
Abstract
Health systems in Canada and elsewhere are reeling from ongoing syndemic shocks and mounting political-economic concerns that are having significant negative impacts on health equity, and on staff recruitment, wellbeing, and retention. Pressures to privatize delivery of publicly funded healthcare services in Canada are mounting, posing an additional risk to equity in access and outcomes, especially for those least well-served by current systems. This paper examines existing approaches to health system improvement and their alignment with the quintuple aim of enhancing patient experiences and outcomes, service and system efficiency, provider well-being, and health equity. Quality improvement efforts derived from private sector models such as Lean and Six Sigma have been shown, in the Canadian context and elsewhere, to add costs and negatively impact key aims such as provider well-being and patient experiences of care, though they can improve process-specific aspects of care, especially when an integrated team approach is applied in properly resourced contexts. Models that treat equity as an add-on to Lean/Six Sigma-based approaches have not been well-tested. Equity-oriented health care (EOHC) provides a promising alternative for health system improvement aligned with the quintuple aim, and is positioned as an emerging, innovative way to mitigate mounting system pressures, enhance health service effectiveness, and improve population health.
Keywords
Introduction
Health inequities – unjust and modifiable differences in health and well-being between and within groups 1 – continue to increase, 2 with SARS-CoV-2 bringing the toll of structural inequities in Canada (as elsewhere) into stark view. 3 Those facing various forms of social disadvantage and marginalization, including poverty, racism and intersecting forms of discrimination, were among the first to suffer and continue to suffer the most from the direct health impacts of COVID-19 and “long COVID”, as well as from their related effects, including financial stress, morbidity and mortality. 4 In Canada, these health and social disparities are evident across a range of health contexts and conditions, from how care is provided to older people, to increasing rates of unregulated drug poisoning-related deaths and gender-based violence3,5
These overlapping public health crises have been termed a “syndemic”, where the new disease (COVID-19) compounded and exacerbated existing conditions prompting a “simultaneous occurrence of diseases and their determinants that promote and enhance the overall negative effects on health and other conditions experienced by individuals and populations” (p. 2). 6 These syndemic effects, including long COVID, itself a stigmatized condition, 7 will continue to disproportionately affect marginalized people and increase health and social inequities. At the same time, COVID-19’s ongoing impacts are taking a significant toll on the healthcare workforce, including physical and cognitive symptoms that affect work productivity. 8
Given this evolving context, and especially the stresses on the healthcare workforce, this paper examines the political-economic landscape in which our healthcare systems have been operating, and how, in particular, the mindset and strategic priorities of “quality improvement” need revisiting. We propose equity-oriented health care (EOHC), which attends to the complexity of individual contexts and multi-faceted systems, as a primary way to mitigate this ongoing damage, protect “Canada’s most popular social program” (p. 43), 9 and re-align quality improvement with the quintuple aim’s focus on equity. 10
Quality Improvement – A Brief Review
Quality improvement (QI) – data-driven, systematic and continuous actions aimed at enhancing the efficiency, effectiveness, and safety of health care services – made an explicit appearance in Canadian federal policy documents approximately three decades ago. 11 Harrigan 12 discussing the quest for quality in Canadian health care, highlights the core value of “equality” (of access to health services), and invokes the World Health Organization’s broad definition of health, including social well-being. However, in addition to using the concept of equality rather than equity, Harrigan focused not on structural factors such as policies and social norms, but on the “non-medical determinants of health” related to an individual’s characteristics, demographics and behaviours. As ecological understandings of population health gained traction, and constructs of “accountability” were used to examine facets influencing poor health outcomes, 13 there was increasing recognition that “one size fits all” approaches do not improve effectiveness of health services, and may in fact be harmful, 14 in part by further marginalizing those already least well-served.
