
Abstract
Objective:
Death from tuberculosis or HIV among people from racial and ethnic minority groups who are aged <65 years is a public health concern. We describe age-adjusted, absolute, and relative death rates from HIV or tuberculosis from 2011 through 2020 by sex, race, and ethnicity among US residents.
Methods:
We used mortality data from the Centers for Disease Control and Prevention online data system on deaths from multiple causes from 2011 through 2020 to calculate age-adjusted death rates and absolute and relative disparities in rates of death by sex, race, and ethnicity. We calculated corresponding 95% CIs for all rates and determined significance at P < .05 by using z tests.
Results:
For tuberculosis, when compared with non-Hispanic White residents, non-Hispanic American Indian or Alaska Native residents had the highest level of disparity in rate of death (666.7%). Similarly, as compared with non-Hispanic White female residents, American Indian or Alaska Native female residents had a high relative disparity in death from tuberculosis (620.0%). For HIV, the age-adjusted death rate was more than 8 times higher among non-Hispanic Black residents than among non-Hispanic White residents, and the relative disparity was 735.1%. When compared with non-Hispanic White female residents, Black female residents had a high relative disparity in death from HIV (1529.2%).
Conclusion:
Large disparities in rates of death from tuberculosis or HIV among US residents aged <65 years based on sex, race, and ethnicity indicate an ongoing unmet need for effective interventions. Intervention strategies are needed to address disparities in rates of death and infection among racial and ethnic minority populations.
Understanding preventable deaths in people aged <65 years is important because the life expectancy at birth in the United States in 2020 was >65 years for all racial and Hispanic populations. 1 Various conditions contribute to preventable deaths in people aged <65 years, including infectious diseases, chronic diseases, mental health disorders, and health behaviors. 2 Despite government and community efforts to address these issues, disparities in mortality and morbidity rates exist among racial and ethnic groups.3-7 Structural racism—a condition that propagates racial discrimination through housing, education, employment, health care, and criminal justice—can play an insidious role.3,8-12 The Centers for Disease Control and Prevention (CDC) has recognized the imbalance in disease severity and the disproportionate incidence of diseases among racial and ethnic minority groups and urged public health programs to acknowledge and address these broader realities and contexts. 13 In the United States, data on race and health have been continuously collected since 1790, and these data are essential for research that supports policy decisions. 14 Poverty, low education levels, cultural barriers, and other factors have been identified as contributing to poor health outcomes among people from certain racial and ethnic minority groups, especially non-Hispanic Black and American Indian or Alaska Native (AI/AN) people.15,16 Despite the availability of state and federal government-subsidized health services, length and quality-of-life measures for non-Hispanic Black and AI/AN people continue to lag those of other racial and ethnic populations in the United States.17-19
The health care delivery system is complex and varied among population segments in the United States. The major sources of US government–subsidized health care for AI/AN and non-Hispanic Black residents are distinctly different. The Centers for Medicare & Medicaid Services within the US Department of Health and Human Services administers the Medicare program and works with state governments to administer the Medicaid program and Children’s Health Insurance Program. Medicaid and Medicare are both government-sponsored health insurance programs. Medicaid is a joint federal and state program that, with the Children’s Health Insurance Program, provides health coverage to low-income families, qualified pregnant women and children, individuals receiving Supplemental Security Income, and other groups. Medicare provides health insurance for people who are aged ≥65 years, have a disability, or have certain health conditions. 20 Race, ethnicity, or Hispanic origin is not a requirement to qualify for Medicare or Medicaid. However, disparities in health insurance coverage exist by race and Hispanic origin 21 and access to care and health care use. 18 In the United States, health insurance coverage is importance in health care access. Non-Hispanic Black and AI/AN residents are eligible to receive medical treatment and preventive services for which they qualify from US government–subsidized sources (eg, Medicaid, Medicare, Veterans Health Administration). In addition, AI/AN residents can receive medical diagnosis, treatment, and preventive care services from the Indian Health Service, community health centers, and private health insurance. However, despite the availability of US government–subsidized health care services, the health of AI/AN and Black people lags that of people in other racial and ethnic groups.17-19,22,23
