
Abstract
Objective:
While the number of overdoses in the United States continues to increase, lags in data availability have undermined efforts to monitor, respond to, and prevent drug overdose deaths. We examined the performance of a single-item mandatory radio button implemented into a statewide medical examiner database to identify suspected drug overdose deaths in near-real time.
Materials and Methods:
The New Jersey Office of the Chief State Medical Examiner operates a statewide mandated case management data system to document deaths that fall under the jurisdiction of a medical examiner office. In 2018, the New Jersey Office of the Chief State Medical Examiner implemented a radio button into the case management data system that requires investigators to report whether a death is a suspected drug overdose death. We examined the performance of this tool by comparing confirmed drug overdose deaths in New Jersey during 2020 with suspected drug overdose deaths identified by investigators using the radio button. To measure performance, we calculated sensitivity, specificity, positive predictive value, negative predictive value, and false-positive and false-negative error rates.
Results:
During 2020, New Jersey medical examiners investigated 26 527 deaths: 2952 were confirmed by the state medical examiner as a drug overdose death and 3050 were identified by investigators using the radio button as a suspected drug overdose death. Sensitivity was calculated as 96.1% (2837/2952), specificity as 99.1% (23 362/23 575), positive predictive value as 93.0% (2837/3050), negative predictive value as 99.5% (23 362/23 477), false-positive error rate as 7.0% (213/3050), and false-negative error rate as 3.9% (115/2952).
Practice Implications:
Implementation of a radio button into death investigation databases provides a simple and accurate method for identifying and tracking drug overdose deaths in near-real time.
Drug overdose is the leading cause of preventable injury-related death in the United States. 1 In 2021, nearly 107 000 drug overdose deaths occurred, a record high and a 14% increase from the previous year. 2 The main driver of these deaths is synthetic opioids, primarily illicitly manufactured fentanyl and its analogs. 2 While the number of overdoses continues to increase, lags in data availability have undermined efforts to monitor, respond to, and prevent drug overdose deaths. Drug-related deaths typically require forensic autopsy and toxicology analyses, which often delay the completion of death certificates. Consequently, death certificate records for drug overdose deaths have longer lag times than records for all other injury-related deaths. 3 For drug overdose deaths that occurred from March 2015 through July 2016, the mean percentages of death records available for national surveillance reports at 13, 26, and 39 weeks (quarterly) were 38%, 83%, and 95%, respectively. 3 In addition to lengthy autopsy, toxicology, and other data collection techniques required for suspected drug-related deaths, the timely and accurate reporting of overdose mortality data has been complicated by regional variations in coding and the rapidly evolving nature of the opioid overdose crisis.4,5
In response to the demand to produce faster statistics on the worsening overdose crisis, state and local health jurisdictions are attempting methods that would allow timely identification of suspected drug overdose deaths. Identification measures include using syndromic surveillance platforms, 6 compiling multiple data sources as part of a comprehensive drug overdose fatality surveillance system, 7 making a suspected drug overdose a notifiable condition, 8 and uploading data to the Overdose Detection Mapping Application Program platform. 9 Public health departments and other agencies and institutions have also implemented web portals to make preliminary data on overdose death counts publicly available in near-real time.10-14 Despite an increased availability of timely data on suspected drug overdoses, methods for determining whether a death is a suspected drug overdose often remain unknown, are inconsistent across platforms, and generally do not use medical examiner data.
Medicolegal death investigations are initiated as required by state laws in cases of unexplained, sudden, and/or unnatural deaths, including suspected intentional or unintentional drug overdose deaths. 15 Medical examiners are licensed physicians with specialized training in forensic pathology who, along with coroners, are authorized to certify drug overdose deaths.16,17 Under the direction of a medical examiner, medicolegal death investigators are responsible for collecting and documenting information related to the decedent’s death for the medical examiner to use to determine and certify the cause and manner of death. Although these certifications are aided by delayed toxicology data, several other key data points associated with drug overdose fatality are available in these reports and provide opportunities to rapidly identify cases of overdose mortality and conduct time-sensitive activities (eg, delivery of overdose prevention resources) before death certificates are finalized. However, these data are underused because they are often not standardized and are recorded in large free-text fields. 18 Although researchers are developing methods that use data generated during death investigations to identify suspected drug overdose deaths in near real time, such as New York City’s Suspected Potential Overdose Tracker (SPOT), 19 these methods require substantial resources or advanced data extraction techniques to produce analyzable data sets from narrative reports. A simplified method for identifying suspected drug overdose deaths in near real time by death investigators would improve adoption of such methods and provide timely insights into the drug overdose epidemic.
