
Abstract
Background:
The prevalence of combusted cigarette (CC) smoking among older adults is stagnant, with 0 declines attributable to e-cigarette (EC) use. Given that normative beliefs are associated with quitting and switching to ECs, we assessed cross-sectional associations between age, CC, and EC descriptive and injunctive norms and potential interactions with tobacco use behavior.
Methods:
Data are from people with current, established (≥100 lifetime CCs) CC use (n = 8072) at Wave 5 (2018-2019) of the adult Population Assessment of Tobacco and Health Study. We used adjusted multivariable logistic regressions to model social norms as a function of age (18-24, 25-34, 35-44, 45-54, 55-64, ≥65 years). We also dichotomized age (≥55 vs 18-54) to investigate interactions between age and social norms on past 12-month CC quit attempts and past-month EC use.
Results:
Older age was positively associated with pro- and anti-CC norms and anti-EC norms. Significant interactive effects revealed that being advised to quit smoking by a healthcare provider was more strongly associated with CC quit attempts among adults ≥55 years (adjusted odds ratio [aOR] [95% CI]: 2.12 [1.66, 2.71]) than adults <55 years (aOR: 1.63 [1.34, 2.00]). Reporting people close to you use ECs was also more strongly associated with EC use among adults ≥55 years (aOR: 4.37 [3.35, 5.69]) than among adults <55 years (aOR: 3.43 [2.89, 4.08]).
Conclusions:
This study identified modifiable risk factors for tobacco use that may be particularly beneficial for older adults. Behavioral and communication interventions that target normative beliefs may maximize smoking cessation, or harm reduction when cessation is not possible.
Introduction
Despite declines in combusted cigarette (CC) smoking in all other age groups, CC use among US older adults remains stagnant (2015 prevalence: 17.0% among ages 45-64; 8.4% among ages ≥65 years; 2020 prevalence: 14.9% among ages 45-64; 9.0% among ages ≥65 years).1 -3 Compared to younger adults, adults ages ≥45 years are less likely to make quit attempts, less likely to quit, and more likely to suffer significant negative health effects due to smoking such as cancer, lung disease, and dementia.4 -6 Older adults who are unable to quit smoking CCs are also less likely to switch to using alternative nicotine products that may reduce harm, such as e-cigarettes (ECs). 7 Accordingly, a recent modeling study attributed a 43% to 53% and 11% to 20% decreased CC prevalence among adults ages 18 to 24 and 25 to 44 years, respectively to EC use, but observed no reduction for adults ages ≥45 years. 8
Older adults have unique lived experiences and social environments that may contribute to their tendency toward continuing use of CCs rather than transitioning to ECs. 9 Two types of social norms related to tobacco product use are descriptive norms (beliefs about others’ use of tobacco products) and injunctive norms (beliefs about others’ approval/disapproval of tobacco use). 10 Regardless of age, decades of research demonstrate the importance of these norms to CC smoking. CC smoking is especially influenced by the CC behaviors and beliefs of individuals in close social networks such as family and close friends.11 -13 Additionally, recent research demonstrates similar patterns for ECs. EC use is influenced via social networks, for instance, individuals may be susceptible to ECs if family or friends support ECs as a tool for CC cessation.14,15 While there is minimal current research characterizing these norms among older adults, a 2016 cross-sectional 4-country survey found that adults ages ≥55 years were less likely than younger age groups to report positive descriptive and injunctive EC norms such as close friends using ECs. 16 Other socioenvironmental factors also differ by age: adults ages ≥65 years are less likely to be referred to cessation counseling, prescribed nicotine replacement therapy, or discuss their smoking in healthcare settings.17 -19 There are also lower odds of having a smoke-free home with increasing age.20,21
Importantly, these socioenvironmental factors and normative beliefs may be associated with nicotine product use. In a longitudinal, international study, seeing others use ECs on some days increased the odds of initiating EC use at a later time point. 22 People who smoke CCs who have fewer people in their lives who also smoke have increased odds of high quit motivation. 23 Additionally, people who smoke with stronger descriptive and injunctive social norms against smoking are more likely to have made a quit attempt in the past year. 23 A recent study of adults ages ≥45 years (2015) indicates that older adults who are not seriously considering quitting in the next 6 months are more likely than those seriously considering quitting to believe that friends and family approve of smoking. 24 This study also reports that an interest in trying ECs among older adults is significantly associated with endorsing that friends and family think ECs are acceptable. 24 Longitudinal studies also indicate that smoking cessation advice from healthcare professionals 25 and living in a location with a smoke-free policy 26 is positively associated with quit attempts and smoking cessation.
