
Abstract
The World Trade Center (WTC) Health Program, a limited federal health care program for eligible people exposed to the terrorist attacks on September 11, 2001, expanded telemedicine services during the COVID-19 pandemic (2020-2021). We analyzed service use trends from January 2020 through December 2021 to describe how the program implemented telemedicine services. About three-quarters (75%) of telemedicine visits were for mental health–related services. In the second quarter of 2020 (April–June), the number of telemedicine visits per 1000 members (n = 367) increased, exceeding in-person visits (n = 152) by 1.4-fold. The number of telemedicine visits per 1000 members decreased gradually during the rest of the study period but still represented 38% of total visits by the end of 2021. Changes in telemedicine visits were offset by comparable changes for in-person visits, such that the rate of total visits was essentially constant during the study period. Multivariate logistic regression models showed differences in telemedicine visit rates by member type and by demographic characteristics. Survivor members (vs responder members), those self-identified as non-Hispanic Other races (vs non-Hispanic White), those with preferred language not English (vs preferred language English), and those not living in the New York metropolitan area (vs living in the New York metropolitan area) were less likely to use telemedicine. Implementing telemedicine services in the WTC Health Program during the COVID-19 pandemic underscored the importance of extensive collaboration among partners, the capacity to rapidly develop necessary technical guidance, and the flexibility to address frequent regulatory guidance updates in a timely fashion. These lessons learned may guide similar health care providers posed with time-sensitive disruptions of in-person services.
The World Trade Center (WTC) Health Program (hereinafter, the Program) is a limited federal health care entitlement program administered by the National Institute for Occupational Safety and Health within the Centers for Disease Control and Prevention (CDC) that provides no-cost medical monitoring and treatment for certified WTC-related health conditions to eligible people directly affected by the 9/11 terrorist attacks in New York City, the Pentagon, and in Shanksville, Pennsylvania.1,2 A comprehensive list of allowable WTC-related health conditions is available elsewhere.2,3 The eligible population comprises WTC responders who were involved in rescue, response, recovery, cleanup, and related support activities and WTC survivors who were present in the dust or dust cloud on 9/11 or who worked, lived, or attended a school, childcare center, or adult day care center in the New York City disaster area and have symptoms of a WTC-related health condition. 4 An estimated 400 000 people were exposed to the 9/11 attacks.5,6 To be eligible for the Program, individuals must meet specified criteria related to exposure (ie, activity, location, time, and hours of exposure).1,2 Program members receive their medical services at 1 of 8 designated Clinical Centers of Excellence (CCEs) in New York City or New Jersey or with health care providers across the country through a contracted vendor, the Nationwide Provider Network (NPN). As of December 31, 2019, a total of 102 049 members were enrolled in the Program. 7
In 2020, during the community transmission of SARS-CoV-2, the virus that causes COVID-19, in-person medical care in the United States was disrupted by public health measures (ie, social distancing and stay-at-home orders) or concerns about contracting COVID-19.8,9 New York City and New Jersey were substantially affected by the COVID-19 pandemic early on.10 -12 To mitigate medical care disruptions, US health care providers shifted from in-person services to telemedicine.13,14 Telemedicine is defined as a real-time exchange of medical information between the patient and provider through electronic communication (eg, audio [telephone] or visual [videoconferencing]). 15 Before 2020, the Program covered only telemedicine services for certified mental health conditions through a limited pilot program in 1 CCE.
