
Abstract
Cannabis vaping has emerged as a predominant mode of cannabis use among United States (US) adolescents and young adults (AYA) primarily due to the popularity of modifiable designs of vaping devices coupled with changes in cannabis policies and increased availability of cannabinoid products. New methods for cannabis vaping by e-liquid/oil vaping, dry plant vaping, and cannabis concentrate vaping (ie, dabbing) have had high uptake among American youth with unclear long-term health implications. Issues with contamination, mislabeling, and expansion of the vaped cannabis market to include not only delta-9-tetrahydrocannabinol (delta-9-THC) and cannabidiol (CBD) but also delta-9-THC analogs (eg, delta-8 and delta-10) sold as hemp-derived “legal highs” further complicated this healthcare space. Recent research suggests that cannabis/THC vaping carries distinct and overlapping risks when compared to cannabis smoking and may be associated with greater risk for acute lung injuries, seizures, and acute psychiatric symptoms. Primary care clinicians providing care for AYA are in an ideal position to identify cannabis misuse and intervene early to address cannabis vaping. To improve public health outcomes, a need exists for pediatric clinicians to be educated about different ways/methods that youth are vaping cannabinoid products and associated risks related to cannabinoid vaping. Further, pediatric clinicians need to be trained how to effectively screen for and discuss cannabis vaping with their youth patients. In the current article, we present a clinically focused review of cannabis vaping among young people with 3 main aims to: (1) identify and describe the cannabis vaping products commonly used by American youth; (2) review the health correlates of youth cannabis vaping; and (3) discuss clinical considerations related to identifying and treating youth who vape cannabis.
Introduction
Broad changes in cannabis legislation over the past 25 years legalizing cannabis for medical and recreational use in the majority of US states has shifted cannabis use patterns and altered Americans’ perceptions related to its harms and benefits. 1 For young people, a vulnerable population with regard to adverse health outcomes related to cannabis exposure, cannabis remains one of the most commonly used drugs and the primary drug for which youth receive substance use disorder treatment.1 -3 In 2021, 38.6%, 22.0%, and 10.8% of US 12th, 10th, and 8th graders reported lifetime cannabis use. 4 Technological advances occurring within the context of expanding cannabis markets have led to the introduction of a number of novel cannabis-based products into the legal and illegal markets and resulted in several new methods of cannabis administration. These technological advances, coupled with greater acceptance of cannabis use, have significantly increased cannabis vaping use in youth and young adult populations. Among these new methods, vaping cannabis, defined as the consumption of cannabis through inhalation of vaporized/aerosolized cannabinoids, has increased significantly among US youth. Current prevalence data from 2021 show that approximately 2.9% of 8th-grade students, 8.4% of 10th-grade students, and 12.4% of 12th-grade students reported past-month cannabis vaping. 4 A recent meta-analysis of studies examining adolescent cannabis vaping prevalence rates in the US found that lifetime, past 12-month, and past 30-day cannabis vaping showed a 2-to-7-fold increase from 2013 to 2020. 5 For young adults, there has also been an increase in cannabis vaping. Survey data from the Monitoring the Futures study show that past-month cannabis vaping rates have doubled in US young adults between 2017 and 2021. 6 Current prevalence data from 2021 show that approximately 13.6%, 21.8%, and 13.0% of 19 to 20, 21 to 22, and 23 to 24 year-olds reported past-month cannabis vaping, respectively. 6
Over the past decade, vaping has quickly become one of the 2 most common methods of cannabis consumption among American youth (along with smoking). 7 Although, notably, most youth who vape cannabis also regularly consume the drug through other methods (eg, smoking cannabis and orally ingesting cannabis edibles). In addition, youth who vape cannabis engage in other drug use including vaping tobacco/nicotine, alcohol consumption, and also use other drugs at higher rates than non-cannabis vapers.8,9 The increase in youth cannabis vaping carries unknown long-term health implications for American youth. 10 Given growing evidence for adverse health outcomes related to adolescent-onset cannabis use via smoking and within the context of rising rates of youth vaping, it is of growing importance for clinicians who provide medical or psychiatric care to young people to know about vaping and novel cannabis-based products and understand how to screen for and address cannabis vaping in their patients.11,12 In the current article, we present a clinically focused review of cannabis vaping among young people with 3 main aims to: (1) identify and describe the cannabis vaping products commonly used by American youth; (2) review the health correlates of youth cannabis vaping; and (3) discuss clinical considerations related to identifying and treating youth who vape cannabis.
