days (18.8%; 95% CI, 16.4%-21.6%) as compared with never (1.2%; 95% CI, 1.1%-1.4%).
Correlates of Cannabis Vaping Among Adults, Stratified by Disability Status
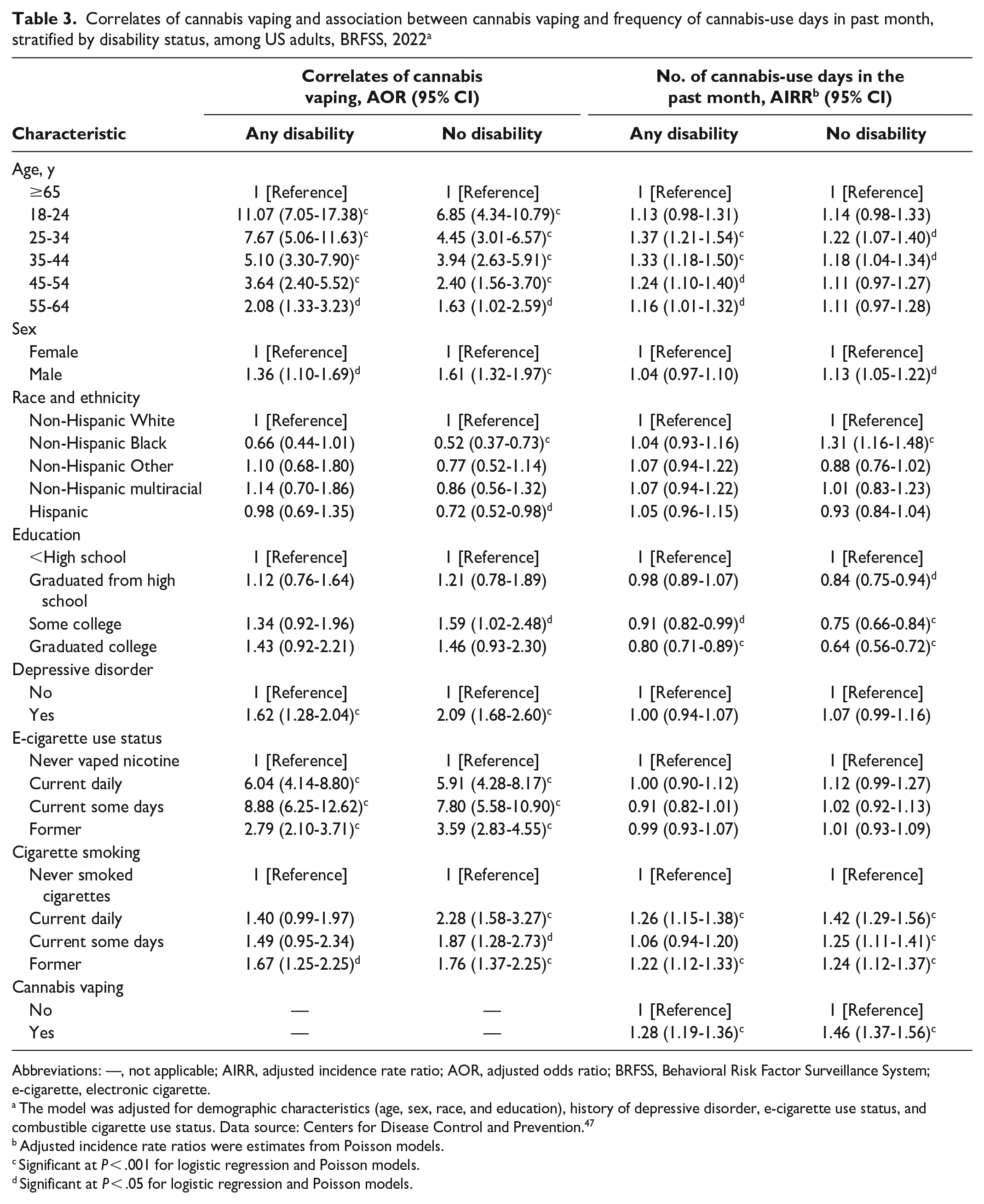
Among people with any disability, the odds of cannabis vaping were significantly higher among adults aged 18-24 years (vs ≥65 y) (adjusted odds ratio [AOR] = 11.07; 95% CI, 7.05-17.38), male (vs female) (AOR = 1.36; 95% CI, 1.10-1.69), and people with a history of depressive disorder (vs no history) (AOR = 1.62; 95% CI, 1.28-2.04) (Table 3). Also, among adults with disabilities, those who vaped nicotine daily (AOR = 6.04; 95% CI, 4.14-8.80), some days (AOR = 8.88; 95% CI, 6.25-12.62), and formerly (AOR = 2.79; 95% CI, 2.10-3.71) had significantly higher odds of vaping cannabis than those who had never vaped nicotine. Only those who were former cigarette smokers had significantly higher odds of cannabis vaping (AOR = 1.67; 95% CI, 1.25-2.25). Among people without disabilities, people who smoked cigarettes daily (AOR = 2.28; 95% CI, 1.58-3.27) and some days (AOR = 1.87; 95% CI, 1.28-2.73) had significantly higher odds of cannabis vaping than those who had never smoked cigarettes. Furthermore, our interaction model showed that disability modified the effect of cigarette smoking on cannabis vaping (P < .001).