In March 2020, regulatory changes by the Centers for Medicare & Medicaid Services expanded access to telemedicine. 16 The US Department of Health and Human Services also declared a public health emergency that enabled state governors to waive geographic restrictions pertaining to in-state licensure requirements for some health care professionals. 16 National data showed a substantial increase in the number of Medicare beneficiaries receiving telemedicine services before (n = 13 000) and after (n = 1.7 million) the declaration of this public health emergency. 16
After such federal regulatory changes, 16 the Program administrator promptly approved expanded use of telemedicine services to facilitate continuity of care through well-established staff-level partnerships with their CCEs, NPN, and business support vendors. Long-standing communication forums facilitated the formal change process for the CCEs/NPN, including weekly medical, mental health, pharmacy, and case management meetings and monthly formal Program partner meetings. Telemedicine services allowed members to virtually access their attending physicians and other health care professionals (who managed WTC-related conditions), obtain their prescription medication (including 90-day refills at local pharmacies and home deliveries), and receive case management support. The Program also began reimbursing health monitoring services rendered via telephone, allowing physicians to optimize complex care needs for members who contracted COVID-19 and had WTC-related comorbidities that raised their risk for severe COVID-19 illness and mortality.17,18 These added telemedicine services allowed medically complex Program members to minimize health-related needs to travel outside the home. Telemedicine services enabled the Program’s CCEs/NPN to achieve continuity of care during the COVID-19 pandemic. A description of advantages of and barriers to telemedicine implementation in the United States can be found elsewhere.19,20
Purpose
This case study analyzed service use trends among Program members from January 2020 through December 2021, when in-person medical care in the United States was disrupted during the COVID-19 pandemic. During the COVID-19 public health emergency, the Program stayed abreast of relevant federal health care policy changes and developed technical guidance to promptly enable telemedicine services. We discuss lessons learned during this rapid programmatic transition that may guide similar health care providers in responding to public health emergencies.
Methods
The Program uses a multilayer administrative claims system to process authorized health benefits and collect claims data. 2 Medical claims are reviewed and approved by various entities before being paid by the federal administrative and payer system. Data used for this study are protected under the Health Insurance Portability and Accountability Act of 1996 (HIPAA). The Program is authorized to collect, analyze, and report administrative claims data per Section 3304 of the Zadroga Act, the law that created the Program. 2 Program administrative claims data are not available to the public.
Institutional review board approval was not needed for this analysis because this work was determined to meet the requirements of public health surveillance as defined in 45 CFR 46.102(l)(2) 21 ; therefore, informed consent was not required for this surveillance activity. This work used existing information from enrollment and claims collected by the Program. No individual members were contacted, and no identifiable personal information was included for the analysis. This work was reviewed by CDC and was conducted consistent with all applicable federal law, regulations, and CDC policy.
We used administrative and claims data that have been routinely collected by the Program since July 1, 2011, when the Program began. For this analysis, administrative data included members’ enrollment information, such as member type (responder or survivor), sex (male, female), date of birth, race and ethnicity (Hispanic, non-Hispanic White, non-Hispanic Black, non-Hispanic Other [Asian, American Indian or Alaska Native, Native Hawaiian/Other Pacific Islander, >1 race], unknown), preferred language (English, other [Spanish, Polish, Chinese], unknown), and most recent residence (coded to indicate whether or not living in the New York Metropolitan Area [NYMA]). Members’ residential address data were collected at their most recent physical examination by the end of calendar year 2021. Medical claims data included claims that were billed to the Program for monitoring and treatment of WTC-related conditions. The Program requires that medical claims be submitted for payment within 18 months from the date of service. To describe service use among Program members from January 2020 through December 2021, we included living members. A living member is defined as a member who was alive and enrolled in the WTC Health Program for at least 1 day during 2020-2021. We used the most recently available claims data, processed by April 30, 2023, to identify medical services that were telemedicine-eligible or performed via telemedicine during 2020-2021.
Medical services that can be provided by telemedicine (ie, telemedicine-eligible) were identified using any of the following 4 criteria: (1) Medicare’s list of Current Procedural Terminology (CPT) codes eligible for telemedicine, 15 (2) any telemedicine CPT codes 98966-98968 (5- to 30-minute telephone consultation [assessment and management] by a qualified, nonphysician, health professional) or 99441-99443 (5- to 30-minute telephone call by a physician to report test results, receive care updates, adjust therapy, clarify instructions, or perform another task related to coordinating care), (3) place of service code 02 (telehealth provided other than patient’s home) or 10 (telehealth provided in patient’s home), 22 or (4) with modifier codes GT (via interactive audio and video telecommunication systems), GQ (via asynchronous telecommunications system), G0 (telehealth services for diagnosis, evaluation, or treatment of symptoms of an acute stroke), or 95 (synchronous telemedicine service rendered via a real-time interactive audio and video telecommunications system). All telemedicine-eligible visits that met criteria 2 through 4 were defined as telemedicine visits (medical services that were actually provided via telemedicine); otherwise, they were deemed as in-person visits. The types of telemedicine services were determined by examining CPT codes, diagnostic codes, and provider specialty listed on medical claims. Consultation, evaluation, and preventive care visits for other health conditions were based on procedure codes. Telephone evaluation and management services were based on CPT codes 99441-99443.