Given the persistent state of health disparities, the US government has encouraged partnership building and community involvement to meet Healthy People 2030 objectives, 2 reduce health disparities, and achieve health equity. 24 Partnership building provides an opportunity to address common objectives by combining resources among US government agencies and organizations. 25 The combining of resources could benefit non-Hispanic AI/AN and non-Hispanic Black people by preventing and controlling deaths from HIV or tuberculosis (TB). HIV coinfection as a driver of TB disease and the high prevalence of TB disease among certain population groups in the United States have increased the importance of examining deaths from TB or HIV in people aged <65 years.19,26 Despite reductions in HIV-related death rates since 1981, in 2018 the highest death rate from HIV was among non-Hispanic Black people. 27 However, the rates of people living with diagnosed HIV infection from 2014 through 2018 increased among all racial and ethnic groups, except people of multiple races, for which the rate decreased from 730.0 to 665.7 infections per 100 000 population. 27 In a study (1994-2016) that examined whether decreased TB incidence is accompanied by reduced TB disparities, disparities persisted and increased for some population groups even though TB rates decreased. 28 These findings led to a focus on screening and treatment of latent TB infections.
We examined age-adjusted death rates (AADRs) associated with HIV or TB among people aged <65 years by sex, race, and ethnicity to identify modifiable disparities among Healthy People 2030 objectives that were set in 2010, when US public health programs in socially disadvantaged populations were given a high priority, among other competing priorities, in the allocation of resources to address these diseases.2,19,26,27
Methods
We used data from CDC Wide-ranging Online Data for Epidemiologic Research (CDC WONDER), a system that provides access to an array of public health information. 29 The WONDER system uses data queries for analysis of public health data in the WONDER database and has safeguards to protect individual privacy. The CDC Institutional Review Board reviewed and approved this analytic study, determined that the research did not constitute human participant research, and waived formal ethical review.
We accessed mortality files from 2011 through 2020 for the 50 US states and the District of Columbia; these files included data on the underlying and contributing causes of death 30 and are based on death certificate data reported to CDC’s National Center for Health Statistics (NCHS). This dataset has been used extensively for health-related research, following the recommendations of Redelings et al, 31 who noted that the underlying cause of death alone greatly underestimates the importance of the underlying and contributing cause of death. Therefore, we used data that included multiple causes of death to identify all deaths (ie, we included deaths in which underlying or contributing deaths were mentioned) initiated by or contributing to TB or HIV.31,32 We obtained data on the number of deaths, population number, and death rates by year, sex, race, and ethnicity.
We limited our analysis to deaths associated with HIV (International Classification of Diseases, Tenth Revision codes B20-B24) 30 or TB (codes A16-A19) 30 that occurred before age 65 years to assess the implications of death from HIV or TB for adequate allocation of resources.33,34 Demographic characteristics included sex (male or female) and race and ethnicity (non-Hispanic AI/AN, non-Hispanic Asian or Pacific Islander, non-Hispanic Black or African American, non-Hispanic White, or Hispanic all races). For brevity in data presentation, we used AI/AN, Asian or Pacific Islander, Black, and White and did not include non-Hispanic when presenting, describing, or comparing the results among racial groups. We used a similar presentation format when describing or comparing racial groups by sex.