Correlates of cannabis vaping and association between cannabis vaping and frequency of cannabis-use days in past month, stratified by disability status, among US adults, BRFSS, 2022 a
Abbreviations: —, not applicable; AIRR, adjusted incidence rate ratio; AOR, adjusted odds ratio; BRFSS, Behavioral Risk Factor Surveillance System; e-cigarette, electronic cigarette.
The model was adjusted for demographic characteristics (age, sex, race, and education), history of depressive disorder, e-cigarette use status, and combustible cigarette use status. Data source: Centers for Disease Control and Prevention. 47
Adjusted incidence rate ratios were estimates from Poisson models.
Significant at P < .001 for logistic regression and Poisson models.
Significant at P < .05 for logistic regression and Poisson models.
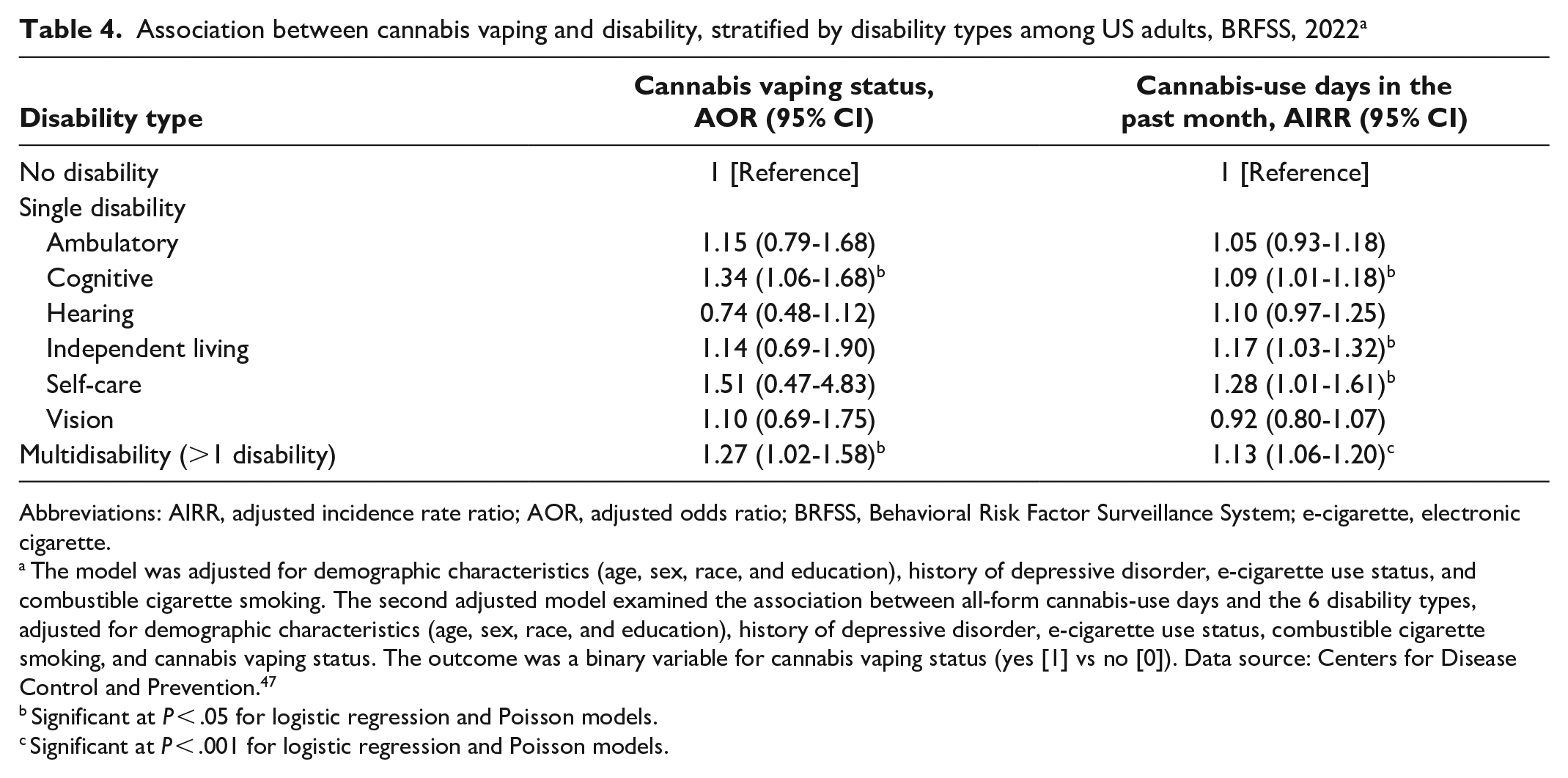
When we examined the relationship between cannabis vaping and the 6 disaggregated disability subtypes, we found that people with only cognitive disabilities (AOR = 1.34; 95% CI, 1.06-1.68) and people with multiple disabilities (AOR = 1.27; 95% CI, 1.02-1.58) had significantly increased odds of cannabis vaping than those with no disabilities, after adjusting for demographic characteristics, depressive disorder, e-cigarette use, and combustible cigarette use (Table 4).
Association between cannabis vaping and disability, stratified by disability types among US adults, BRFSS, 2022 a
Abbreviations: AIRR, adjusted incidence rate ratio; AOR, adjusted odds ratio; BRFSS, Behavioral Risk Factor Surveillance System; e-cigarette, electronic cigarette.
