
Abstract
Objective:
To investigate the experience of people experiencing unsheltered homelessness (PEUH) in meeting their basic needs for food, drinking water, toilet, hygiene, and healthcare in Los Angeles County.
Methods:
Cross-sectional, in-person health assessment survey (modified HOUSED BEDS instrument) from 2022 to 2023 among PEUH age 18+ years and initiating care with street medicine (N = 665).
Results:
Few participants reported access to a toilet (23%), shower (44%), primary care (7%), and food (x̅ = 8.3 meals per week ±5.7). Geographical area was associated with statistically significant differences in participant demographic characteristics, access to, and source type of basic resources.
Conclusions:
Key gaps in access to basic resources for survival for PEUH continue to exist in an urban county where state and local government entities have prioritized addressing homelessness by heavily investing in housing solutions.
Policy Implications:
Pervasive unmet needs for basic resources among PEUH threatens wellbeing and holds important implications for public health, healthcare providers, and payers. Geographical differences in access to basic resources for PEUH suggests a need for heterogeneous services, resources, solutions, and policies to better support PEUH.
Introduction
Homelessness in the United States continues to grow, with the latest statistics showing that just over 770 000 people are experiencing homelessness across America. 1 California is home to 30% of the nation’s homeless population and approximately 42% of the state’s homeless population resides in Los Angeles County. 2 Previous research has made important distinctions between people experiencing sheltered and unsheltered homelessness. “Unsheltered” homelessness means “rough sleeping” outside in the elements or in places not intended for human habitation (ie, on sidewalks, bridges, underpasses, riverbeds, encampments, cars, etc.). 3 In Los Angeles County, 75% of the homeless population lives unsheltered2,4; the most out of any state and attributed to a dearth of emergency shelters, transitional, and supportive housing. 5
Unsheltered homelessness significantly impacts health and contributes to accelerated aging and premature death due to poor access to healthcare, poor nutrition, and exposure to the elements.6 -8 People experiencing unsheltered homelessness (PEUH) also have competing priorities 9 and different personal and environmental challenges in maintaining their health and accessing healthcare. 10 Barriers to accessing traditional (ie, brick-and-mortar) healthcare are well documented among PEUH and include lack of transportation, feeling unwelcome in these settings, distrust of clinicians, stigma, and past experiences of poor treatment or discrimination.11 -14 This contributes to higher rates of illness 15 and an all-cause mortality rate 10 times higher than housed individuals and nearly 3 times higher than sheltered homeless individuals. 16 A recent literature review also highlights high rates of trimorbidity (ie, co-occurring chronic illness, mental health condition(s), and substance use disorder) with lower healthcare utilization and lack of health insurance. 8 Another study that did not distinguish shelter status found that patients who were experiencing homelessness had a 6-times higher medical risk score and cost over 6 times more than the average Medicaid Managed Care patient. 17
A seminal concept in psychology, Maslow’s hierarchy of needs, explains that basic physiological needs (water, food, shelter, and bare necessities for human survival) comprise the foundation of the most essential needs for humans. It further describes that deprivation at this base level precludes meeting subsequent ranked needs higher up the hierarchy such as those around safety, social, esteem, and self-actualization. 18 Basic physiological needs are met by homeless shelters and temporary housing sites for the people who access them and existing research has focused on this service-accessing and sheltered population due to increased feasibility of data collection. Recently, a landmark study in California explored who is experiencing homelessness, how they became homeless, and what their experiences has been, 13 however, little is known about the needs for survival, outreach services, and healthcare among PEUH, specifically. Understanding the basic physiological needs of PEUH is important to inform health and social services, policy, and advocacy for this population. To this end, we engaged exclusively with PEUH and employed a clinical tool specifically designed for obtaining a history with this population. The purpose of this study was to explore the experience of adults experiencing unsheltered homelessness with meeting their basic needs for food, drinking water, toilet, hygiene, and healthcare in Los Angeles County. The study objectives were: To identify the overall primary sources of basic needs for PEUH at initiation of street medicine care, and; To identify any differences in primary sources of basic needs across 5 geographical areas of Los Angeles County for PEUH at initiation of street medicine care.