We calculated absolute disparity (ie, absolute difference in risk between groups) and relative disparity in AADRs per 100 000 population (ie, relative difference in risk between groups).35-37 We calculated absolute disparity for each pair of racial and ethnic groups (ie, the estimate for the reference group minus the estimate for each of the other racial and ethnic groups). We calculated relative disparity (ie, [absolute disparity/reference group] × 100%) for each pairwise comparison between the reference group and the complementary sex and racial and ethnic groups.35-37 For AADRs, age groups, and the standard population (the age distribution used as weights to calculate or create age-adjusted statistics), we used the following age groups as defined in CDC WONDER: <1 year, 1 through 4, 5 through 14, 15 through 24, 25 through 34, 35 through 44, 45 through 54, and 55 through 64 years. 29 We used the 2020 standard population to calculate AADRs. The population numbers for 2020 are bridged-race estimates of the July 1 resident population from the Vintage 2020 postcensal series released by NCHS on September 22, 2021. 29
We determined significant differences in absolute and relative disparity between comparison groups based on the z test, with P < .05 indicating significance. We assessed significance of the trends in death rates using Joinpoint trend analysis software (Joinpoint Regression Program, version 4.7.0.0; Statistical Methodology and Applications Branch, Surveillance Research Program, National Cancer Institute). We assumed that death counts were in Poisson distribution under the null hypothesis of an approximately normal distribution. 38 For presentation of results, we used non-Hispanic White as the reference group (ie, group with the best or lowest rate). We also examined AADRs for HIV or TB by the urbanization index based on the 2013 NCHS Urban–Rural Classification Scheme for Counties. 39
In data collected from 2011 through 2020, 30 of 3538 (0.9%) total records for TB and 749 of 68 809 (1.1%) total records for HIV were missing race-specific information. These data were included in total rate calculations but were excluded in race and ethnicity rate calculations.
Results
Tuberculosis
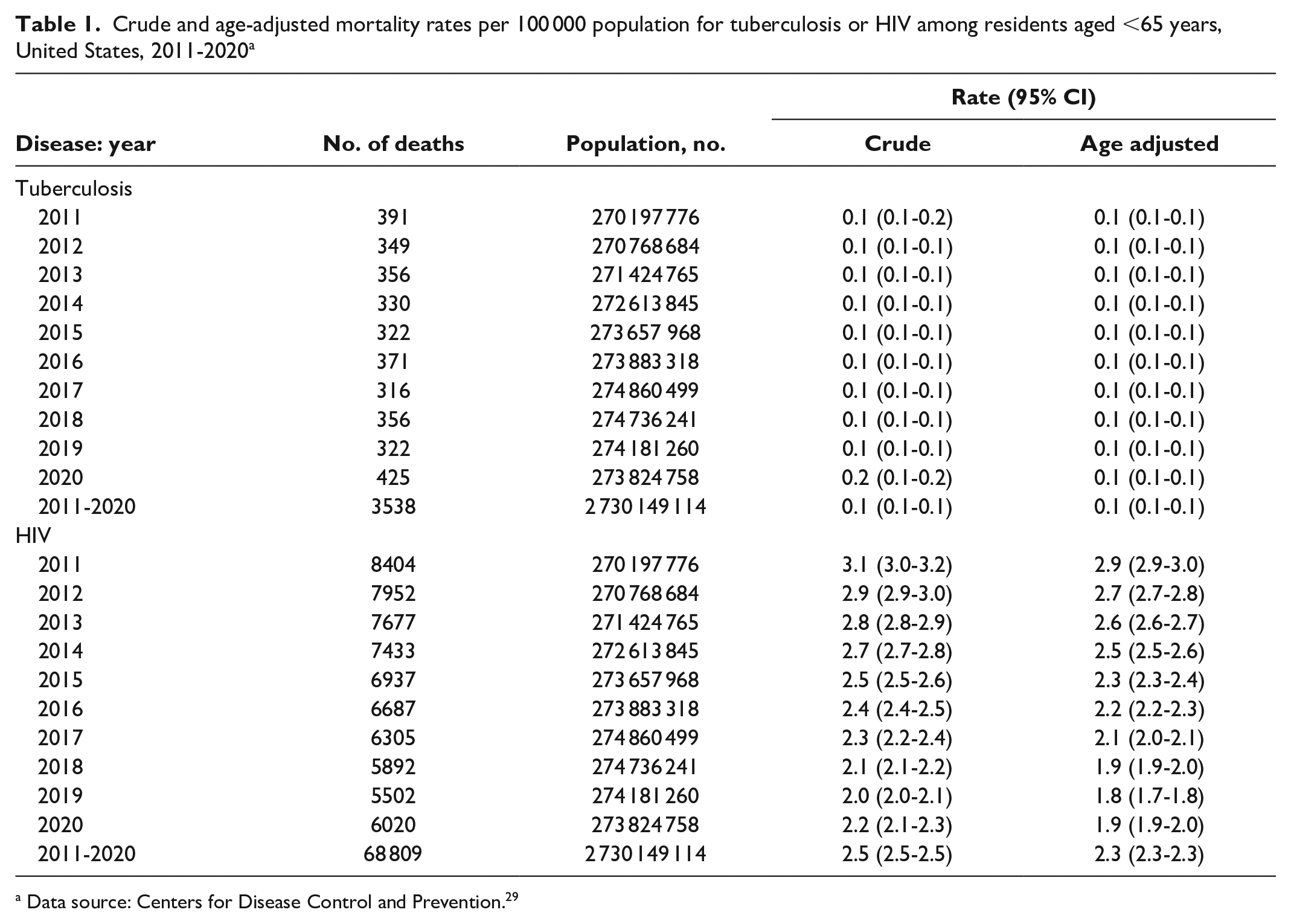
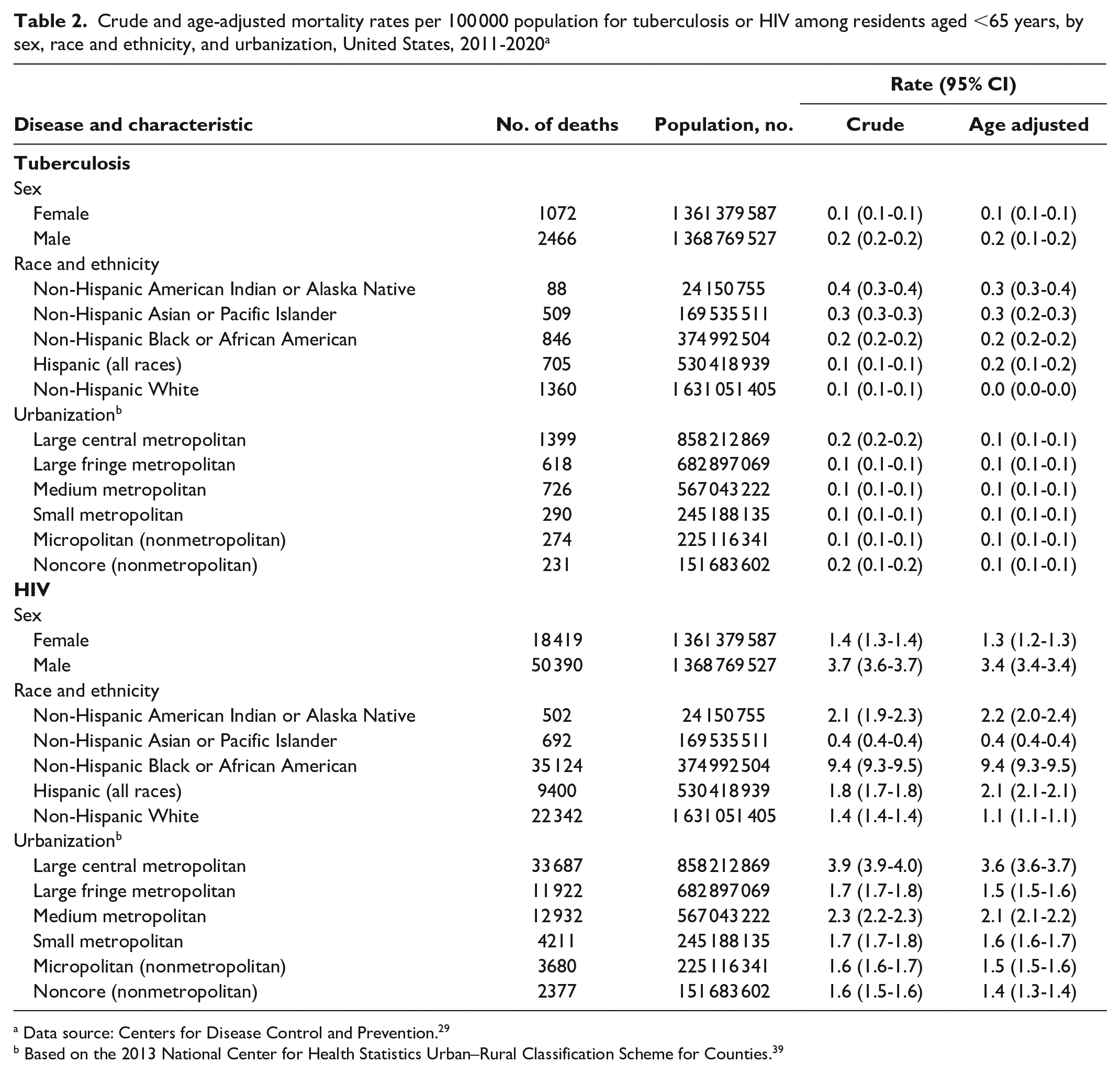
From 2011 through 2020, 3538 deaths were associated with TB, with an average of 354 TB-associated deaths per year. As indicated by the overlapping 95% CIs for the AADRs from year to year and the results of the Joinpoint analysis, rates did not significantly change (stabilized) during the study period (0.1 deaths per 100 000 population) (Table 1). The AADR was higher among male residents than among female residents and differed by race and ethnicity (Table 2). The AADR per 100 000 population was