
Abstract
Introduction
Adverse childhood experiences (ACEs) are associated with poorer health, developmental and academic outcomes. This study aims to describe the profile of kindergarten children exposed to ACEs in a tertiary hospital.
Methods
In this prospective cross-sectional study conducted between January 2023 and March 2024, demographic and health information were collected using a data collection form. Standardized screening tools were used to screen the child’s development, academics, behaviour, and caregiver’s mental well-being. Chi-square statistics was used for categorical variables.
Results
Among 52 children with exposure to ACEs, 78.8% experienced maltreatment, while 21.2% were exposed to household dysfunction (HD) alone. 35.9% had experienced four or more ACEs. Physical abuse (70.7%) was the most common abuse type, and biological parents (73.1%) were the most common alleged perpetrators. 63.5% were victims of repeated maltreatment. A significant proportion come from families with financial difficulties (55%), domestic violence (50%) or divorced parents (40.4%). Screening revealed a high prevalence of developmental delay (65.9% in maltreated group, 54.5% in HD group), academic concerns (61% in maltreated group, 54.5% in HD group), and behavioural concerns (65.8% in maltreated group, 33.3% in HD group). Children with behavioural concerns screened positive for developmental delays (p = 0.02) and academic concerns (p = 0.04). 15.4% have missed vaccinations.
Conclusion
Among kindergarten children who experience ACEs, screening revealed a high prevalence of developmental, academic, and behavioural concerns. Many have incomplete immunizations and come from families with socioeconomic stressors. Comprehensive screening of these children and families and timely intervention are essential to improving outcomes.
Introduction
Adverse Childhood Experiences (ACEs) are potentially traumatic events that occur in childhood 1 that can negatively impact health and well-being, with long-lasting effects into adulthood. 2 They encompass various forms of maltreatment (physical, sexual and emotional abuse and neglect) 3 as well as household dysfunction (HD) including domestic violence, parental separation and having a household member with substance abuse, mental illness or a history of incarceration. 4
Across international studies, 22% of children have experienced at least one ACE and 14.8% have experienced four or more. 5 Within certain Asian populations, the estimated prevalence was high among adolescents ranging from 40.2% to 81.4% for at least one ACE.6,7 In Singapore, data on ACEs in children are lacking, but a study among adults reported that 63.9% had experienced at least one ACE. 8
Toxic stress from ACEs may alter gene expression via epigenetic modifications and affect brain architecture and other organ systems during sensitive developmental periods. 9 ACE exposure is associated with behavioural problems 10 and poorer health and developmental outcomes with a dose-response relationship in children. 11
Childhood maltreatment is linked to poorer academic attainment and school readiness 12 with affected children more likely to underperform in literacy and numeracy, require special education, repeat grades13,14 and exhibit poorer academic performance in adolescence. 15 These challenges often extend into adulthood, contributing to unemployment, 16 antisocial behaviors, health-compromising behaviors, and greater odds of incarceration. 17
In Singapore, Ngiam et al. 18 reported that 19% of maltreated children aged zero to 16 years had developmental delay. Studies in children under 4 years report prevalence rates of 15% to 73.6%, with 31.7% demonstrating behavioural concerns.19,20 While these studies highlight the developmental and behavioural challenges of young children exposed to ACEs, data on kindergarten-aged children remain limited.
HD is often overlooked compared to presentation with child maltreatment, which is more easily identified. However, it is important to screen for ACEs in children exposed to HD as well as siblings of maltreated children, who similarly have poorer outcomes even without direct maltreatment. Previous research revealed siblings of physically abused children had lower reading proficiency and reduced school attendance compared to their peers. 21
Kindergarten years are crucial in laying the groundwork for future academic achievement and significantly impact a child’s transition to primary school. However, literature on kindergarten children among this vulnerable population is limited, particularly in Singapore.
Children with suspected maltreatment are referred to KK Women’s and Children’s Hospital (KKH) for evaluation of concerning injuries, neglect, or disclosed allegations of physical, sexual or emotional abuse. In recent years, the number of young children seen for safety and protection concerns in KKH has increased. This study aims to describe the profile of kindergarten children exposed to ACEs seen in a tertiary hospital.