To address the need for timely and actionable data on overdose fatalities, the New Jersey Office of the Chief State Medical Examiner (OCSME) implemented a mandated data field into its statewide case management data system requiring medicolegal death investigators to report on suspected overdoses at the time of data entry. This technique allows reporting and dissemination of drug overdose death statistics to be expedited, well before toxicology and autopsy data are documented and death certificates are completed. Our study aimed to examine the performance of the mandated data field for rapidly identifying and reporting drug overdose deaths.
Materials and Methods
Setting
New Jersey is composed of 21 counties and operates a county-based medical examiner system with 10 regional offices. The OCSME has regulatory and operational oversight over all 10 regional offices. The regional offices enter information on deaths that fall under the jurisdiction of a New Jersey medical examiner office into the statewide case management data system, allowing for streamlined tracking and reporting on deaths investigated by medical examiners across the state. In 2018, the OCSME implemented a radio button into the case management data system requiring medicolegal death investigators to select yes or no for a data field that reads “suspected drug toxicity.” We used 2020 data from the OCSME to evaluate how the radio button performed in capturing drug overdose deaths in New Jersey. Thus, by using 2020 data, we allowed for a phase-in period >1 year to ensure proper implementation of this new reporting feature before our evaluation.
Because this study did not involve human data or participants, the Western-Copernicus Group Institutional Review Board determined that assessment was not necessary per its guidelines.
Suspected Drug Overdose Deaths
Medicolegal death investigators record suspected drug overdose deaths in the case management data system’s investigations module. When entering investigative information of a case into the system, investigators are required to use the mandatory radio button to report whether they suspect that the death was a drug overdose. New Jersey requires medicolegal death investigators to be certified by the American Board of Medicolegal Death Investigators within 3 years of hire. To prepare and train staff on the use of the mandatory radio button, the OCSME distributed guidelines that explained the modifications made to the case management data system and provided examples of key indicators of suspected drug toxicity (eSupplement). Examples of indicators of suspected drug toxicity include a history of illicit/prescription drug misuse, drug and drug paraphernalia or prescription medication present at the scene, and presence of needle track marks on the body. However, investigators are not required to use specific criteria and can use discretion when determining a suspected drug overdose death. Investigators make the determination based on their training as a medicolegal death investigator and, when necessary, with guidance from the medical examiner in the office at the time that they are investigating the case. In other words, investigators select yes to the suspected drug toxicity radio button if they find reasonable suspicion that the death was drug related based on evidence from the death scene and/or initial toxicology results from a hospital.
Confirmed Drug Overdose Deaths
After the medicolegal death investigator has completed an initial investigation and transferred the case to the applicable medical examiner’s office, a medical examiner conducts autopsy and toxicology investigations. Using toxicology and autopsy findings, the medical examiner confirms drug toxicity in the case management data system’s pathology module. At the end of each year, the OCSME epidemiologist and the chief state medical examiner perform a final review of cases by running a report of all cases that are closed (ie, no longer pending) and have confirmed drug toxicity as determined by the medical examiner. During this step, the OCSME epidemiologist and the chief state medical examiner remove cases (typically a small number) that were drug related but in which drugs were not determined to be the cause of death (eg, drownings).
Dashboard
Along with the addition of the suspected overdose radio button, the OCSME has automated reporting on suspected drug overdose deaths and made data publicly available on a dashboard. 20 The dashboard is updated weekly and uses interactive data visualizations to present the number of suspected drug-related deaths by county each week (overall and by race and ethnicity, sex, and age), the trend in suspected drug overdose deaths by month and by county, and other statistics on suspected drug-related deaths. This dashboard improves reporting transparency and reduces extensive data requests, and it provides timely information on drug overdoses for public health practitioners, researchers, policy makers, law enforcement, and the public.
Performance Measures
We examined the performance of the radio button tool by comparing suspected drug overdose deaths identified by medicolegal death investigators with drug overdose deaths confirmed and certified by the chief state medical examiner as deaths in which drug overdose or intoxication was listed as the cause of death. We measured the performance of the radio button tool by examining sensitivity, positive predictive value (PPV), false positives, false negatives, specificity, and negative predictive value (NPV). Sensitivity (ie, true positive rate) is defined as the probability that a death was identified as a suspected drug overdose given that it was a true (confirmed) drug overdose death. PPV is defined as the proportion of all suspected overdoses that were confirmed to be overdoses. False positives are deaths that were identified as suspected overdoses but were later confirmed not to be overdoses or where the final cause of death was undetermined (ie, type I error). False negatives are deaths that were confirmed overdoses but were not identified as suspected overdoses (ie, they were missed by the investigator; type II error). Specificity (ie, true negative rate) is defined as the probability that a death was determined not to be a suspected overdose given that it was a confirmed nonoverdose. NPV is defined as the proportion of deaths determined not to be suspected overdoses that were confirmed as nonoverdoses. We calculated sensitivity, PPV, and the proportion of false-positive and false-negative errors overall and by demographic subgroup (sex, age, race, and ethnicity).
