
Abstract
Objectives:
Evidence has emerged on the health dangers of electronic cigarette (e-cigarette) use among pregnant women and neonates. We examined whether rural residence is a risk factor for smoking and e-cigarette use among women during the peripartum period in the United States.
Methods:
This study was based on pooled cross-sectional 2015-2020 data from the Pregnancy Risk Assessment Monitoring System. The outcome was exclusive smoking, exclusive e-cigarette use, and use of both products (ie, dual use) versus use of neither tobacco product by women with live infants aged 2 to 6 months. We examined rural–urban differences in outcome by using univariate and multivariable multinomial logistic regressions with post hoc contrasts and marginal analyses, adjusting for complex survey design and nonresponse.
Results:
During the peripartum period, 5.0% of women were smoking combustible cigarettes, 5.0% were using e-cigarettes, and 1.9% were using both tobacco products. The crude prevalence of e-cigarette use was 1.1 percentage point higher, and the adjusted prevalence was 0.8 percentage points lower for rural versus urban women (P < .001 for both). Among rural women, 6.7% (95% CI, 6.3%-7.1%) smoked combustible cigarettes exclusively and 2.6% (95% CI, 2.3%-2.8%) used both products, as compared with 4.5% (95% CI, 4.4%-4.8%) and 1.7% (95% CI, 1.6%-1.8%) of urban women, respectively, adjusting for sociodemographic and health-related characteristics.
Conclusions:
Maternal sociodemographic and health-related characteristics differed by combustible smoking versus e-cigarette use during the peripartum period. The effect of residence on e-cigarette use was significantly confounded by sociodemographic and health-related characteristics, resulting in clinically comparable prevalence of e-cigarette use in rural and urban mothers with live infants aged 2 to 6 months.
Although the prevalence of tobacco product use has decreased among adults during the previous 5 decades, it has remained higher among rural residents than urban ones in the United States. 1 Based on the 2021 National Health Interview Survey, the prevalence of any tobacco product use was 26.2% and that of combustible cigarette smoking was 18.0% among rural residents, as compared with 17.5% and 10.5%, respectively, among urban residents. 1 The prevalence of electronic cigarette (e-cigarette) use rose from 3.9% to 5.3% among rural residents and from 3.7% to 4.4% among urban residents from 2020 to 2021.1,2 Based on the 2007-2016 trend analyses of the National Survey on Drug Use and Health, rural women had a lower rate of decrease in the prevalence of tobacco and nicotine product use than rural men, urban men, and urban women.3-5
Combustible cigarettes and e-cigarettes have several common toxicants, such as nicotine and various volatile organic compounds, as well as heavy metals, and their adverse maternal and fetal health effects are well established. 6 Studies have highlighted that data are insufficient to draw conclusions on the effects of e-cigarette use during pregnancy.6-8 Meanwhile, applying the precautionary principle is advisable (ie, to avoid harm while evidence is accumulating), given the potential risks from known compounds. In 2014, the US Surgeon General noted that the evidence had already been sufficient to provide warnings to pregnant women and women of reproductive age about the use of nicotine-containing products, including smokeless tobacco, e-cigarettes, and newer forms of nicotine-containing tobacco products. 9
Higher rates of tobacco product consumption in rural versus urban areas have been attributed to several factors. For example, rural children and adolescents are exposed as early as age 11 years to tobacco products because of targeted retail advertising.10,11 Owing to restrictions on public advertising, tobacco companies have diverted their focus toward point-of-sale advertising by incentivizing retailers to post advertising and signage, to display products, and to promote tobacco products based on prices. 12 Social–ecological theory suggests that this type of advertising has a powerful influence on adolescents’ behavior because it increases their perception of the popularity and availability of tobacco products as early as age 15 to 20 years. 13 Another factor commonly attributed to rural individuals being more likely than urban individuals to accept tobacco products is a history of growing tobacco and its adverse effects on norms, values, and perspectives toward accepting tobacco use, especially intergenerational tobacco use.10,13 Adolescents in rural areas are exposed to tobacco products earlier in their lives and are more likely to experience adverse consequences of their use than adolescents in urban areas.10,13 Thus, targeted advertising and acceptance or, tolerance of tobacco use, are believed to contribute to the heightened prevalence of tobacco product use in rural areas as compared with urban areas.
