
Abstract
In an attempt to move the field of public health from documenting health disparities to acting to rectify them, in 2001, the American Public Health Association (APHA) recognized racism as a fundamental cause of racial health disparities. Both APHA and the Council on Education for Public Health have moved to incorporate new competencies in health equity for public health professionals. As schools and programs of public health work to establish curricular offerings in race and racism, a need exists to identify approaches currently in use that can be replicated, adapted, and scaled. This systematic review sought to identify pedagogical methods and curricula that exist to support the training of US public health students in understanding racism as a structural determinant of health. We found 11 examples from peer-reviewed literature of curricula, lessons, and competencies that have been developed by public health faculty and departments since 2006. The articles discussed a range of approaches to teaching about structural racism in public health, suggesting that little consensus may exist on how to best teach this material. Furthermore, we found little rigorous evaluation of these teaching methods and curricula. The results of this review suggest future research is needed on public health pedagogy on structural racism.
With the resurgence of white nationalism in the past 2 decades, 1 -3 renewed calls have been made to address racism and white supremacy in US institutions. Many fields, including public health, are examining their past to understand how historical steeping in racist thought and behavior may influence present-day positionality and outcomes. 4 Although these efforts may be more broad based and publicly visible now than previously, such critical engagement builds on decades of scholarship and advocacy in public health. 5 This previous work led to the development of a rich body of research and practice that documents racial disparities, characterizes the ways in which racism functions as a structural driver of social determinants of health, and promotes equity and intergenerational healing from racist trauma. 6 -11 Despite the growth of the related fields of health equity and antiracist public health research and praxis in recent decades, relatively little is written about teaching these concepts in public health education.
US public health education is indelibly shaped by the legacy of Jim Crow. At the turn of the 20th century, the field was in its infancy and largely considered a subspecialty of medicine; public health was also sometimes referred to as preventive medicine or hygiene and sanitation. 12 The 1910 publication of Medical Education in the United States and Canada by Abraham Flexner, better known as the Flexner Report, 13 and the 1915 Welch–Rose Report 14 were instrumental in shaping the early development of public health pedagogy. The Flexner Report, often credited with establishing criteria for schools of medicine, reorganized medical education around laboratory and clinical science. 13 It also shuttered 5 of the 7 schools of medicine that admitted Black students, arguing Black students needed “good schools rather than many schools—schools to which the more promising of the race can be sent to receive a substantial education in which hygiene rather than surgery, for example, is strongly accentuated.” 13 The Flexner Report stated that schools serving Black students were “at this moment in no position to make any contribution of value” but provided no further evidence to support the claim. 13 Remaining schools were then able to broaden their curricular offerings, including through programs of study in public health.
The 1915 Welch–Rose Report, developed by a Flexner-led commission, laid the foundation for institutes of public health as professional training schools. The report stated that schools of public health should “be closely affiliated with a university . . . medical school” 14 and underscored a biomedical disease model of public health centered on hygiene. 15 Institutions serving White students were closed to Black students, severely curtailing access to education and credentialing in medicine and public health. 16 Throughout the 20th century, institutions of higher education that served White students primarily offered public health programs of study, at a time when the color line was still well-established and strongly enforced. In fact, the Council on Education for Public Health (CEPH) did not accredit a master of public health degree program at a Historically Black College or University until 1999 17 ; therefore, no accredited public health courses of study were available to Black students until institutions serving White students began to desegregate under legal orders in the 1950s. 18 Details on the history of desegregation in public health institutions are available elsewhere. 5,19,20 These historical barriers to accessing public health education have lasting importance, contributing to, for example, the contemporary dearth of senior Black academicians.