The last several decades have seen an infusion of private sector principles and practices into the Canada’s public sector, 9 in many cases brought in through quality improvement discourses and initiatives grounded in New Public Management (NPM) thinking. NPM features “privatization and contracting out, marketization of services still inside the public sector, and stronger performance management and manageralization” (p. 2). 15 Many Canadian provinces were early and enthusiastic adopters of NPM, 16 including in healthcare, with Alberta, Manitoba, Nova Scotia, Ontario, Quebec and Saskatchewan justifying health system reorganizations by leveraging public grievances of their perceived inefficiencies to promote the need for “centralization” as the means to “fix” ballooning budgets and improve patient care. 17 A strong sign of this has been the increased enthusiasm for private sector quality control philosophies, in particular Lean and Six Sigma. 18 The U.S. Institute for Healthcare Improvement (IHI) promotes IHI-QI that uses elements from Lean, such as total quality management and continuous improvement, geared to healthcare contexts. 19 Table 1 (first three rows) summarizes the key features of each of these quality improvement models.
Comparison of Quality Improvement Approaches.

Evidence of Effectiveness
Deblois and Lepanto’s 18 systematic review of Lean and Six Sigma in acute care found extreme variability in the quality of available evidence, with poorly operationalized definitions of core concepts such as “quality of care” and outcomes used in individual studies ranging from infection rates to reduced walking time for staff. The authors concluded that “evidence suggests that Lean and Six Sigma are better adapted to settings where processes involve a linear sequence of events” (p. 192), 18 a finding echoed by others. 20 Similarly, in their comprehensive systematic review of 22 studies, Moraros et al (p. 163) 21 concluded that “Lean interventions have: (i) no statistically significant association with patient satisfaction and health outcomes, (ii) a negative association with financial costs, and worker satisfaction and (iii) potential yet inconsistent benefits on process outcomes like patient flow . . . and safety . . .”. More recent systematic reviews of Lean, Six Sigma and related methods note the heterogeneity of studies, a lack of consistency in findings, with especially scant evidence for improvement in patient outcomes, and significant barriers to sustainability,22,23 even when including new digital technology enhancements. 24 Thus, while very specific and well-resourced implementation cases have shown some benefits of Lean thinking on process variables such as patient flow and procedure standardization, 25 the broader effectiveness of these strategies remains inconclusive. One positive finding from a systematic review of Lean methods applied in Emergency Departments (ED) is that integrating multidisciplinary teams, including their managers, in process improvement efforts shows promise as an underlying mechanism for success. 25
In Canada, Lean methods formed the basis of Ontario’s efforts to improve patient flow in EDs, 26 and Lean was broadly implemented across Saskatchewan’s health sector – at the time, claimed to be the largest such Lean implementation world-wide. 27 While official data from Saskatchewan have not been released, analysis of publicly available data found few benefits, some harms, and very poor cost effectiveness with $1 saved for every $1511 spent. 21 A follow-up survey with Saskatchewan health professionals working during the implementation period found the major barriers to uptake included insufficient training and lack of resources; nurses indicated that the new processes increased their workloads. 28 In Quebec, an open letter from over 200 health professionals decried the use of Lean – what they referred to as “the Toyota method” – as authoritarian, and against the best interests of providers and patients, especially those most affected by inequities. 29 An analysis of this implementation identified a key barrier to effective implementation as poor understanding of contextual factors noting that “implementation tended to be isolated, driven by efficiency targets, and unable to trigger cultural change” (p. 37). 30
Ontario’s ED implementation showed modest improvements over time in selected outcomes (eg, wait times and left-without-being-seen rates), but no differences when comparing Lean to control EDs. 26 A critical ethnographic study of some of these EDs found that “the emphasis on wait times resulted in more importance being placed on ‘getting the patient out’ of the ED than on providing safe, compassionate, person-centred medical care” (p. 56). 31 Patients, especially those with multiple, often stigmatizing chronic conditions (eg, substance use disorders, obesity related illness, mental illness), became the focus of blame for increased costs and stresses on the ED. Provider stress related to efficiency instead of effectiveness, its impacts on perceptions of patients and their care, along with the implicit bias directed against “complex” patients is antithetical to health equity goals.