In addition to these contextual factors, research has emerged on individual reasons for e-cigarette use and differences by social identities.14,15 A study based on data from the 2014-2015 Tobacco Use Supplement to the Current Population Survey reported that, nationally, 63.9% of ever e-cigarette users believed that e-cigarettes might be less harmful to people around them than combustible cigarettes. 14 No difference was found between rural and urban adults in perceptions and beliefs about e-cigarettes as a substitute tobacco product being less harmful to them than combustible cigarettes and being useful with smoking cessation. 14 In terms of differences in individual reasons for e-cigarette use by sex, female users are motivated by family recommendations and weight control, whereas men are motivated by health and smoking cessation goals.16-18 Yet, during pregnancy, the common perceptions of e-cigarettes are that they are a safer and potentially healthier alternative for mother and baby than cigarette smoking and that they may be used as a tool for smoking cessation. 19
The purpose of this study was to examine rural–urban differences in smoking and e-cigarette use among women during the peripartum period (ie, 2- to 6-month period after the child’s birth). Understanding the smoking prevalence, types of tobacco product use, and risk factors of combustible cigarette use and e-cigarette use among rural women of reproductive age is of particular importance because it could narrow the disparities of adverse health outcomes of rural mothers and their infants.20,21
Methods
We conducted an observational study based on pooled cross-sectional data from the 2015-2020 Pregnancy Risk Assessment Monitoring System (PRAMS), a joint surveillance project of the Centers for Disease Control and Prevention, Division of Reproductive Health, and state health departments. More details on PRAMS can be found elsewhere. 22 Briefly, developed in 1987, PRAMS collects state-specific, population-based data on maternal behaviors and experiences before, during, and shortly after pregnancy. The PRAMS sample of women who have had a recent live birth is drawn from the state’s birth certificate file. Each participating state draws a stratified systematic sample of 100 to 250 new mothers every month from a frame of eligible birth certificates. Many states oversample low-weight births or stratify by mother’s race or ethnicity. Annual sample sizes range from 1000 to 3000, divided among 3 to 6 strata of public health interest. Mothers’ responses are linked to extracted birth certificate data items for analysis, which provide PRAMS with demographic and medical information collected through the state’s vital records system. The sampling procedures allow for results that are generalizable to the state’s entire population of annual live births. Nonresponse adjustment factors attempt to compensate for the tendency of women with certain characteristics (eg, unmarried, low education levels) to respond at lower rates than women without those characteristics. 23 PRAMS has a threshold policy on the minimum overall weighted response rate for the data release each year. The threshold was 55% for 2015 and 2017 and 50% for 2018-2021. From 2015 to 2020, weighted response rates ranged from 33.7% to 81.3%. 24 Questions on e-cigarette use were first included in PRAMS 2015. Our final analytic sample consisted of 247 537 unweighted observations, which included 243 582 observations with urban–rural designation collected from 2015 to 2020 in 49 jurisdictions.
Because PRAMS data are deidentified and publicly available, analysis of these data does not constitute human subjects research, and we did not have to obtain informed consent. The study was exempt from review by the research ethics boards at the investigators’ institutions (Georgia Southern University and Middle Georgia State University).
Measures
The outcome was a nominal variable that differentiated among women who smoked combustible cigarettes exclusively, used e-cigarettes exclusively, used both tobacco products (ie, dual use), or used neither product during the peripartum period. Smoking and use of e-cigarettes were operationalized by using variables created in the PRAMS dataset, which were based on women’s responses to the 2 questions on use in the past 2 years. The first question asked whether a mother smoked. The second question asked whether a mother had “used any of the following products in the past 2 years.” For each item, the respondent was asked to check “no” if she did not use it or “yes” if she did. One of the items was e-cigarettes and other electronic nicotine products that are battery-powered devices that use nicotine liquid rather than tobacco leaves and produce vapor instead of smoke (eg, vape pens, e-hookahs, hookah pens, e-cigars, e-pipes). If women responded affirmatively to both questions, we categorized them as using both tobacco products.