The 1980s and 1990s witnessed the rise of a cadre of Black public health scientists and increasing focus on “minority health.” 5 Although Black scholars called attention to ways public health failed to serve Black and other communities of color, the pedagogy of the predominantly White academy largely reinforced structural racism by presenting health disparities as the result of cultural deficits and poor personal health choices rather than systems of oppression. 21 To move the field from documenting disparities to rectifying them, in 2001 the American Public Health Association (APHA) recognized racism as a fundamental cause of racial health disparities. 22 Both APHA and CEPH have moved to incorporate new competencies in health equity, 23,24 underscoring the need for curricula that name racism and equip emerging professionals to actively dismantle racist systems. These changes are largely in response to ongoing leadership and advocacy by Black scholar–activists who have championed efforts to teach and address the role of internalized, interpersonal, and structural racism in the etiology of health disparities. 25
As schools and programs of public health expand curricular offerings on racism, identifying approaches that can be replicated, adapted, and scaled is necessary. Although much has been written about teaching cultural competency and implicit bias, 26,27 less has been published on teaching about racism as a structural determinant of health (tracing its history, how it was encoded into health-related policy, and how it produces disparate health outcomes) or methods to address structural racism to achieve health equity. Therefore, the objective of this systematic review was to synthesize peer-reviewed literature describing programs, curricula, and pedagogical methods designed to train students attending schools and programs of public health in the United States in structural racism and the application of racial equity principles to public health practice and scholarship.
Methods
Search Strategy
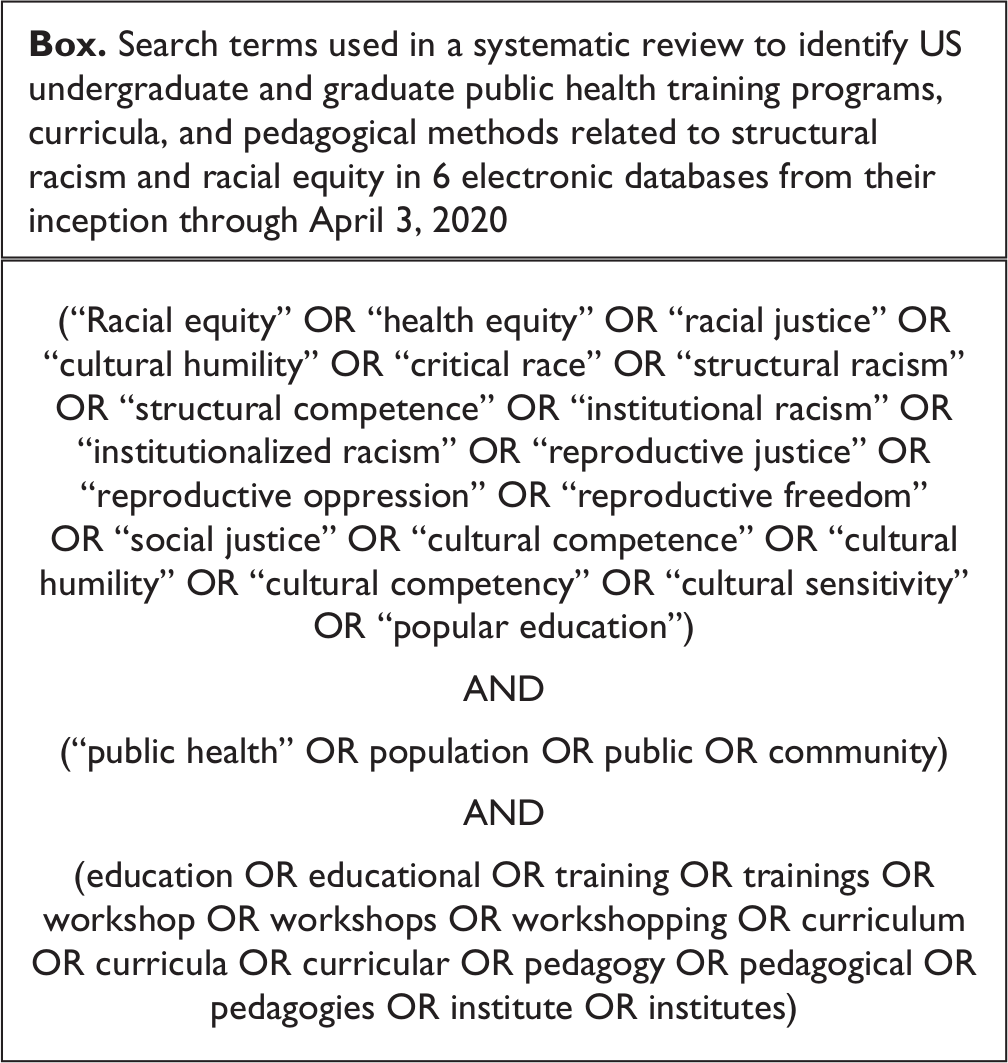
We developed a search protocol following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines to identify literature catalogued in 6 electronic databases (PubMed, ProQUEST Health Management, EBSCOHost ERIC, EBSCOHost MasterFILE Premier, Scopus, and Web of Science) published from inception through February 15, 2019. The search was subsequently updated through April 3, 2020. We collaborated with a health sciences librarian to develop a search strategy for each database with search terms related to racial equity, public health, and education (Box).