Methods
We conducted a cross-sectional health assessment survey over 2 years (January 1, 2022, to December 31, 2023) among PEUH at the time of care initiation with USC street medicine. Data were collected prospectively as part of usual care and were analyzed retrospectively for research. This study was reviewed and approved by the institutional review board (IRB) of the University of Southern California and determined to be exempt research; not requiring written consent declarations (approval number UP-22-00587). This determination was made due to the anonymous nature of the survey, the inability to retrace any data to a particular person, the non-sensitive survey topic, and retrospective analysis of the existing deidentified data. Participants did provide signed consent to engage in medical care with USC and have deidentified data (reported here) retrospectively analyzed for research and quality improvement, and publication. Patients were also given the option to consent to medical care but decline use of their data in research and quality improvement.
Procedures and Sample
Street medicine team members (physician, physician assistant, or community health worker) conducted census sampling (ie, complete enumeration) by verbally administering the survey to all patients as part of usual care at the initial visit/outset of establishing care with USC. Data were self-reported by patients and entered by the team member into Qualtrics (USC-HIPAA compliant subscription) without any personal identifiers. Eligible patients included those aged 18 years or older, self-identified as experiencing unsheltered homelessness at the time of contact, and agreeing to engage in care with USC street medicine (no exclusion criteria). Although patients were followed longitudinally for healthcare, survey data reported here are cross-sectional and were analyzed retrospectively. Subsequent follow-up assessments are conducted periodically as part of usual care when a patient’s condition and/or environment changed, but are not recorded in a dataset or available for analysis.
Study Site
Street medicine care was delivered to patients by 5 teams of providers across unique geographical coverage areas in Los Angeles County. Geographical areas were designated as: Eastside, Southside, Hollywood, and Council District-1 (CD-1) all within the City of Los Angeles, and the San Gabriel Valley (SGV). See Appendix A. Los Angeles County is 4753 mi2 of diverse topography comprised of 88 unique urban and suburban cities and home to approximately 9.6 million residents; the most populated county in the United States. Distinguishing geographical areas is important due to the vast differences in landscape, resources, and population density. During the study period, the street medicine program was growing and adding new clinical teams covering particular geographical areas. Geographical area sample sizes are indicative of the length of time that teams were established and operating in the field. For example, the Eastside team was the original team and represents the largest subsample of patient surveys. Council District-1 was the newest team, established in September 2023 and has the smallest sample size.