Our primary exposure of interest was respondents’ residence in an urban or rural county, as reported in PRAMS. The PRAMS variable is based on the 2013 National Center for Health Statistics (NCHS) Urban–Rural Classification Scheme for Counties. 25 This classification scheme contains 6 categories, commonly dichotomized into urban areas (all metropolitan statistical areas, including 4 NCHS categories of urban–metropolitan areas) and rural areas (all nonmetropolitan statistical areas, including micropolitan and noncore counties in the original NCHS categorization). Rural–urban residence is commonly operationalized for rural–urban analysis as a binary variable and is the only geographic variable consistently available across all states (not all states report all 6 NCHS categories). 26
Given previous research, we included several variables that may confound the association between rural–urban residence and tobacco product use: age, race and ethnicity, marital status, education, WIC food receipt (Special Supplemental Program for Women, Infants, and Children), annual household income, trying to get pregnant, body mass index (BMI), previous live birth, alcohol use, and receipt of prenatal care within the first trimester.27-31 For example, previous studies reported lower smoking prevalence among Black women from nonmetropolitan areas when compared with White women from metropolitan areas.3,31 An examination of data from the Kansas WIC program revealed higher rates of smoking among low-income rural pregnant women before, during, and after pregnancy as compared with their high-income urban counterparts. Being aged ≤17 years, Hispanic, a high school graduate, and an urban dweller; having a normal BMI; and having had no live births prior to the current pregnancy were associated with reduced odds of smoking 3 months before pregnancy. 29 The potential confounding variables were self-reported and captured at the time of childbirth.
We also examined whether the prevalence of using various tobacco products changed over time by including year in the adjusted multinomial regression analysis. Rapid market changes and increased use of tobacco and nicotine products among high school students from 2015 to 2020 might have been reflected in the use of these products among young women who had babies. 32
Statistical Analysis
To describe all categorical variables, we calculated weighted proportions and corresponding 95% CIs. To examine crude differences in prevalence of smoking and e-cigarette use by rural–urban residence, we used univariate multinomial logistic regression models. To assess whether additional sociodemographic and health-related characteristics of women with live infants aged 2 to 6 months were confounding rural–urban differences in each outcome, we used multivariable multinomial logistic regressions. To facilitate interpretation of results and comparisons among subgroups of women by type of tobacco product used, we used post hoc contrasts and marginal analyses. 33 Given the high collinearity between annual household income and WIC participation and the high rate of missing data for the former, we used WIC in adjusted analyses. We set significance at α = .05, and all tests were 2-tailed. Statistical analyses were weighted to account for the complex survey design of PRAMS and for nonresponse and were performed with Stata/SE version 17 (StataCorp LLC).
Results
Most US women with live infants aged 2 to 6 months born between 2015 and 2020 were aged 20 to 34 years (77.1%; 95% CI, 76.8%-77.4%), White (69.9%; 95% CI, 69.7%-70.2%), and non-Hispanic (80.7%; 95% CI, 80.5%-81.0%) (Table 1). More than 60% of mothers had completed high school: 27.0% (95% CI, 26.7%-27.3%) had completed an undergraduate degree and 35.8% (95% CI, 35.5%-36.1%) had completed a graduate or postgraduate degree. Fewer than 2 in 3 women were married (61.3%; 95% CI, 61.0%-61.6%) and had a previous live birth (61.1%; 95% CI, 60.8%-61.5%). While 88.2% (95% CI, 88.0%-88.4%) of women neither smoked nor used e-cigarettes peripartum, 5.0% (95% CI, 4.8%-5.1%) smoked combustible cigarettes exclusively, 5.0% (95% CI, 4.8%-5.1%) used e-cigarettes exclusively, and 1.9% (95% CI, 1.8%-2.0%) used both tobacco products peripartum. Approximately 1 in 10 women (10.2%; 95% CI, 9.7%-10.8%) used e-cigarettes alone or in combination with combustible cigarettes. Among them, 41.8% (95% CI, 39.1%-44.6%) used both products peripartum.