This study is part of a larger project including Anchor Start (AS), a screening programme for maltreated children and their siblings aged zero to 6 years. It was established by KKH with support from Ministry of Health (MOH) to identify these children’s needs early and provide timely intervention.
Methods
Participants
Children in Kindergarten 1 (child turns 5 years old for the year) or Kindergarten 2 (child turns 6 years old for the year) who were evaluated at KKH for suspected maltreatment (neglect or physical, sexual or emotional abuse) as well as their siblings without direct maltreatment but exposed to HD (including domestic violence or having caregivers with mental health concerns), and other children with similar exposures, were referred to AS. Enrolled children who were screened by AS between January 2023 and March 2024 were included in this prospective cross-sectional study. Children who were not screened and excluded from this study included children (a) who were screened by established programs such as KidSTART, 22 (b) with known developmental delays and on follow-up with the Department of Child Development (DCD) or Early Intervention Programme for Infants and Children (EIPIC) or (c) whose parents were uncontactable or declined participation.
Procedure and outcome measures
Screening instruments used in Anchor Start.

aKK Women’s and Children’s Hospital, Department of Child Development.
Academic delay was defined as scoring below average in the Brigance Early Childhood Screen III 24 academic domain or failing to meet age-appropriate expectations on the Snake and Ladder assessment. Language delay was defined as scoring below average in the Brigance Early Childhood Screen III language domain or failing the language screener. Motor development delay was defined as scoring below average in the physical domain of the Brigance Early Childhood Screen III. Developmental delay was defined as having a delay in either language or motor domain. Behavioral concerns were defined as scoring low or very low for the prosocial domain or high or very high for domains of emotional, conduct, hyperactivity or inattention, or peer relationship in the Strengths and Difficulties Questionnaire. 25 Mental health concerns of caregivers were defined as having a score of 15 or more for GAD-7 26 or PHQ-9 27 or a known history of mental health issues. Missed vaccination was defined as a vaccine in the Singapore National Childhood Immunization Schedule 28 that is not given within 3 months after it is due. Financial difficulty was defined as requiring financial assistance to pay for medical expenses or to provide for the family or a Per Capita Income (PCI) of less than $800, fulfilling criteria for government financial assistance. 29
Data analysis
Descriptive statistics tabulated included demographic and clinical characteristics. The association between behavioural concerns, developmental delay, and academic concerns were assessed using Pearson’s Chi-square test or Fisher’s exact test for proportions and Mann-Whitney U test for numerical data.
Ethical consideration
The study was exempted from SingHealth Centralised Institutional Review Board (IRB) review as it was considered a service evaluation (reference number 2023/2111).
Results
Demographic and socioeconomic information of the children (N = 52).

aP-values from Chi-square test or Fisher’s exact test for proportions and Mann-Whitney U test for numerical data.
bPer Capita Income (PCI) data presented as median [interquartile range].
Clinical information of the children (N = 52).

Socioeconomic risk factors
Among factors for HD, domestic violence was the most common (26/52, 50%), followed by divorce (21/52, 40.4%), history of incarceration (15/52, 28.8%), and substance abuse (13/52, 25%). Nearly two-thirds (33/52, 63.5%) of the children were known to child protection services for previous allegations of maltreatment. About half faced financial difficulties (28/52, 53.8%) and stayed in rental housing (18/38, 47.4%). Six out of 44 (13.6%) caregivers screened had mental health concerns. Less than half of biological parents, 22 mothers (35.3%) and 17 fathers (48.5%), had attained secondary school education or lower.
General health and vaccination practices
Nine out of 52 (17.3%) children had pre-existing medical conditions, including eczema, recurrent wheezing, anemia, tethered pulmonary valve, ex-prematurity, history of Kawasaki disease, and faltering growth. Eight (15.4%) had missed vaccinations.