The IHI-QI approach imports Lean-based ideas into healthcare QI; it discusses “Profound Knowledge”, which comes from closeness to process, emphasizes that health settings are varied and complex, better integrates human behaviour and motivations than business-oriented Lean work, and attempts to specify a theory of action. 19 However, only recently does it mention equity, 32 but other than descriptive case studies on the IHI website, it is difficult to find empirical evidence of IHI-QI’s effectiveness on any outcome, or specific to health equity. 33
The Quintuple Aim and Equity-Oriented Health Care – A Complexity Lens
Equity-oriented health care (EOHC) is an emerging strategy to reduce the effects of structural inequities that sustain health inequities (eg, how poverty impedes healthcare access), the impacts of multiple forms of racism, discrimination and stigma on the quality of care delivered, and the frequent mismatches between conventional models of care and the needs of people most impacted by inequities. As conceptualized through ongoing research, EOHC aims to improve organizational processes and policies, and individual practices, by enacting evidence-based and theoretically-informed strategies supported by practice and learning resources. These are operationalized through three key dimensions and ten tailored strategies (Table 2; Figure 1). This work is grounded in initial studies in urban primary care sites whose explicit mandates are providing comprehensive care to Indigenous Peoples, and subsequent studies have been co-led by Indigenous Elders, and policy, administrative and clinical leaders, with one explicit goal being to address anti-Indigenous racism. 35
Key Dimensions of Equity-Oriented Health Care – The EQUIP Model.

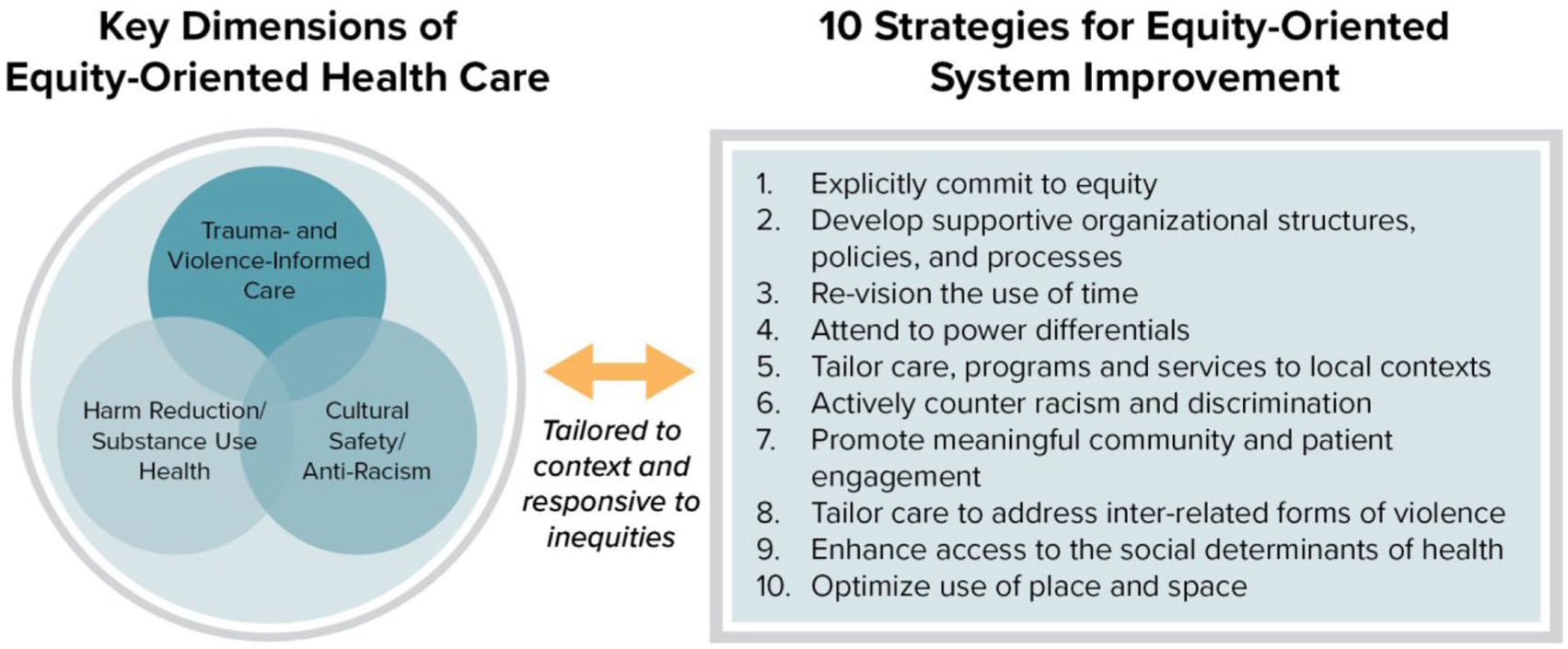
EQUIP’s key dimensions of equity-oriented health care.