Sociodemographic and health-related characteristics of women with live infants aged 2 to 6 months (N = 247 537), overall and by rural versus urban residence, United States, 2015-2020 PRAMS a
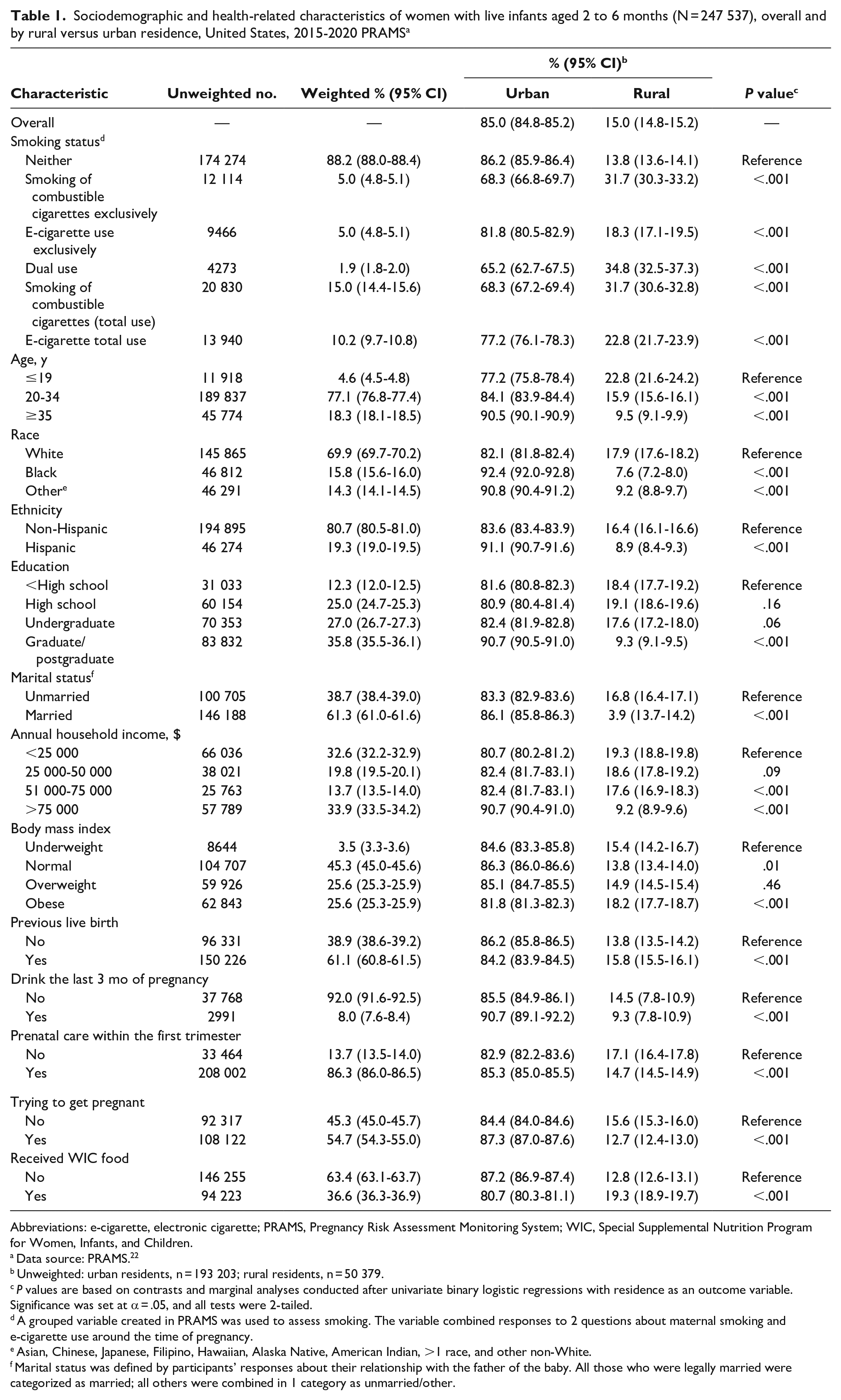
Abbreviations: e-cigarette, electronic cigarette; PRAMS, Pregnancy Risk Assessment Monitoring System; WIC, Special Supplemental Nutrition Program for Women, Infants, and Children.
Data source: PRAMS. 22
Unweighted: urban residents, n = 193 203; rural residents, n = 50 379.
P values are based on contrasts and marginal analyses conducted after univariate binary logistic regressions with residence as an outcome variable. Significance was set at α = .05, and all tests were 2-tailed.
A grouped variable created in PRAMS was used to assess smoking. The variable combined responses to 2 questions about maternal smoking and e-cigarette use around the time of pregnancy.
