
Abstract
Objectives:
Veteran homelessness has declined in the past decade, but the proportion of unsheltered homeless veterans has increased. We identified characteristics of unsheltered homelessness in a large contemporary veteran cohort and examined outpatient and inpatient encounters before and after intake to US Department of Veterans Affairs (VA) homeless programs.
Methods:
National data from the Homeless Operations Management Evaluation System (HOMES) database and the Corporate Data Warehouse were analyzed on 191 204 veterans experiencing housing instability from January 2018 through December 2021. We used hierarchical multivariate logistic regressions to model associations between sheltered status and veteran correlates. Repeated-measures analysis of variance assessed changes in care utilization after intake in homeless programs.
Results:
Age <50 years (odds ratio [OR] = 1.3; 95% CI, 1.2-1.4), Hispanic ethnicity (OR = 1.2; 95% CI, 1.1-1.3), some college education (OR = 1.1; 95% CI, 1.0-1.1), and a bachelor’s degree (OR = 1.2; 95% CI, 1.1-1.2) were associated with veteran unsheltered homelessness. Unsheltered veterans were more likely to have a VA service-connected disability (OR = 1.4; 95% CI, 1.4-1.5), military sexual trauma (OR = 1.1; 95% CI, 1.0-1.1), and/or combat exposure (OR = 1.1; 95% CI, 1.0-1.1). Unsheltered and sheltered homeless veterans had an increase in outpatient encounters and a decrease in inpatient care after intake to the VA homeless program.
Conclusions:
Contemporary unsheltered homeless veterans are younger and Hispanic with some college education. Innovative public health approaches that better engage and reduce barriers to entry need to be tested for a diverse unsheltered homeless population.
While the overall number of people experiencing homelessness in the United States was relatively consistent from January 2020 through January 2022, the proportion of unsheltered homelessness increased by 3%. 1 The Federal Strategic Plan to Prevent and End Homelessness has underscored the rise in unsheltered homelessness across the country and has consequently prioritized the need for strategies to help response systems address this crisis. 2 Homelessness in the United States is a public health problem that spurs much debate. 3 In 2022, a minimum of 582 462 people in the United States reported homelessness, and this number is expected to increase as a repercussion of recent economic downturns, scarcity of affordable housing, and numerous other community shortfalls.4-6 Some forms of homelessness are more publicly visible than others, ranging from sleeping unsheltered in public spaces not meant for human habitation (eg, abandoned buildings, cars, encampments) to staying in shelters or residing with others.3,7 An estimated 40% (n = 232 980) of homeless people were sleeping unsheltered on a single night in January 2022. 6 As unsheltered homelessness has become more visible, the number of state and local laws that criminalize certain activities, such as sleeping in public, has increased. 1
Nearly 70% of people experiencing chronic homelessness remain unsheltered throughout their homelessness, exacerbating existing health conditions and increasing the risk of premature death.7-9 Studies have found that unsheltered homeless adults tend to be sicker 6 and have a higher comorbidity of physical illness, mental health conditions, substance use, and trauma than sheltered homeless adults.10,11 Despite poorer health status than the general US population, unsheltered people often lack continuity in access to preventive medicine and care, relying on emergency services to meet their care needs.12,13 As such, differences may exist in the types of health care services that unsheltered and sheltered homeless adults use; however, few studies to date have compared their use.
US veterans represent about 7% of the total US population and account for about 8% of people experiencing homelessness.14-16 While homelessness among veterans has declined dramatically in the past decade, the proportion of unsheltered homeless veterans has increased in recent years.17,18 Risk factors for unsheltered homelessness among veterans include multiple diagnoses of physical and mental health conditions,3,12 substance use disorder (SUD), 7 and past incarceration. 3 Studies have reported low outpatient utilization 12 but high health care spending 11 and all-cause mortality 10 among this population. According to several studies, unsheltered homeless veterans are predominantly White, male, and aged >50 years; have an SUD; and live in extreme poverty without access to US Department of Veterans Affairs (VA) benefits.12,19 While the literature has provided some insight into the unsheltered homeless veteran population, research has been limited to specific communities and small sample sizes and may no longer be current within the context of the broad demographic changes in the veteran population. For example, 1 study focused on veterans who screened positive for homelessness but were not necessarily using VA homeless services, which presents a different set of questions than focusing on users of VA homeless services. 12 Another recent study was informative but surveyed only unsheltered homeless veterans receiving primary care. 3 A need exists for a contemporary characterization of the sociodemographic and clinical characteristics of unsheltered homeless veterans, especially as the overall veteran population has become more gender and racially and ethnically diverse during the past decades.20-22 An examination of the differences in VA health care use between sheltered and unsheltered homeless veterans would also provide insight into whether unsheltered homeless veterans use costly services at a higher rate than sheltered homeless veterans, which would further support dedicating resources (ie, outpatient services) to address their unsheltered homeless status.