Measures
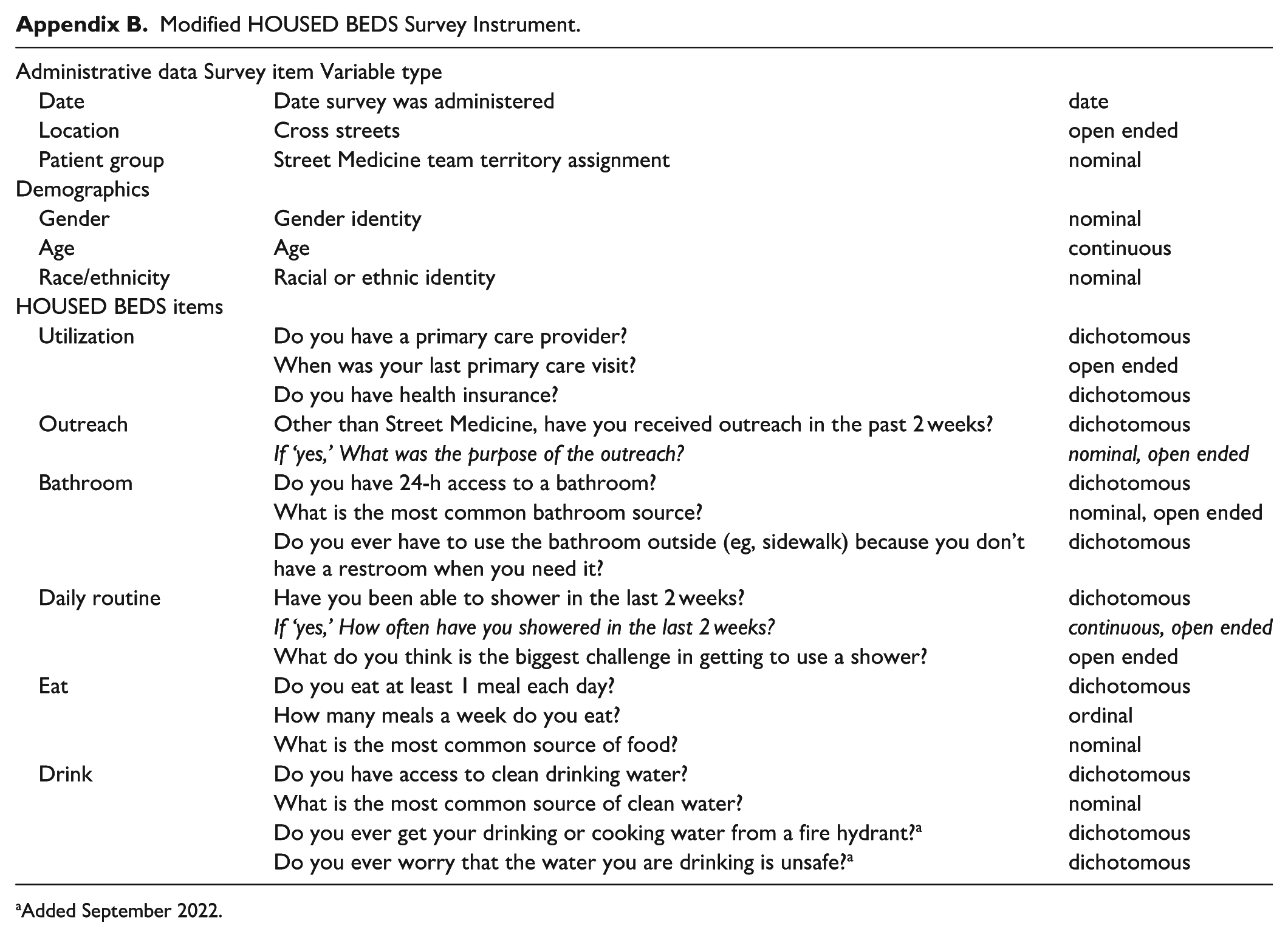
The in-person baseline health assessment was conducted with a modified version of the HOUSED BEDS 19 clinical tool, specifically designed for obtaining a history on a person experiencing unsheltered homelessness. The full HOUSED BEDS tool was modified by its creators and clinical members of the USC street medicine team before being pilot tested by 3 team members and among 54 patients between November and December 2021. Pretest revealed no further modifications to the survey assessment tool and data collection began January 2022 through the end of December 2023.
The full acronym stands for:
Analysis
Univariate statistics (frequency, percent, mean, and standard deviation) were used to describe all survey data points for the overall sample and for each of the 5 different street medicine team’s geographical coverage areas. Bivariate analyses (1-way ANOVA and chi-square tests) were conducted to test for differences between all continuous and categorical variables and the 5 different geographical areas. An additional chi-square test was conducted to detect any relationship between having health insurance and having a primary care provider. Analyses were conducted retrospectively by the study team’s lead researcher using SPSS statistical software version 29.
Results
Demographic Characteristics
Between January 1, 2022, and December 31, 2023, modified HOUSED BEDS surveys were conducted with 665 unique patients during their initial medical encounter to establish care with USC street medicine. The overall response rate was 100% (missingness per measure is discussed below). On average, patients were aged 45 years (SD = 13.3 years), however, a wide range of ages was observed (minimum = 18 years; maximum = 77 years). Patients commonly identified as male (63.9%), followed by female (35.0%) and transgender (1.1%). Patients’ self-reported racial/ethnic identity was commonly Hispanic/Latino (46.4%), white (26.6%), or Black (20.5%). See Table 1.
Sample Characteristics of Adult Patients in Street Medicine in LA County, by Geographical Area.

Chi-square and ANOVA analyses performed to detect differences by geographic area; Chi-square between health insurance and has PCP.
Other race/ethnicity = Native American, Middle Eastern, Moroccan, Multiple ethnicities.
% of overall sample.
Other = Circle team, COVID-related, Urban Alchemy, food/water, harm reduction.
P < .05.