Despite the influence of social norms on tobacco use, there is limited research focused on older adults or differences across age groups. The current study among people who use CCs in Wave 5 (2018-2019) of the Population Assessment of Tobacco and Health (PATH) Study aims to determine whether the relationship between social norms and (1) past-year CC quit attempts and (2) past-month EC use varies as a function of age. We hypothesize that positive CC social norms will be negatively associated with quit attempts and vice versa, and the relationships will be stronger among older adults. We also hypothesize that positive EC social norms will be positively associated with EC use and vice versa, and that these relationships will likewise be stronger with older age.
Methods
Data Source
Data are from Wave 5 (2018-2019) of the adult PATH Study, a nationally representative, US longitudinal cohort study assessing tobacco use characteristics and health outcomes. 27 The PATH team surveyed participants using computer-assisted personal interviewing and audio computer-assisted self-interviewing. In addition, they obtained informed consent and kept the data confidential. The PATH team previously described all study design and methods elsewhere. 27 Westat IRB originally approved PATH; the current study (performed in 2022-2023) did not require Institutional Review Board (IRB) approval given its use of public-use data. We restricted analyses to n = 8072 adults with current (smoked CCs in the past year and currently smoke regularly) and established CC use (smoked ≥100 lifetime CCs).
Measures
Descriptive Norms
Participants answered, “In general, do you think most people disapprove of smoking cigarettes?” and “. . .disapprove of using e-cigarettes or other electronic nicotine products?” We dichotomized response options into “definitely yes/probably yes” and “definitely not/probably not.”
Injunctive Norms
Participants answered “yes/no” to the question, “Thinking about the people who are important to you, do any of them use any of the following products?” where 2 of the product options were “cigarettes” and “EC or other electronic nicotine products.” Participants also answered, “Thinking about the people who are important to you, how would you describe their views on using tobacco in general?” and we dichotomized response options into “very positive/positive/neither positive nor negative” and “negative/very negative.” 28 Lastly, participants responded to the question, “In the past 12 months, to what extent, if at all, [has/did] the disapproval of close friends and family [led/lead] you to think about quitting?” We dichotomized answers into “somewhat/very much” and “not at all.”
Other Socioenvironmental Factors
Participants responded to the question, “For tobacco products that are burned, such as cigarettes, cigars, pipes, or hookah, which statement best describes the rules about smoking a tobacco product inside your home?” We classified those who indicated “Smoking is not allowed anywhere or at any time inside my home” as individuals with a complete home smoking ban. We classified respondents who indicated either “Smoking is allowed in some places or at some times inside my home” or “Smoking is allowed anywhere and at any time inside my home” as individuals without a complete home smoking ban. Participants who reported seeing a medical doctor, nurse, other health professional, or dentist in the past 12 months responded “yes/no” to the question, “In the past 12 months, did any medical doctor, dentist, or other health professional advise you to stop using tobacco, [including e-cigarettes or other electronic nicotine products]?”
Age
The public-use PATH dataset included age as a categorical variable with the following options: 18 to 24, 25 to 34, 35 to 44, 45 to 54, 55 to 64, or ≥65 years. In dichotomized analyses, we collapsed age categories into 18 to 54 and ≥55 years.2,29
Quit Attempts
Participants reported their most recent CC quit attempt, if any. We classified participants with quit attempts within the past 12 months as such, and we classified participants with no reported quit attempts or quit attempts greater than 12 months ago as having no quit attempts within the past 12 months.
Covariates
Included covariates were sex (male/female), race/ethnicity (non-Hispanic White/non-Hispanic Black/Hispanic/non-Hispanic other), education (less than high school degree/high school degree or greater), self-reported physical health (1-5 continuous, where 1 = excellent and 5 = poor), and smoking status (daily/non-daily).