We described the characteristics of Program members included in this study, including member type, sex, age, race and ethnicity, preferred language, and residence in the NYMA. NYMA was identified by 3-digit zip codes: 068-079, 085-089, 100-119, and 189. We also estimated use rates of telemedicine-eligible services and telemedicine services by all included Program members and by subgroups of members defined by member type (responder or survivor) and selected characteristics for the study period 2020-2021. In addition, we used a multivariate logistic regression model to examine the associations (odds ratios [ORs] and 95% CIs) between member characteristics and telemedicine use rates. We also described the use trends of total telemedicine-eligible visits, telemedicine visits, and in-person visits, respectively, by quarter. We calculated quarterly use rates per 1000 living members by using the following equation: (total number of specified type of visits in the quarter)/(total number of living members enrolled for at least 1 day in the quarter) × 1000. We performed all analyses using SAS version 9.4 (SAS Institute, Inc) and Microsoft Excel (Microsoft Corp).
Outcomes
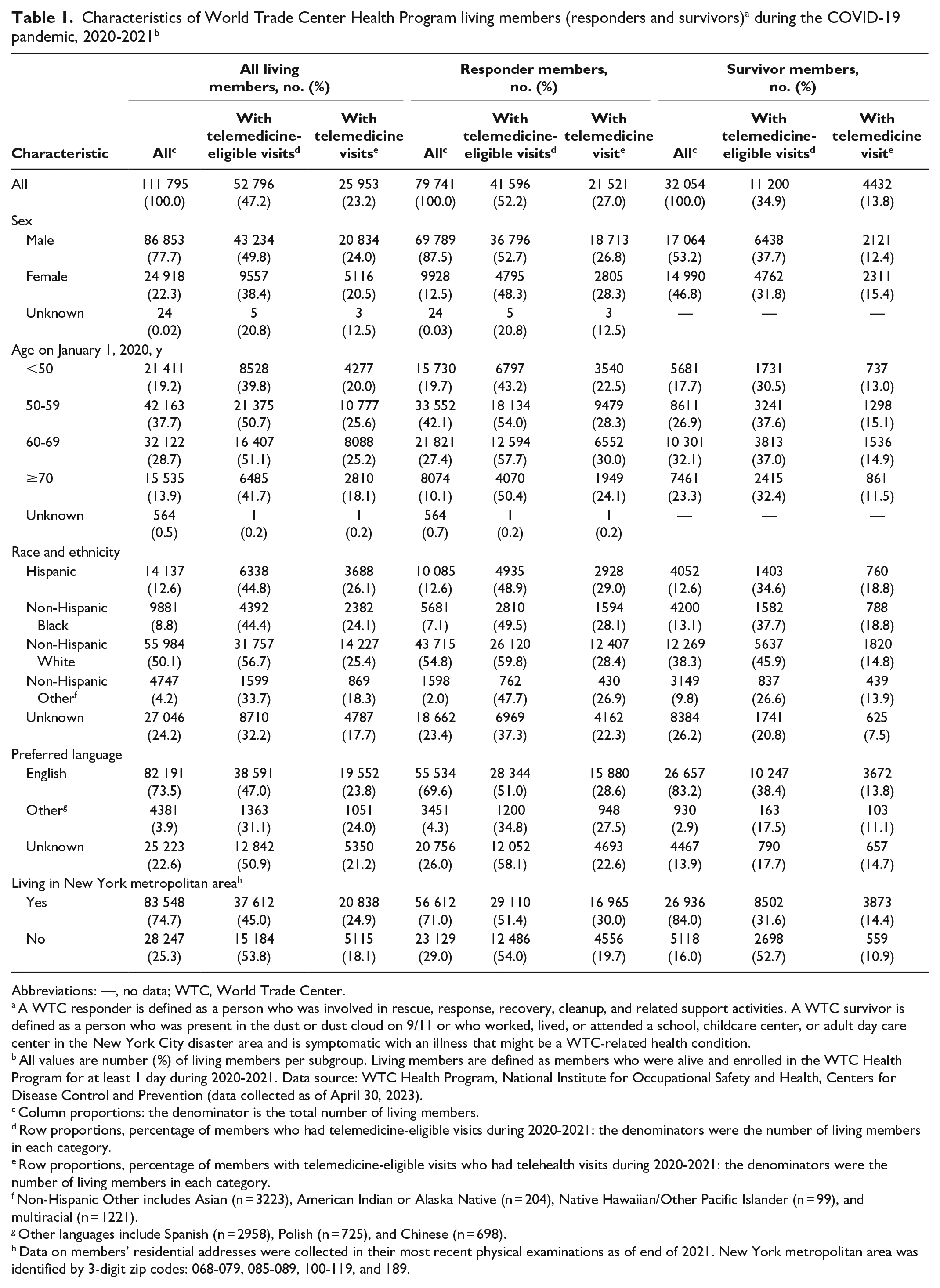
During 2020-2021, 111 795 living members were enrolled in the Program (Table 1). Among these members, 71.3% (n = 79 741) were responders, 77.7% (n = 86 853) identified as male, 66.4% (n = 74 285) were aged 50-69 years on January 1, 2020, 50.1% (n = 55 984) identified as non-Hispanic White, 73.5% (n = 82 191) self-reported English as their preferred language, and 74.7% (n = 83 548) self-reported residing in the NYMA. Among these members, 52 796 (47.2%) had at least 1 telemedicine-eligible visit, and 25 953 (23.2%) had at least 1 telemedicine visit.