Modified HOUSED BEDS: Outcomes
Utilization
Patients were asked if they currently had a primary care provider (PCP) at the time of the survey and initial street medicine engagement, and if they did, when was their last visit. The majority (74.5%) of respondents reported having health insurance, but 83% reported not having a PCP. Of those with a PCP, fewer than half (48.9%) reported seeing them within the last year. Thus, 7% of the overall sample had been seen by a PCP in the last year. While an established PCP was low for all patients surveyed, a significant association with having health insurance and having a PCP was identified (χ2 = 46.52, df = 4, P < .001). See Table 1.
Outreach
Patients were queried about being engaged by formal outreach organizations other than street medicine in the previous 2 weeks; an interval chosen due to the frequency of movement by PEUH and informed by the experience of street medicine clinicians who have found it to be the most reliable interval for successful engagement by clinical teams. Thirty-one percent had been engaged in outreach other than street medicine. Housing outreach was the most common type among those who were contacted, however, this equated to only 20.1% of the overall sample, followed by outreach for physical health (8.9%), and mental health (3.2%). See Table 1.
Bathroom
Patients were queried about their bathroom access, primary source, and having to resort to open defecation. Fewer than one-fourth (22.5%) of the overall sample reported having 24-h access to a bathroom. Patients’ most common bathroom source was: outside (36.8%), business (26.5%), “other” (13.5%), porta-potty (10.2%), and park (10.2%). Most patients reported having to resort to open defecation due to not having an available restroom when needed (81.9%). See Table 2.
Access to and Source of Toileting and Hygiene, among Adult Patients in Street Medicine in LA County, by Geographical Area.
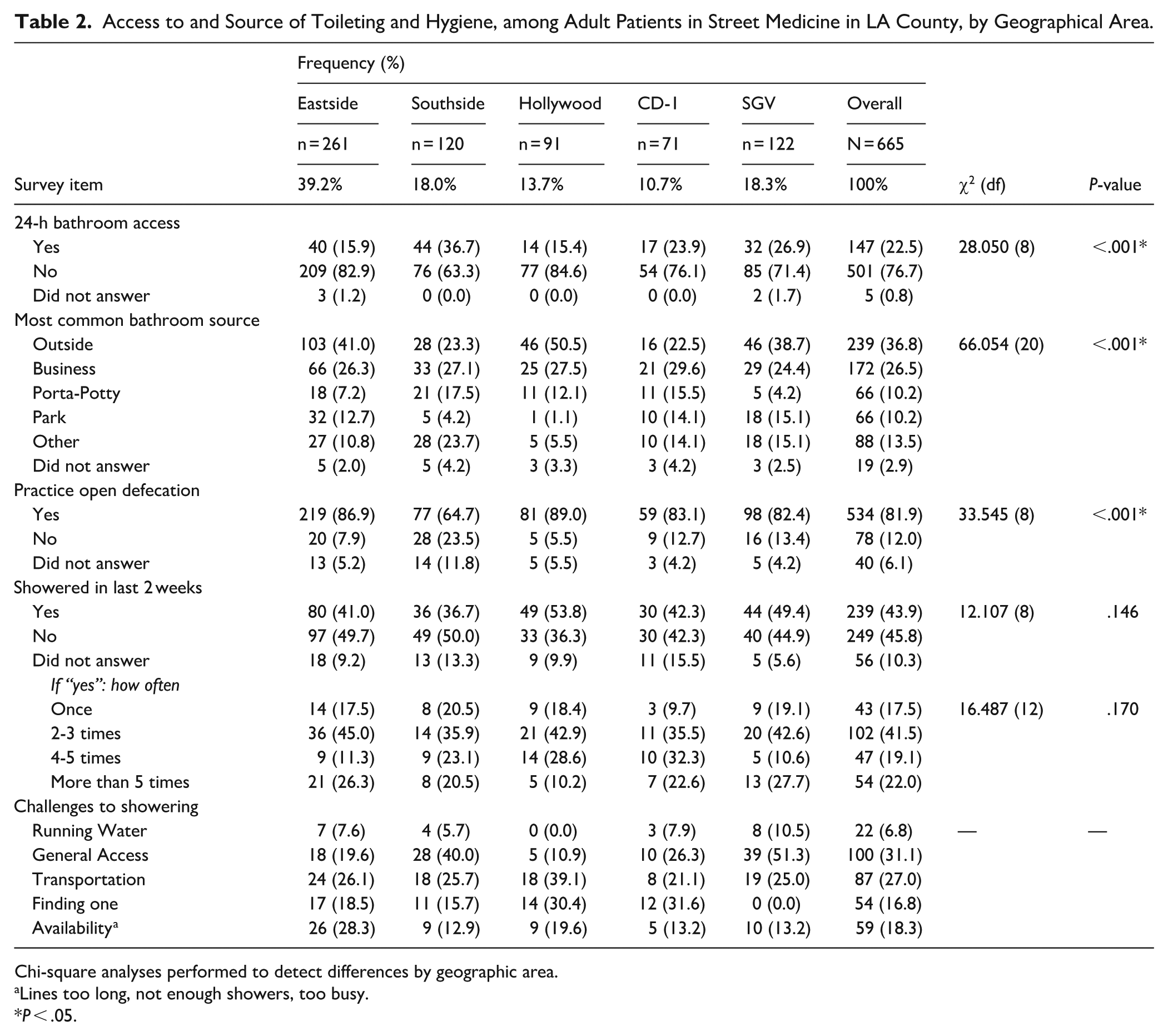
Chi-square analyses performed to detect differences by geographic area.