Statistical Analysis
We conducted analyses using Stata 17 30 with alpha set to .05. We used recommended survey procedures, sampling weights, and variance estimation with Fay = 0.3 such that the data were representative of the noninstitutionalized, civilian US population during 2018 to 2019.31,32
We collapsed social norms into dichotomous measures and identified the “negative” response to each social norm item (ie, definitely not/probably not) as the reference value. The first set of models assessed the association between age and social norms, utilizing all 6 categories of age. Multivariable logistic regression models included age as the independent variable and each social norm as the dependent variable. We adjusted all models for the following covariates: race/ethnicity (ref: non-Hispanic White), sex (ref: male), education (ref: high school or greater), self-reported health, and smoking status (ref: daily). In addition, we calculated the weighted prevalence of each social norm for each of the 6 age groups.
Next, we dichotomized age into older (ie, ≥55 years) versus younger (ie, 18-54). Because of our central hypotheses, we created weighted, multivariable logistic regression models to identify the relationships between social norms (independent variable) and (1) past 12-month CC quit attempts, and separately (2) past 30-day EC use (dependent variable), including the interaction term age. If interaction terms were not significant, we removed them, and retained age in the models as a covariate. We adjusted all models for the same covariates as above.
Results
Out of 8072 adults reporting current established smoking, 74.1% (5,985) were ages 18 to 54 and 25.9% (2087) were ≥55 years. Other demographics and smoking-related characteristics by CC quit attempt status and EC use status are reported in Tables 1 and 2.
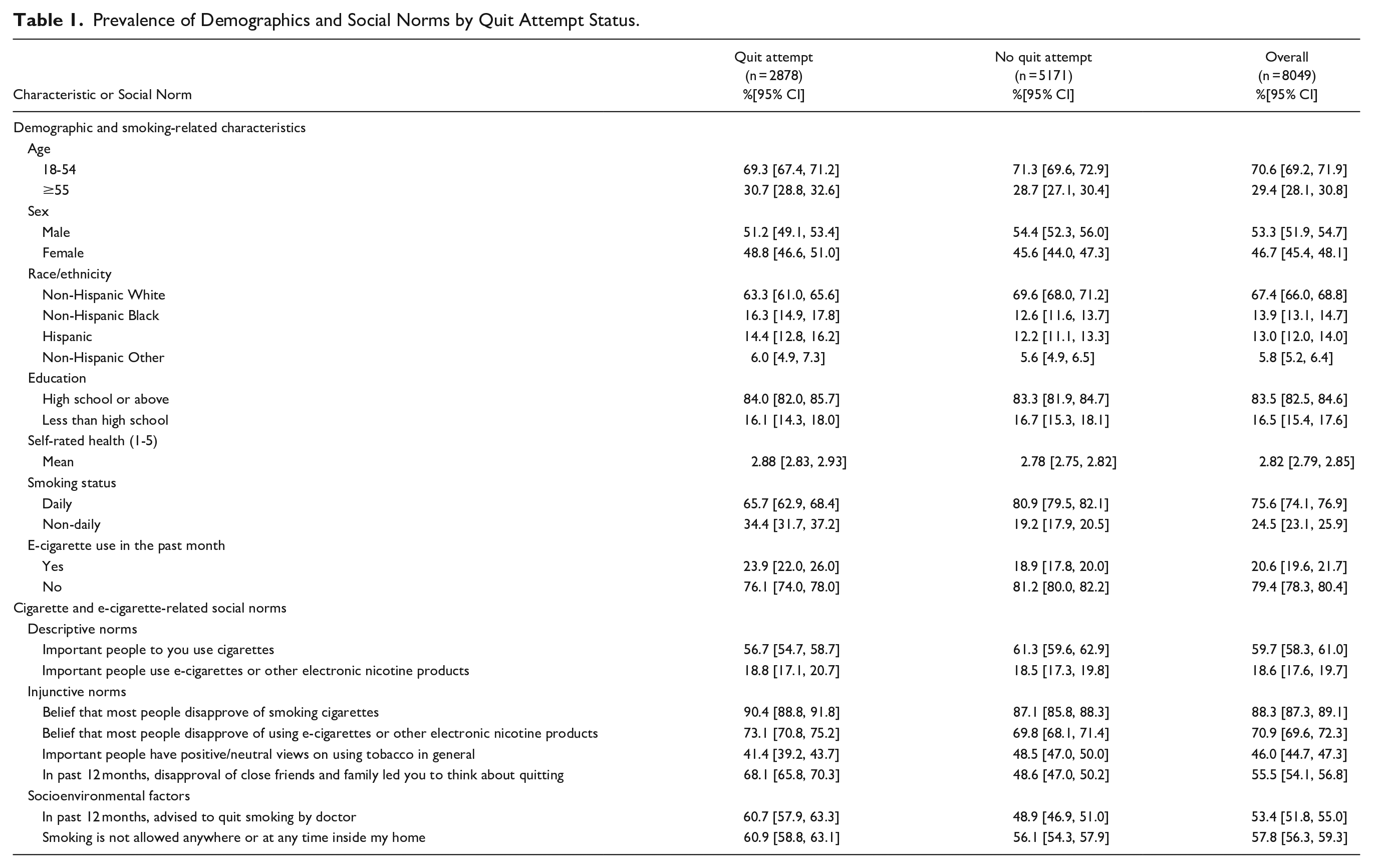
Prevalence of Demographics and Social Norms by Quit Attempt Status.