Statistical Analysis
We used the Wilson score interval to calculate 95% CIs for point estimates. We used the Pearson χ2 test to compare the proportion of false-positive and false-negative results across age, sex, and race and ethnicity subgroups. We also compared false-positive and false-negative results across the 10 regional offices. We conducted statistical analyses using Stata/SE version 17.0 (StataCorp LLC) and determined significance as P < .05.
Results
In 2020, the New Jersey OCSME investigated 26 527 deaths. The chief state medical examiner confirmed 2952 deaths as drug overdose deaths, and medicolegal death investigators identified 3050 deaths as suspected drug overdose deaths. An average of 8.2 more suspected drug overdose deaths than confirmed drug overdose deaths occurred per month in 2020 (Figure).
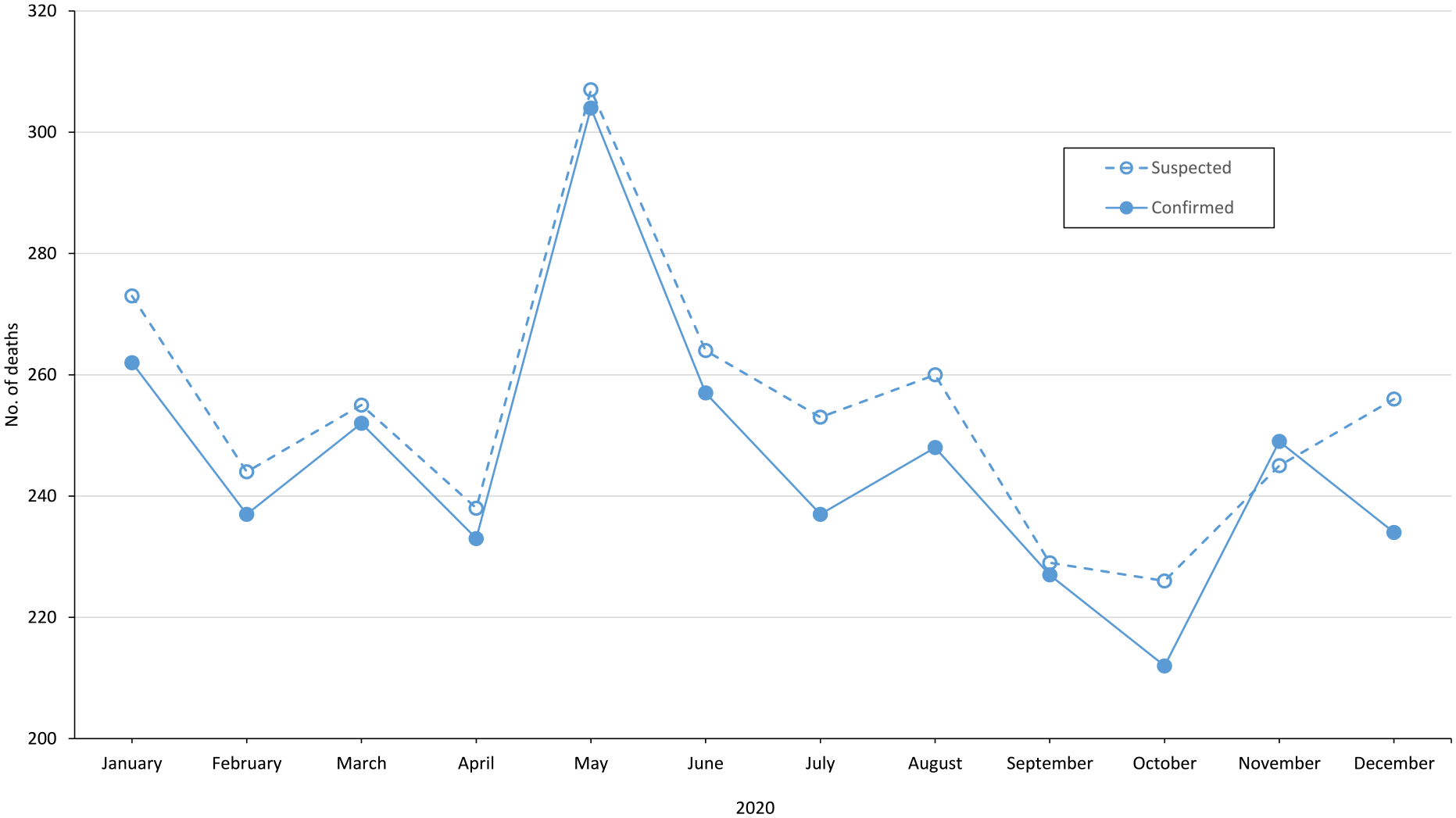
Suspected and confirmed drug overdose deaths, New Jersey, 2020.