Development, academic and behaviour outcomes
15% (7/47) of children who completed all assessments were typically developing with no developmental, academic, or behavioural concerns. Almost two-thirds (33/52, 63.5%) screened positive for developmental delay (Figure 1), and more than half (31/52, 59.6%) for academic concerns (Figure 2). Language delay (33/52, 63.5%) was more common than motor delay (14/52, 26.9%). Among those who experienced maltreatment, 65.9% (27/41) screened positive for developmental delay, and 61% (25/41) for academic concerns. Among those exposed to HD, 54.5% (6/11) screened positive for developmental delay and similarly for academic concerns. More than half (28/47, 59.6%) screened positive for behavioural concerns (Figure 3). Conduct problems were the most common (13/47, 27.7%), followed by prosocial problems (12/47, 25.5%), hyperactivity or inattention (11/47, 23.4%) and emotional (4/47, 8.5%) or peer problems (4/47, 8.5%). Behavioural concerns were significantly associated with developmental delay (p = 0.02) and academic concerns (p = 0.04). Developmental assessment outcomes, as measured by the Brigance Early Childhood Screen III and Language Screener. Academic assessment outcomes, as measured by Brigance Early Childhood Screen III and the Snake and Ladder tool. Behavioural screening outcomes, measured using the Strengths and Difficulties Questionnaire.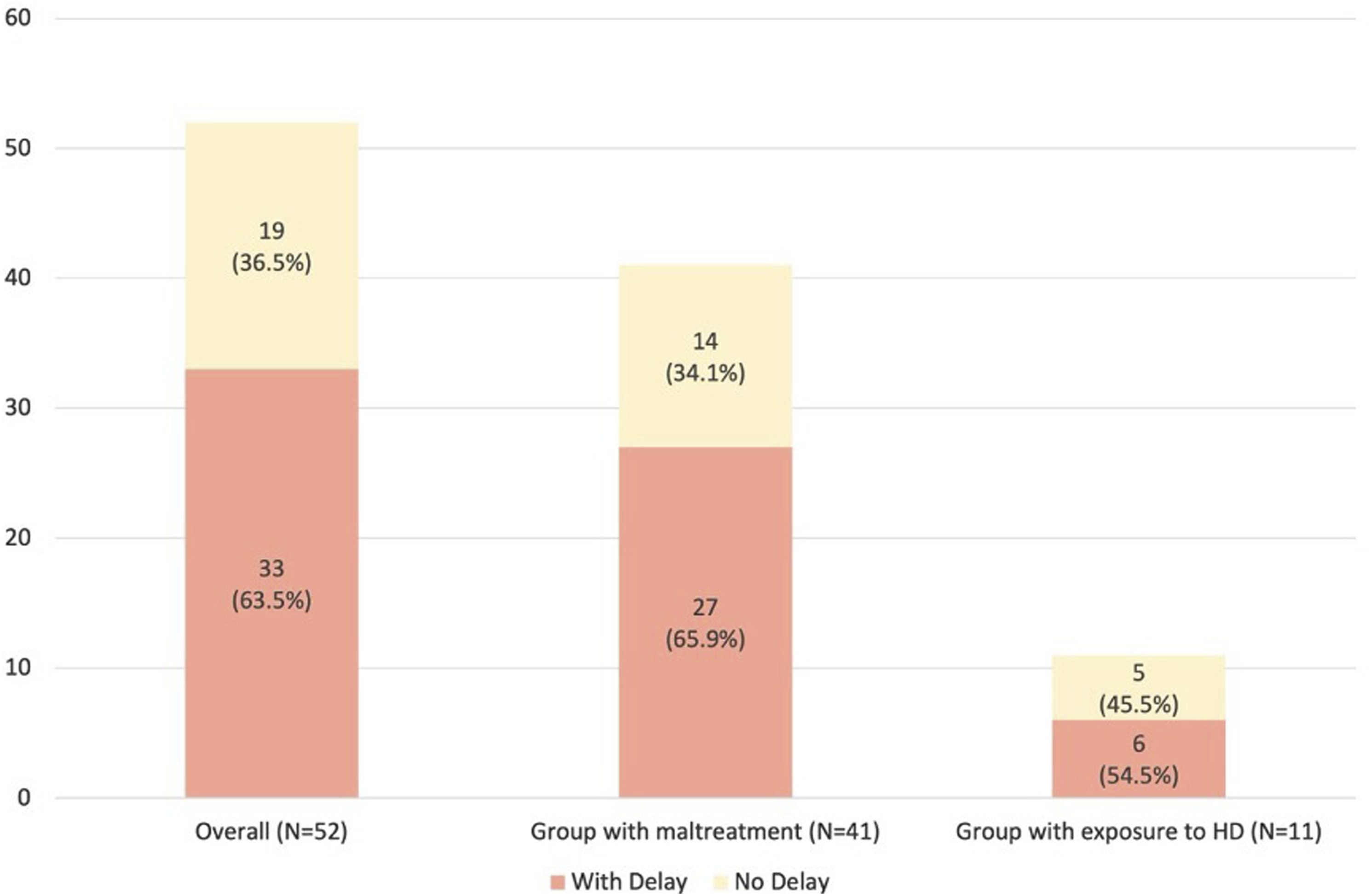


Referrals
21 out of 52 (40.4%) required medical referrals for developmental, academic, behavioural, or growth concerns, of which three had declined. Six (11.5%) were referred to allied health for therapy, and eight (15.4%) were referred to psychology for symptoms of post-traumatic stress disorder, emotional dysregulation, or behavioural concerns.
Discussion
The prevalence of ACEs among Singapore children is not well studied. To our knowledge, this is the first study describing ACEs experienced by kindergarten children in Singapore. More than half (53.8%) of our study population experienced four or more ACEs or one to three ACEs but with possible trauma symptoms. This is concerning as research has shown that both cumulative ACE exposure and presence of associated symptoms contribute to toxic stress, which increases the risk of adverse developmental, behavioural and health outcomes.4,30,31