Lines too long, not enough showers, too busy.
P < .05.
Shower Access
Patients were asked about their shower access, frequency, and barriers to showering. Overall, fewer than half of patients in the sample reported showering at least once in the past 2 weeks (43.9%). Among patients who had been able to shower in the last 2 weeks, 78.1% did so 5 times or less. Numerous barriers to accessing showers were identified by patients. Barriers were most commonly: general access issues (31.1%; ie, location, environment, leaving possessions behind, wheelchair accessibility, etc.), transportation/getting there (27.0%), availability (18.3%; ie, limited number, busy, wait times, etc.), finding one or knowing where a shower is (16.8%), and access to running water/water hookup for recreational vehicle (6.8%). See Table 2.
Eat
Patients were asked about their number of weekly meals, consumption of a daily meal, and most common source of food. Overall, patients reported eating an average of 8.25 (SD = 5.7) meals per week. Approximately one-third reported eating less than 1 meal per day (32.7%), with 22% eating between 1 and 4 meals per week, and 4.8% not eating any meals. Overall, purchased food was the primary source for patients (49.2%). See Table 3.
Access to and Primary Source of Food and Drink among Adult Patients in Street Medicine in LA County, by Geographical Area.

Chi-square and ANOVA analyses performed to detect differences by geographic area.
“Other” common food source: Miscellaneous = panhandling, stealing, etc.
P < .05.
Drink
Patients were asked about their access to drinking water, primary source of drinking water, use of fire hydrants for drinking water, and concern over water safety. Overall, most patients reported having access to clean drinking water (72.4%). Patients’ most common source for clean drinking water was purchased bottled water (36.9%). Just over one-third (35.4%) of the sample reported concern for unsafe drinking water, and 28% used water from a fire hydrant. See Table 3.
Geographic Differences
Bivariate analyses were conducted to reveal differences in how patients meet their basic needs for survival across the 5 geographic service areas. Notably, significant differences were detected for: respondents’ demographic characteristics (all characteristics, P < .001), having health insurance (P < .001), having a PCP (P < .001), receiving outreach (P < .001), having 24-h access to a bathroom (P < .001), primary bathroom source (P < .001), having to practice open defecation (P < .001), consumption of a daily meal (P < .001), primary food source (P < .001), access to drinking water (P < .001), primary source of drinking water (P = .003), using water from a fire hydrant (P < .001, and concern over unsafe drinking water (P < .001). Differences in the average number of meals per week, showering practices in the past 2 weeks, and frequency of showering did not reach statistical significance across the 5 geographical areas.