We analyzed data from a large national sample of homeless veterans in the VA health care system to compare unsheltered and sheltered homeless veterans. Our objectives were to (1) identify sociodemographic and clinical characteristics associated with unsheltered homelessness among veterans and (2) examine changes in outpatient and inpatient use among veterans experiencing unsheltered and sheltered homelessness over time. A comprehension of the contemporary characteristics associated with veteran unsheltered homelessness is not only important from an epidemiologic standpoint but may also inform policy efforts.
Methods
The VA operates a continuum of homeless programs and tracks data on use of these programs in the Homeless Operations Management Evaluation System (HOMES) database, which allows identification of veterans in various states of housing instability and homelessness. In this study, we focused on veterans who were recorded as experiencing unsheltered homelessness or staying in an emergency shelter, and we excluded veterans in other categories (eg, veterans at risk of homelessness in rapid rehousing programs, veterans in transitional housing). This study included unsheltered and sheltered homeless veterans who completed an intake documented in the HOMES database during the study period, January 1, 2018, through December 31, 2021. The HOMES database is an in-depth assessment that collects information about veterans’ demographic characteristics and needs; veterans complete the assessment upon entry into VA homeless programs. 9 Emergency shelters are facilities that offer temporary shelter for people experiencing homelessness. This study sample was restricted on the basis of answers to the following HOMES intake question, “Where were you residing prior to today (where did he/she sleep last night)?” Veterans who responded “a place not meant for habitation (eg, a vehicle, abandoned building, outside)” were considered unsheltered, and veterans who had stayed in an “emergency shelter, including hotel paid for with emergency shelter voucher” were considered sheltered. We excluded from analyses other veterans experiencing housing insecurity (eg, staying in a medical facility, prison/jail, nursing home, with family/friends).
We extracted data from HOMES and the Corporate Data Warehouse 23 —a national repository of clinical, administrative, and financial data from VA medical facilities—on the following demographic characteristics: age (17-29, 30-39, 40-49, 50-59, 60-69, ≥70 y), sex (male, female), race and ethnicity (non-Hispanic White, non-Hispanic Black, Hispanic, non-Hispanic other/multiracial), marital status (married/partnered, single/never married, divorced/separated, widowed), education (less than high school diploma, high school diploma, some college, bachelor’s degree or more), percentage of VA service-connected disability (<10%, 10% to <50%, ≥50%), 24 combat exposure (yes or no), and experience of military sexual trauma (yes or no). A service-connected VA disability indicating ≥50% indicates an injury or illness attributed to military service. For each veteran in our cohort, the index date was the date of the first HOMES assessment completed during the study period. We also used the Corporate Data Warehouse to extract veterans’ medical records for 6 months before and after the HOMES index date to examine patterns of health care use and identify the presence of mental health disorders and SUDs, using codes from the International Classification of Diseases, Tenth Revision. 25 The VA Institutional Review Board considered this study not human subjects research because of the lack of interaction with, or collection of identifiable information about, human subjects and because it was conducted as part of public health surveillance based on deidentified data.