Clinical vignette
Ms. X, a 17-year-old female with a past psychiatric history of depression and anxiety, was brought to the emergency department (ED), accompanied by her sister and mother, with concerns for rapid heart rate, nausea, and chest tightness. She stated that a few hours ago, she took multiple puffs from a “THC cart(ridge)” she recently acquired from her dealer and developed the above symptoms approximately an hour after vaping with her friend. She reports that she did not know what was in the e-liquid but was told that it had “THC” in it and was disposable. She reported that she had used cannabis in the past but had never experienced these symptoms. In ED, the heart rate was 100 beats/minute, blood pressure was 138/79, and blood oxygen saturation was 99%. Medical workup examining troponin T levels, complete blood count, and basic metabolic profile were all within normal limits. A 12-lead echocardiogram (EKG) showed a normal sinus rhythm without tachycardia or ST-segment elevation or depression and no ectopy. Results of a urine drug screen were positive for delta-9-tetrahydrocannabinol (THC) but negative for other drugs. Based upon this evaluation, the patient was diagnosed with a panic attack precipitated by THC. The patient was monitored in the ED for a few hours. After the cardiac symptoms had resolved and the patient was asymptomatic, she was discharged home. Ms. X had a scheduled visit with her psychiatrist 3 weeks later. She reported to her psychiatrist that over the week and a half following the discharge from the ED, she experienced persistent panic symptoms and paranoia, described, in the patient’s words, as having the sense that someone was following her and experiencing a feeling of impending doom and fear that something might happen to her and “she will die.” She did not want to be alone and would not sleep or go to the bathroom alone. These symptoms gradually decreased over the next week and a half, and on the day of the appointment with the psychiatrist, the patient reported that her symptoms had improved significantly.
Vaping and Novel Cannabis-Based Products
Cannabis vaping is done through battery-operated electronic devices (like electronic cigarettes) or other inhalation devices/set-ups that heat and vaporize cannabinoids in either a liquid form (ie, e-liquid) or solid form (ie, wax), with the cannabis vapor then being inhaled through the mouth and into the lungs. 13 There are many electronic vaping devices on the market including disposable and reusable models, with reusable devices being able to be refilled by purchasing cannabis-containing cartridges (slang term “carts”) or refillable e-juice containers. The liquid that is vaporized in electronic vaping devices (e-liquid) can contain nicotine, flavorings, cannabinoids such as delta-9-tetrahydrocannabinol (delta-9-THC), delta-8-THC (sold at convenience stores and gas stations), and cannabidiol (CBD), along with flavorings and additives such as propylene glycol and vegetable glycerin. Cannabis vaping cartridges are also available in a variety of formulation ratio of cannabinoids, for example, 10:1 CBD:THC.
