
Abstract
Objectives:
COVID-19–related stay-at-home orders (SAHOs) created an immediate physical barrier between children and professionals such as pediatricians and teachers, who are often first to identify and report signs of child maltreatment. Our objective was to determine how the SAHO in a southern state was associated with reports of child maltreatment and whether this association was modified by sociodemographic characteristics.
Methods:
We linked data on reports of child maltreatment from a southern state in the United States from October 1, 2018, through September 30, 2020, to data from the US Census Bureau to obtain data on county-level socioeconomic characteristics. We fit a segmented regression model to evaluate changes in reports before and after the SAHO, March 20, 2020. We evaluated potential disparities by child age, case and allegation severity, and socioeconomic characteristics.
Results:
Of 374 885 hotline calls, 276 878 (73.9%) were made before the SAHO and 98 007 (26.1%) after it. Although an immediate decrease in reports of child maltreatment occurred on the day of the SAHO, the rates of reporting within socioeconomic groups started increasing thereafter. While we found no significant change in the overall rate of change in hotline calls after versus before the SAHO (0.23; 95% CI, −0.11 to 0.58), stratified analyses indicate that the rates at which reporting increased varied by education level, health insurance coverage, median annual household income, and unemployment.
Conclusions:
Evaluating these trends is important for policy makers and practitioners to understand how policies enforced during the pandemic influence child maltreatment reporting and how these policies may affect reporting differently across socioeconomic groups.
Child maltreatment is a serious public health issue and has major consequences for individuals, families, and society as a whole. 1 Every year, 1 in 10 children are neglected or psychologically abused, and 4% to 16% are physically abused in high-income countries such as the United States. 2 In the United States alone, >3 million referrals are received annually that involve >6 million children. 1 Child maltreatment is determined by complex factors related to individuals, families, communities, and cultures. 3 It has lifelong cascading effects on children, negatively altering current and future physical and mental health, education, work, social relationships, and violent behavior. 2 Child maltreatment also imposes an economic burden on individuals and society. Among individual victims of child maltreatment, per-victim lifetime costs can vary from $210 012 to $16.6 million. 4 About $80.3 billion each year is spent in the United States in direct and indirect costs related to cases of child abuse or neglect. 1
Child-level outcomes can be affected by broader societal structures.5 -7 Economic factors in the household may directly and indirectly affect child and family health outcomes.7-12 Specifically, greater rates of poverty, lower incomes and education levels, and higher unemployment have been positively associated with rates of child maltreatment at the community level.8,9,13-20 In addition, lower rates of health insurance in a community have been found to increase the risk of a child being placed into out-of-home care. 21 Other socioeconomic characteristics of a community related to economic disadvantages, such as the percentage of female-headed households, have been positively associated with rates of child abuse and maltreatment.8,10,19,20,22-25
Reports of child maltreatment come in many forms. The 1974 Federal Child Abuse Prevention and Treatment Act requires some individuals to be mandatory reporters of child maltreatment. 26 The list in each state may vary, although the most common groups required to report child maltreatment include social workers, school personnel, health care workers, mental health professionals, child care providers, medical examiners or coroners, and law enforcement officers. In some states, all people are required to report suspected abuse or neglect, regardless of profession. 26 Reporting behavior among professionals versus nonprofessionals can vary, given that each group of potential reporters is involved in different aspects of a child’s life. 27 While institutions such as schools have clear internal policies and procedures for reporting and handling maltreatment, 26 reporting among the general population is less structured and may be influenced by the relationship to the child or family, community context, perceived level of collective community efficacy, personal experiences with child maltreatment, ethnicity, and culture, among others.27 -30 In 2019, 21.0% of all reported child maltreatment in the United States was reported by education personnel; 19.1% by legal and law enforcement personnel; 16.3% by social services or mental health personnel; 15.3% by parents, friends, neighbors, or other relatives; and 11.0% by medical personnel. 31
By the end of 2020, the COVID-19 pandemic was the leading cause of death in the United States 32 and was associated with increased economic uncertainty among families and societies, 33 higher unemployment rates, 34 and greater perceived parental stress, 35 all of which are known risk factors for child maltreatment. 36 In addition, COVID-19–related stay-at-home orders led to social isolation for children and families, 37 creating an immediate physical barrier between children and the most common mandatory reporters of child maltreatment during a time of heightened risk of maltreatment.