Analysis Plan
We first conducted bivariate comparisons using the Pearson χ2 test to compare characteristics of sheltered and unsheltered homeless veterans at admission to VA homeless programs, with P < .05 considered significant. Then, using repeated-measures analysis of variance, we analyzed Corporate Data Warehouse data to compare service use in the 6 months before the veteran’s HOMES intake date with that in the 6 months after this assessment. We further examined before-and-after service use by sheltered versus unsheltered status. We conducted the repeated-measures analysis of variance with time (before and after assessment) and sheltered status entered as main effects and with time × sheltered status entered as an interaction effect. Lastly, we conducted hierarchical multivariate logistic regressions to model associations between sheltered status and sociodemographic characteristics, clinical characteristics, and health care use. We conducted all analyses using SAS version 9.4 (SAS Institute Inc).
Results
Of 191 204 veterans who completed a HOMES assessment, 77 835 (40.7%) met the eligibility criteria to be included in the study analysis. Of these, 51 920 veterans were documented at intake as experiencing unsheltered homelessness and 25 915 as experiencing sheltered homelessness.
When compared with sheltered homeless veterans, unsheltered homeless veterans were significantly more likely to be male (91.0% vs 90.1%), younger (aged 17-29 y, 5.7% vs 4.0%; aged 30-39 y, 16.2% vs 12.8%), Hispanic (10.7% vs 8.5%), and with higher education levels (some college, 43.8% vs 41.9%; bachelor’s degree or more, 12.3% vs 11.0%; all P < .001) (Table 1). A significantly higher proportion of unsheltered homeless veterans than sheltered homeless veterans (33.1% vs 24.9%; P < .001) had a VA service-connected disability rating ≥50%. Unsheltered homeless veterans were also significantly more likely than sheltered homeless veterans to have experienced combat exposure (26.3% vs 21.8%) or military sexual trauma (10.4% vs 9.7%) and to have a diagnosis of posttraumatic stress disorder (20.8% vs 17.8%; P < .001 for all).