The proportion of suspected drug overdose deaths that were confirmed to be drug overdose deaths (PPV) was 93.0% (2837/3050) (Table 1). The proportion of suspected overdoses that were confirmed not to be overdoses (false positives) was 7.0% (213/3050), and the proportion of confirmed overdoses that were not identified as suspected overdoses (false negatives) was 3.9% (115/2952). The proportion of confirmed drug overdose deaths that were captured by investigators as suspected drug overdose deaths (sensitivity) was 96.1% (2837/2952). In addition, the proportion of confirmed nonoverdose deaths that were determined by investigators not to be suspected drug overdose deaths (specificity) was 99.1% (23 362/23 575), and the proportion of deaths determined not to be suspected drug overdose deaths that were confirmed as nonoverdose deaths (NPV) was 99.5% (23 362/23 477).
Overall performance of the suspected overdose radio button, New Jersey Office of the Chief State Medical Examiner, 2020 a
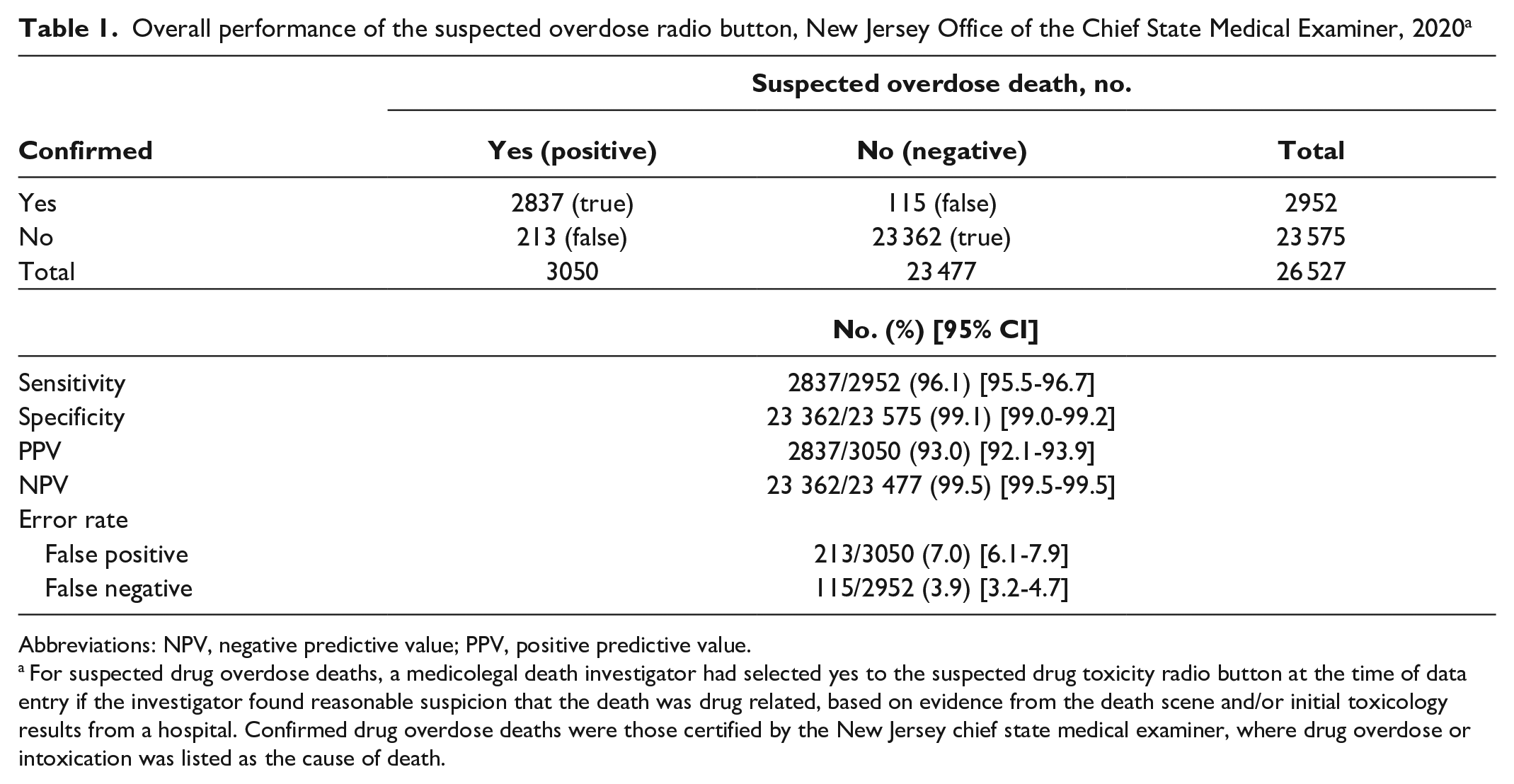
Abbreviations: NPV, negative predictive value; PPV, positive predictive value.