The model was adjusted for demographic characteristics (age, sex, race, and education), history of depressive disorder, e-cigarette use status, and combustible cigarette smoking. The second adjusted model examined the association between all-form cannabis-use days and the 6 disability types, adjusted for demographic characteristics (age, sex, race, and education), history of depressive disorder, e-cigarette use status, combustible cigarette smoking, and cannabis vaping status. The outcome was a binary variable for cannabis vaping status (yes [1] vs no [0]). Data source: Centers for Disease Control and Prevention. 47
Significant at P < .05 for logistic regression and Poisson models.
Significant at P < .001 for logistic regression and Poisson models.
Association Between Cannabis Vaping and Frequency of Cannabis-Use Days in the Past Month, Stratified by Disability
Cannabis was used on more days in the past month among people with disabilities who vaped cannabis along with other routes of use (mean [SD] = 22 [10] d) than among people without disabilities who vaped cannabis (20 [11] d) (Figure). Furthermore, among participants with a disability who vaped cannabis, there was a 28% (95% CI, 1.19-1.36) increase in the rate of cannabis-use days as compared with non–cannabis vapers (Table 3). For adults without disabilities who vaped cannabis, we found a 46% (95% CI, 1.37-1.56) increase in the rate of cannabis-use days as compared with people without disabilities who did not vape cannabis (Table 3).