Search terms used in a systematic review to identify US undergraduate and graduate public health training programs, curricula, and pedagogical methods related to structural racism and racial equity in 6 electronic databases from their inception through April 3, 2020
Eligibility Criteria
We included articles in peer-reviewed journals published in English that discuss teaching, training, and/or capacitating public health students in racial equity. We defined racial equity capacitation as a curriculum or training on (1) the historical antecedents of racialized health disparities/inequities, (2) institutional and/or structural racism, (3) the intersection between policy and racialized health disparities (both historic and contemporary), or (4) applied antiracism. Articles included quantitative, qualitative, and mixed-methods studies; commentaries; and case reports (which may not have been peer reviewed despite being published in a peer-reviewed publication). We included articles that described lessons, curricula, or programs for students enrolled in a school or program of public health in the United States, regardless of level (undergraduate, master, or doctoral), format (residential or online), or accreditation status. The primary outcome measures for this review were increased awareness of racial equity principles, improved understanding of how structural and institutional racism undermine population health, and enhanced ability to apply racial equity approaches to conducting public health work and scholarship. We included studies if these outcomes were described in the curriculum/training learning objectives and/or evaluation outcomes, although evaluation of the curriculum/training was not necessary for inclusion.
We excluded studies that focused solely on in-service training or continuing education and training designed exclusively for direct service providers (eg, social workers, health practitioners in clinical roles). Because the focus of this review was public health professional training programs in the United States, we excluded studies that discussed public health training for high school students or students in other grades, were conducted outside the United States, were designed for students in other countries, and/or exclusively focused on geographic contexts other than the United States. Finally, reflecting our focus on structural racism, we excluded studies focused solely on instructional programs to reduce or eliminate interpersonal racism and/or bias.
Screening Protocol
Our searches returned 6384 results, including 4865 unique articles (Figure). Three reviewers (C.E.C., M.W.T., C.R.W.) screened each title and abstract for potential inclusion and identified 202 articles for full-text review. In pairs, the same 3 reviewers independently screened each article in full-text review. The team of 3 reviewers held conferences to resolve discrepancies in decisions to include or exclude articles as well as discrepancies in the reason for exclusion. Eleven articles met eligibility criteria. A hand search of reference lists of included articles did not identify any additional articles to include.