Abbreviations: —, no data; WTC, World Trade Center.
A WTC responder is defined as a person who was involved in rescue, response, recovery, cleanup, and related support activities. A WTC survivor is defined as a person who was present in the dust or dust cloud on 9/11 or who worked, lived, or attended a school, childcare center, or adult day care center in the New York City disaster area and is symptomatic with an illness that might be a WTC-related health condition.
All values are number (%) of living members per subgroup. Living members are defined as members who were alive and enrolled in the WTC Health Program for at least 1 day during 2020-2021. Data source: WTC Health Program, National Institute for Occupational Safety and Health, Centers for Disease Control and Prevention (data collected as of April 30, 2023).
Column proportions: the denominator is the total number of living members.
Row proportions, percentage of members who had telemedicine-eligible visits during 2020-2021: the denominators were the number of living members in each category.
Row proportions, percentage of members with telemedicine-eligible visits who had telehealth visits during 2020-2021: the denominators were the number of living members in each category.
Non-Hispanic Other includes Asian (n = 3223), American Indian or Alaska Native (n = 204), Native Hawaiian/Other Pacific Islander (n = 99), and multiracial (n = 1221).
Other languages include Spanish (n = 2958), Polish (n = 725), and Chinese (n = 698).
Data on members’ residential addresses were collected in their most recent physical examinations as of end of 2021. New York metropolitan area was identified by 3-digit zip codes: 068-079, 085-089, 100-119, and 189.