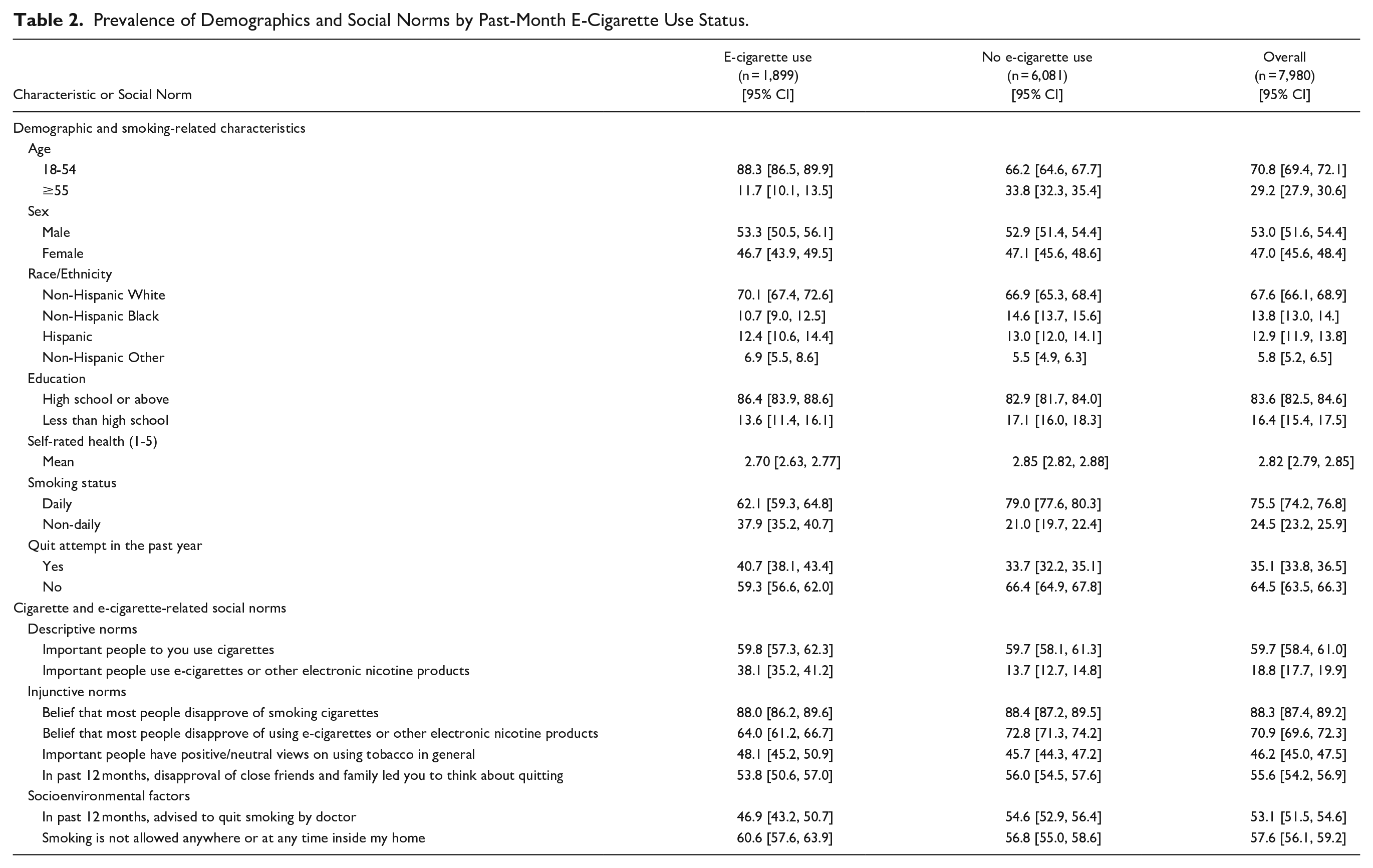
Prevalence of Demographics and Social Norms by Past-Month E-Cigarette Use Status.