Characteristics of sheltered and unsheltered homelessness among veterans in the United States (N = 77 835), January 1, 2018, through December 31, 2021 a
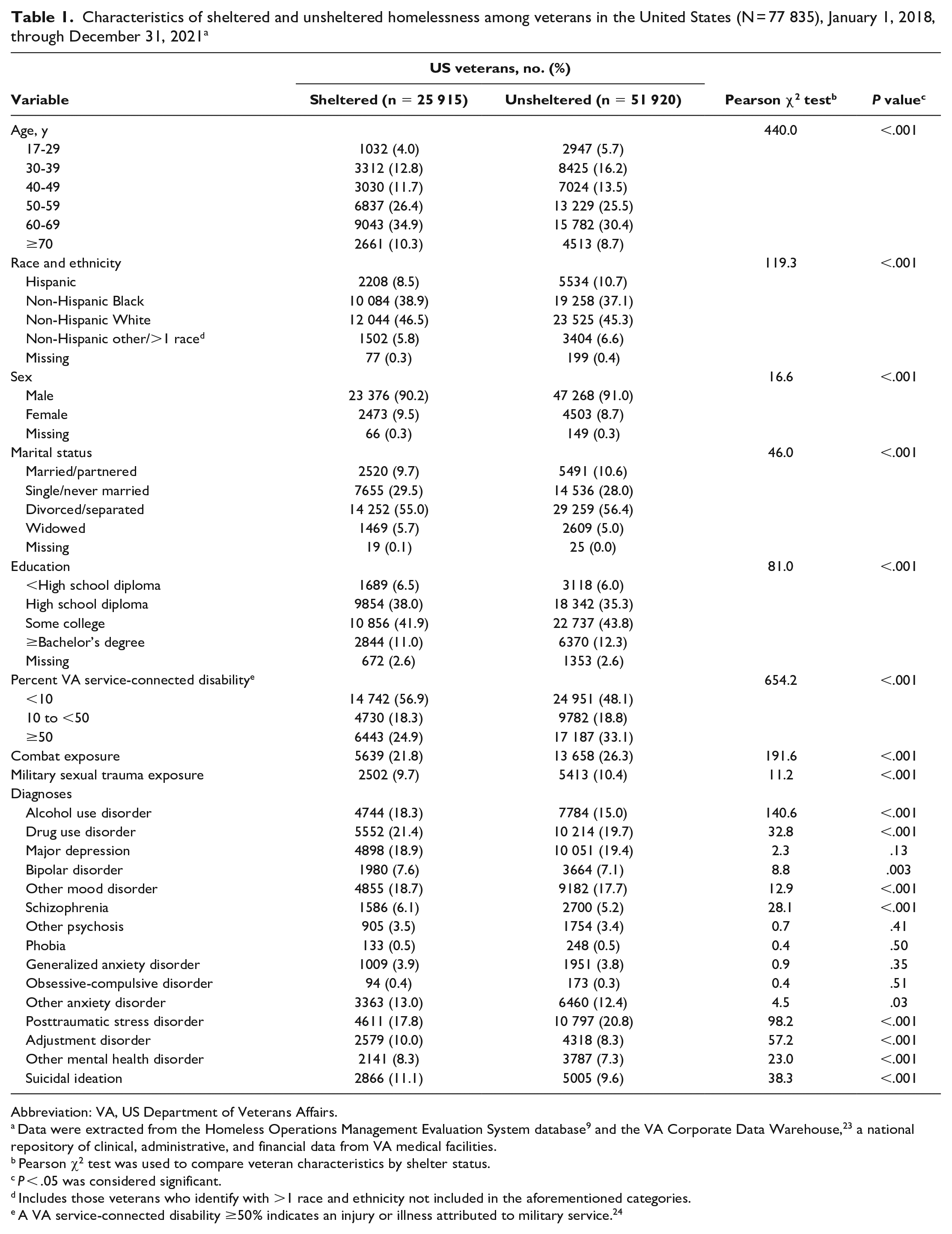
Abbreviation: VA, US Department of Veterans Affairs.
Data were extracted from the Homeless Operations Management Evaluation System database 9 and the VA Corporate Data Warehouse, 23 a national repository of clinical, administrative, and financial data from VA medical facilities.
Pearson χ2 test was used to compare veteran characteristics by shelter status.
P < .05 was considered significant.
Includes those veterans who identify with >1 race and ethnicity not included in the aforementioned categories.
A VA service-connected disability ≥50% indicates an injury or illness attributed to military service. 24
Several behavioral health conditions were significantly more prevalent among sheltered homeless veterans than among unsheltered homeless veterans: 18.3% vs 15.0% had a diagnosis of alcohol use disorder; 21.4% vs 19.7% reported drug use disorder; 6.1% vs 5.2% were diagnosed with schizophrenia; 10.0% vs 8.3% had adjustment disorder; and 11.1% vs 9.6% reported suicidal ideation (all P < .001) (Table 1).
Comparing the 6 months before with the 6 months after admission to VA homeless programs, we found significant changes in health care use among unsheltered and sheltered homeless veterans over time. We noted increases in receipt of the following services in both groups after initial assessment: outpatient mental health (F = 30.82, P < .001), rehabilitation (F = 6.48, P = .01), and emergency department/urgent care (F = 4.17, P = .04) (Table 2). We also identified in both groups a significant change in outpatient homelessness encounters after assessment, although the increase in homelessness services among the sheltered cohort was larger than the increase among the unsheltered cohort (F = 147.42, P < .001). Both groups showed a decrease in mental health inpatient admissions over time, with the sheltered cohort demonstrating a larger decline than the unsheltered group (F = 13.67, P < .001). We revealed no significant changes between the groups across the remaining outpatient and inpatient services of interest.