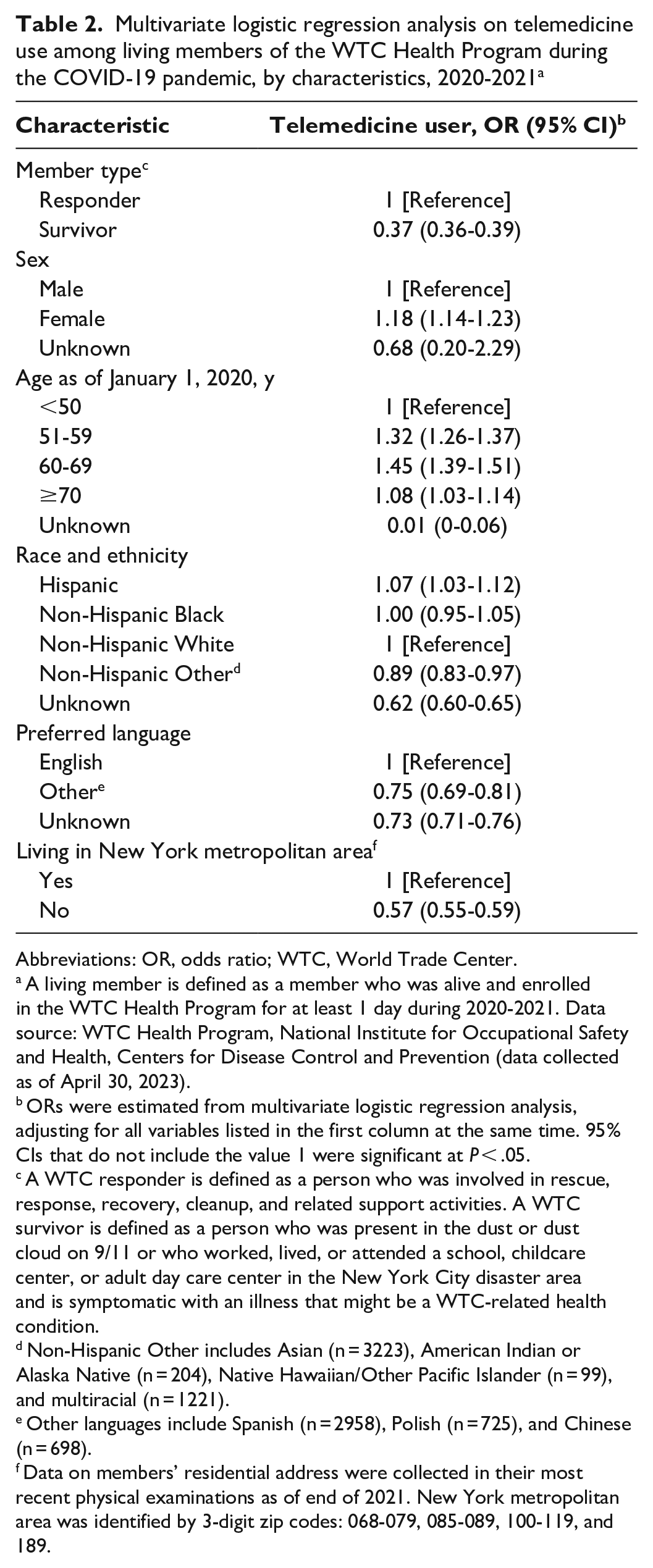
In the multivariate logistic regression analysis, telemedicine use rates were significantly lower among survivors than among responders (OR = 0.37; 95% CI, 0.36-0.39), among members of non-Hispanic Other races than among non-Hispanic White members (OR = 0.89; 95% CI, 0.83-0.97), among members who preferred other languages than among members who preferred English (OR = 0.75; 95% CI, 0.69-0.81), and among those who lived outside the NYMA than among those in the NYMA (OR = 0.57; 95% CI, 0.55-0.59) during the study period (Table 2).
Multivariate logistic regression analysis on telemedicine use among living members of the WTC Health Program during the COVID-19 pandemic, by characteristics, 2020-2021 a
Abbreviations: OR, odds ratio; WTC, World Trade Center.
A living member is defined as a member who was alive and enrolled in the WTC Health Program for at least 1 day during 2020-2021. Data source: WTC Health Program, National Institute for Occupational Safety and Health, Centers for Disease Control and Prevention (data collected as of April 30, 2023).
ORs were estimated from multivariate logistic regression analysis, adjusting for all variables listed in the first column at the same time. 95% CIs that do not include the value 1 were significant at P < .05.
A WTC responder is defined as a person who was involved in rescue, response, recovery, cleanup, and related support activities. A WTC survivor is defined as a person who was present in the dust or dust cloud on 9/11 or who worked, lived, or attended a school, childcare center, or adult day care center in the New York City disaster area and is symptomatic with an illness that might be a WTC-related health condition.
Non-Hispanic Other includes Asian (n = 3223), American Indian or Alaska Native (n = 204), Native Hawaiian/Other Pacific Islander (n = 99), and multiracial (n = 1221).
Other languages include Spanish (n = 2958), Polish (n = 725), and Chinese (n = 698).