Majority of our study population experienced maltreatment with the most common form being physical abuse (55.8%). This is consistent with local trends, 32 but contrasting with global patterns where neglect predominates.33–36 This may be contributed by the cultural acceptance of physical discipline in Singapore, resulting in more reports of physical abuse,37,38 coupled with an ambivalence reflected by the Singapore law which only implicitly prohibits corporal punishment of children by their parents. 39 As it can be difficult to distinguish non-abusive discipline from outright abuse, with the former having potential to escalate in frequency and severity, the use of physical discipline should not be condoned. 40 This is supported by a local study of family profiles entering CPS, which found that families adopting harsh parenting had the highest risk of recurrence of harm. 41 Another reason for Singapore’s differing maltreatment profile may lie in the challenges of identifying neglect. A local study on perceptions of child maltreatment found inconsistencies between professionals and the public, with some professionals perceiving neglect or emotional maltreatment as less serious. 42 Concerns related to malnutrition, missed vaccinations and insecure attachments, which could be features of physical and emotional neglect, may also often be under-recognised.
Lower family socioeconomic status, domestic violence, substance use disorders, 43 and caregiver criminality issues 41 are associated with child maltreatment as they may negatively affect parental functioning and stress, thus increasing the risk for maltreatment. This is consistent with our results, as about half of the study population faced financial difficulties (55%) and stayed in rental housing (47.4%). The median PCI is SGD 1224.40, which is lower compared to the average Singapore PCI of SGD 2886 in 2020. 44 Half of the households (50%) had a history of domestic violence, which is much higher than the estimated national rate of 3% to 20% reported in 2019. 45 The frequency of caregivers with incarceration history (28.8%) and substance abuse (25%) is similar to a previous study examining family profiles of maltreated children in Singapore. 41 This underscores the need to support high-risk families with targeted interventions to reduce child maltreatment.