VA health care encounters, by sheltered and unsheltered homelessness among veterans, before and after intake to VA homeless programs, United States, January 1, 2018, through December 31, 2021 a
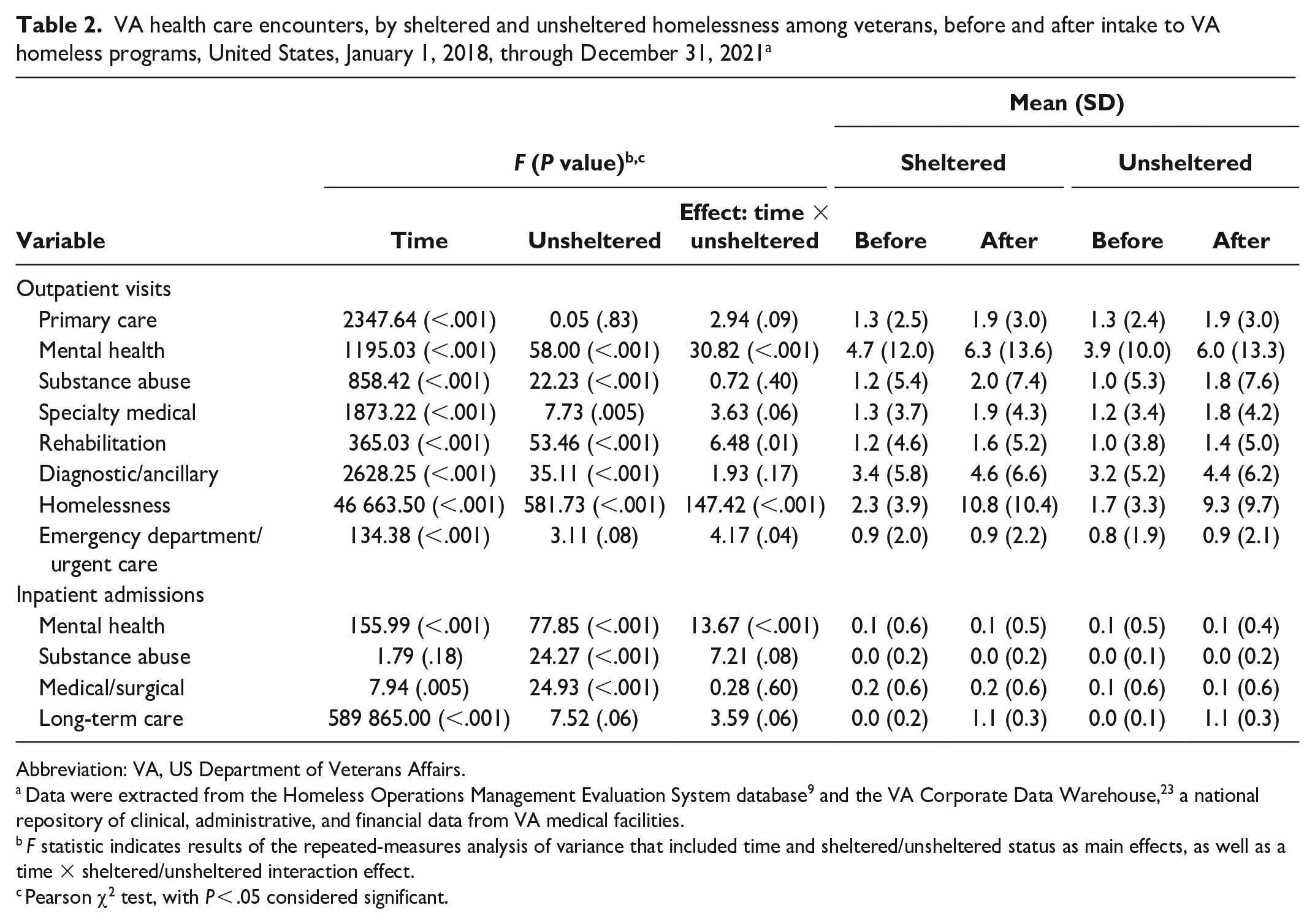
Abbreviation: VA, US Department of Veterans Affairs.
Data were extracted from the Homeless Operations Management Evaluation System database 9 and the VA Corporate Data Warehouse, 23 a national repository of clinical, administrative, and financial data from VA medical facilities.
F statistic indicates results of the repeated-measures analysis of variance that included time and sheltered/unsheltered status as main effects, as well as a time × sheltered/unsheltered interaction effect.
Pearson χ2 test, with P < .05 considered significant.
In the multivariable analyses, being younger (aged <50 y; odds ratio [OR] = 1.3; 95% CI, 1.2-1.4), being Hispanic (OR = 1.2; 95% CI, 1.1-1.3), and having some college education or a bachelor’s degree or more (OR = 1.2; 95% CI, 1.1-1.2) were associated with unsheltered homelessness (Table 3). Veterans who were older, female, and single/never married had reduced odds of unsheltered homelessness.