Data on members’ residential address were collected in their most recent physical examinations as of end of 2021. New York metropolitan area was identified by 3-digit zip codes: 068-079, 085-089, 100-119, and 189.
A total of 177 508 telemedicine visits were conducted during the study period. The top 3 telemedicine services provided during the study period were mental health–related services (n = 133 507; 75.2% of visits); consultation, evaluation, and preventive care visits for other health conditions (n = 27 502; 15.5% of visits); and telephone evaluation and management services (n = 13 579; 7.6% of visits).
Telemedicine visit rates per 1000 person-quarters increased during the study period by 363% (from 41 in quarter 1 of 2020 [January–March] to 190 in quarter 8 of 2021 [October–December]), peaking and surpassing the rate of in-person services in quarter 2 of 2020 (April–June), and then stabilizing in subsequent quarters (Figure). The rate of in-person visits per 1000 person-quarters decreased during the study period by 33% (from 463 in quarter 1 of 2020 to 312 in quarter 8 of 2021), with a sharp decrease to the lowest rate in quarter 2 of 2020, and then increased and stabilized in subsequent quarters.
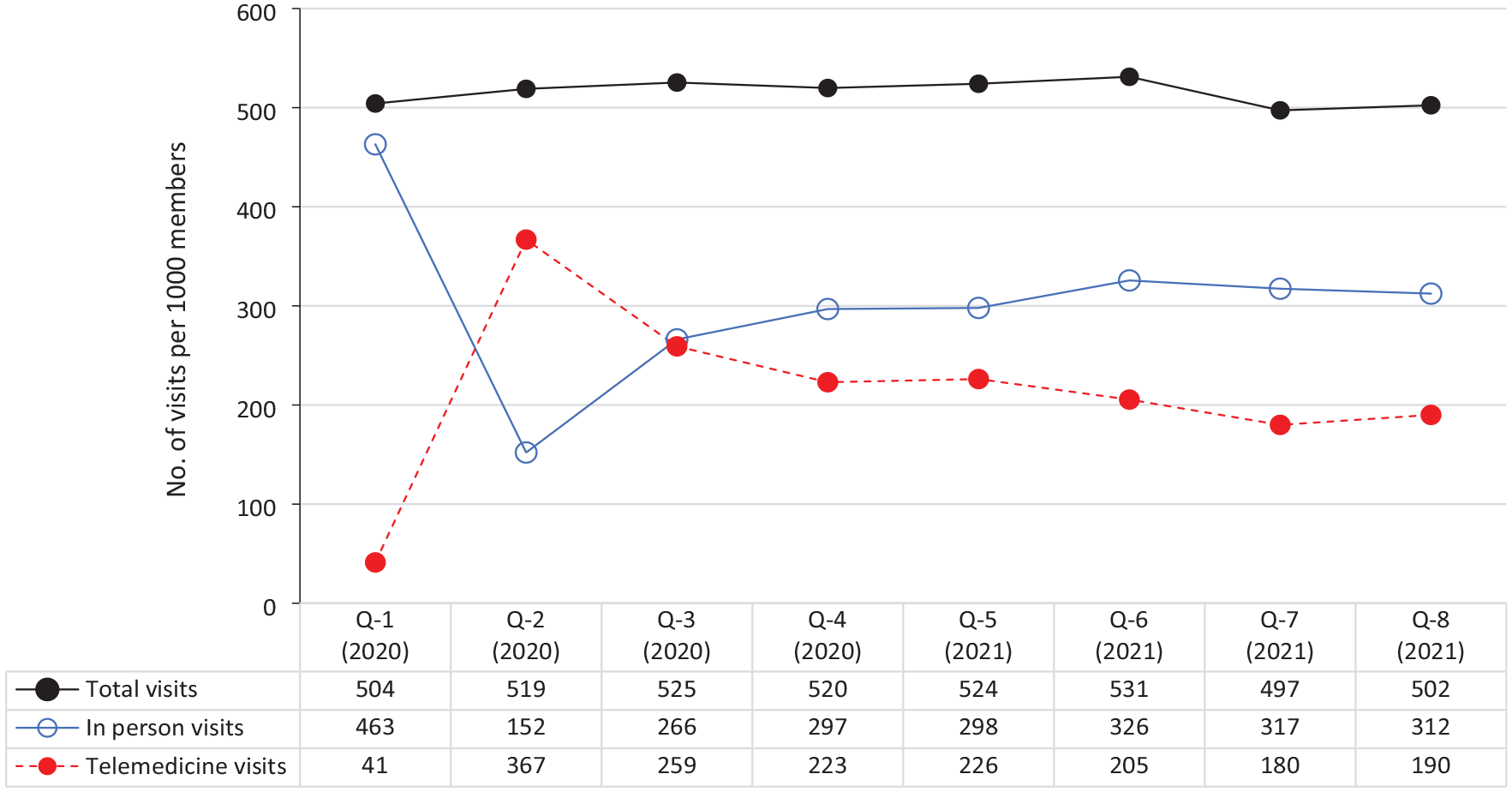
Trends in total visits, in-person visits, and telemedicine visits per quarter (Q) during the COVID-19 pandemic, January 2020–December 2021. Q1 is January–March 2020; Q2 is April–June 2020; Q3 is July–September 2020; Q4 is October–December 2020; Q5 is January–March 2021; Q6 is April–June 2021; Q7 is July–September 2021; and Q8 is October–December 2021.