For suspected drug overdose deaths, a medicolegal death investigator had selected yes to the suspected drug toxicity radio button at the time of data entry if the investigator found reasonable suspicion that the death was drug related, based on evidence from the death scene and/or initial toxicology results from a hospital. Confirmed drug overdose deaths were those certified by the New Jersey chief state medical examiner, where drug overdose or intoxication was listed as the cause of death.
When we examined performance measures by demographic subgroups, we found significantly more false-positive errors among people aged ≥55 years (11.3%) than among people aged 33-54 years (5.2%) and people aged ≤32 years (6.3%; P < .001) (Table 2). We found significantly fewer false negatives among people aged ≤32 years (1.5%) than among people aged 33-54 years (4.3%) and people aged ≥55 years (5.4%; P < .001). Sex and race/ethnicity were not significantly associated with the number of false-positive or false-negative errors. The proportion of false-positive errors ranged from 1.1% to 14.0% across the 10 regional offices (Table 3). The proportion of false-negative errors ranged from 1.3% to 8.5% across the 10 regional offices.
Performance of suspected overdose radio button by demographic subgroup, New Jersey Office of the Chief State Medical Examiner, 2020 a
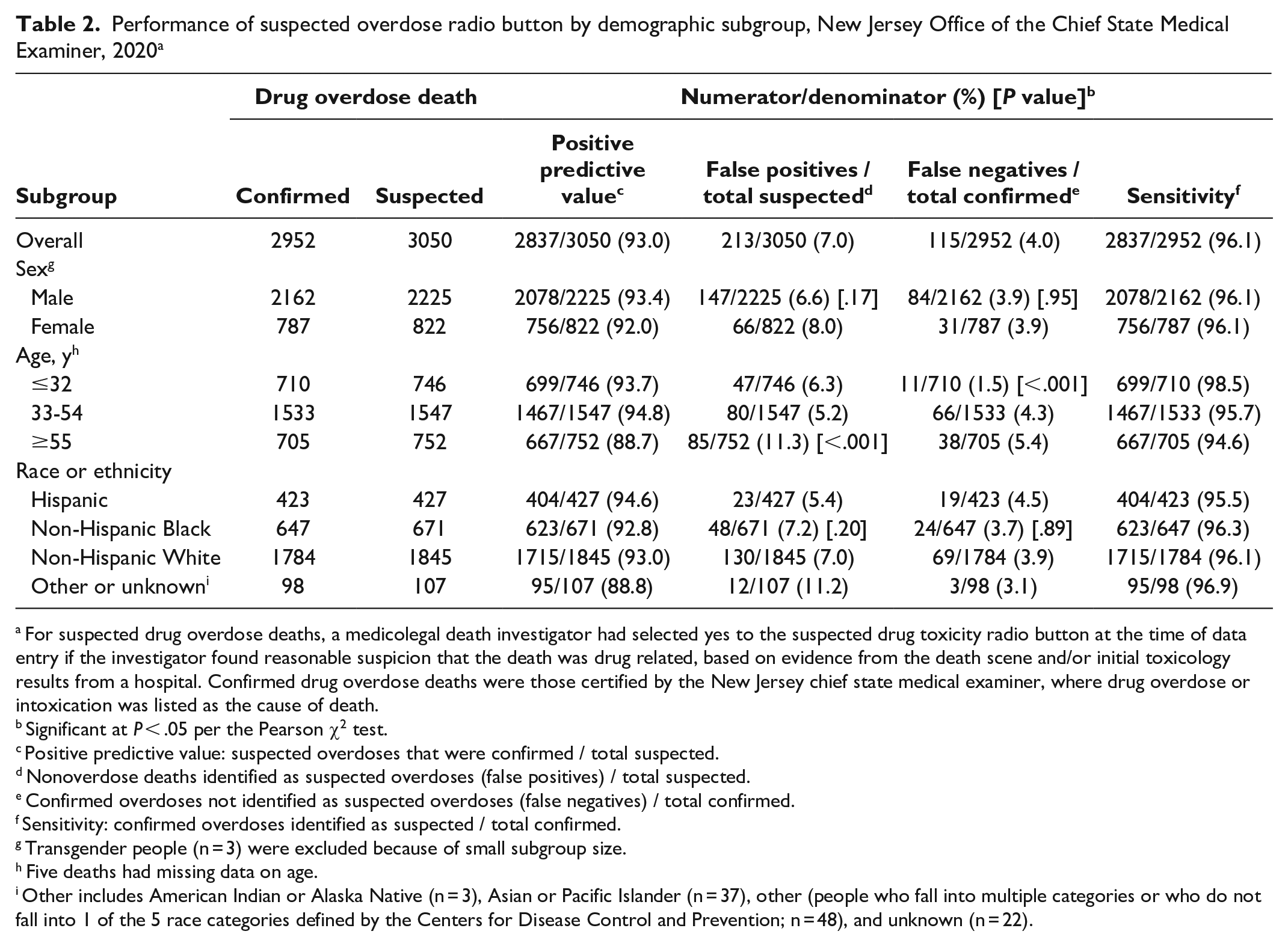
For suspected drug overdose deaths, a medicolegal death investigator had selected yes to the suspected drug toxicity radio button at the time of data entry if the investigator found reasonable suspicion that the death was drug related, based on evidence from the death scene and/or initial toxicology results from a hospital. Confirmed drug overdose deaths were those certified by the New Jersey chief state medical examiner, where drug overdose or intoxication was listed as the cause of death.