Recent epidemiological studies have revealed a substantial increase in delta-8-THC use resulting from a its recent increase in popularity among youth as a vaping substrate. 14 Delta-8-THC is a naturally occurring chemical analog of delta-9-THC which is found in the cannabis plant but at substantially lower concentrations than delta-9-THC. Delta-8 THC is typically manufactured from hemp-derived CBD by a chemical process and has psychoactive and intoxicating effects, similar to delta-9 THC. Delta-8-THC for vaping is often sold in existing hemp marketing networks and these compounds are labeled as hemp products, which mislead consumers about its psychoactive potential. 15
Cannabis vape devices sold in marijuana dispensaries and at smoke shops should have the content and quantity of cannabinoids and other ingredients contained in the e-liquid listed on the label. However, contamination and mislabeling remain a problem, making it difficult for the physician to know what a patient is consuming. Additionally, disposable electronic vaping devices (eg, THC vape pens) are sometimes sold on the black market by drug dealers. These may contain other unknown substances added intentionally (eg, fentanyl) or accidentally (eg, vitamin E acetate) during manufacturing.16,17 Vaping cannabis among adolescents and young adults is generally more appealing because it is considered “trendy” and “cool” by users because of a user-friendly design, being easy to conceal, and less physically irritating to the upper respiratory tract than combustible products, and its perception of being safer than smoked cannabis. 18
Cannabis vaping types and methods generally fall into three broad categories
Cannabis e-liquid vaping
Young people either buy cannabis vaping devices (eg, PAX) that resemble commonly used JUUL devices or modify the vaping devices sold in the market to alter the e-liquid or device itself to add cannabis/THC derivative to vape cannabis.
Cannabis dry herb vaping
As the name indicated, dry herb vaping is the use of dry, unprocessed, ground cannabis flower that is inserted into the chamber of the device and heated through a process of convection (hot air passes through the cannabis) or conduction (cannabis is directly placed on the heated surface) rather than combustion to produce vapor that is then inhaled.
Cannabis concentrates vaping
Cannabis concentrates are made by extracting cannabinoids from the cannabis plant. Solvents such as butane or carbon dioxide etc., are used to leach out the cannabinoids from the cannabis plant and the resultant is known by many names such as dabs (the act of using dab known as “dabbing”), wax, ear wax, budder, shatter, and butane hash oil. The concentrates can have a THC content of about 54% to 69% compared to the actual cannabis flower and reach as high as 95%. 19 Nonsolvent methods are also used to make concentrates. For example, pressing or sieving the flower is known as hashish and kief, respectively. 20
Youth Cannabis Vaping and Adverse Health Outcomes
The unique harm associated with cannabis vaping among adolescents and young adults is its ability to offer high potency THC to their bodily systems and decrease in perceived harms of vaping among youth. 21 Cannabis in vaporized form undergoes fast absorption through the lungs resulting in almost immediate detectable drug levels in plasma which peak after 5 to 10 minutes. 22 Extensive evidence from preclinical and clinical studies show that adolescent cannabis exposure can negatively impact brain development and result in adverse health outcomes. The extent to which these findings apply to vaped cannabis is unclear. Preclinical studies using rodent and primate models show clear evidence for adverse developmental outcomes related to adolescent cannabis exposure, regardless of the method of administration. In addition, physiological and behavioral effects observed after vapor exposure is closely matched when THC is administered by other routes of administration. 22 There have been few studies in humans focusing on vaping-related health correlates, but no longitudinal studies have investigated young adult health outcomes related to chronic cannabis vaping during adolescence. Given that the emergence of vaping as a primary method of cannabis consumption has only occurred in the past decade, the paucity of literature in this field is understandable. It highlights the significant need for additional research on this topic to assess the potential disease manifestation from cannabis vaping in the coming years. Below we review critical preclinical and human studies examining the effects of vaping cannabis on health outcomes and describe factors that may contribute to variance in the risk for negative health outcomes in cannabis vaping youth (eg, acute and cumulative THC dose, co-occurring substance use, etc.).
Adverse medical outcomes related to youth cannabis vaping
Preliminary evidence from preclinic studies, small observational studies, and case series from FDA surveillance data suggest that vaping, whether with cannabis, nicotine, or flavor alone, may be associated with damage to cardiopulmonary structures.23,24 However, the long-term consequences of youth vaping on these structures are unknown. Preclinical studies show that vaping leads to oxidative stress in the lung epithelial cells, induces DNA damage, and impairs DNA repair, which is consistent with a potential carcinogenic effect—in addition, vaping leads to a pro-inflammatory response in the respiratory systems, including airway resistance and impaired mucociliary clearance.25 -29 In animal models, heated polyethylene glycol and vegetable glycerin increased inflammatory infiltrates, cytokine production, lung infections, reactive oxygen species, and gene expression. 30
Pre-clinical research also show that THC downregulates nitric oxide production and tumor necrosis factor-α secretion and impairs phagocytic activity in macrophages.31 -33 Human studies show that THC inhalation (but not tobacco inhalation) was also associated with impaired alveolar macrophage functioning resulting in their diminished ability to kill bacteria and tumor cells which could enhance the susceptibility to infectious diseases, cancer, and AIDS. 34 Deep inhalation of cannabis vaping and holding aerosol in the lungs for a more extended period of time further expose respiratory systems to deleterious effects of THC.