Descriptive Norms
Among adults <55 years, the percentage who reported people who are important to them use CC (60.1%) was greater than the percentage who reported people who are important to them use ECs (20.2%; P < .001). In addition, among adults ≥55 years, the percentage who reported people who are important to them use CCs (58.5%) was greater than the percentage who reported people who are important to them use ECs (14.8%; P < .001).
Compared to those aged 18 to 24, being aged ≥35 years was negatively associated with reporting that people important to you use CCs (see Table 3 for models; see Supplemental Table 1 for covariates; see Supplemental Table 3 for prevalence of norms by age group). Adults ≥25 years were also less likely to report that people important to them use ECs, with the largest effects observed among people ages 55 to 64 (adjusted odds ratio [aOR] = 0.47, P < .001) and ages ≥65 years (aOR = 0.52, P < .001).
Age Terms for Adjusted Multivariable Logistic Regression Models With Outcome of Cigarette/E-Cigarette Social Norms (n = 8072).
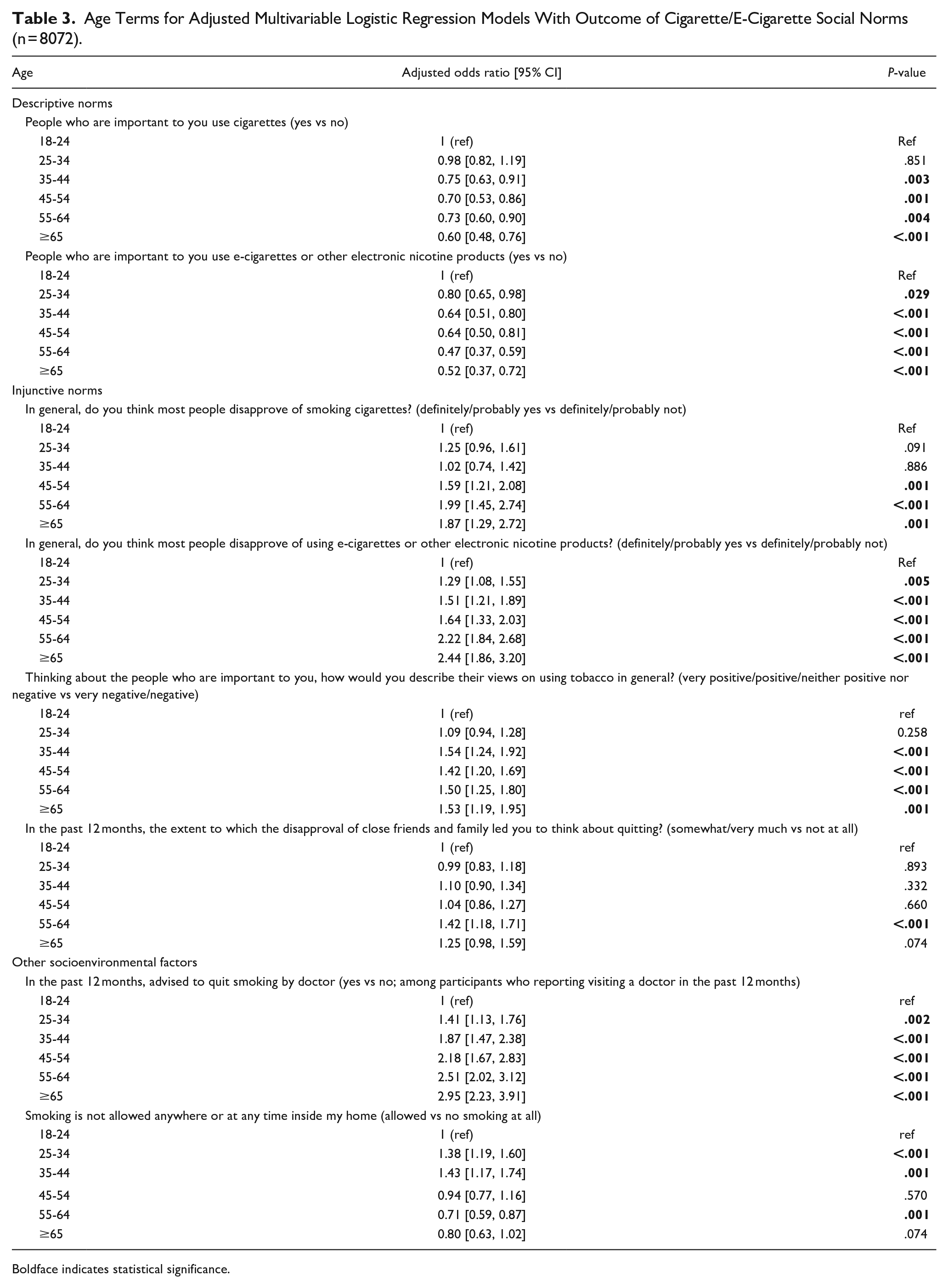
Boldface indicates statistical significance.