Asian, Chinese, Japanese, Filipino, Hawaiian, Alaska Native, American Indian, >1 race, and other non-White.
Marital status was defined by participants’ responses about their relationship with the father of the baby. All those who were legally married were categorized as married; all others were combined in 1 category as unmarried/other.
One in 7 mothers lived in rural counties (15.0%; 95% CI, 14.8%-15.2%) (Table 1). Among them, significantly fewer rural women (22.0%; 95% CI, 21.4%-22.6%) had completed a graduate or postgraduate education than urban women (38.3%; 95% CI, 37.9%-38.6%). The percentage of women with other sociodemographic and health-related characteristics differed significantly by residence in rural versus urban counties, except for women who had an annual household income of $25 000 to $50 000 or were overweight.
Based on crude analyses, the use of tobacco products was significantly higher among rural than urban women with live infants aged 2 to 6 months. The prevalence of smoking combustible cigarettes exclusively was 10.4% (95% CI, 9.8%-10.9%), of e-cigarette use exclusively was 5.9% (95% CI, 5.5%-6.3%), and of both products was 4.3% (95% CI, 3.9%-4.7%) among rural women (Table 2). The differences between crude and adjusted estimates of tobacco product use were >10%. In adjusted analyses, rural women were significantly more likely to smoke combustible cigarettes exclusively (6.7%; 95% CI, 6.3%-7.1%) and use both tobacco products (2.6%; 95% CI, 2.3%-2.8%) than urban women (4.5% [95% CI, 4.4%-4.8%] and 1.7% [95% CI, 1.6%-1.8%], respectively; P < .001). We found a significant 0.8 percentage-point difference in adjusted prevalence of exclusive e-cigarette use between rural mothers (4.5%; 95% CI, 4.1%-4.8%) and urban mothers (5.3%; 95% CI, 5.1%-5.5%; P < .001).
Crude and adjusted prevalence of maternal cigarette smoking and e-cigarette use, United States, 2015-2020 PRAMS a
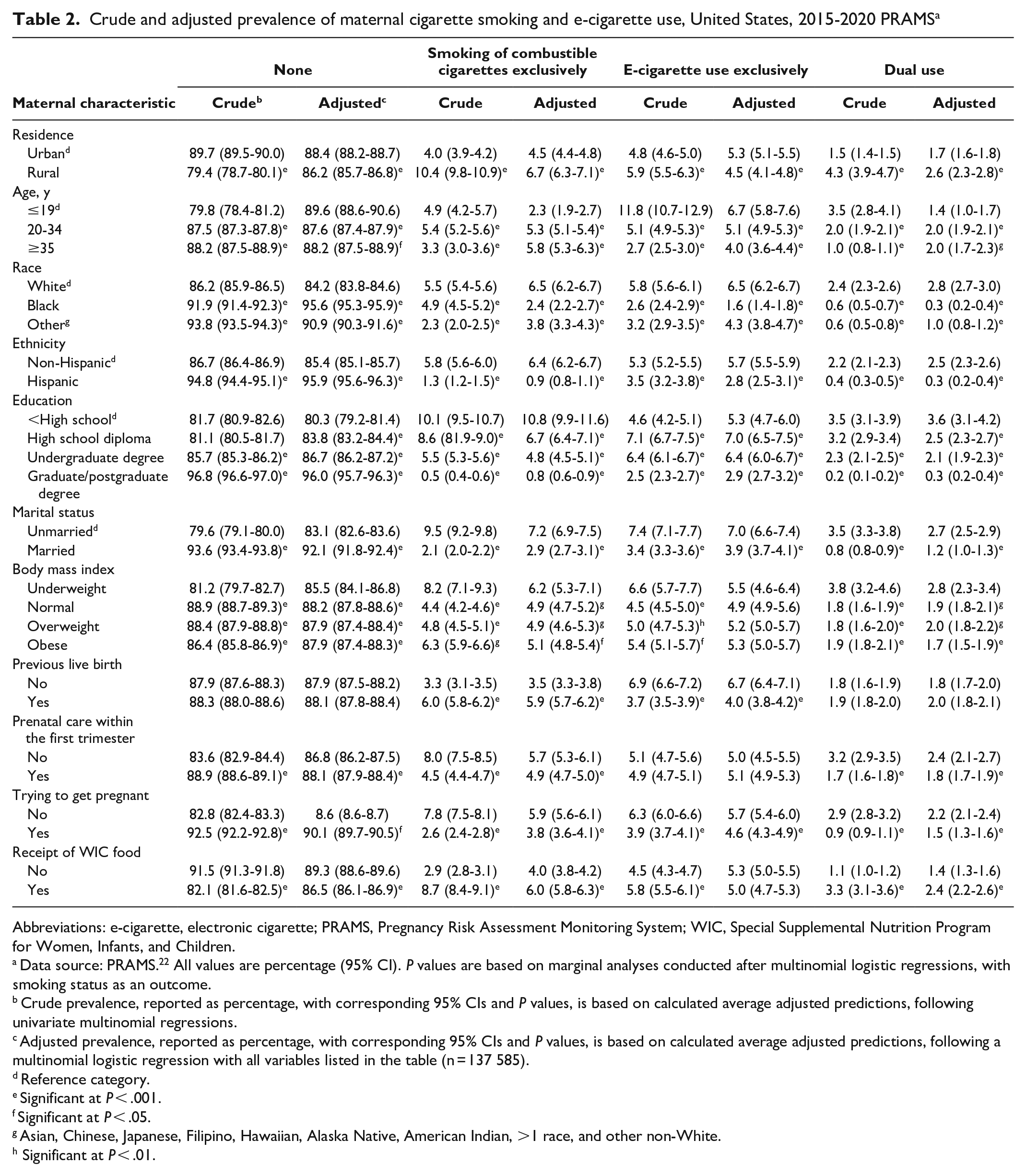
Abbreviations: e-cigarette, electronic cigarette; PRAMS, Pregnancy Risk Assessment Monitoring System; WIC, Special Supplemental Nutrition Program for Women, Infants, and Children.
Data source: PRAMS. 22 All values are percentage (95% CI). P values are based on marginal analyses conducted after multinomial logistic regressions, with smoking status as an outcome.
Crude prevalence, reported as percentage, with corresponding 95% CIs and P values, is based on calculated average adjusted predictions, following univariate multinomial regressions.
Adjusted prevalence, reported as percentage, with corresponding 95% CIs and P values, is based on calculated average adjusted predictions, following a multinomial logistic regression with all variables listed in the table (n = 137 585).
Reference category.
Significant at P < .001.
Significant at P < .05.
Asian, Chinese, Japanese, Filipino, Hawaiian, Alaska Native, American Indian, >1 race, and other non-White.
Significant at P < .01.