Correlates of unsheltered homelessness among veterans in the United States, January 1, 2018, through December 31, 2021 a
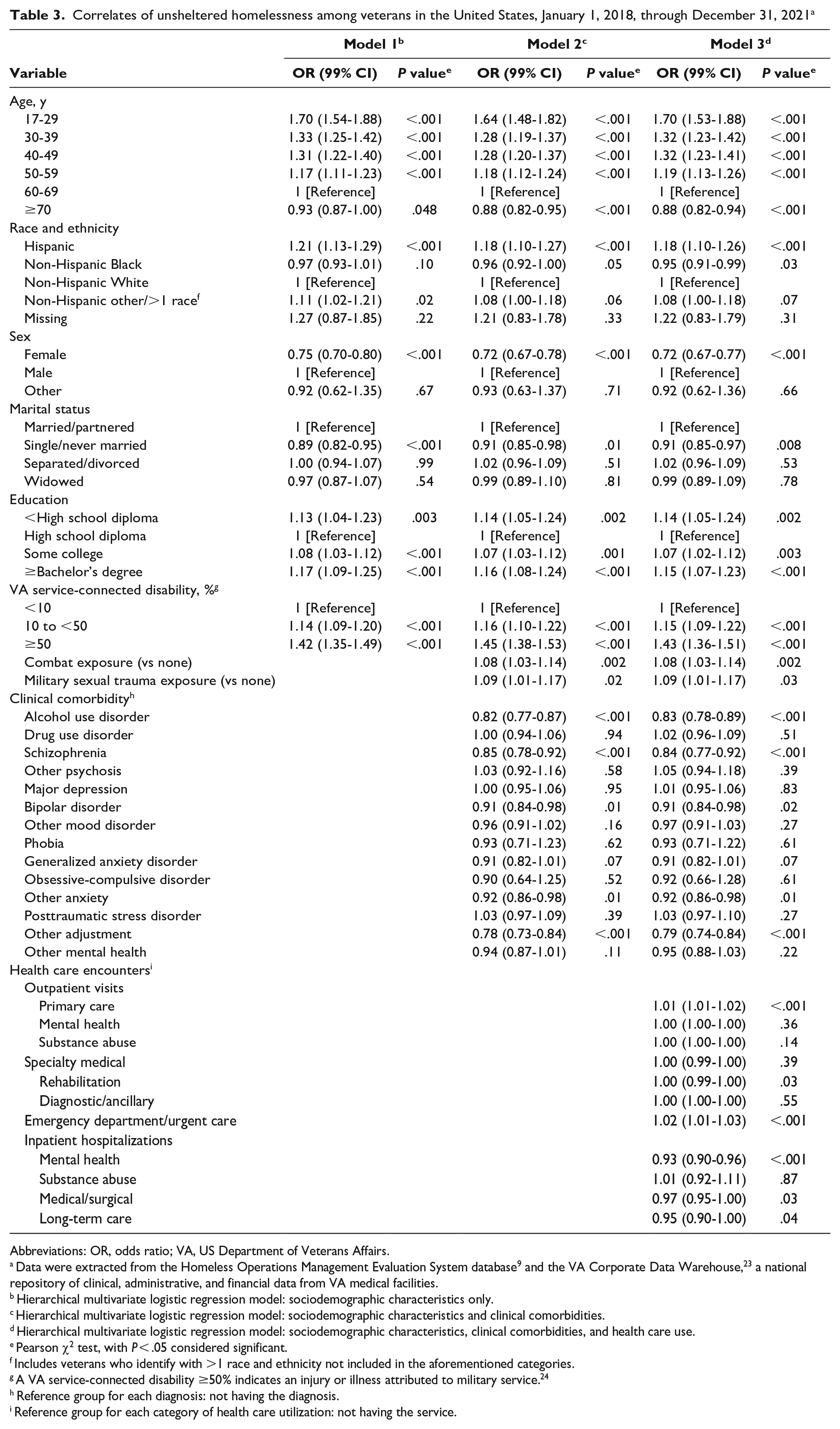
Abbreviations: OR, odds ratio; VA, US Department of Veterans Affairs.