During 2019 to 2020, the presence of vitamin E acetate and possibly other chemicals found in nicotine- and THC-containing vaping products were associated with acute lung injury, which was termed e-cigarette or vaping-associated lung injury (EVALI). 35 Youth who develop EVALI report a history of recent vaping and typically present with nonspecific respiratory symptoms ranging from shortness of breath and fever to compromised lung function. 36 Given the non-specific nature of pulmonary symptoms seen in EVALI, which overlap with other respiratory illnesses, including pneumonia and seasonal flu, EVALI is a diagnosis of exclusion typically made based on the history of use of vaping products with nicotine, THC, or both in the last 3 months and after excluding infectious and other etiologies of pulmonary distress. Emerging evidence shows that vaping among adolescents is associated with asthma and asthma exacerbation.37 -39 In addition, contamination of e-liquid may inadvertently expose youth to drugs they did not intend to ingest and carry additional risks. For example, some black market-acquired disposable THC vape products have been found to contain fentanyl, resulting in a risk of opioid overdose by unsuspecting users. 17 Vaping nicotine and THC products have also been associated with other adverse medical problems in youth, including seizures, cardiovascular and oral health problems, burns, and traumatic injuries related to vaping device malfunctions resulting in devices exploding or heating up.40 -42
Co-occurring substance use in cannabis vaping youth
Co-occurring substance use, defined as the consumption of 2 or more substances concurrently or sequentially, is a well-described phenomena that is common among adolescents and young adults. A large body of evidence shows that young people who consume cannabis are more likely to consume alcohol and tobacco and vice versa. 43 Studies also show that baseline non-cannabis vaping (e-cigarette use) during adolescence is associated with simultaneous 44 and future 45 cannabis use (vaping, blunting, and any cannabis use) and an increased likelihood of drinking alcohol 46 compared to non-vapers. The modifiable design of vaping devices and users’ ability to select e-liquid (flavor, nicotine, THC, etc.) and type of cannabis product content prompts non-specific drug use patterns in young people. Measuring these use patterns among adolescents is challenging in both clinical and research settings but needs attention. Regardless of the type of drug use, the interaction between environmental and social factors in an adolescent life potentially determines the trajectory between initiation of drug use and progression to further drug use.
