
Abstract

Addressing racial health inequities and structural racism requires the concerted efforts of local public health departments (LHDs), which are often the main link between the US public health system and the diverse communities served by LHDs. Structural racism can be considered policies and practices within the interrelated network of society’s institutions (eg, criminal–legal, education) that favor one or more racial groups over others. These policies and practices are not dependent on individual people within the institutions to intend harm for some racial groups.1,2 Structural racism encompasses multiple dimensions of history, culture, interconnected policies and institutions, and racial ideology. Although structural racism exists across all sectors of society, Camara Phillis Jones, MD, PhD, MPH, a family physician, epidemiologist, and antiracism activist, has asked public health institutions to look within and ask, “How is racism operating here?” and then act by “organizing and strategizing.” 3 One way to implement action is through the creation of an antiracist mindset within the public health system, which could lead to antiracist policy making and programming. We use a definition of antiracism to help guide understanding: “a commitment to dismantling racism, which has dimensions that are institutional and social as well as attitudinal and behavioral.” 4 In this commentary, we describe (1) why LHDs are essential sites for antiracist capacity building, (2) what we mean by antiracist LHD, and (3) how LHDs can organize and strategize to disrupt structural racism internally and externally to promote health equity.
LHDs as Essential Sites of Antiracist Capacity Building
The Commonwealth Fund stresses that public health agencies should work to earn public trust among people who have had experiences with racism and discrimination in the public health infrastructure. 5 Research and tools on building antiracist LHDs are insufficient and have prevented public health agencies from internally confronting racism; thus, LHDs may not be able to externally practice antiracism in their roles as service providers (eg, providing vaccines, testing for sexually transmitted diseases, administering the Special Supplemental Nutrition Program for Women, Infants, and Children), policy makers (eg, vaccine prioritization, face mask mandates, water boil advisories), collaborators (eg, partnering with nonprofit organizations and other government agencies), and employers (eg, establishing hiring, pay, and promotion criteria). These roles of LHDs can affect racial health inequities in preventive care, nutrition, chronic disease management, and infectious disease. 6 LHDs play a key role in the public’s health and in health inequities experienced by their constituents but especially by historically racially marginalized and minoritized groups (eg, Black people, indigenous people). As such, community health and the inequities based on race, ethnicity, gender, and income are influenced by the people, programs, policies, and power-sharing practices within LHDs and the demographic makeup of the community served by LHDs. Views on social and political issues vary across community types, with communities influenced by historical, geographic, and political features, in addition to the size and governance of the LHD. The varied conditions that contribute to how the LHD is formed and the constituents of the community (eg, urban vs rural) will influence the extent to which racism is considered a public health issue worthy of being addressed. Antiracist work by LHDs is challenging if their communities do not value such work. Another potential challenge is an LHD workforce that does not reflect the community that it is serving. However, LHDs should consider and start antiracism work even if they do not fully represent their community.
Despite the makeup of the LHD, what remains important is that the LHD leadership has ownership of efforts needed to transform the LHD into an antiracist entity. The LHD director and associated executive leadership team must work together with community representatives to collectively make change. Ultimately, LHD leadership will hold members in the public health institution, the local board of health, and other units throughout the local government accountable to their constituents to go beyond identified areas of needed change.
LHDs often declare racism a public health issue, 7 but a gap remains between what public health officials say and what public health institutions do. 8 With bold leadership and political will, antiracist capacity building within LHDs can help shrink this gap, particularly because LHDs can enhance readiness to address institution-level activities that can promote equity (Figure). In addition, although early definitions of racism have centered on people and institutions,6,9 much of the public health work related to racial inequities has historically focused on communities that have been racially marginalized rather than on institutions. 10 The focus on communities neglects how institutions—including public health institutions—require systematic long-term investment (time, personnel, and funding) and intervention to build capacity for effective antiracist practices that will actively work against structural racism over time. Griffith et al 11 used the case of a county public health department to illustrate how “organizations, often unintentionally, function as tools of oppression, reproducing and reinforcing the very marginalization that some are committed to undoing.” Unintentional oppression may occur because of the complex interconnection between LHDs and their larger sociopolitical context, as well as the influences from the society in which LHDs exist. Plainly, a racist society produces racist institutions whether they aim to be racist or not. Of note, although many LHDs certainly have done work to undo racism within (eg, New York City’s Race to Justice Initiative, 12 the King County, Washington, “Anti-racism Crisis Response Bill of Rights” 13 ), work often occurs in progressive settings and is relatively nascent. More research and sharing of evidence-based practices among LHDs are still needed.