Injunctive Norms
Among adults <55 years, the percentage who thought most people disapprove of smoking CCs (86.8%) was greater than the percentage who thought most people disapprove of using ECs (68.2%; P < .001). In addition, among adults ≥55 years, the percentage who thought most people disapprove of smoking CCs (91.7%) was greater than the percentage who thought most people disapprove of using ECs (77.5%; P < .001).
Being ≥45 was positively associated with reporting that most people in general disapprove of smoking CCs (see Table 3 and Supplemental Tables 1 and 2). Additionally, adults ≥25 years were more likely than those who are 18 to 24 to report that most people in general disapprove of using ECs, with those ≥55 being more than twice as likely (ages 55-64: aOR = 2.22; ages ≥65: aOR = 2.44, P’s < .001) to report perceived disapproval.
Adults ≥35 years were more likely than adults who are 18 to 24 to report that people important to them have positive or neutral views on tobacco use (P’s ≤ .001). Adults ages 55 to 64 were also more likely than adults ages 18 to 24 to report that friends/family disapproving of CCs led them to think about quitting smoking CCs (P < .001).
Other Socioenvironmental Factors
Among individuals who visited a healthcare provider in the past year (39.3%; n = 3171), odds of being advised to quit smoking by a healthcare provider were significantly higher among those aged ≥25 compared to those aged 18 to 24 (see Table 3 and Supplemental Tables 1 and 2). The largest effect was observed among people ages ≥65 versus 18 to 24 (aOR = 2.95, P < .001). Additionally, adults ages 55 to 64 were less likely than adults ages 18 to 24 to report a home smoking ban (P = .001).
Interactions of Age and Norms on Tobacco Use
Among individuals who visited a healthcare provider in the past year, being advised to quit smoking was positively associated with having a past-year CC quit attempt (P = .032), and this relationship was stronger among adults ≥55 (aOR: 2.12) than adults <55 (aOR: 1.63); see age stratified effects columns in Table 4 and covariates in Supplemental Table 2. Reporting that people important to you use ECs was positively associated with past month EC use (P = .035), and this relationship was stronger among adults ≥55 (aOR: 4.37) than adults <55 (aOR: 3.43).
Main Effects of Social Norms on Tobacco Use Outcomes and Interactions With Age (n = 8072).