Adverse psychiatric outcomes related to youth cannabis vaping
Recent studies have begun to clarify associations between health and functioning in poly-type cannabis users.47,48 For example, a recent study by Leventhal et al 49 showed that the “poly-type” cannabis product using adolescents had increased the severity of comorbid psychiatric problems, particularly externalizing disorders, compared to “single-type” product cannabis-using adolescents. However, limited evidence exists about the acute and long-term dose effects of vaporized cannabis in humans and its head-to-head comparison with smoked cannabis. A recent laboratory-based human study found that cannabis vaping produced significantly greater subjective drug effects, cognitive and psychomotor impairment, and higher blood THC concentrations compared to cannabis smoking at the same dose. 50 This study also showed that at the 25 mg THC dose, self-reported paranoia was significantly higher in individuals following the vaped compared to smoked administration method. In a longitudinal study of 14 days, young adult participants were asked to keep a daily diary record of whether they used any cannabis and, if any, which mode(s) were used, the number of hits used per mode, overall subjective intoxication, and the socio-environmental context in which they used cannabis. The study found that participants felt higher subjective intoxication on “bong-only” days than “vape-only” days, but similar across days they vaped and smoked blunts, joints, and pipes. 51
Triangulation of evidence from cross-sectional, longitudinal human studies and animal studies suggests that THC is associated with adverse health outcomes in young people and suggests a dose-response relationship. For example, the use of high THC potency cannabis products by adolescents has been associated with a greater risk for the development of schizophrenia and a poorer course of psychotic disorders in young people. 52 Problematically with regard to cannabis vaping, e-liquid and concentrates commonly contain very high amounts of THC (80%-95%); thus, vaping cannabis with these products may contribute to adverse health outcomes among youth cannabis users. For example, inhalation of high doses of THC via cannabis vaping may result in a greater risk for adverse psychiatric outcomes in youth.53,54 A number of case reports have described severe mood, anxiety, psychotic symptoms, aggression, catatonia 55 , and suicidality following vaping cannabis products, with many of these cases requiring emergency medical treatment and hospitalization. Preliminary studies in this area have focused almost exclusively on delta-9-THC toxicity. Given the growing use of delta-8 and delta-10, further investigation is needed to determine whether these and other analogs of delta-9-THC carry the same risk for adverse health outcomes, as is suggested from anecdotal evidence. Additional research is also needed to clarify the risk related to the use of different vaped cannabis product types and whether the addition of CBD or other phyto-cannabinoids or terpenes to THC-containing vapes mitigates this risk. In addition, since cannabis vaping is considered “cool” by young people, many start vaping at an earlier age, further increasing the risk of developing a cannabis use disorder (CUD) and experiencing cannabis-related harm by young adulthood. 56
Management of Cannabis Vaping in Busy Outpatient Practice
Best practices in clinical management for problematic cannabis use, including cannabis vaping in adolescents and young adult, focuses on (1) strategic and systematic screening for cannabis use and vaping in all young people presenting to primary care clinical settings; (2) proper identification of at-risk youth; and (3) administration of evidence-based psychosocial interventions such as motivational interviewing, cognitive behavioral therapy, and family-based therapies targeting cannabis cessation (see Figure 1 for strategic screening and clinical management algorithm). Emerging research suggests that clinicians can improve youth CUD treatment outcomes by adding contingency management and aggressively treating co-occurring psychiatric and medical symptoms in these patients. 57 While there are currently no FDA-approved medications for CUD, recent studies testing n-acetylcysteine have shown promising safety and efficacy results when this supplement is used in conjunction with psychosocial treatment in youth (ages 13-21 years) with CUD. 58 For acute psychiatric symptoms that can be linked to the recent cannabis intake, like those described in the clinical vignette about Ms. X, supportive care, decreased stimulation, and reassurance may be helpful. There is anecdotal evidence for the use of benzodiazepines or antipsychotics to target transient panic/anxiety or paranoia in patients presenting to the ED, however, the evidence for this approach outside of ED settings is limited.59,60 Severe agitation or aggression requires a thorough investigation of other possible drug use, and co-occurring psychiatric disorders. This should prompt mental health expert consult.