We found no significant changes over time, except for significant but clinically small increases in exclusive use of e-cigarettes from 4.2% in 2018 to 5.2% in 2019 (P < .001) and to 6.4% in 2020 (P < .001) and a decrease in the proportion of women who used neither combustible cigarettes nor e-cigarettes from 88.1% in 2019 to 87.1% in 2020 (P = .008).
Discussion
We found differences in sociodemographic and health-related profiles of women by type of tobacco products used. Women who used combustible cigarettes exclusively or used both products had similar sociodemographic and health-related profiles, except for plurality, unlike women who used e-cigarettes exclusively. The distinguishing characteristics were age, level of educational attainment, BMI, plurality, receipt of prenatal care, and receipt of WIC benefits.
The differences in types of tobacco products used are supported by sociodemographic specificities such us living in rural or urban areas and regulatory approaches toward e-cigarettes in the United States.34,35 In our study, after adjusting for sociodemographic characteristics, rurality remained significantly associated with each type of use; however, in terms of public health or clinical significance, the adjusted prevalence of e-cigarette use was comparable for rural and urban women (ie, rounded to 5% for both groups). This comparability could be attributed to the increased accessibility of e-cigarettes due to the widespread distribution of vape shops and the vast online market, including internet-based and on-demand apps for retailers to sell, ship, and deliver tobacco products to consumers. 34 In addition to the widespread availability of e-cigarettes, the lower average cost of vaping has increased the popularity of these devices. 35 In a study based on Universal Product Code retail sales for e-cigarette products from the Nielsen Company, which includes data on sales from convenience stores and all other outlets combined, from 2012 through 2016 e-cigarette unit sales increased significantly for all types of e-cigarette devices, such as rechargeable and disposable devices, disposable cartridges prefilled with e-liquid, and e-liquid bottles for filling reusable cartridges. 36 During the same period, national e-cigarette prices significantly decreased for these product types, except for e-liquids, with increases in price occurring in 5 states and Washington, DC. 36 A study based on NielsenIQ retail scanner data from January 2017 through September 2022 revealed that disposable e-cigarettes had quintupled in volume capacity, nearly tripled in average nicotine strength, and fell an average per-milliliter price of e-liquid by nearly 70%. 35 The advancing online retail landscape and lower costs of e-cigarettes as compared with other tobacco- and nicotine-containing products are likely factors that diminish the effects of characteristics such as economic status, health service shortage, and rurality in terms of geographic isolation.