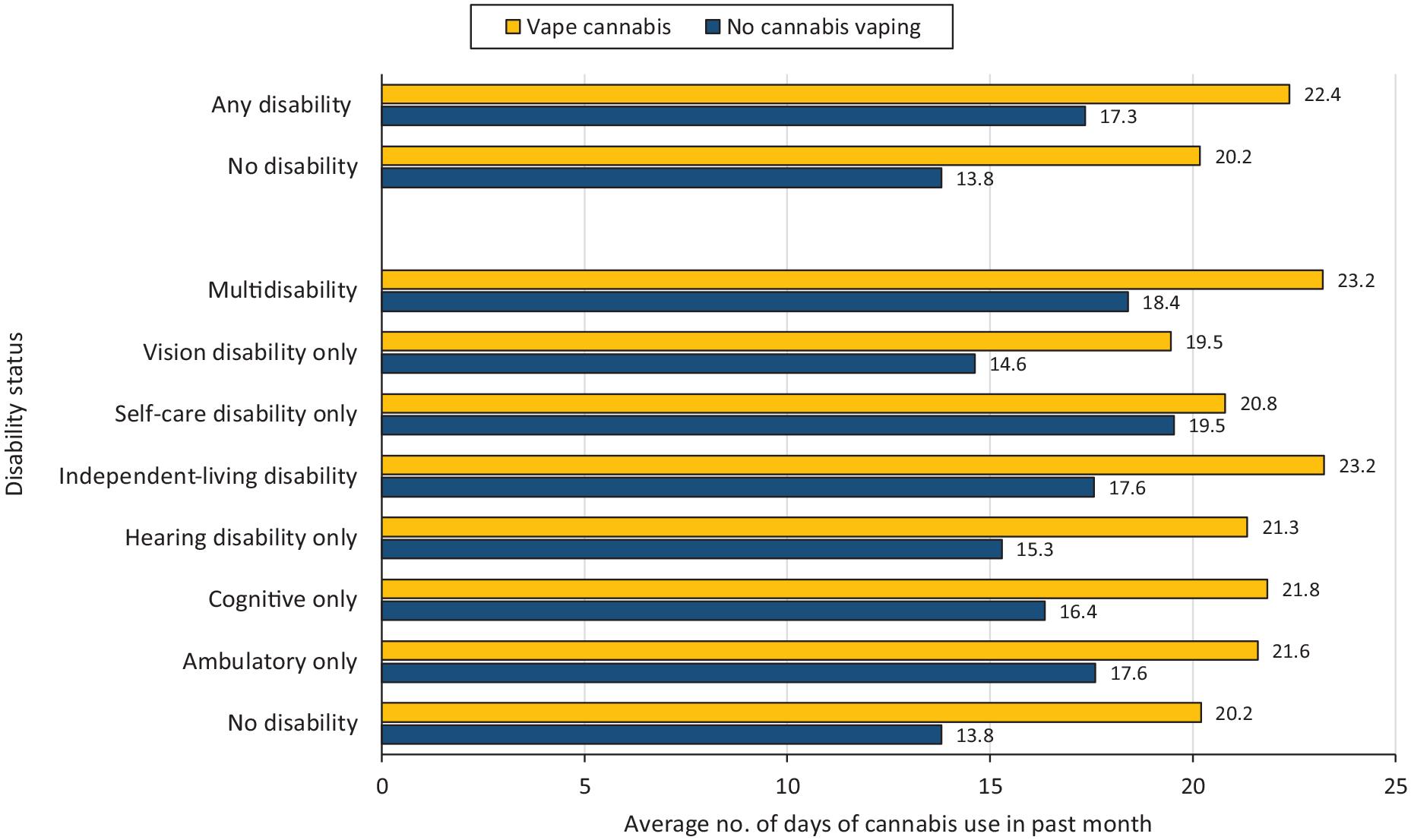
Average cannabis-use days in any form in the past month among US adults in 2022, stratified by disability type and status. Cannabis-use days ranged from 1 to 30.
When we examined the association between past-month cannabis-use days and the 6 disaggregated disability types, respondents with only cognitive disabilities (adjusted incidence rate ratio [AIRR] = 1.09; 95% CI, 1.01-1.18), only self-care disabilities (AIRR = 1.28; 95% CI, 1.01-1.61), only independent living disabilities (AIRR = 1.17; 95% CI, 1.03-1.33), and multiple disabilities (AIRR = 1.13; 95% CI, 1.06-1.20) had higher rates of all-form cannabis-use days than people with no disabilities.
Discussion
The findings from this study suggest that the prevalence of cannabis vaping is higher among adults with disabilities than among adults without disabilities and that adults with cognitive disabilities account for the highest prevalence of cannabis vaping in this population. In addition, we found that younger age (18-24 y), a history of depressive disorders, and daily and some-days nicotine vaping were associated with cannabis vaping among adults with disabilities, although the presence of a disability modified the relationship between cigarette smoking and cannabis vaping. Furthermore, on average, people with disabilities consumed cannabis on more days than those without disabilities, and overall the frequency of cannabis-use days in the past month was higher for people who vaped cannabis than for people who used cannabis in other forms (ie, smoking, eating, dabbing) except vaping. These findings underscore the need for clinical and regulatory efforts that prioritize screening adults with disabilities for cannabis vaping, particularly those with cognitive disabilities, with tailored guidelines that address risk factors such as younger age, depressive disorders, and nicotine vaping.