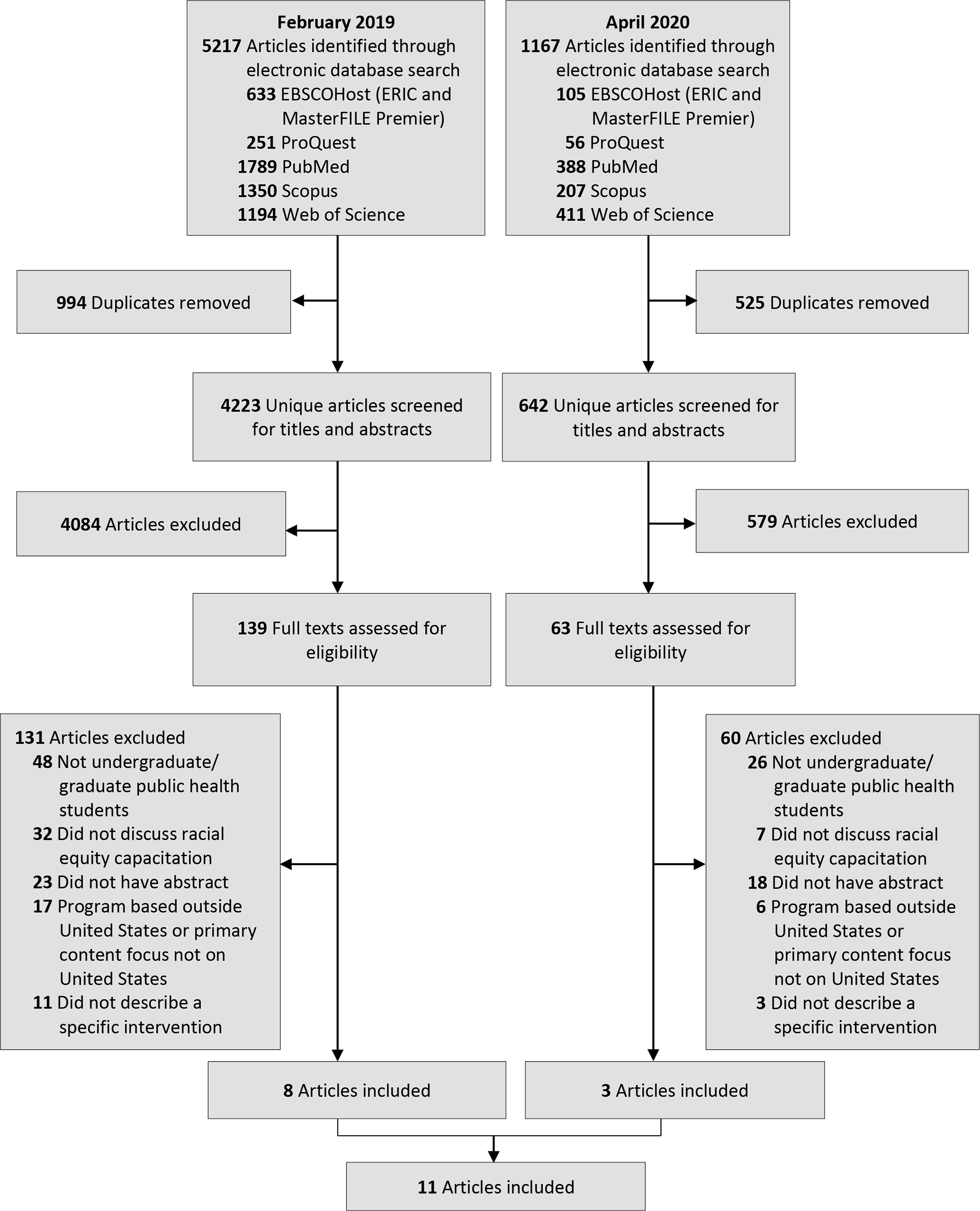
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram of articles identified as describing approaches for training public health students in structural racism and racial equity. Searches conducted in February 2019 and April 2020. Exclusion criteria were not mutually exclusive; only the primary reason for exclusion is reflected in the PRISMA diagram.
Data Extraction and Analysis
We extracted data from the 11 articles meeting eligibility criteria. We developed a standardized data extraction form through REDCap, an open-source online platform that facilitates data collection and management. We conducted a thematic analysis on extracted data to identify commonalities in key topic areas and pedagogical approaches across the instructional programs described in the identified articles.