The negative impact of COVID-19 on child maltreatment reporting has been documented in Australia, 38 Brazil, 39 Japan, 40 South Africa, 41 the United Kingdom, 42 France, 43 Mexico, 44 and Korea, 45 among others. 46 Major cities such as New York City 47 and Los Angeles, California, 48 saw a decrease in child maltreatment reporting after stay-at-home orders, as did states such as Florida, 49 California, 50 Colorado, 51 North Carolina, 52 and Georgia. 53 The impact of COVID-19 stay-at-home orders on child maltreatment reporting has been investigated by reporter type,51,54 race, 54 maltreatment type, 54 and association to allegations of domestic violence. 50
Social determinants of health should not be ignored while conducting COVID-19 policy–related research. 55 However, to our knowledge, no study has evaluated the impact of COVID-19–related stay-at-home orders on child maltreatment or disproportionality with socioeconomic characteristics. We evaluated whether the stay-at-home order during the COVID-19 pandemic resulted in a significant change in the number and rate of change in reports of child maltreatment, focusing on differences related to socioeconomic characteristics such as income, poverty, unemployment, education, health insurance, and head of household.
Methods
Data Sources and Study Population
We used administratively collected data on child maltreatment allegations (also referred to as hotline call data) from a southern state in the United States during the 2-year period from October 1, 2018, through September 30, 2020 (N = 374 885 calls). Reports were made to trained case managers by calling a statewide hotline when child abuse and neglect were suspected. The data included variables such as child age (<5, 5-9, 10-14, 15-17, ≥18 y), allegation and case severity (severe, not severe), and county where the call occurred. Allegation severity was determined by the case manager who received the call. Each case was then assigned to a specific assessment or investigation group where the case severity was then confirmed. We merged data from the US Census Bureau’s American Community Survey from 2018 to 2020 to hotline call data at the county level to obtain data on socioeconomic characteristics. 56 The Vanderbilt University Institutional Review Board (#212114) and the state Department of Children’s Services Review Board reviewed and approved this study. The Vanderbilt Institutional Review Board determined that the study posed minimal risk to participants and met criteria for exempt review per 45 CFR 46.104(d)(4)(ii). The state requested that it not be identified; thus, we omitted this information from the article.
The primary outcome for our analysis was 7-day moving average of the number of hotline calls. County-level socioeconomic characteristics obtained from US Census data included the median annual household income and the percentage of households below the federal poverty level, total population unemployed, college-educated residents, female-headed households, and residents with private or public health insurance. All categories were adopted from published standards of the Harvard Public Health Disparities Geocoding Project if available. 57 No recommended cutoffs for percentage of total population unemployed were found in the literature, so we grouped it by quintiles across all counties. We chose these socioeconomic characteristics a priori according to subject matter knowledge and existing literature on child maltreatment risk factors.8,13,15,16,21 While individual child demographic information such as race may also be associated with child maltreatment,54,58 the data source used in this study did not include that information; therefore, we did not include race as a study variable.
Data Analysis
We conducted a segmented regression analysis for an interrupted time series to model trends in hotline calls before and after March 20, 2020, the day of the statewide stay-at-home order due to COVID-19. The analysis model included report date, indicator for statewide stay-at-home order (before vs after), and an interaction between the date and the indicator. We used model results to estimate the average number of hotline calls and corresponding 95% CIs on the day before and the day of the stay-at-home order. We determined significant differences in these 2 values by fitting a corresponding model with a centered report date and by examining the significance of the coefficient on the indicator for statewide stay-at-home order at the α = .05 level (eTable in Supplemental Material). We also examined the rate of change in hotline calls before versus after the stay-at-home order, represented by the model coefficient on the interaction term. If the coefficient was significant (ie, the 95% CI for the coefficient did not include 0), we determined the rate of change to be significant at the α = .05 level. Additionally, to examine potential disparities, we stratified models by the following variables: case severity, allegation severity, and child age, as well as, at the county level, median annual household income and percentage of households below the federal poverty level, total population unemployed, college-educated residents, female-headed households, and residents with private or public health insurance. We created displays of piecewise segments to visualize trends of the average number and change of rate of calls before and after the stay-at-home order overall and by case severity, allegation severity, child age, and socioeconomic characteristics. We used R version 4.0.3 (R Core Team) for all analyses.