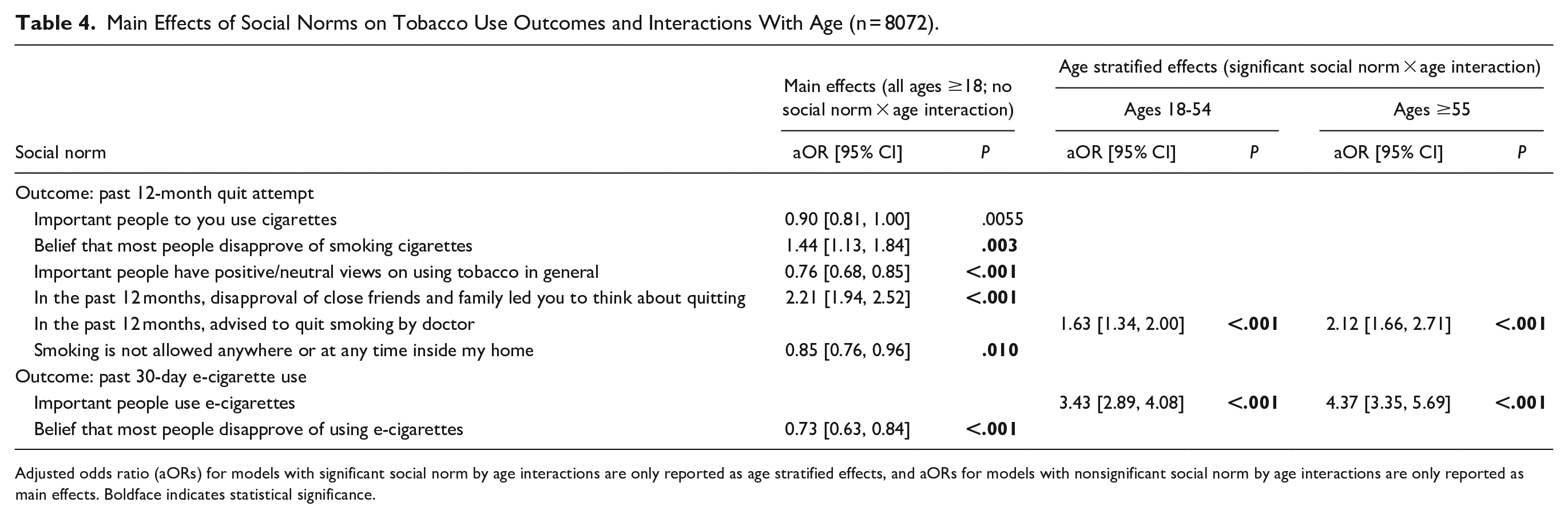
Adjusted odds ratio (aORs) for models with significant social norm by age interactions are only reported as age stratified effects, and aORs for models with nonsignificant social norm by age interactions are only reported as main effects. Boldface indicates statistical significance.
Main Effects of Social Norms on Tobacco Use
Significant main effects of injunctive norms on past-year CC quit attempts were observed such that past 12-month quit attempts were positively associated with believing that people in general disapprove of CCs, family/friends disapproving of CCs, important people having negative views about tobacco, and home smoking bans (see main effects columns in Table 4 and covariates in Supplemental Table 2). Additionally, a significant main effect in the model of believing people in general disapprove of ECs suggested that this injunctive norm was negatively associated with past-month EC use.
Discussion
This analysis sought to investigate associations of social norms related to tobacco use with age. As hypothesized and consistent with prior research,16,24 older age was associated with positive and negative norms related to CCs and negative norms related to ECs. Reporting that important people use ECs was associated with past-month EC use, especially among adults ≥55. Furthermore, cessation advice was more likely among adults ≥55 and associated with quit attempts, while home smoking bans were less likely. As previous research emphasizes the importance of social norms in tobacco use behavior, this study indicates specific differences in normative beliefs between older and younger adults that are essential to address via behavioral and communication interventions to decrease age-related disparities.
Adults over 35 being less likely to report CC use among important people is consistent with the documented negative association between CC prevalence and age. 1 Likewise, the association of older age with positive tobacco views in this study is consistent with greater tobacco health risk misperceptions among adults with increasing age. 33 Consistent with prior work, older age was associated with being less likely to report important people use ECs. 16 However, adults (especially adults over 55 years) who reported EC use by important people were more likely to have used ECs in the past month. Since past-month EC use may serve as a proxy for “trying” ECs among adults who smoke, this is also consistent with research showing that endorsing family/friends’ approval of ECs is associated with an interest in trying ECs among adults over 45 years. 24 While the current study cannot discern reasons for EC use, and multiple tobacco product use (ie, substitution vs complementarity) 34 is a possibility, results may also indicate that adults may be differentially interested in switching from CC to EC depending on age and social norms.
Older age was positively associated with believing that people in general disapprove of smoking CCs and with believing that people disapprove of using ECs. These findings are in contrast with decreased CC risk perceptions but in line with the descriptive norms described above and lower prevalence of CC use with increasing age. 1 The EC norms findings are in parallel with increased EC risk perceptions with increasing age. 33 In an international survey, respondents with increasing age were less likely to perceive that society approved of ECs. 16 Potential reasons for the observed anti-CC and anti-EC norms with increasing age may stem from longstanding exposure to anti-smoking messages, increased stigma associated with smoking, and increased smoking regulation (eg, indoor smoking bans), along with concerns regarding newer products such as ECs. 9 Interestingly, older age was positively associated with reporting disapproval of family/friends led to thoughts about quitting smoking. Social support is a factor associated with smoking cessation in previous studies, with gender as a potential moderator.35,36 These results suggest that age should be further investigated as a potential moderator in this relationship.