Results
Topic and Content
The 11 articles framed key instructional topic areas in terms of health disparities or inequities (n = 3), 28 -30 structural issues (n = 3), 28,31,32 social determinants of health (n = 3), 32 -34 racism or antiracism (n = 2), 33,35 social justice (n = 1), 36 health (n = 1), 37 and pedagogy of collegiality (ie, application of feminist and critical theories in classroom activities and assignments to promote inclusion of diverse learning styles, open communication between students and instructors, community building, and multicultural education) (n = 1), 38 and used widely varying program content to capacitate students in racial equity (Table 1). For example, programs incorporated racial equity capacitation by using interactive lessons to teach about power, oppression, and privilege 28,38 or through using the television show The Wire to study the interplay of political, cultural, structural, and individual factors that perpetuate health disparities. 30,31 Other faculty members lectured on Dr Camara Jones’ Three Levels of Racism framework. 39 Moving beyond the classroom, some curricula guided students through a museum tour of exhibits on Black Wall Street and the Tulsa Race Massacre 33 or incorporated arts rooted in African communities to teach about the role of historical relations among political authorities, individuals, and collectives in producing health inequities without reifying inequities. 29 Other programs examined the effects of federal and state policies on health disparities 32,36 ; explored the social, political, and economic upstream factors, such as trade policy, that contextualize individual behaviors 34 ; and analyzed the effect of colonial processes on the health outcomes of Indigenous Peoples. 37 One program developed a schoolwide antiracism competency with courses that build students’ skills in antiracist analysis. 35
Components of US undergraduate and graduate public health training programs, curricula, and pedagogical methods for teaching about structural racism and racial equity in studies published before April 2020: results of a systematic review
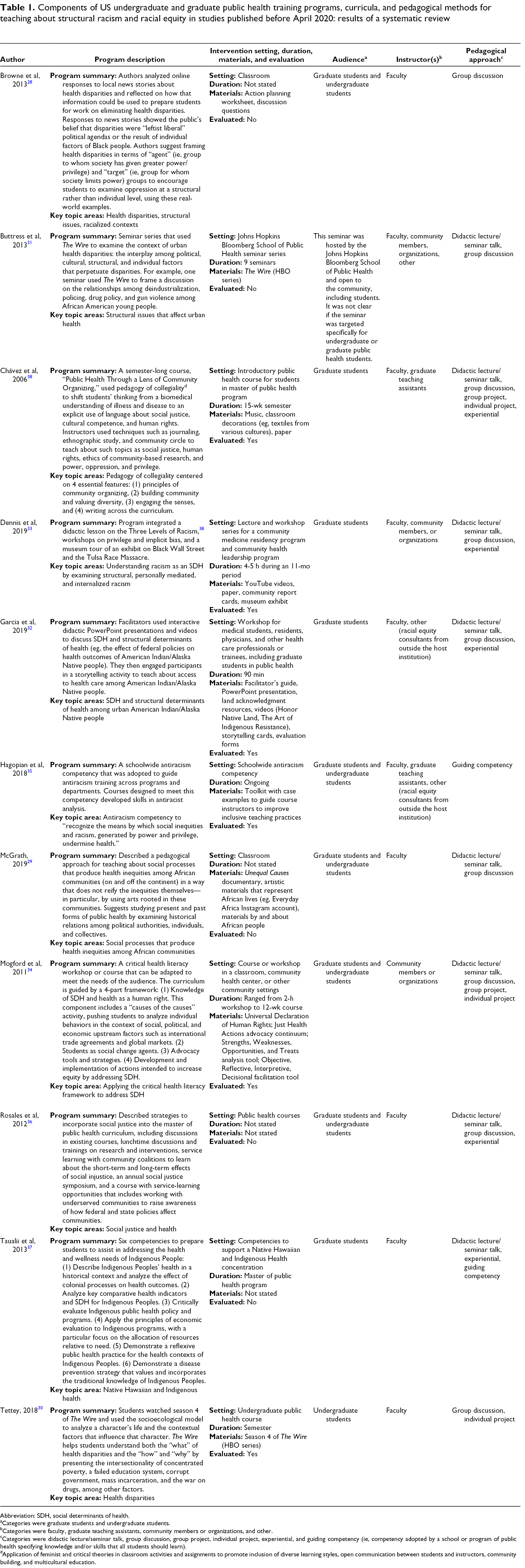
Abbreviation: SDH, social determinants of health.
aCategories were graduate students and undergraduate students.
bCategories were faculty, graduate teaching assistants, community members or organizations, and other.
cCategories were didactic lecture/seminar talk, group discussion, group project, individual project, experiential, and guiding competency (ie, competency adopted by a school or program of public health specifying knowledge and/or skills that all students should learn).
dApplication of feminist and critical theories in classroom activities and assignments to promote inclusion of diverse learning styles, open communication between students and instructors, community building, and multicultural education.