Results
From October 1, 2018, through September 30, 2020, a total of 374 885 hotline calls were made: 276 878 (73.9%) before the statewide stay-at-home order on March 20, 2020, and 98 007 (26.1%) after it (Table 1). On average, 3702 and 3224 calls per week were being made before and after the stay-at-home order, respectively. The median (IQR) child age decreased from 8.0 (3.0-12.0) to 7.0 (3.0-12.0) before and after the stay-at-home order, while the mean (SD) child age decreased from 7.9 (5.1) to 7.6 (5.2). The percentage of severe allegations increased from 9.3% to 10.3%, while the percentage of severe cases increased from 14.3% to 16.7% before and after the stay-at-home order.
Characteristics of hotline calls to report allegations of child maltreatment before and after stay-at-home orders during the COVID-19 pandemic, on March 20, 2020, in a southern state in the United States, October 1, 2018, through September 30, 2020 a

Data sources include administratively collected data on child maltreatment allegations for information on case severity, allegation severity, and age of child, as well as the US Census Bureau American Community Survey from 2018 to 2020 for information on county-level socioeconomic characteristics. 56
Day-to-day variability in average hotline calls decreased after the stay-at-home order, with the SD decreasing from 147 to 100. Piecewise segments suggest that the average number of hotline calls tended to decrease on the day of the stay-at-home order as compared with the day before, while the change in rate of calls increased after the stay-at-home order overall (Figure 1B) and by case severity, allegation severity, child age, and socioeconomic characteristics (Figure 2).