Complexity theory views health systems as complex adaptive systems, that is, networks of interconnected people, organizations, and processes that continuously evolve and respond to change. Complexity theory recognizes that outcomes are often unpredictable, non-linear, and shaped by interactions across multiple levels of the system. 36 Based in this understanding, EOHC encourages flexibility and tailoring when implementing this complex intervention into complex healthcare settings. This two-way complexity means attending to intervention and site features that interact and influence one another; these interactions include and extend beyond the patient-provider to the organizational and policy levels of healthcare. Given the consistency in the literature on the importance of addressing complex contextual factors when implementing such initiatives,37,38 EOHC’s focus on ten strategies tailorable to the setting (Figure 1) are a key implementation feature.
In primary care settings in Ontario and British Columbia (BC), provinces with among the highest and most diverse, and under-served, populations in Canada,39,40 EOHC was associated with better patient-reported health outcomes over time, and with improvements in staff confidence and comfort with providing EOHC.34,41,42 Analysis of funding sources and policies in participating sites demonstrated how integrating attention to equity (eg, by attending to performance indicators at multiple levels) influences an organization’s ability to plan and deliver EOHC. 43
Recognizing that emergency departments in Canada play a significant role in responding to population health needs in tandem with the primary care sector, the EQUIP Healthcare research team, which designed and evolved the present EOHC model, studied the feasibility and effectiveness of implementing EOHC in three diverse EDs in BC. 35 In doing so, they found that the site that managed, during the COVID-19 pandemic and other disruptions, 44 to implement EOHC most robustly demonstrated significant reductions in their rate of patients leaving without their care completed, 45 a key indicator used in ED, 46 including Lean-ED, studies.
Reflecting on the findings of Lean-related implementations reviewed above, it is in large part contextual factors that determine what is possible in terms of sustainable organizational change. These factors include: who is visiting the ED and why, what social and health system factors are influencing ED use, the mismatch between why many present in ED and the kinds of services EDs are designed to provide, and how an individual team, department and hospital, including its staff, leadership and policies, understand these inter-related problems. At the same time, staff working in conditions of stress, vicarious trauma, moral distress and uncertainty are often put into a position to decide who may be most deserving of care, leaving space for stigmatizing assumptions (eg, about substance use) to drive these decisions.
Given promising results across settings, EOHC is positioned as a promising equity-promoting approach to changing health systems that have not been designed to acknowledge or address inequities. 47 Unlike Lean-based QI methods, EOHC also aligns theoretically and empirically with the quintuple aim of healthcare improvement by enhancing patient experiences and outcomes, efficiency, provider well-being, and health equity. 10
Implications
In Canada, we have seen some moves to address aspects of syndemic impacts including, for a time, government resources to combat the ongoing unregulated drug poisoning and gender-based violence crises. However, while calls have abounded to “build back better” using structurally competent systems-level reforms and interventions 48 – that is, truly transformative approaches – we now see evidence of backsliding to entrenched New Public Management positions grounded in austerity, despite record health care funding transfers from the federal government to provinces delivering health care.9,49 While some forms of public-private partnerships can benefit cost and process efficiencies, there is instead accelerated profitization, 8 with public funds actively diverted from core services into for-profit long-term care, surgical clinics, pharmacies and nursing agencies.50,51 In fact, Hedden and McGrail (p. 293) 49 argue that “the best defence [to privatization] is a good offence” that includes protective legislation with transparency around payment arrangements and accountabilities regarding how service models align with the Canada Health Act, especially with regards to access and equity. As they conclude, private delivery of publicly funded primary care is antithetical to health equity.
Equity-Oriented Health System Improvement
A health equity lens draws attention to the structural context of health and healthcare and indeed is a precursor to understanding what needs to change. For those starting to consider equity-promoting change, this means considering how both social arrangements and healthcare delivery create disproportionate harm for some groups; both from inter-related negative health impacts, and from unintended consequences of inequitable policy responses. Equity-oriented health system improvement explicitly starts with equity values and goals, such as those operationalized through EOHC’s key dimensions and strategies (Figure 1). An equity lens prompts the following types of questions at any level of a system or organization:
(1) Recognizing the risks and consequences of discrimination and stigma, deepening inequities, and their disproportionate effects on certain groups, how can policy and practice responses be tailored to benefit people who experience health inequities?