Instructional Program Format
Instructional programs included in-person classes (n = 8) 28 -30,34 -38 and workshops or seminars (n = 4). 31 -34 Instructional program durations varied, from 90-minute workshops 32 to semester-long courses. 30,38 One instructional program was designed only for undergraduate students, 30 5 were designed only for graduate students, 31 -33,37,38 and 5 were designed for both undergraduate and graduate students. 28,29,34 -36 The instructors for half the instructional programs were faculty members only (n = 5), 28 -30,36,37 whereas others included faculty members 31 -33,35,38 and a combination of graduate teaching assistants, 35,38 community members, 31,33 or other types of instructors (eg, racial equity consultants from outside the host institutions). 31,35 One instructional program was led solely by a nonprofit organization that taught critical health literacy working toward health equity. 34 Pedagogical approaches included didactic lecture/seminar talk (n = 8), 29,31 -34,36 -38 group discussion (n = 9), 28 -34,36,38 group projects (n = 2), 34,38 individual projects (n = 3), 30,34,38 worksheets (n = 1), 28 experiential learning (n = 5), 32,33,36 -38 and guiding competencies (n = 2). 35,37 All but 1 article 35 used a combination of pedagogical approaches. Materials and resources ranged widely and included in-person presentations, 32 music, 38 classroom decorations and other artistic materials, 29,38 YouTube videos, 33 a local museum, 33 documentaries, 29 television shows, 30,31 and toolkits. 35
Evaluation
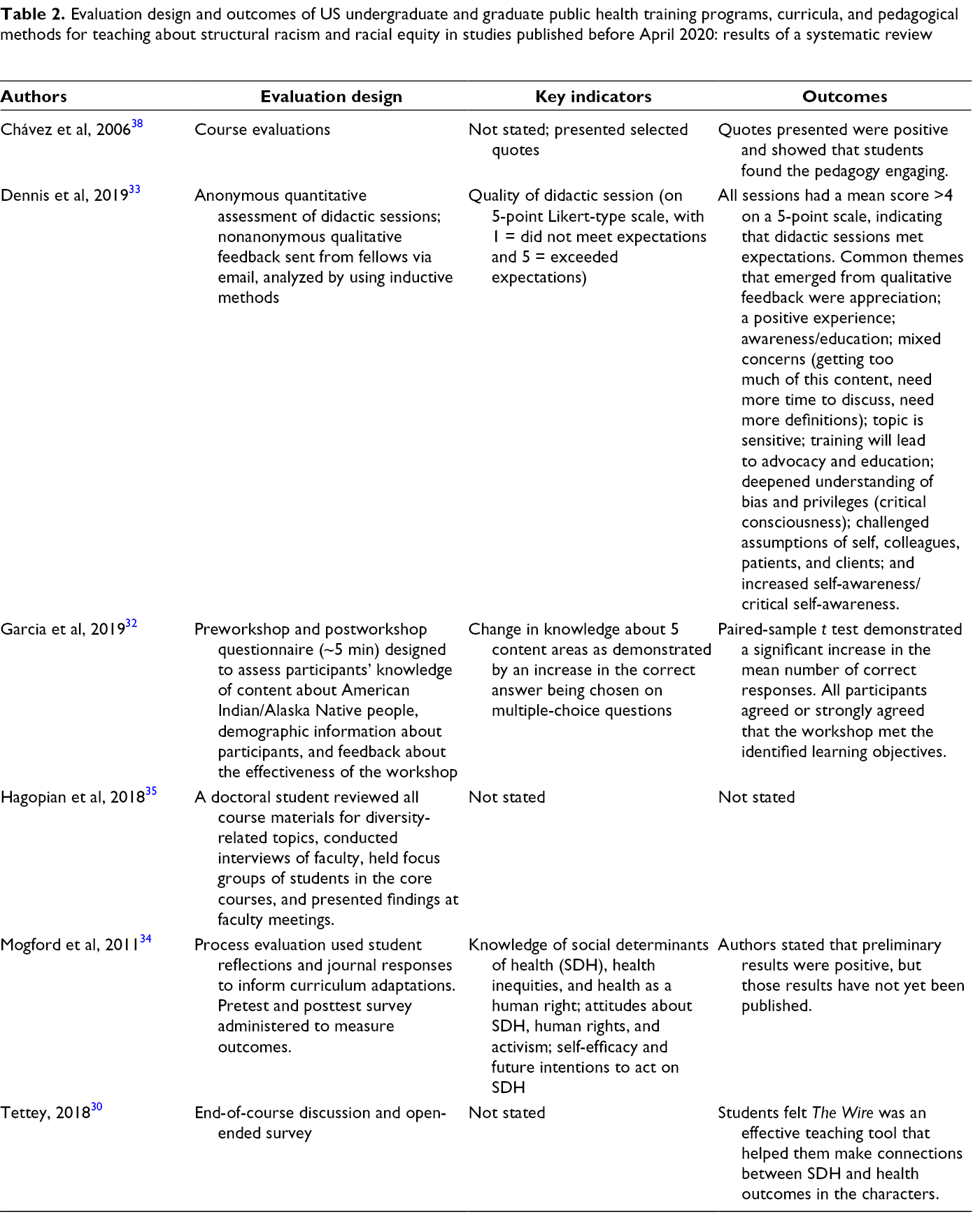
Six of the 11 programs included some form of evaluation (Table 2). 30,32 -35,38 Evaluation designs included qualitative and quantitative feedback on lessons, courses, or course offerings (n = 4) 30,32,33,38 ; pretests–posttests of knowledge (n = 2) 32,34 ; and audits of course materials (n = 1). 35 Key evaluation indicators included feedback on sessions 33,38 and knowledge of core concepts. 32,34 Key indicators were not stated in 2 articles. 30,35 Outcomes of the evaluations showed positive qualitative and quantitative feedback on sessions (eg, enjoyment of session) and self-reported increases in knowledge. 30,32,33,38 Two articles did not discuss the results of the evaluations. 34,35
Evaluation design and outcomes of US undergraduate and graduate public health training programs, curricula, and pedagogical methods for teaching about structural racism and racial equity in studies published before April 2020: results of a systematic review
Discussion
Since at least 2008, racism has been described as a structural determinant that shapes access and positionality with respect to social determinants of health. 40 Yet, the present systematic review found only 11 examples in the peer-reviewed literature that describe teaching about racism in this way, and only 7 of those examples presented any form of evaluation of teaching outcomes. The most rigorous evaluation design was a pretest–posttest in knowledge; most evaluations examined students’ emotional response to the material. Although key topic areas, settings, and pedagogical approaches for each instructional program differed, nearly all programs incorporated sociocultural content or materials to aid in students’ understanding of the historical contexts of racism in the United States.