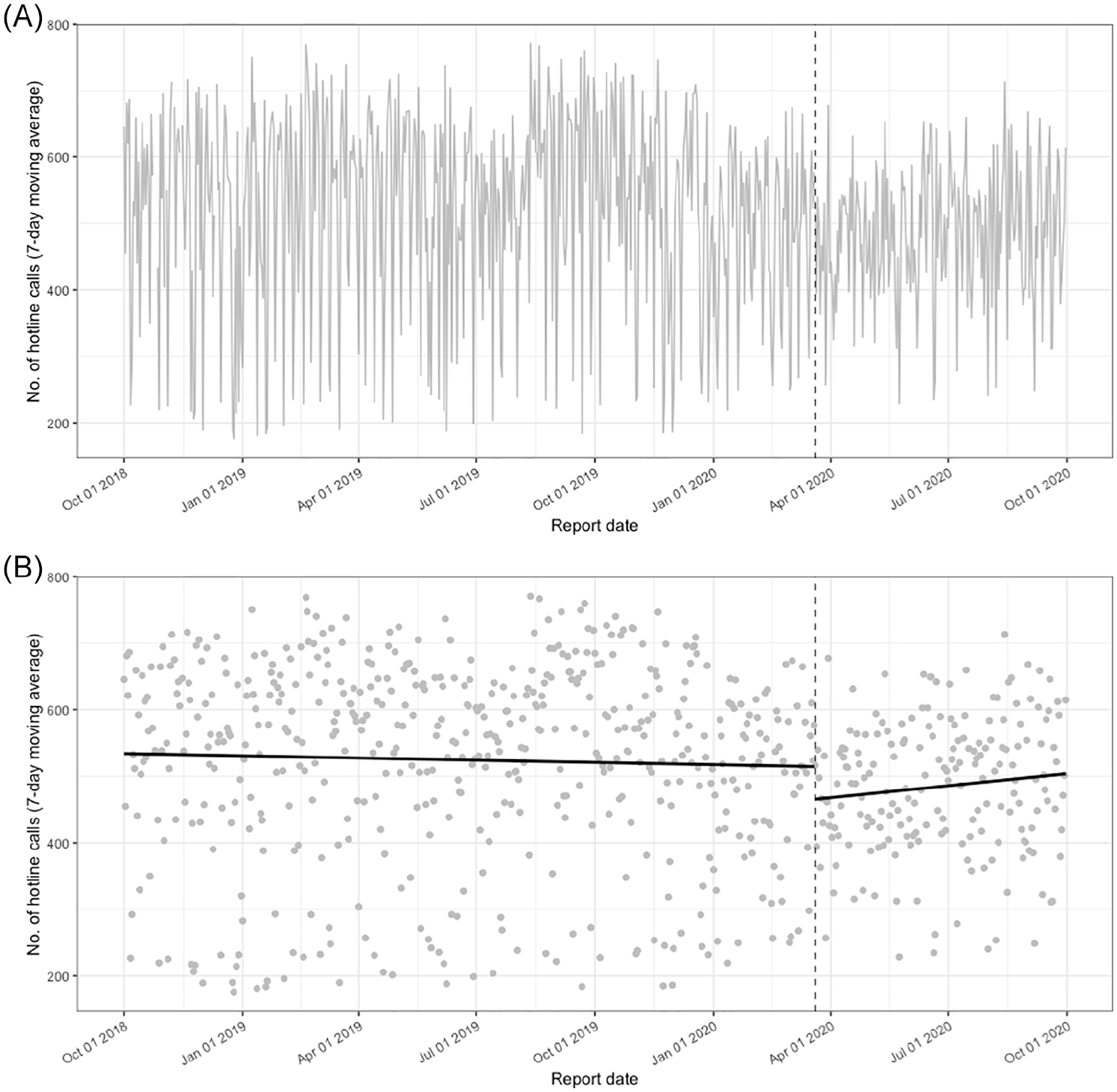
Trends and variability in 7-day moving average of hotline calls for child maltreatment allegations (A) and segmented regression graph with piecewise segments (B) before (SD = 147) and after (SD = 100) stay-at-home orders during the COVID-19 pandemic, from October 1, 2018, through September 30, 2020, in a southern state in the United States. The dashed vertical line indicates the first day of the statewide COVID-19 stay-at-home order on March 20, 2020. Data source: administratively collected data on reports of child maltreatment from a southern state in the United States.
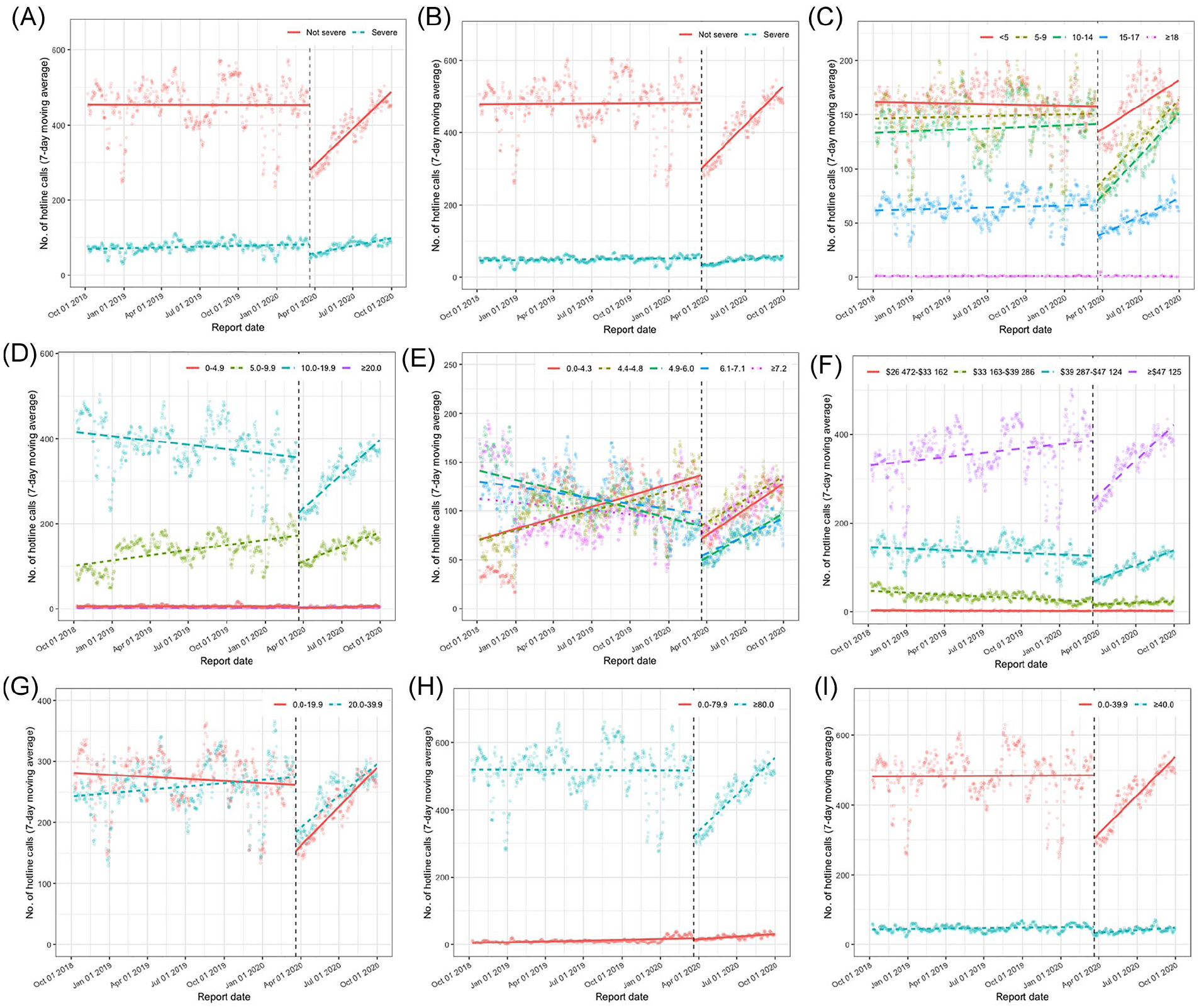
Segmented regression graph with piecewise segments by case severity (A), allegation severity (B), age of child (C), county-level percentage of households below the federal poverty level (D), county-level percentage of total population unemployed (E), county-level median annual household income (F), county-level percentage of female-headed households (G), county-level percentage of residents with private or public health insurance (H), and county-level percentage of college-educated residents (I) from October 1, 2018, through September 30, 2020, in a southern state in the United States. The dashed vertical line indicates the first day of the statewide COVID-19 stay-at-home order on March 20, 2020.