Data were extracted from the Homeless Operations Management Evaluation System database 9 and the VA Corporate Data Warehouse, 23 a national repository of clinical, administrative, and financial data from VA medical facilities.
Hierarchical multivariate logistic regression model: sociodemographic characteristics only.
Hierarchical multivariate logistic regression model: sociodemographic characteristics and clinical comorbidities.
Hierarchical multivariate logistic regression model: sociodemographic characteristics, clinical comorbidities, and health care use.
Pearson χ2 test, with P < .05 considered significant.
Includes veterans who identify with >1 race and ethnicity not included in the aforementioned categories.
A VA service-connected disability ≥50% indicates an injury or illness attributed to military service. 24
Reference group for each diagnosis: not having the diagnosis.
Reference group for each category of health care utilization: not having the service.
A VA service-connected disability, a history of combat exposure, and exposure to military sexual trauma were associated with increased odds of unsheltered homelessness (Table 3). While diagnoses of alcohol use disorder, schizophrenia, bipolar disorder, other anxiety disorder, and adjustment disorder were significantly associated with lower odds of unsheltered homelessness, the remaining mental health diagnoses were not.
Unsheltered homelessness among veterans was associated with a higher use of outpatient primary care (OR = 1.01; 95% CI, 1.01-1.02) and emergency department (OR = 1.02; 95% CI, 1.01-1.03) services than among sheltered homeless veterans. However, the unsheltered group was associated with significantly lower use of outpatient mental health and rehabilitation services, inpatient mental health services, medical/surgical services, and long-term care services as compared with sheltered homeless veterans.
Discussion
Unsheltered homelessness is a public health problem that is a complex sociopolitical phenomenon involving a measurable stack of intertwined personal and community-level factors. This study compared sociodemographic, clinical, and health care use characteristics of unsheltered and sheltered homeless veterans. Our findings indicate that contemporary characteristics of unsheltered homeless veterans now extend beyond those attributes of the past12,23 to veterans who are younger, are of Hispanic ethnicity, have higher education levels, and have a VA service-connected disability. Similar to previous literature, 12 we found low rates of VA outpatient use among unsheltered homeless veterans and that sheltered and unsheltered homeless veterans increased their VA service use over time.
Our study highlights some important differences between unsheltered and sheltered homeless veterans that should be considered given the recent federal initiative to develop effective strategies to reduce homelessness by 2025, 2 such as ALL INside. 26
Unsheltered homelessness is no longer limited to older, White, male veterans living without VA benefits or in extreme poverty; rather, unsheltered homelessness has extended its reach to younger, educated veterans who may become homeless shortly after exiting the military. 27 These findings may reflect the broader demographic changes in the veteran population and of changing immigration patterns in the general US population. Projected estimates indicate that while the veteran population will decline from 19.5 million (2020) to 13.6 million (2045), Hispanic veterans will double in proportion during this period. 28 With the VA’s new evolved data collection tools and increased emphasis on accurate recording of demographic characteristics,29,30 better data on race and ethnicity will be captured in the unsheltered homeless veteran population. Between 2020 and 2022, homelessness among people identifying as Hispanic or Latino in the general population concurrently increased by 8%, with a 16 percentage-point increase among those who are unsheltered. 31 These findings also indicated that Latino and Hispanic homeless veterans are more likely than non-Hispanic homeless veterans to be experiencing their first homelessness event 31 and may face various racial and ethnic cultural barriers when attempting to access VA services; thus, they may be less knowledgeable about the VA’s homeless program resources, which could be improved by increasing culturally sensitive outreach efforts.