The relative “thinness” of this literature means that as schools and programs of public health reexamine how they teach about racism and health equity, the available peer-reviewed literature provides little pedagogical guidance to inform such examination and consider changes. Schools and programs of public health must, per CEPH accreditation criteria, “explain the social, political and economic determinants of health and how they contribute to population health and health inequities,” 24 yet our findings suggest that little peer-reviewed evidence or consensus exists on how to effectively teach about racism. Individual scholars steeped in theory and research about racism as a structural determinant of health may be able to provide such education in a deep and thoughtful way (eg, threading together theory-based discussions of racism with scholarship on health disparities). However, other scholars may be ill-equipped to design course content that engages students to push past erroneous biological determinist beliefs about the origins of health disparities to understand the systems of inequity that underlie disparate outcomes. Without clear guidance on best practices and minimum standards, faculty members (who may themselves never have received such training) are left to exercise their best judgment in developing curricula on racism. Consequently, student learnings may vary.
Such concerns are not limited to education on racism as a structural determinant of health. The last decade has seen calls for more systematic and rigorous approaches to public health pedagogy, including through the development of competency-based models and learning communities on evidence-based education. 41 -43 Thus, our findings come alongside this broader movement for strengthening public health education, as increasing numbers of students pursue public health degrees. 44,45 Entering their degree programs on the heels of severe racial disparities in the COVID-19 pandemic and major national awakening around racism, incoming students will likely be aware that race is associated with health outcomes. In shaping that awareness into understanding, it will be incumbent on schools and programs of public health to provide evidence-based frameworks that contextualize race as an artificial construct with profound social meaning, not a biological fact. 5 Medicine and social work have begun to develop robust pedagogical literatures on racism as a structural determinant (often referred to as “structural competency”), which can help to inform public health thinking. 46 -50 This scholarship must be adapted to address population health but can serve as a useful starting point.