Significant at P < .05 per the Pearson χ2 test.
Positive predictive value: suspected overdoses that were confirmed / total suspected.
Nonoverdose deaths identified as suspected overdoses (false positives) / total suspected.
Confirmed overdoses not identified as suspected overdoses (false negatives) / total confirmed.
Sensitivity: confirmed overdoses identified as suspected / total confirmed.
Transgender people (n = 3) were excluded because of small subgroup size.
Five deaths had missing data on age.
Other includes American Indian or Alaska Native (n = 3), Asian or Pacific Islander (n = 37), other (people who fall into multiple categories or who do not fall into 1 of the 5 race categories defined by the Centers for Disease Control and Prevention; n = 48), and unknown (n = 22).
False-positive and false-negative error rates of the suspected overdose radio button, by regional office, New Jersey Office of the Chief State Medical Examiner, 2020 a
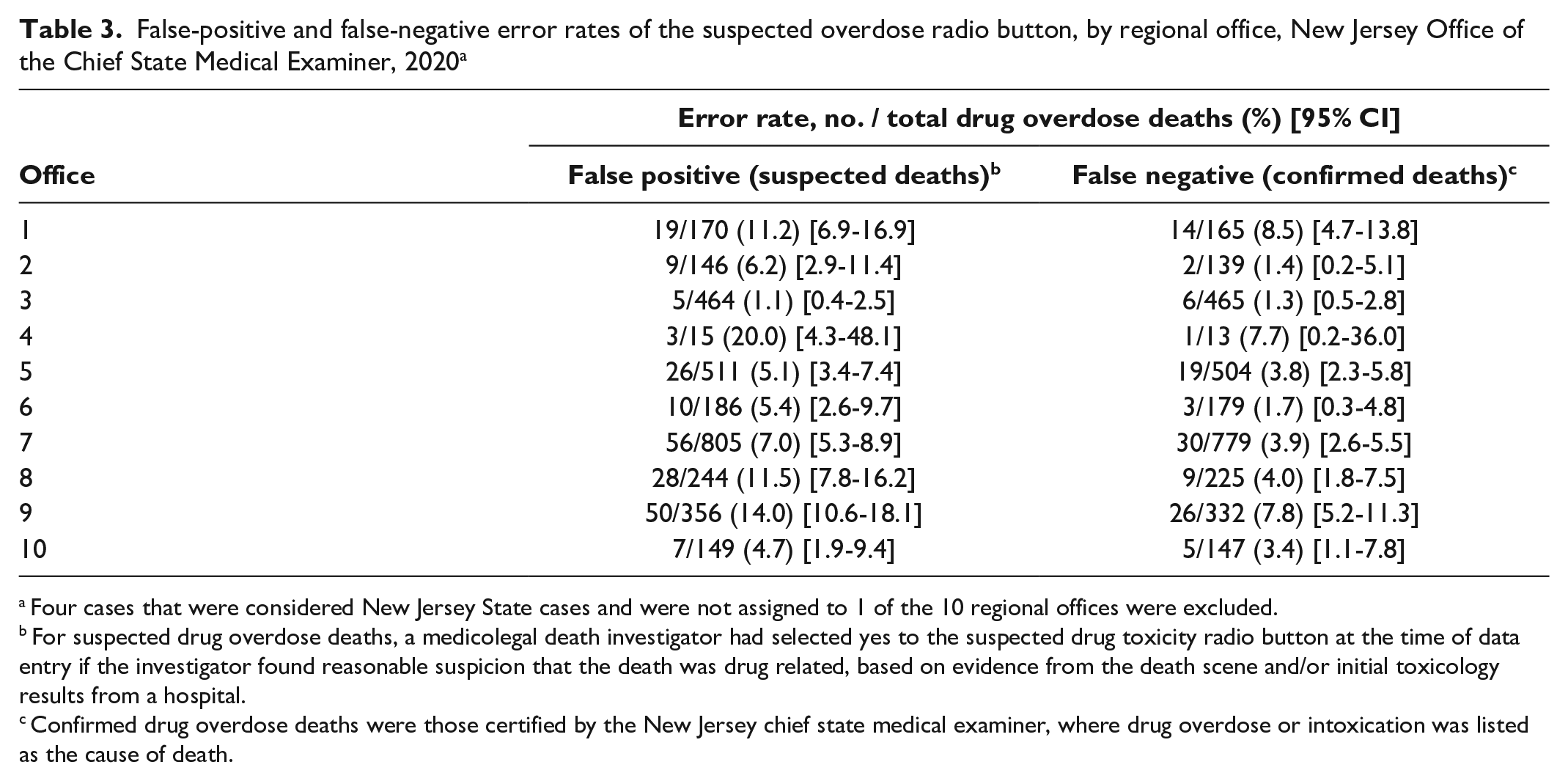
Four cases that were considered New Jersey State cases and were not assigned to 1 of the 10 regional offices were excluded.