We found a significant difference between the overall average number of hotline calls on the day of the stay-at-home order (March 20, 2020) (466; 95% CI, 428-505) and the day before (March 19, 2020) (509; 95% CI, 486-532). We also found a significant drop in the average number of hotline calls on the day of the stay-at-home order across all variable categories, except among those who were aged ≥18 years, those who resided in a county with a median annual household income of $26 472-$33 162, and those who lived in a county in which ≥20% of the households lived below the federal poverty level (Table 2). Despite these decreases, after 6 months the number of hotline calls eventually reached the levels seen before the stay-at-home order.
Estimated average number of hotline calls to report allegations of child maltreatment before and on the day of a statewide stay-at-home order during the COVID-19 pandemic in a southern state in the United States, March 2020 a
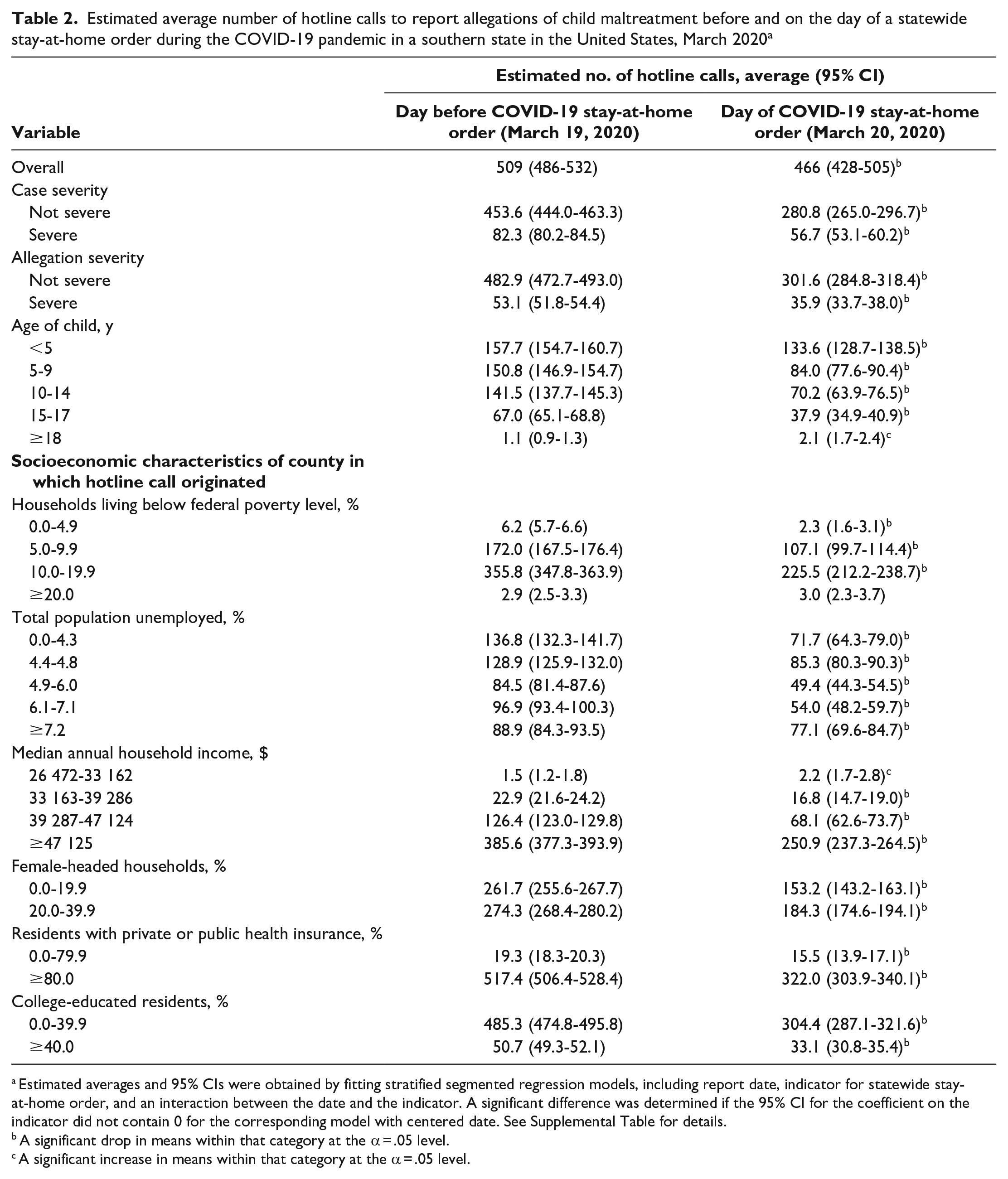
Estimated averages and 95% CIs were obtained by fitting stratified segmented regression models, including report date, indicator for statewide stay-at-home order, and an interaction between the date and the indicator. A significant difference was determined if the 95% CI for the coefficient on the indicator did not contain 0 for the corresponding model with centered date. See Supplemental Table for details.
A significant drop in means within that category at the α = .05 level.
A significant increase in means within that category at the α = .05 level.
We found no significant change in the overall rate of change in hotline calls after versus before the stay-at-home order (0.23; 95% CI, −0.11 to 0.58) (Table 3). Stratified analyses indicated a significant increase in the rate of change in hotline calls after the stay-at-home order among all variables, except among those who resided in a county in which ≥20% of the household lived below the federal poverty level or a county with a median annual household income of $26 472-$33 162. This finding indicates a faster increase in the day-to-day change in hotline calls after the stay-at-home order (vs before) in all other groups. We observed the rate of change in hotline calls to differ most notably among groups in the following variables: case severity, allegation severity, percentage of county with college-educated residents, percentage of residents with private or public health insurance, and median annual household income. The rate of change in average hotline calls increased with median annual household income and percentage of residents with private or public health insurance and decreased with case severity, allegation severity, and percentage of county with college-educated residents. The rate of change in average hotline calls increased with the percentage of the population unemployed, albeit not as strongly as other socioeconomic characteristics.