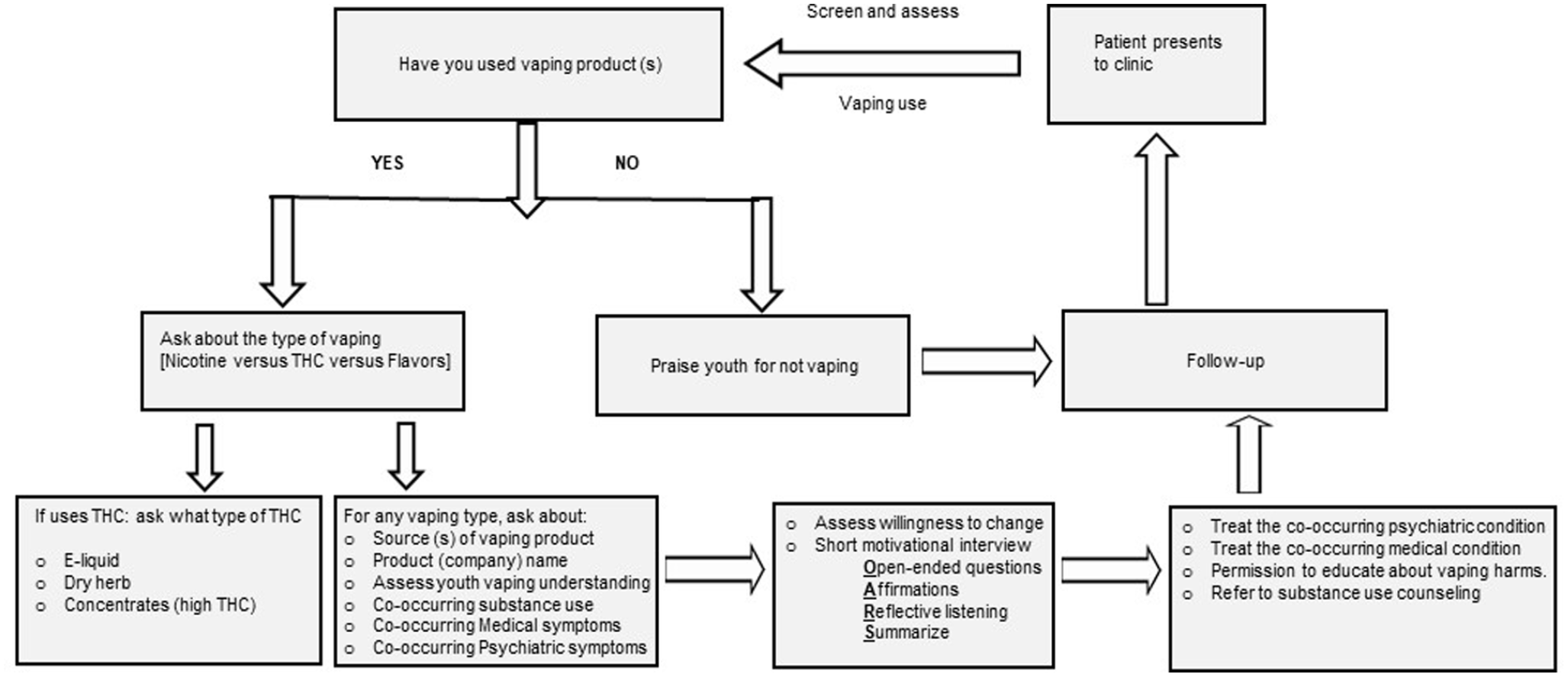
Strategic screening and clinical management algorithm.
It should be noted that the use of cannabis and its psychiatric sequelae are dependent on cannabis dose and chemotype, family history of substance use, genetic vulnerability, and age of exposure. Not all young people who vape cannabis experience adverse psychiatric symptoms. Still, a risk assessment should be conducted on every patient in the clinical space. In addition, a large number of adolescents and young adults that clinicians see in their clinical practice choose to abstain from vaping and other drug use; positive reinforcement such as praising “no-vaping behavior” should be given to these youth.
Conclusion
Over the past decade, youth cannabis vaping has increased significantly and is now a major public health problem in the US. The field of science focused on youth cannabis vaping is in its infancy and much work is needed given the rapid expansion of this behavior. Associations between medical problems, adverse psychiatric outcomes, and cannabis use from smoked cannabis and vaped cannabis are similar in many ways, but some notable differences exist. Preliminary studies suggest that vaping cannabis may be associated with unique health risks that are not commonly seen in relation to smoking cannabis (eg, EVALI and seizures). Additionally, some aspects of cannabis vaping (eg, more efficient delivery method and higher THC potency of products) place young people at a higher risk of psychotic symptoms and acute psychiatric decompensation related to the higher acute and cumulative THC exposure from vaped cannabinoid products. Pediatric clinicians should be aware of the types and kinds of vape products, the risks related to cannabis vaping, and should receive training focused on screening for and treating cannabis use disorders related to vaped cannabis use in youth.