Consistent with prior research, adults who visited a healthcare provider were more likely to have received quit advice with increasing age. 37 Advice to quit was positively associated with past-year CC quit attempts, with a stronger effect among adults over 55. These results indicate a potential future avenue to reduce age-related tobacco use disparities, given that longitudinal results indicate that receiving quit advice from a health professional is positively associated with subsequent quit attempts. 25 While quit advice seems to be a major driving factor, there may also be other factors contributing to this difference, such as age-related differences in prevalence of medical conditions associated with provider advice to quit (eg, cancer, chronic obstructive pulmonary disease, heart disease). Additionally, as demonstrated in prior research, older age was negatively associated with home smoking bans.20,21 Smoke-free homes are longitudinally associated with increased subsequent smoking cessation among adults who smoke and decreased relapse among adults who quit. 26 These age differences in socioenvironmental factors indicate that home smoking bans and provider advice to quit should be promoted to encourage CC cessation.
Limitations
Strengths of the study include leveraging a US nationally representative sample. The primary limitation of this study is that it is cross-sectional. As a next step, longitudinal relationships between social norms and tobacco use patterns and the role of age should be examined. Past-year CC quit attempts and past-month EC use as used in this study acted as proxies for potential trajectories of tobacco use but we did not assess reasons for these behaviors in this study. While the social norm questions were largely comprehensive, we were unable to use this dataset to assess more specific questions, such as those relating to specific numbers of friends or family who smoke and partner smoking behaviors and beliefs. Finally, the analysis focused on age as an effect modifier and did not explore heterogeneity in the data further by other characteristics of people who smoke. Future studies examining the moderating role of race and cultural identity are therefore also recommended.
Conclusions
Social norms about CCs and ECs differ by age, with older age generally associated with both positive and negative norms related to CCs and negative norms related to ECs. Socioenvironmental factors such as healthcare provider advice and home smoking bans are associated with both tobacco use behavior and age, suggesting that further emphasis on these factors can further improve clinical outcomes. Communication interventions would also be helpful to correct misperceptions and normative beliefs about tobacco products. A social norms communications campaign approach, for instance, could be developed to increase perceptions of approval of EC among adults ≥55 by their peers, making them more likely to consider switching from CCs. Social norms should continue to be evaluated and addressed, especially as the tobacco regulatory environment changes, leading to even larger disparities related to age, gender, socioeconomic status, disability, and more.
Supplemental Material
sj-docx-1-saj-10.1177_29767342231210554 – Supplemental material for Differences in Normative Beliefs and Tobacco Product Use by Age Among Adults Who Smoke: Cross-Sectional Analysis of a Nationally Representative Sample
Supplemental material, sj-docx-1-saj-10.1177_29767342231210554 for Differences in Normative Beliefs and Tobacco Product Use by Age Among Adults Who Smoke: Cross-Sectional Analysis of a Nationally Representative Sample by Dana Rubenstein, BA, Dana M. Carroll, PhD, MPH, Rachel L. Denlinger-Apte, PhD, MPH, Jennifer Cornacchione Ross, PhD and F. Joseph McClernon, PhD in Substance Abuse
Footnotes
Acknowledgements
The authors acknowledge Lauren R. Pacek, PhD for her contributions to analyses. We also thank PATH participants for their time and effort.
Author Contributions
DR: Conceptualization, formal analysis, writing—original draft, writing—review and editing; DC: writing—review and editing; RD-A: Conceptualization, writing—review and editing; JR: Conceptualization, writing—reviewing and editing; FM: Conceptualization, writing—reviewing and editing, supervision.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is based upon work supported by the National Institutes of Health [grant numbers TL1TR00255 and K01MD014795]. Supporting organizations had no further role in the study design; in the collection, analysis, and interpretation of data; in the writing of the report; or in the decision to submit the article for publication.
Compliance,Ethical Standards,and Ethical Approval
Institutional Review Board’s approval was not required.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.