Lessons Learned
Our study found that survivor members (vs responders) and those living outside the NYMA (vs in the NYMA) were less likely to use telemedicine services during the study period. Differences in telemedicine use rates by survivor members can be attributed to the Program’s statutory and regulatory requirements that the primary insurer for survivors be billed before the Program.2,3 Therefore, not all data on service use were captured using programmatic claims data. National studies have shown that individuals living in nonmetropolitan areas are less likely to use telemedicine than those living in metropolitan areas.23,24 Differences in telemedicine use rates by geography need further investigation, as disparities in access to telemedicine in the Program may be multifactorial (eg, differences in resource availability/accessibility, urban and rural connectivity, technological literacy). Our model also indicated disparities in telemedicine use rates among racial and ethnic minority groups (vs non-Hispanic White people) and those who prefer languages other than English (vs those who prefer English). Previous studies demonstrated that racial and ethnic minority groups (ie, Asian, American Indian or Alaska Native, Native Hawaiian/Other Pacific Islander) and those with limited English proficiency have lower odds of telemedicine use than non-Hispanic White people and those who are proficient in English, respectively.23,24 Our results identify a possible language barrier to telemedicine use in the Program, although this outcome deserves further investigation.
Our data show that 75.2% of telemedicine visits during the study period were for mental health related–services. National data during the initial phase of the COVID-19 pandemic revealed an increase in mental health conditions (anxiety, depression, substance misuse, and suicidal ideation).25,26 A perspective article described how Program health care providers responded to traumatic stressors during the pandemic. 27 Further research is warranted to understand these phenomena in the Program.
During the COVID-19 pandemic, the Program promptly expanded telemedicine services. While rates of in-person service delivery declined, particularly during the second quarter of 2020, rates of telemedicine use increased substantially as a result of timely administrative actions taken by the Program and its contractors (CCEs, NPN, and business support vendors). Thus, the pattern of total telemedicine-eligible visits from quarter 1 to quarter 8 indicated no significant fluctuations. These results are comparable with those of other national studies.13,14,16 The rapid shift from in-person services to telemedicine services, as well as increases in the supply of retail medications and use of the Program’s mail-order pharmacy, provided continuity of medically necessary care during the pandemic. 28
The experiences encountered during the study period resulted in 3 lessons learned. First, the transition to telemedicine required extensive collaboration between Program administration and partnering clinical health care providers (CCEs, NPN). During the initial phase of the pandemic, Program leadership and health care providers shared 5 goals: (1) providing continuity of essential health services, (2) addressing the psychosocial support needs of members, (3) ensuring the health and safety of members, (4) supporting the health, well-being, and stability of CCE/NPN staff, and (5) ensuring the financial stability of CCEs/NPN. These goals share common elements described in a Program perspective publication related to mental health during the COVID-19 pandemic. 27 The long-standing partnership between Program administrators and contracted provider entities (CCEs/NPN) was instrumental in meeting these goals. For example, Program administrators and clinicians participated in weekly meetings to address ongoing challenges to telemedicine services brought on by the public health emergency.