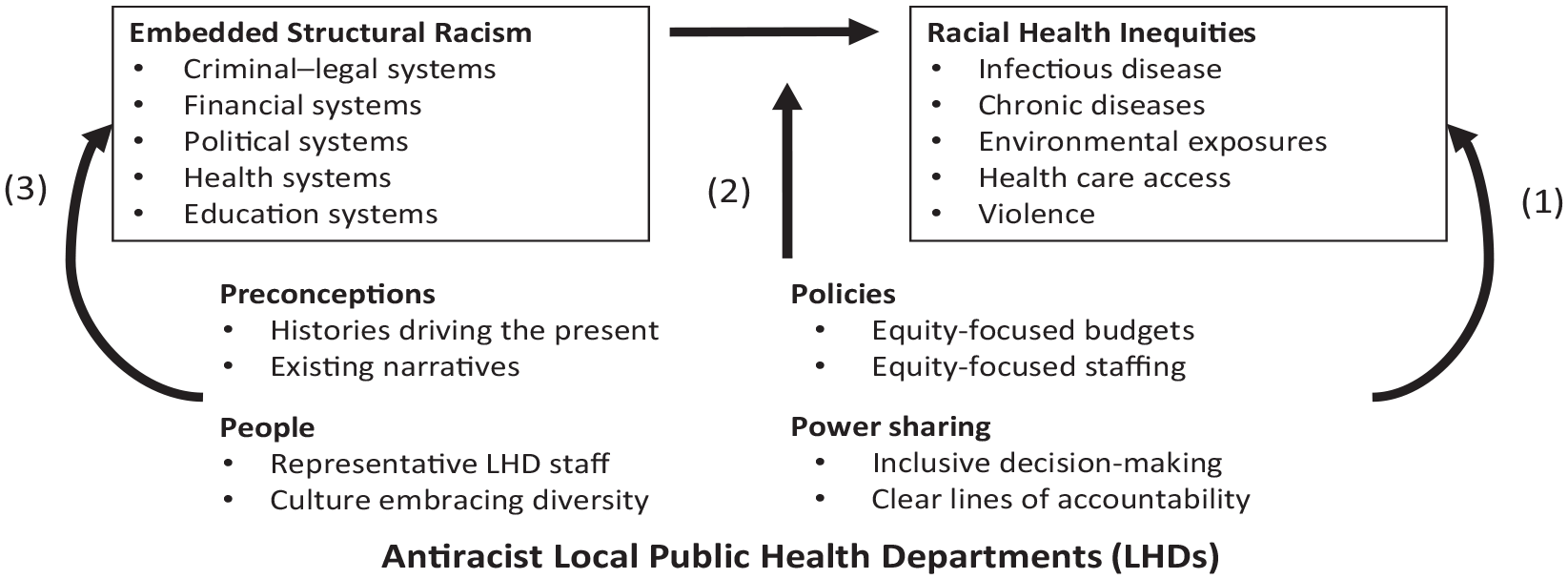
Conceptual model of antiracist local public health departments (LHDs) disrupting the relationship between structural racism and health inequities in 3 ways (arrows 1-3). Arrow 1 represents engagement of antiracist LHDs in advocacy to transform other systems to become antiracist. Arrow 2 represents engagement of antiracist LHDs in cross-sector collaborations and partnerships with community-based organizations to moderate and reduce the negative health effects of other systems on racially marginalized communities. Arrow 3 represents engagement of antiracist LHDs to provide direct services in racially marginalized communities that follow antiracism principles. Reprinted with permission from Creary et al. 19
Incorporating organizations into a structural theory of racial inequality can help us better understand stability, change, and the “institutionalization” of racism. 14 Jones 15 defines institutional racism as “the structures, policies, practices, and norms resulting in differential access to the goods, services, and opportunities of society by ‘race.’” Addressing “structure” means that the LHD recognizes and intervenes against cumulative, historical, and societal processes that create racial inequality. 16 By operating within a “White racial frame,” 17 the public health system can rationalize the structures that perpetuate inequities, injustices, and racial patterns—for example, by inequitable allocation of resources because of race/place-neutral policies or dissemination of critical information created with an educated White population in mind. This White worldview can affect the creation and implementation of policies and programs to address racial health inequities.17,18 Thus, building capacity is needed within LHDs to take antiracist action that removes the White racial frame and instead places the needs of communities that have been racially marginalized at the center of their work.