The lack of perceived health risks attributable to the exclusive use of e-cigarettes has also increased their use, especially among women of childbearing age. E-cigarettes have been marketed as an alternative to help pregnant women quit or reduce the use of tobacco. 37 Research aimed at identifying the perceptions of pregnant women toward e-cigarettes has found that women perceive e-cigarettes to be less harmful than combustible cigarettes.38-41 The marketing and misinformation on the safety of e-cigarettes have led to their increased use. 37 In our adjusted and crude models, women with previous live births were less likely to use e-cigarettes and more likely to use both products than nulliparous women. Prior studies have attributed the switch to e-cigarettes to being viewed as a safer alternative to combustible cigarettes.41,42 In terms of dual use, women may be attempting to convert to e-cigarettes because they mistakenly perceive the devices to be safer than combustible cigarettes. 43 Yet, dual users may be exposed to higher amounts of nicotine and have greater access to nicotine than if they were using either product exclusively. 44 Emerging research in animal studies 45 and the general population, including results from a systematic review, suggests that dual use is at least as harmful, possibly more harmful, than exclusive smoking of combustible cigarettes.46,47
Furthermore, differences by sex in tobacco preferences and reported reasons for smoking have been well established; thus, similar differences by sex may exist for e-cigarettes. Male users are more likely than female users to report vaping for health reasons and to curb addiction to combustible cigarettes, while female users are more likely than male users to vape because of recommendations from family and friends as well as information obtained from advertisements. 16 E-cigarette marketing is not subject to the same restrictions as combustible cigarettes; therefore, e-cigarette companies are permitted to advertise on television and the internet. 34 Tobacco companies have viewed US women as key consumers since the 1920s and have developed products to appeal to women by associating smoking with independence, beauty, and thinness. 16 E-cigarette retailers are applying similar strategies to influence female users with messages claiming that the devices are healthier than combustible cigarettes, helpful for smoking cessation, and permissible for use in smoke-free environments. 44 The targeted marketing and e-cigarette messaging may facilitate increased use of e-cigarettes among women of reproductive age.
Strengths and Limitations
Our study had several strengths and limitations. First, PRAMS data provide a national representative sample and are linked to birth certificates or the actual profiles of the women who delivered live infants, which strengthened the external and internal validity of our results. However, because women’s reports on tobacco products were self-reported, the possibility of information bias cannot be ruled out. Furthermore, because we relied on cross-sectional data, our findings must be interpreted as associative rather than causal: residence in a rural area is one of the contributing rather than causal factors to a woman’s smoking status or use of combustible cigarettes and e-cigarettes.
Conclusion
When compared with urban women, rural women were significantly more likely to smoke combustible cigarettes and use both tobacco products concurrently. Rural women are less likely than urban women to have access to evidence-based tobacco cessation programs. 48 Our study further highlights the importance of applying public health approaches to reducing the urban–rural disparities in prevalence of, recommendations, services, and health outcomes related to tobacco use.
Effects of rural residence on e-cigarette use are significantly confounded by women’s sociodemographic and health-related characteristics. When adjusting for these characteristics, we found no significant differences in the prevalence of e-cigarette use between rural and urban women. Coupled with higher rates of dual use among rural women, a need exists for public health interventions, including restrictions on e-cigarette marketing and educational campaigns tailored to rural women, to help deter women of childbearing age from using any type of tobacco product.
Footnotes
Acknowledgements
The authors thank Cyrille Kouambo Beckodro, MPH, Jiann-Ping Hsu College of Public Health, Georgia Southern University, for his contribution to data management and literature search as a graduate research assistant.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.