The findings from this study of a higher prevalence of cannabis vaping among adults with disabilities is consistent with prior studies that found that people with disabilities are more likely to consume cannabis than people without disabilities.30-33 To our knowledge, our study is the first to examine cannabis vaping among adults with disabilities in a US sample and build on prior knowledge of cannabis consumption patterns among adults with disabilities.30-33 Specifically, people with cognitive disabilities only and those with multiple disabilities had the highest proportions of cannabis vaping and higher odds of cannabis vaping than those with no disabilities. These findings showing that people with disabilities have a higher prevalence of cannabis consumption than those without disabilities might be explained by the growing interest in the use of cannabis for medical purposes in the disability community.38,39,49 Adults with disabilities who are more likely to experience health conditions such as chronic pain and sleep disorders that affect physical and cognitive well-being 50 might find the use of cannabis beneficial.51-53 In addition, a combination of other factors may account for these findings. For example, while adults with disabilities may use cannabis for medical purposes,20,21,29 young adults with disabilities who vape nicotine might also vape cannabis for experimental, recreational, and self-medication purposes, thus compounding uptake for cannabis in vaporized forms.27,54
Another important finding was that the odds of cannabis vaping were higher among those with depressive disorders than among those without depressive disorders,14,16 because these disorders are more prevalent among people with disabilities than among people without disabilities.30,31 This finding suggests that other underlying factors may contribute to increased depression and cannabis use among adults with disabilities. For example, environmental and social stressors, including limited access to social amenities (ie, transportation and recreational facilities) and barriers such as stigma or a lack of timely access to health care, may increase the use of cannabis to manage chronic pain. Overall, these findings highlight the need for comprehensive interventions that address environmental and psychosocial factors, ensuring that people with disabilities have optimal engagement with society and access to appropriate mental and physical health rehabilitation services. 36
The 2022 BRFSS data on cannabis vaping indicate that people who vape cannabis consume cannabis more frequently than those who do not vape but consume cannabis through other methods (eg, smoking, eating, dabbing). Among cannabis users, adults with disabilities consumed cannabis more frequently than those without disabilities, regardless of vaping status. Notably, similar to other studies,30,31,33 people with cognitive, self-care, independent living, and multiple disabilities reported higher cannabis-use days in the past month than nondisabled individuals. These findings underscore the need for targeted public health interventions to promote safe cannabis use and mitigate escalation to cannabis use disorder, particularly among people with disabilities, in jurisdictions where cannabis is legal. 4
Furthermore, as seen in studies among adults without disabilities,29,55,56 we found that men (vs women), non-Hispanic White people (vs people in racial and ethnic minority groups), people who vape nicotine (vs do not vape nicotine), and people with depressive disorders (vs without depressive disorders) had higher odds of vaping cannabis. These findings were consistent among people with disabilities. Our findings relating to the association between nicotine and cannabis vaping highlight the interconnected nature of psychoactive substances and the potential for common liability of substance use behaviors among populations with disabilities. 57
Limitations
Our study had several limitations. First, the data on cannabis vaping came from 18 states and territories instead of all 50 states, and, therefore, may not be generalizable to the overall US population. Second, the use of cross-sectional data precluded us from making any causal inferences about the measures examined. Third, we used BRFSS data, which rely on self-reports of cannabis and tobacco use without biochemically verified measures; as such, these data can be influenced by social desirability bias and may underestimate the prevalence of use behaviors. Nonetheless, self-report measures for drug use are reliable alternatives for biochemically verified drug use assessments in large population-level assessments. 58 Fourth, BRFSS data assess only noninstitutionalized adults and, therefore, exclude people with severe disabilities who may be institutionalized. 47 The BRFSS interviews do not collect responses by proxy, which may also underestimate findings among participants with sensory and cognitive impairments. However, computer-assisted telephone interview systems were used in 2022 and, as such, could mitigate barriers to responses from participants with disabilities.
Conclusion
These results highlight the need for targeted interventions to support the safe consumption of cannabis and reduce the risk of polysubstance use (nicotine and THCs). Health care providers should prioritize screening adults with cognitive disabilities for cannabis vaping and provide tailored interventions that target risk factors such as young age, depressive disorders, and nicotine vaping.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: O.O. is supported by the National Institute on Drug Abuse of the National Institutes of Health under award K01DA055127. W.L. is supported by the National Institute on Drug Abuse and the US Food and Drug Administration Center for Tobacco Products (U54DA036151). Z.B.T. is supported by the National Institute on Drug Abuse of the National Institutes of Health under award R03DA054417-02. The content of this article is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health and the US Food and Drug Administration Center for Tobacco Products.