Estimated change in rate of hotline calls to report allegations of child maltreatment in a southern state after a statewide COVID-19 stay-at-home order on March 20, 2020, versus before the stay-at-home order, stratified by case severity, allegation severity, age, and socioeconomic characteristics a
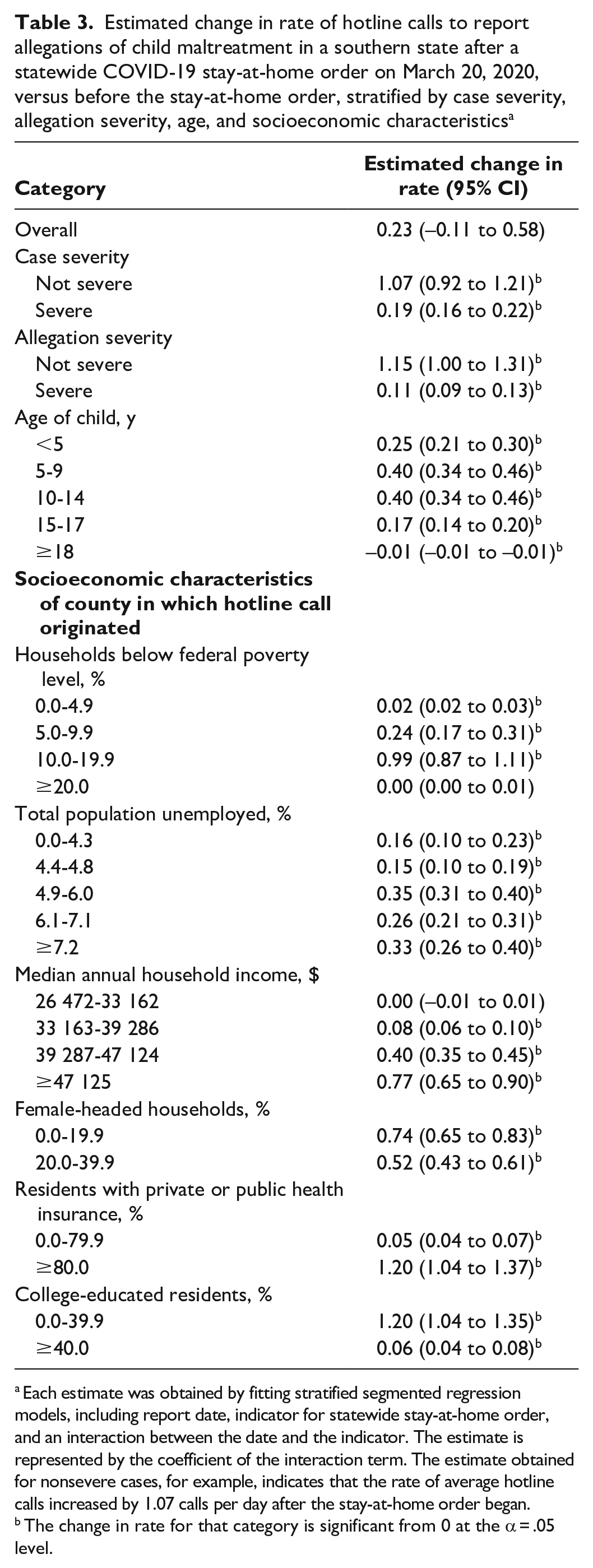
Each estimate was obtained by fitting stratified segmented regression models, including report date, indicator for statewide stay-at-home order, and an interaction between the date and the indicator. The estimate is represented by the coefficient of the interaction term. The estimate obtained for nonsevere cases, for example, indicates that the rate of average hotline calls increased by 1.07 calls per day after the stay-at-home order began.
The change in rate for that category is significant from 0 at the α = .05 level.
Discussion
We used data from a southern state in the United States to examine changes in the trend in hotline calls before and during the COVID-19–associated stay-at-home order across various age groups, allegation severity, case severity, and socioeconomic characteristics. We found that despite an immediate decrease in the average number of hotline calls on the day of the stay-at-home order, the rate of change after the order increased across all socioeconomic groups and case and allegation severity. The rates at which reporting increased varied by county-level education, health insurance coverage, median annual household income, and unemployment.
Many studies are consistent with ours in that they show an immediate decrease in the number of child maltreatment reports after COVID-19–related stay-at-home orders at the city and state levels in the United States. Across the United States, studies indicated a decrease in child maltreatment reporting during the early stages of COVID-19.59,60 In Los Angeles, the number of child abuse and neglect reports made to the Los Angeles Police Department decreased by 8.0% following stay-at-home orders. 48 Similar stay-at-home policies in New York City led to 28.8%, 51.1%, and 46.6% fewer reports of child maltreatment than expected in March, April, and May 2020, respectively, when compared with 2019. 47 In California, the number of child protection reports dropped 14.3% after stay-at-home orders, although the proportion alleging domestic violence increased. 50 After statewide stay-at-home orders in Colorado, referrals and responses of child maltreatment dropped by 27.9% as compared with 2019, with 68.7% and 39.2% drops coming from school professionals and daycare providers, respectively. 35 The number of daily reports fell from 43.5 in 2019 to 31.6 in 2020 following stay-at-home orders in Michigan. 54 Decreases in reports were also seen in states near the state that we studied. The number of reported allegations of child maltreatment was 27% lower than expected in March and April 2020 in Florida. 49 Reports in Georgia decreased by 58% during 2020 as compared with earlier years, driven by fewer reports made by educational personnel. 53 Lastly, in North Carolina the rate of child maltreatment reporting fell from 2716 per 100 000 population in 2019 to 2547 in 2020. 52 In the United States, reports made by education or medical personnel make up almost one-third of all child maltreatment reporting 31 ; therefore, we believe that the immediate separation of children and these mandatory reporters, among all others, likely led to the decrease in reporting following stay-at-home orders.