(2) How can evidence-based knowledge about effective equity-oriented approaches be mobilized in the service of counteracting the ongoing and harmful intersecting forms of systemic inequities that people experience in heath care?
(3) How do peoples’ experiences of systemic and interpersonal violence affect access to and use of needed health and social services (safe housing, immunizations, primary care, etc.)? How can this be accounted for in the design and delivery of services?
(4) What strategies are needed to actively counteract harm? What are the effects of implementing these strategies in health systems?
Common elements that EOHC shares with the other QI approaches in Table 1 include engagement of all actors in developing and driving change based on close examination of process and using data to assess needs, iterate in real time, and measure success – indeed these are some of the processes underlying Lean-based implementations in EDs with some success. 25 EOHC additionally focuses on: (a) enhancing care for those most affected by inequities, and (b) counteracting the ongoing impacts of structural and systemic violence that limit people’s access to healthcare and their experiences in health settings. 52
Key lessons from evolving and evaluating EOHC implementations can help re-articulate tools like the Plan-Do-Study-Act (“PDSA”) 19 for equity-promoting work. First, the emphasis on “front-line ownership” 53 in the belief that those closest to the process of care are best placed to identify and implement change, while important, is insufficient. In the context of pressurized work environments, staff must be supported by resources, policies and engaged leaders, a finding in EQUIP research, as well as Lean-based studies.23,25 Second, equity work is disruptive; while opportunities for positive change arise, disruptions need to be anticipated and buffered. 34 Third, time and timing are crucial; in studying primary care and ED contexts, it was evident that unfolding the implementation over too long a period can dilute its effect. An intensive “bottom-up and top-down” intervention with attention to long-term sustainability through ongoing education and integration, human resource practices, etc., is recommended. Finally, the key dimensions of EOHC have proven adaptable to diverse contexts and are a useful way to integrate attention to inequities within complex adaptive systems, 54 toward greater service and system effectiveness, and population health.
Keeping equity at the forefront of system improvement moves beyond QI and status quo attempts to simply improve current practice. In the face of new austerity measures, and the frayed social safety net emblematic of ongoing neoliberal interventions, the need to sustainably embed health equity into health services is urgent. EOHC is therefore both a “call to action” 54 and a set of strategies responsive to those most in need of equity-promoting care, that improves patient satisfaction and outcomes 41 and staff capacity,34,47 and even shifts important administrative metrics, 45 addressing four aspects of the quintuple aim of health system improvement. As yet, system cost/efficiency data for EOHC are not available, nor are findings from larger implementations across multiple organizations or systems of care, though some work examining the scalability of EQUIP’s EOHC model is underway. 55 Research on equity-first approaches to improvement in other contexts is urgently needed, as are analyses of how the various contextual factors that can influence success interact. Health system improvement efforts, as noted, are complex, and require balancing tensions among what are often competing demands to achieve meaningful gains across the five aims, for example, how to support staff autonomy and judgement (within scopes of practice) in caring for those with complex needs, while also keeping costs within specific targets, especially in the context of austerity; or how to give each patient the time they require while managing flows through already overwhelmed EDs. We do not intend to gloss over these tensions but rather argue that approaches grounded in core values like equity and human rights can bring clarity to identifying goals and operationalizing how to achieve them in these complex decision spaces.
Conclusion
While other equity-focused work has long existed in specific contexts outside of Canada (eg, Alaska’s Nuka System 56 ), and some systems of care within Canada are mandated to support highly marginalized groups (eg, community health centres), more recent calls note the need to expand equity actions across all aspects of Canadian healthcare. 57 Not just “nice to have”, equity-oriented health care is the essential fifth point on the “star” 58 of the quintuple aim and truly transformative quality improvement; it is a way to mitigate the larger threats to publicly funded health care in Canada and beyond.
Footnotes
Acknowledgements
CNW and VB re supported by the Canada Research Chairs Program.
Author Contributions
CNW conceived of an wrote the paper with ongoing input from AB and review and discussion of manuscript versions by VB, EW and CV. All authors approved the final submitted manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.