Discussion
Eliciting the perspective of people experiencing unsheltered homelessness is critical to identifying unmet needs and priorities for survival for this population. This study aimed to investigate how adults experiencing unsheltered homelessness meet their basic needs for food, drinking water, sanitation, and healthcare in Los Angeles County. Results of this study show a temporal mismatch between insufficiently met immediate, daily, basic needs of PEUH and heavy financial investment in housing solutions by state and local government entities that require a lot of time to build and establish. 20 For example, Los Angeles’ Measure H and complementing Proposition HHH which created a sales tax to fund building housing for people experiencing chronic homelessness (Prop. HHH), and short-term housing and homeless services (Measure H). This prioritization of preventing and addressing homelessness 20 is laudatory but raises concerns that if PEUH do not have their basic needs met, they will be less likely to be able to complete the necessary tasks (ie, obtain government-issued identification, meet with case management, etc.) in preparation for accessing housing solutions when they become available due to poor health and competing priorities for survival. Additionally, results suggest geographical variation in access to- and primary source of basic survival resources. These findings extend beyond previous research by focusing exclusively on PEUH under care by street medicine teams; allowing new insights into the deprivation of basic human needs among this population.
The condition of unsheltered homelessness and living a life of scarcity and social deprivation correspond to significant deficits from the bottom to the top of Maslow’s hierarchy, holding significant implications for healthcare engagement and health outcomes. Without access to basic resources for survival, it is unrealistic to expect PEUH to have the capacity to seek out and navigate a complex healthcare system. Furthermore, PEUH are unlikely to shower and eat regularly, which means that they are also unlikely to enter, wait, and engage with traditional office-based medical settings, or feel comfortable doing so. Combined with an excess burden of chronic medical and mental health conditions, this may begin to explain the disproportionate burden of excess morbidity and mortality in this population.
Food and water security are critical to the prevention, management, and recovery from acute and chronic health conditions. This study found that PEUH were primarily purchasing food and drinking water, and rates differed within the County. Another recent study that focused on the unhoused in the Skid Row area of Los Angeles (known for a high concentration of unhoused individuals and outreach services, and not included in our study) also found a prevalence of purchased water. 21 Reliance on buying food and water is costly and consumes scant financial resources. Additionally, food and hydration are fundamental needs that dictate PEUH priorities before paying for things such as healthcare or transportation. In 2023, California’s supplemental nutrition assistance program (CalFresh) offered maximum monthly benefits of $291 for low-income individuals who qualify, successfully navigate the system, and maintain their application. 22 To make dollars stretch, less expensive, calorie dense foods are often purchased; foods known to contribute to preventable diseases among all populations, such as heart disease and cancer, 23 and disproportionately observed among people experiencing homelessness.24,25 Researchers have identified “food deserts” (ie, areas of poor and disparate access to healthy food), several of which are in Los Angeles County and included in the geographical areas of our study, as additional contributors to risk for cardiovascular 26 and chronic kidney disease. 27 In line with our results, Smith and colleagues investigated the impact of a food desert on people experiencing homelessness in Minnesota and found high rates of obesity (80%), reliance on purchased food, reliance on food assistance programs that did not adequately cover food costs, and high food prices dictating food choices. 28 A resource map for Los Angeles County developed by USC street medicine shows charitable food donation services with limited days and hours of operation, in addition to other known access barriers for people experiencing homelessness including requirements to show government-issued identification. Furthermore, soup kitchens and other resources targeted toward PEUH are concentrated within Skid Row. Lack of free food options results in many PEUH outside of Skid Row, such as those participating in this study, being reliant upon purchasing foods with funds from government benefits or other means. Results from the present study and others suggest deleterious health effects for PEUH relying on purchased food and living within food deserts. Benefits designed for PEUH should prioritize food as medicine. Further in-depth investigation is needed to fully understand the challenges that PEUH face with obtaining food from other sources and to develop actionable strategies, benefits, and fair reimbursement models to address this fundamental issue.
The human right to sanitation is commonly violated for PEUH and presents public health concerns for infectious disease transmission.29,30 Our study found high rates of open defecation practices, pervasive lack of 24-h toilet access, and variable shower access. Other studies among people experiencing homelessness in the U.S. corroborate these findings of sanitation and hygiene insecurity.21,29,30 A lack of bathroom access is a dehumanizing experience, can be criminalized, leads to distain and blame from the public, and could contribute to public health concerns (eg, hepatitis A outbreaks).21,29,30 Previous research suggests the effectiveness of public restroom interventions at reducing reports of exposed feces, including installation of new bathrooms, strategically placed porta potties, and employing restroom attendants. 30 However, other studies highlight important considerations for restroom and hygiene interventions such as: geographic location, overnight or 24-h access, showers that are compliant with disability laws, and prevalence of sanitation resources.21,29 Reliance by PEUH on businesses to access bathrooms is limited to operating hours, customer and employee resistance, cost for access, and is overall unreliable and problematic. Coordinated efforts to improve access to sanitation by PEUH should focus on public options that take the unique needs of this population into account.