For suspected drug overdose deaths, a medicolegal death investigator had selected yes to the suspected drug toxicity radio button at the time of data entry if the investigator found reasonable suspicion that the death was drug related, based on evidence from the death scene and/or initial toxicology results from a hospital.
Confirmed drug overdose deaths were those certified by the New Jersey chief state medical examiner, where drug overdose or intoxication was listed as the cause of death.
Discussion
The aim of this study was to examine the performance of a radio button implemented into New Jersey’s electronic statewide medical examiner case management data system for identifying suspected drug overdose deaths in near-real time. To our knowledge, this is the first time a mandatory data field such as this has been implemented and evaluated. This single-item mandatory data field demonstrated high sensitivity (96.1%), specificity (99.1%), PPV (93.0%), and NPV (99.5%) for predicting whether a death was a drug overdose. This study used data on deaths falling under the jurisdiction of a medical examiner office in New Jersey during 2020, demonstrating the reliability of the radio button under difficult circumstances, as medical examiner offices faced an overwhelming increase in deaths because of the COVID-19 pandemic. The addition of the suspected overdose radio button was accompanied by the OCSME developing a user-friendly and publicly available dashboard that various regional partners can access to support program goals. Implementing a radio button into coroner and medical examiner electronic data systems allowed for the collection of timely data on suspected drug overdose fatalities, which may be used by public health departments, epidemiologists, public health programs, and others in a multitude of ways to improve monitoring of the drug overdose epidemic and provide actionable insights.
Our study showed more false-positive errors among the older group (aged ≥55 y) than the younger groups (aged ≤32 and 33-54 y), possibly because the rate of health problems that cause death tends to be higher among people aged ≥55 years than among those aged <55 years. Similarly, our study showed fewer false-negative errors among people aged <55 years than among those aged ≥55 years. In other words, fewer overdoses are missed among younger people than older people, perhaps because younger people are less likely to die of other natural causes or experience other health complications. Our study also showed differences in error rates across the 10 regional medical examiner offices. These results can be used to identify offices and investigators that have low performance and that need additional training on evaluating the evidence of a drug overdose death and making an informed decision. However, we found a wide range in the number of deaths investigated by each regional office (range, 15-805 suspected drug overdose deaths), likely reflecting the size and urbanicity or rurality of the office. Thus, a few errors in a small office can inflate false-positive and false-negative error rates. A wide range in error rates across offices may also be due to differences in implementation (eg, receipt of the training guide, additional training, guidance/direction of the supervising medical examiner during implementation). Future studies are needed to investigate the causes of these errors, examine implementation outcomes, and assess whether additional training improves performance and how performance compares across investigator characteristics (eg, age, number of years in practice).
The key strengths of the radio button method for identifying and reporting suspected drug overdose deaths are that it is quick and simple. The simplicity of this radio button provides important advantages over other tools for identifying suspected overdoses, such as the New York City medical examiner’s SPOT tool, which is resource and time intensive and requires substantial investment by the agency (eg, funding, personnel). 19 In contrast, the single-item radio button provides data on suspected drug overdose deaths in as little as a few seconds with minimal changes needed to databases and death investigators’ data collection procedures. Of note, the overall sensitivity and PPV of the radio button (96.1% and 93.0%, respectively) were higher than those of SPOT (66%-77% and 77%-85%) 19 and the King County, Washington, medical examiner system (83% and 89%), which uses probable overdose indicators to classify suspected drug overdose deaths. 21 Our study suggests that a method based on an investigator’s own discretion, such as the New Jersey OSCME’s radio button, outperforms tools that require specific criteria to be met (eg, paraphernalia on scene), such as the SPOT and the King County rapid overdose identification systems. Additionally, implementing a radio button that requires investigators to select a single response option (yes or no) versus an optional data field that could be missed (ie, a checkbox) ensures that each death is considered a potential drug overdose and that data are collected.