Lower parental education attainment is associated with child neglect 46 as it often reflects lower socio-economic status, contributing towards parental stress and poorer awareness or access to support services. In our study, many biological parents (64.7% of mothers and 51.5% of fathers) had education above secondary school level, comparable to national averages. 47 However, despite higher education attainment, a large proportion faced financial difficulties which may reflect the bigger role of family socio-economic status as a risk factor in child maltreatment.
Many children in our study sample have missed vaccinations with vaccine coverage being lower (84.6%) than the national average of 95% to 99% 48 for the key preventable childhood diseases despite many of these vaccinations being fully subsidized. Moreover, under Singapore’s Infectious Diseases Act, it is compulsory for school-going children to be vaccinated. Hence, it is important to understand parental barriers and perceptions around routine health-related behaviors in order to address these knowledge-practice gaps.
Nearly two-thirds (63.8%) of our study population experienced repeated maltreatment which is much higher than what was previously reported in a local study (29.2%) reviewing maltreated children aged zero to 16 years. 18 Most alleged perpetrators were parents (73.1%), and the majority of children were placed in familial care upon discharge (75%). This may be reflective of Singapore’s child protection system’s focus on family preservation and in-home care supported by coordinated services to strengthen the family, while promoting a safe and secure environment for the child. However, persistent family risk factors may contribute to recurrence of maltreatment. Home visitation programmes supporting family preservation have been shown to reduce recurrence and improve child development.49,50 Locally, a similar programme for maltreated children also demonstrated improvements in developmental and behavioural outcomes. 20 This emphasizes the need for comprehensive family assessments, continued surveillance and adequate support, to prevent recurrence and improve developmental outcomes.
In our study population, only 15% (7/47) of children who completed all assessments were typically developing with no developmental, academic, or behavioural concerns. A sizeable proportion screened positive for behavioural concerns, some of which are likely trauma symptoms, especially among those who experienced maltreatment (65.8%). This prevalence exceeds that reported in younger children under four, 20 suggesting the cumulative impact of trauma over time, with kindergarten children at higher risk of persistent behavioural concerns. ACEs are linked to behavioural problems, with a greater impact on externalizing behaviours. 51 This is consistent with our findings of a much higher prevalence of externalizing behaviours (27.7% for conduct problems and 23.4% for hyperactivity or inattention) than internalizing behaviours (8.5% for emotional and peer problems). This may be because younger children often display distress through outward behaviours such as aggression or impulsivity while internalising symptoms often emerge later as cognitive and emotional awareness develops. In addition, one-quarter (25.5%) had concerns for prosocial domain. These behavioural problems can heighten caregiver stress and increase risk of recurrence of maltreatment. Hence, identifying these concerns early enables caregivers to understand their child’s behavioral responses and adopt positive parenting strategies to manage them.
There is a high prevalence of children who screened positive for developmental delay and academic concerns among both groups (children who experienced maltreatment and those exposed to HD). In our study, 65.9% of maltreated children screened positive for developmental delay, likely an underestimate of the true prevalence as children with known developmental delays who were on follow-up were excluded. This prevalence is substantially higher than previous Singapore studies using retrospective case notes reviews, which reported a prevalence of 19% among maltreated children aged zero to 16 years 18 and 15% among children under 4 years, 19 compared to 10% in the general population. 52 Our findings are consistent with Chan et al. 20 who similarly used standardised screening tools and found a prevalence of 73.1% among children under 4 years. These results suggest that without early identification and support, developmental and behaviour concerns in children exposed to ACEs are likely to persist. In our study, developmental delay was significantly associated with behavioural concerns (p = 0.02), consistent with prior research showing that children with developmental delays were three times as likely to score in the clinical range for behavioural problems than their non-delayed peers. 53
More than half (61%) of the group with alleged maltreatment screened positive for academic concerns and had behavioural concerns (p = 0.04). This aligns with previous studies examining school readiness and academic achievement among maltreated children. A meta-analysis of 59 studies found all types of child maltreatment were significantly linked to poorer academic outcomes. 54 Similarly, a longitudinal study reported that maltreated children face increased risks of grade repetition and poor performance in English and Mathematics as early as kindergarten and grade 1 compared to their peers. 55 These findings likely reflect the challenges that maltreated children often exhibit in concentration, memory and cognitive abilities which can hinder learning and academic achievement. 56 These challenges, in addition to behavioural difficulties, persist long after the abuse or neglect has ended 57 and can have significant long-term adverse effects into adulthood. Moreover, parents who perpetrate abuse often face multiple competing needs, limiting their involvement in their children’s education and negatively affecting academic performance. 58
The group exposed to HD showed similar outcomes to those who experienced maltreatment. An American study revealed that children who experienced ACEs had increased odds of below-average academic skills by the end of kindergarten, with greater ACE exposure linked to worse outcomes, suggesting a dose-response relationship. 59 This suggests that other than abuse or neglect, household dysfunction also has a significant impact on an individual. Thus, we recommend comprehensive screening of the child and family in the community should any adversities be identified.