Although the number of child maltreatment reports tended to decrease after COVID-19 stay-at-home orders, previous studies showed that parental experiences associated with higher risk for child maltreatment increased during the pandemic, 61 consistent with our results of increased rates of reporting following stay-at-home orders. Domestic violence as a whole and substance use also increased during the pandemic, with police calls indicating that domestic violence increased from 7.5% to 12.0% on average as compared with before the pandemic in major US cities.62,63 Mohler et al 64 reported that 911 calls for domestic violence increased in Los Angeles and Indianapolis during the pandemic. In addition, family violence increased among families with a history of violence in rural and suburban areas of North Carolina, 65 and violence-related trauma increased by 55% in Connecticut communities. 66 Finally, substance use and drug overdoses in the United States increased during the COVID-19 pandemic. 67
Strengths and Limitations
Our study had several strengths. First, we analyzed the impact of the stay-at-home order on the number of hotline calls by using the interrupted time-series method, a widely used method in evaluating the effect of policies with a clearly defined start date, 68 as was the case in our context. Second, we examined the number and rate of change in hotline calls, which gives us a better understanding of the immediate and evolving consequences of COVID-19–related policies. By September 30, 2020, the COVID-19–related stay-at-home order was still in place in this southern state; therefore, trends reported from our analysis were not affected by the policy ending. Third, our analysis incorporated county-level socioeconomic variables. Child maltreatment reporting has been shown to differ among socioeconomic groups, 28 and our study quantified some of those differences in the context of COVID-19. To our knowledge, no other study has examined possible disparities in child maltreatment reporting across socioeconomic groups.
Our study also had several limitations. First, the data used in this analysis did not include information on child race or reporter type. Differences in reporting of child maltreatment across various racial groups54,58 and reporter type51,54 have been shown. These variables were not available in our data but could have provided further insight into these differences during the pandemic. Second, we incorporated socioeconomic information into our analysis, although we included these continuous values as county-level categorical variables. Third, while we did include time as a variable in our models, possible autocorrelation of error terms may still be present, although we did not adjust for this further. Fourth, to ensure that our results were easily interpretable, we did not include a model that adjusted for all possible covariates, although unadjusted models may have led to biased estimates. Fifth, we modeled trends of hotline calls linearly, although the relationship between time since the stay-at-home order and allegations may be more complex than a linear relationship. Lastly, we used a single source of data on child maltreatment allegations from a single southern state up to September 30, 2020; therefore, our results should be considered within such context. A more complete picture of how child maltreatment has been affected by COVID-19 across the United States requires understanding our results alongside all other studies on this topic.
Conclusion
We found that the stay-at-home order related to the COVID-19 pandemic was associated with an immediate decrease in child maltreatment allegations in a single southern state. We also noted a subsequent increase in the rate of change in child maltreatment allegations across most age groups, allegation and case severity, and county-level socioeconomic characteristics. Immediate declines in the average number of allegations are likely linked to the physical separation of mandatory reporters of child maltreatment in professional settings and children. The increases in the day-to-day rates of change in allegations may be associated with the increase of domestic violence and/or parental substance use during the COVID-19 pandemic. Evaluating these trends is important for policy makers and practitioners to understand how policies enforced during the pandemic influence child maltreatment reporting and how these policies may affect reporting differently across socioeconomic groups.
Supplemental Material
sj-docx-1-phr-10.1177_00333549241245846 – Supplemental material for Reporting of Child Maltreatment During the COVID-19 Pandemic in a Southern State in the United States
Supplemental material, sj-docx-1-phr-10.1177_00333549241245846 for Reporting of Child Maltreatment During the COVID-19 Pandemic in a Southern State in the United States by Julia C. Thome, Kathy Gracey, Richard A. Epstein, Michael J. Cull, Tarah Kuhn and Rameela Raman in Public Health Reports
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online. The authors have provided these supplemental materials to give readers additional information about their work. These materials have not been edited or formatted by Public Health Reports’s scientific editors and, thus, may not conform to the guidelines of the AMA Manual of Style, 11th Edition.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.