Limitations
This study had several limitations. First, the single-item binary question does not capture data on drug overdose indicators or evidence that informed the investigator’s decision. Thus, we were unable to evaluate the extent to which potential indicators (eg, paraphernalia on scene) were present and predictive of drug overdose. Future studies that are based on investigators’ own discretion should collect information on what informed their decision. Second, generalizability may be limited. A statewide database with oversight by a centralized state medical examiner office allows creation and enforcement of operating and performance standards for every medical examiner office in New Jersey. Although this structure allows for an efficient and standardized mechanism for reporting suspected drug overdose deaths statewide, several states lack this capacity. For example, many states operate a decentralized county-based system with a mixture of coroner and medical examiner regional offices, and few states operate a statewide coroner or medical examiner database. 22 To increase data consistency, researchers have recommended a centralized office with state oversight. 5 Nonetheless, the methodology for reporting suspected drug overdoses described in our study may improve local monitoring in decentralized states. More research is needed to assess the performance of suspected drug overdose tracking tools in other geographic regions, particularly states operating decentralized county-based coroner systems.
Practice Implications
Epidemiological Surveillance, Reporting, and Data Sharing
The mandatory radio button offers a standardized method for public health and safety agencies to obtain preliminary counts of drug overdose deaths from coroner and medical examiner systems. Because state public health departments are required to report to the Centers for Disease Control and Prevention’s National Vital Statistics System, this method could improve national provisional count estimates. 23 Data on suspected drug overdose deaths may also be used to routinely develop reports that describe drug overdose death trends and other key findings. These reports may be tailored and distributed to representatives and leaders from various partner agencies, including public health and safety partners that are most likely to intersect with people at risk of overdose. Partner agencies may use the data to better understand the incidence of drug overdose fatalities in the population that they serve and evaluate their own prevention efforts.
Case-Level Investigations
Accurate and timely data on suspected overdoses may be used to drive case-level investigations. For example, social network members of suspected drug overdose decedents may be identified to collect critical historical and contextual information about the drug overdose death and offer services, as is being done by the New York City medical examiner office. 24 Conducting case-level investigations soon after the death has many advantages over delaying investigations until death certificates are completed. For example, delayed investigations are likely subject to recall bias; family and other social network members may be lost to follow-up; and a high need for services immediately after the loss is likely.
Rapid and Targeted Deployment of Resources
Community and health policy makers can use near–real-time data to guide service planning and inform a rapid deployment of evidence-based interventions to reduce drug overdose deaths, such as where to deploy mobile harm reduction sites and naloxone distribution. These data would allow for the delivery of other time-sensitive interventions, such as those that connect grieving family members to grief and bereavement services and refer decedents’ social network members who also use drugs to treatment and harm reduction services.
Conclusions
The implementation of a simple radio button into death investigation data collection systems allows for the accurate and timely identification of drug overdose deaths. Improved timeliness and accuracy of identifying drug overdose fatalities through a simple and replicable process will allow for data-driven decision-making and the rapid identification of gaps in drug overdose response preparedness among public health and public safety departments. In addition, quick and accurate identification of drug overdose deaths offers opportunities for more expedited evaluation of novel overdose prevention interventions, programs, and policies.
Supplemental Material
sj-docx-1-phr-10.1177_00333549241230921 – Supplemental material for Rapid Identification of Suspected Drug Overdose Deaths by Death Investigators, New Jersey, 2020
Supplemental material, sj-docx-1-phr-10.1177_00333549241230921 for Rapid Identification of Suspected Drug Overdose Deaths by Death Investigators, New Jersey, 2020 by Karli R. Hochstatter, Marlon Williams, Shanna Latham, David Fenton and Andrew L. Falzon in Public Health Reports
Footnotes
Acknowledgements
The authors acknowledge the software engineers at the New Jersey OCSME who supported the development and implementation of the automated dashboard that is publicly available online, including Sean Barton, BS, Kevin McGrath, BS, and Kirk Phillips, BS.
Disclaimer
The content of this article is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is supported in part by the National Institute on Drug Abuse of the National Institutes of Health (R01DA057685).
Supplemental Material
Supplemental material for this article is available online. The authors have provided these supplemental materials to give readers additional information about their work. These materials have not been edited or formatted by Public Health Reports’s scientific editors and, thus, may not conform to the guidelines of the AMA Manual of Style, 11th Edition.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.