Limitations
Study findings may be limited by several factors including potential sampling, response, and interviewer biases. First, this study was limited to quantitative data from patients initiating care with teams within 1 street medicine organization covering a particular geographic service area in Los Angeles County; potentially limiting generalizability of findings. This study was observational; therefore, a sample size power calculation was not performed. Results may not be representative of the larger unsheltered homeless population in Los Angeles, or generalizable to other areas. Responses may be limited by health literacy and understanding by each participant, in addition to selection bias where those who agreed to engage in healthcare with street medicine may have had higher burden of illness. However, we found similar demographic characteristics among our participants compared to those assessed in the latest (2023) annual Point-in-Time Count (PIT Count). 2 This study relied on self-reported data which may be unreliable and introduce bias, although among PEUH, self-reported data may be most reliable because it captures the person’s perception. For the survey question about having a PCP, the care location of the PCP was not distinguished between clinic/office (ie, brick-and-mortar) or street medicine setting. Data were cross-sectional and lack of longitudinal follow-up preclude our ability to explore individual and cohort changes over time.
Implications for Primary Care and Community Health
Pervasive unmet needs for basic resources and access to primary care among PEUH, even in an urban county, highlights threats to patient wellbeing and holds important implications for public health, healthcare providers, and payers. “Food is medicine” (defined as food-based nutritional interventions integrated within health systems to treat or prevent disease and advance health equity31 -33), just as housing is healthcare. In addition to existing funding allocations and programs for housing solutions, programs and delivery models for basic survival needs for PEUH should also be prioritized and tailored to reflect the needs and characteristics of their communities.
Footnotes
Appendix
Modified HOUSED BEDS Survey Instrument.
| Administrative data Survey item Variable type | ||
| Date | Date survey was administered | date |
| Location | Cross streets | open ended |
| Patient group | Street Medicine team territory assignment | nominal |
| Demographics | ||
| Gender | Gender identity | nominal |
| Age | Age | continuous |
| Race/ethnicity | Racial or ethnic identity | nominal |
| HOUSED BEDS items | ||
| Utilization | Do you have a primary care provider? | dichotomous |
| When was your last primary care visit? | open ended | |
| Do you have health insurance? | dichotomous | |
| Outreach | Other than Street Medicine, have you received outreach in the past 2 weeks? | dichotomous |
| If ‘yes,’ What was the purpose of the outreach? | nominal, open ended | |
| Bathroom | Do you have 24-h access to a bathroom? | dichotomous |
| What is the most common bathroom source? | nominal, open ended | |
| Do you ever have to use the bathroom outside (eg, sidewalk) because you don’t have a restroom when you need it? | dichotomous | |
| Daily routine | Have you been able to shower in the last 2 weeks? | dichotomous |
| If ‘yes,’ How often have you showered in the last 2 weeks? | continuous, open ended | |
| What do you think is the biggest challenge in getting to use a shower? | open ended | |
| Eat | Do you eat at least 1 meal each day? | dichotomous |
| How many meals a week do you eat? | ordinal | |
| What is the most common source of food? | nominal | |
| Drink | Do you have access to clean drinking water? | dichotomous |
| What is the most common source of clean water? | nominal | |
| Do you ever get your drinking or cooking water from a fire hydrant? a | dichotomous | |
| Do you ever worry that the water you are drinking is unsafe? a | dichotomous | |
Added September 2022.
Acknowledgements
The authors would like to thank each patient who participated in a survey for this study and for allowing the team to care for them. We would also like to thank the USC street medicine team for all that they do. This report would not be possible without their hard work and commitment to their patients and delivering high quality care on the street. Special thanks to Dr. Lillian Gelberg for her review and input into the development of this manuscript.
Ethical Considerations
This study was reviewed and approved by the institutional review board (IRB) of the University of Southern California as exempt research (UP-22-00587).
Consent to Participate
Participants provided signed consent to engage in medical care with USC Street Medicine (an entity of Keck Medicine of USC) and have deidentified data (reported here) analyzed for research and quality improvement, and published.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.