Transformation Into Antiracist LHDs
An institution’s people, programs, policies, and power-sharing practices are areas where institutions need to be actively antiracist rather than simply being not racist. 19 Ray’s theory of racialized organizations reminds us that institutions are not race neutral and, thus, are either contributing to or fighting against structural racism. 14
Given several researchers’ descriptions of institutional transformation,20-22 we conceptualized the LHD antiracist transformation along a spectrum (Table), with a racially exclusive LHD on one end and a fully antiracist LHD in a transformed society on the other end. We adapted the LHD antiracist transformation from a commonly used resource created by Crossroads Ministry to apply to any organization. 20 Although the original resource is useful for LHDs, we adapted and applied the concepts to the specific role and context of LHDs. Our description can help guide key actions to shift an institution from one that is focused on passive or “symbolic change” to one that is focused on antiracist structural change. We included the same steps of transformation from the Crossroads Ministry model (ie, from exclusive to fully inclusive); however, we further divided each step of transformation into people, policies, programs, and power sharing (4P framework). This framework, which is further described elsewhere, 19 allows clear connection to LHD practices (Table).
Continuum of LHDs from racially exclusive to fully antiracist in a transformed society a
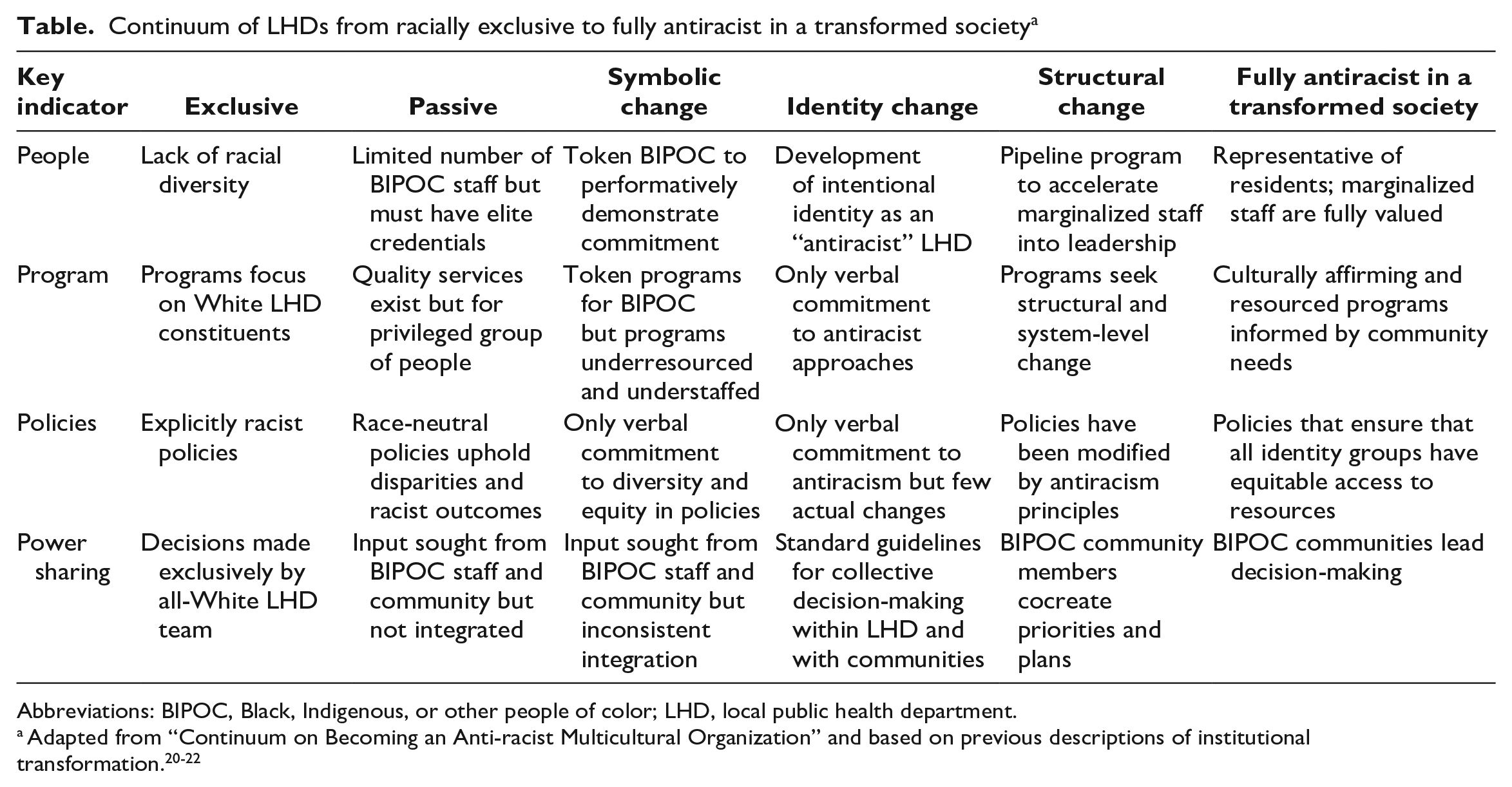
Abbreviations: BIPOC, Black, Indigenous, or other people of color; LHD, local public health department.