The results of our study are concerning as a sizeable proportion of these children have developmental, academic, and behavioural concerns that still need to be identified and addressed despite attending pre-schools and having access to community support. Through early identification, AS facilitated referrals for interventions and provided psychoeducation to caregivers, helping them understand and respond to their child’s needs, with the goal of improving developmental and behavioural outcomes and optimising potential. However, with such a short time frame before entering primary school, it may be challenging for these children to catch up to their peers, and some may require deferment of primary school entry. Thus, early identification is crucial for timely intervention. This will facilitate a smooth transition to primary school, improve learning outcomes, and promote student engagement and positive school experiences, potentially reducing adverse social and occupational impacts.
To our knowledge, this is the only Singapore study assessing developmental, academic, and behavioural outcomes in kindergarten children using standardized screening tools, which included children who experienced maltreatment as well as exposed to HD. Our study adds to the growing literature on child maltreatment in Singapore and has important clinical implications for healthcare providers.
This study has some limitations, such as the small sample size given the specific population. As some caregivers declined to participate or were denied access to the child for safety reasons and were uncontactable, some demographic variables such as parental education, housing, PCI, and ACEs, and some assessments requiring caregiver input were incomplete. This study did not include the children’s growth data and nutritional status, which could be a consideration for inclusion in a later phase of the study. The tools utilized in this study are screening tools and may not reflect the actual extent of developmental delays. These tools, including in-house developed tools such as the Language Screener and Snakes and Ladders, have also not been formally validated in the local setting. Although each tool may individually lack specificity, using them in combination may improve detection of language and academic concerns. Excessive screen time may be a confounding factor, given its known negative impact on child development, especially language skills.60,61 Maltreated children may receive excessive screen time due to lower caregiver engagement. However, studies on screen time in this population are limited and should be explored further. Finally, as this is a cross-sectional study, causality cannot be inferred from our findings. Future longitudinal studies, incorporating outcomes such as psychological health that may affect educational experiences, should be conducted to better understand risk factors and needs in this population and guide targeted prevention and harm reduction programs. The potential of Artificial Intelligence to enhance risk detection can also be explored, as early identification and intervention are key to improving child safety and developmental outcomes.
In conclusion, this study describes the profile of kindergarten children exposed to ACEs, revealing a high prevalence of developmental, academic, and behavioural concerns. Many have missed vaccinations and come from households facing various social or financial stressors. A holistic assessment of the child and family is thus essential and should be extended to all children exposed to ACEs. Early identification allows timely interventions and support, facilitating a smooth transition to primary school and mitigating negative impacts on future academic achievement, health, and overall well-being.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is part of a larger study involving a screening programme, Anchor Start (AS), which was established by KK Women’s and Children’s Hospital (KKH), and supported by Ministry of Health (MOH), Singapore under Grant [number MH 70:08/19].
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
IRB approval
The study was exempted from SingHealth Centralised Institutional Review Board (IRB) review as it was considered a service evaluation (CIRB reference number 2023/2111).
Data Availability Statement
The data that support the findings of this study are available from the Anchor Start programme, but restrictions apply to the availability of these data and are not publicly available. However the data are available from the authors upon reasonable request.