Limitations
This review had several limitations. First, we restricted our search to peer-reviewed journals, which are not the only avenue for sharing information on curricula and educational materials. Institutional websites such as those run by the Association of Schools and Programs of Public Health and the Association for Prevention Teaching and Research offer pedagogical resources to faculty. 43 Professional association meetings, such as the APHA annual meeting, also host sessions on education and pedagogy. 43 Our review omitted such gray literature sources because they are not systematically catalogued, but we acknowledge that they may contain a broader set of materials than represented here. In addition, faculty may learn about innovative pedagogical approaches from colleagues, through discussions, and by sharing syllabi. These informal networks are not documented in peer-reviewed journals yet may serve as an important source of best practices in teaching. Therefore, the dearth of literature in peer-reviewed journals found in our review should not be interpreted as a reflection on the state of teaching about racism as a structural determinant of health. Rather, it serves to show that such teaching is not well documented in the peer-reviewed literature.
A second limitation is related to the language used to describe work on racism in public health. Naming “racism” in public health research and practice was long taboo, and experts working to eliminate health disparities often took pains to find other language, perceived as more neutral, to describe their work. 5 In screening articles, we attempted to maintain a broad stance toward the kind of work that might be considered addressing racism as a structural determinant, and we did not require that the words racism or structural determinant be present to be included if the description of the focus of the program described aligned with definitions of racism and structural determinants of health. On one hand, this decision may have led to analytic imprecision in terms of what materials were included, contributing to the heterogeneity of the results. On the other hand, authors’ use of coded language to describe racism may have led us to exclude articles that otherwise would have merited inclusion.
Finally, this review focused strictly on programs, curricula, and pedagogical methods for students of public health so as to inform faculty in schools and programs of public health on effective strategies for teaching about structural racism and racial equity in the context of population health. This review did not capture information on pedagogical approaches used in other fields, including medicine, or the rich body of literature that is available to teach students about racism as a structural determinant of health. Indeed, textbooks, such as Racism: Science and Tools for the Public Health Professional 4 and Minority Populations and Health: An Introduction to Health Disparities in the United States, 51 and the growing bodies of literature on critical race theory and racism as a driver of health disparities are foundational resources that faculty may find useful as pedagogical tools.
Despite these limitations, this review—to our knowledge, the first systematic review on public health pedagogy of racism as a structural determinant of health—provides important information to the field. The breadth and interdisciplinarity of the included databases provided a wide survey of the field and explicitly included education-focused materials published outside traditional public health venues. The systematic search and screening procedure provided a rigorous methodological approach. Because this review was completed before the antiracist protests that followed the killing of George Floyd, it can provide a useful baseline for the state of peer-reviewed literature about antiracist public health education before renewed attention to racial injustice prompted schools and programs of public health to revisit health equity curricula.
Conclusion
Although a vibrant field exists of research and public health practice that understands the implications of racism as a structural determinant of health, literature on public health pedagogy on this topic is lagging. More research is needed to document how to educate public health students on the roots of the health issues they will address in their careers. Such education is critical so that the research, interventions, programs, and policies the public health workforce creates go beyond individual-level or superficial solutions, to change the systems that structure social determinants of health and subsequent health outcomes.
Footnotes
Acknowledgments
The authors thank Jon Hussey, PhD, University of North Carolina Gillings School of Global Public Health, Department of Maternal and Child Health, for providing critical feedback in conceptualizing and developing this systematic review and Mary White, MS, University of North Carolina at Chapel Hill, Health Sciences Library, for her help in developing the search strategy. We also thank reviewers for their thoughtful feedback.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Ms Chandler was supported by an award to the Carolina Consortium on Human Development from the National Institute of Child Health and Human Development (T32HD007376).