LHDs can move along the spectrum by transforming their workforce (eg, investing resources into antiracist capacity building, hiring, promotion, staff retention), programs and policies (eg, allocating resources proportional to the needs of and inequities faced by historically marginalized and minoritized communities, applying health equity impact assessments before initiatives are implemented), and power-sharing practices (eg, shifting toward more collective and community-engaged decision-making).
Disruption of Structural Racism Through LHDs
An antiracist LHD can disrupt the fundamental relationship between structural racism and racial health inequities. Structural racism is embedded within key institutions throughout society, such as those in criminal–legal systems, financial systems, political systems, health departments and health care systems, and education systems. These systems work synergistically to produce broad and persistent health inequities and poor health for communities that have been racially marginalized.
We propose that antiracist LHDs will be able to disrupt the fundamental relationship between structural racism and racial health inequities in 3 ways (Figure). First, antiracist LHDs should engage in advocacy to transform other systems to become antiracist. Transformation is not possible until LHDs reflexively turn inward and adopt antiracist approaches themselves. Antiracist LHDs can use their power to help frame issues of the health care system, criminal–legal system, voting, education, and financial system injustice as critical racial justice and health justice issues. 20 Antiracist LHDs can also join coalitions and support community activists who are trying to transform these systems.
Second, antiracist LHDs can moderate and reduce the negative health effects of other systems on racially marginalized communities by engaging in cross-sector collaborations and partnerships with community-based organizations. These collaborations should emphasize equity for residents (eg, ensuring access to health care and housing for formerly incarcerated residents, collaborating with school systems to ensure equitable vaccine distribution).
Third, antiracist LHDs can equitably provide direct services in racially marginalized communities that follow antiracism principles. These direct services include vaccine delivery, health care, and environmental protections that will promote health for residents who have been racially marginalized. An equitable distribution of resources requires that resources are matched to need.
Although antiracist LHDs can take these actions, a prescribed step-by-step process to follow is not available. LHDs must work collaboratively with local community members who have been marginalized to take action according to their local context. 19
Antiracist LHDs can serve as influential cross-sector partners to undo structural racism across sectors. Public Health 3.0 calls for an expanded scope for local public health partners to engage in cross-sectoral collaborations to improve community health. 23 For example, LHDs could influence local health care providers. One opportunity to push health care providers further exists within the Affordable Care Act, which requires nonprofit hospitals to assess and respond to community health. 24 LHDs can be resources for health systems and can use that leverage to help health systems adopt more antiracist approaches that benefit the local community beyond individual patient care. The potential of LHDs to leverage their relationship with health systems is amplified when partnered with communities that will be directly affected by local health care providers. LHDs have the opportunity to play a similar role with local criminal–legal system entities (eg, law enforcement, criminal courts) or the local transportation authority. Law enforcement and criminal courts are part of structural racism and are highly influential on health, and LHDs can help frame these other legal and criminal issues as health issues. 25 However, to effectively push other community sectors to be more antiracist, LHDs themselves will need to model and build capacity for being antiracist institutions so that they can effectively influence cross-sector relationships. Having LHDs as models of antiracist institutions will effectively return the field to the community organizing roots of public health, which will assist in the collaboration of efforts to empower people, leverage resources to advocate for communities, and effect change.
Structural racism can undermine or constrain well-intentioned health equity efforts within LHDs. For example, funding is often a contested resource that can open some pathways while constraining others. Funding can often come with stipulations that serve to define problems and appropriate avenues of intervention. These stipulations can silence community voice and expertise and reinforce hierarchies that disempower historically marginalized and minoritized communities and reenact long-standing harms. LHDs with robust antiracist practices can build stamina to adaptively counteract the forces of structural racism and improve health. As a multilayered and deeply embedded system of inequity, structural racism will not be easily uprooted and solved with much of our current health equity work, particularly for work that does not focus on institutional or structural transformation. The concept of “bounded justice” makes clear that even institutions trying to be antiracist are still “bounded” in that they may not swiftly achieve health equity for their residents because the countervailing forces of structural racism are so strong. 26 Antiracist LHDs grounded in a bounded justice perspective and antiracist principles are better able than LHDs not grounded in antiracist principles to identify these bounds and are equipped with the tools and stamina to adaptively respond to and counteract these forces to improve health.
Conclusion
Disrupting structural racism and the effects of structural racism on health inequities will require strategic actions by public health professionals that are both inward and outward facing. Building capacity within LHDs to take antiracist action is urgently needed. Without this lens and grounding, efforts to achieve health equity will have little effect. LHDs are community resources that can play a key role in shifting how local resources are allocated and how other local institutions operate. Investments are needed today in antiracist capacity building for LHDs.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Office of the Vice President for Research at the University of Michigan.