A second lesson was to ensure sufficient Program capacity to rapidly develop necessary guidance. The sudden shift from in-person to telemedicine services came with new requirements for technical guidance that delineated allowable telemedicine reimbursement/plan coverage (between payor and health care provider), especially with respect to changes in allowable coding and billing practices. Given the various billing systems among the health care provider entities, the appropriate technical guidance improved the efficiency of telemedicine service delivery to meet the emerging needs of Program members and reduced the administrative burden among health care providers by proactively addressing the issues that would have prompted numerous calls to the Program for coverage clarification.
Third, the Program required sufficient flexibility to address frequent updates about telemedicine service requirements from federal regulatory agencies. This flexibility supported timely updates to medical/billing codes and procedures that met the demands imposed by the COVID-19 pandemic.
Despite maintaining health service continuity during the early stages of the COVID-19 pandemic, telemedicine implementation presented various challenges at the clinical level. Implementation was more burdensome for some health care providers than for others because of varying levels of existing infrastructure for telemedicine services. Program providers and staff had to be rapidly trained in the available communication technology, screening procedures, billing/coding guidelines, and new workflow modifications. Furthermore, Program members had to be educated on telemedicine expectations, privacy and safety procedures, appointment options, and available technology, in addition to COVID-19 updates, symptoms, testing, and vaccination. The Program’s experience provides insights to help guide future preparedness and response in public health emergencies when in-person services are interrupted.
As COVID-19 pandemic surges subsided, Program providers started to reopen in-person services in various phases. This reopening was evident in data from quarter 3 of 2020, when the rate of in-person visits offset the rate of telemedicine visits. The use of in-person services increased and stabilized throughout the remaining quarters. Of note, many Program providers continued to offer hybrid models that combined in-person and telemedicine services after the end of the COVID-19 public health emergency (May 11, 2023). 29 Hybrid models addressed Program members’ access challenges and allowed for social distancing in clinics during surges of COVID-19 or other respiratory infections (ie, influenza, respiratory syncytial virus). The continuation of both options also alleviated physical space constraints as facilities accommodated a higher volume of seriously ill patients, particularly in metropolitan areas such as New York City. While challenges existed during the COVID-19 pandemic, the availability of telemedicine supported continuity of care and minimized disruption of health services in the Program.
Our study was subject to a limitation that we included only medical services that were paid by the Program; medical services paid by other insurers or medical services not related to WTC conditions were not included in this analysis. As such, both telemedicine use rates and in-person service rates were likely underestimated. Future studies are warranted to understand telemedicine use in the Program. Future research could include topics such as (1) assessing member and health care provider satisfaction with telemedicine services, (2) analyzing telemedicine service data more granularly (ie, zip code location of residence), and (3) assessing telemedicine barriers of members and health care providers.
US health care providers were suddenly forced to shift from in-person services to telemedicine in the early phases of the COVID-19 pandemic. The WTC Health Program rapidly implemented telemedicine services during this period. Expanded telemedicine services allowed the Program to maintain medical screening, monitoring, diagnostic, and selected treatment services during these challenging times. This transition required programmatic adjustments in staff and member education, billing and coding guidance, workflow modification, and other changes. Nonetheless, the rapid transition of in-person services to telemedicine-eligible services at the WTC Health Program provided uninterrupted access to health services for many members during the COVID-19 pandemic. The results and lessons learned outlined in this case study may guide similar health care entities when challenged by time-sensitive disruptions of in-person services.
Footnotes
Acknowledgements
The authors acknowledge and thank for their dedication and service the administrative and health care staff of the Clinical Centers of Excellence and the Nationwide Provider Network who continue to provide care to the World Trade Center Health Program members during the COVID-19 pandemic. The authors also thank Sandra M. Lowe, MD (Icahn School of Medicine at Mount Sinai); Jessica L. Rinsky, PhD, MPH (National Institute for Occupational Safety and Health); and Kelly Armstrong, MA (National Institute for Occupational Safety and Health) for their contributions.
Authors’ Note
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the National Institute for Occupational Safety and Health, the Centers for Disease Control and Prevention, or the US Department of Health and Human Services.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.