In our study, education did not have a protective effect: among younger veterans, those who had higher education levels were at an increased risk for unsheltered homelessness. This finding conflicts with popular opinion that homelessness is a repercussion of individuals who have low levels of education. 6 The repercussions of the COVID-19 pandemic should not go without mention. The United States has experienced a simultaneous increase in unemployment rates and evictions and decrease in affordable housing, 6 which may be contributing to new diverse generations of unsheltered homeless adults. However, more research is needed to examine the causes of these trends. Furthermore, our findings demonstrated that as VA service-connected disability compensation increased, so did the likelihood of unsheltered homelessness. Studies have identified a lack of disability income or extreme poverty as a primary predictor of unsheltered homelessness, but our finding indicates that even when veterans have access to VA disability benefits, more complex resources are still needed to prevent unsheltered homelessness.3,12 Despite efforts designed to increase outreach and direct services to the unsheltered homeless population, the nation has not been able to avoid the prevailing trend of unsheltered homelessness. Our findings support that the reasons for this trend may be complex and interrelated32,33: economic factors, such as stagnant wages and lack of affordable housing, as well as social factors, such as an increase in family dissolution and social isolation in society, may increase the risk of unsheltered homelessness as young veterans leave active duty and attempt to reintegrate into society.
Our findings demonstrate that having a history of military sexual trauma and/or combat exposure was positively associated with unsheltered homelessness.34,35 In our study, a mental health diagnosis, including SUD, was inversely associated with unsheltered homelessness. This finding may be driven by differences between homeless veterans who seek VA care and the unsheltered population that is often difficult to engage in these same services.36,37 Mental health conditions may be underdiagnosed in the unsheltered population because of a lack of service use. The VA offers an array of programs that mitigate homelessness among veterans from multiple backgrounds and with various needs. In an effort to mitigate homelessness and engage unsheltered homeless veterans, the VA offers a Grants Per Diem Low Demand model 38 and a Health Care for Homeless Veterans Safe Haven model, 39 both of which are aligned with the federal strategic plan ALL INside 26 in reducing programmatic and regulatory barriers that systematically delay access to housing among this population. Future longitudinal studies are needed to examine the impact of the Low Demand and Safe Haven models in engaging unsheltered homeless veterans in housing and clinical services.
Unsheltered and sheltered homeless veterans demonstrated an increase in VA outpatient use after the HOMES assessment. Specifically, our findings showed a positive increase in outpatient mental health and rehabilitation services and a decrease in inpatient mental health use during the same time frame. While we observed a positive change in homelessness services in both groups after assessment, the sheltered homeless group demonstrated a sharper increase in these encounters. These findings may reflect the time that it takes for unsheltered homeless veterans to engage in and trust VA health care services. 12 Future longitudinal studies are needed to assess whether the decline in inpatient admissions is a result of increased access to outpatient care and/or housing.
Limitations
This study had several limitations. First, our analysis was limited to veterans who reported being in 1 of 2 distinct homelessness categories on the VA’s HOMES assessment (unsheltered vs sheltered); as such, our findings may not be generalizable beyond these 2 groups. Second, we did not examine the duration of homelessness, and homeless status can fluctuate, as often veterans can return to unsheltered homelessness over time. Future studies should investigate whether these characteristics of unsheltered homelessness remain consistent over time. However, our study did provide a snapshot of the current state of unsheltered homelessness among veterans. Third, given that levels of health care use are typically low among the unsheltered homeless population, physical and mental health conditions may have been underdiagnosed, leading to underestimates. Lastly, because our focus was on VA service use, the rate at which homeless veterans use other services in the community is unknown.
Conclusion
Our study uncovered some new characteristics of unsheltered homelessness among veterans and underscored the need for innovative VA transitional housing programs that may be effective in engaging young veterans in VA programs and clinical services. These study findings are valuable for understanding the current demographic and clinical needs of unsheltered homeless veterans to help anticipate challenges and potential solutions. In an effort to address the unsheltered homelessness crisis, the recent federal strategic plan ALL INside underscores the need to reduce programmatic, regulatory, and other barriers that systematically delay access to housing. 26 Models such as the VA’s Low Demand 38 and Safe Haven 39 approaches need to be evaluated to determine their effectiveness in engaging unsheltered homeless veterans—specifically, the young, educated, Hispanic unsheltered homeless population with exposure to military sexual trauma or combat.
Footnotes
Disclaimer
The views expressed in this article are those of the authors and do not necessarily represent the views of the US Department of Veterans Affairs.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was completed with support from the VA National Center on Homelessness Among Veterans and Veterans Health Administration.