lowest among White residents (0.0) than among those of other racial and ethnic groups (Tables 2 and 3), and AI/AN and Asian or Pacific Islander residents had the highest death rates (0.3 and 0.3), followed by Black residents (0.2). By urbanization, AADRs per 100 000 population were highest in large central metropolitan areas (0.1) and noncore (nonmetropolitan) areas (0.1; data were limited to 1 decimal place).
Crude and age-adjusted mortality rates per 100 000 population for tuberculosis or HIV among residents aged <65 years, United States, 2011-2020 a
Data source: Centers for Disease Control and Prevention. 29
Crude and age-adjusted mortality rates per 100 000 population for tuberculosis or HIV among residents aged <65 years, by sex, race and ethnicity, and urbanization, United States, 2011-2020 a
Data source: Centers for Disease Control and Prevention. 29
Based on the 2013 National Center for Health Statistics Urban–Rural Classification Scheme for Counties. 39
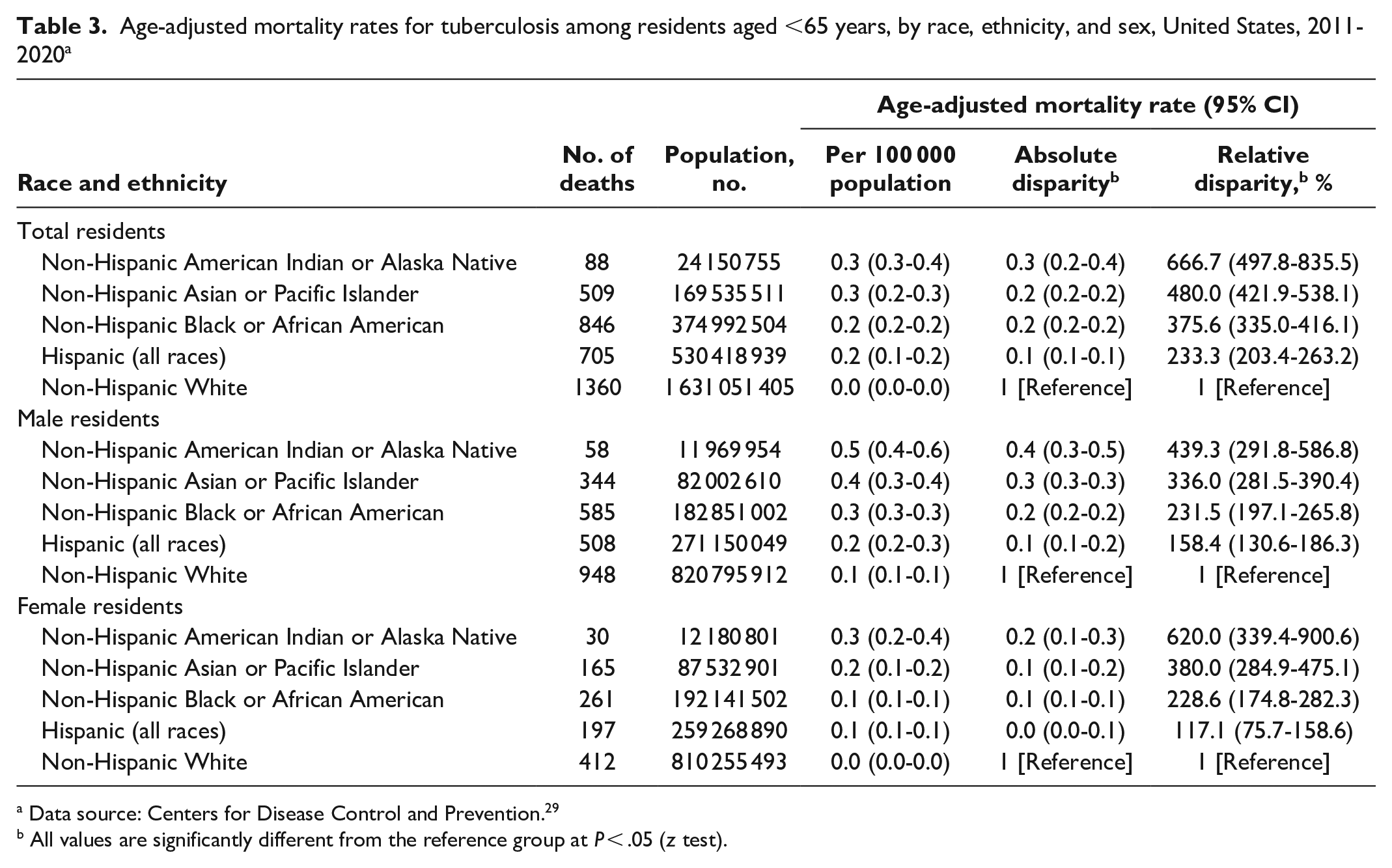
Age-adjusted mortality rates for tuberculosis among residents aged <65 years, by race, ethnicity, and sex, United States, 2011-2020 a
Data source: Centers for Disease Control and Prevention. 29
All values are significantly different from the reference group at P < .05 (z test).
The AADR and relative disparity for death from TB differed significantly between White residents and those from other racial and ethnic groups (Table 3). When compared with White residents, AI/AN residents had the largest relative disparity (666.7%) for death from TB and Hispanic residents had the smallest (233.3%). We also found significant differences by sex among racial and ethnic groups. As compared with White male residents, AI/AN male residents had the highest relative disparity for death from TB (439.3%), followed by Asian or Pacific Islander male residents (336.0%); Black male residents had the lowest relative disparity (231.5%). When compared with White female residents, AI/AN female residents had the highest relative disparity for death from TB (620.0%), which was 3 times that of Black female residents (228.6%).
HIV
From 2011 through 2020, 68 809 deaths were associated with HIV, with an average of 6881 HIV-associated deaths per year (Table 1). AADRs per 100 000 population decreased significantly, from 2.9 deaths in 2011 to 1.9 deaths in 2020, with an overall average rate of 2.3 deaths. As with TB-related mortality rates, we found significant differences in HIV-related AADRs by sex, race, and ethnicity. The AADR per 100 000 population was higher among male residents (3.4) than among female residents (1.3) (Table 2). By race and ethnicity, Black residents had the highest AADR (9.4), which was significantly higher than among White residents (1.1); Asian or Pacific Islander residents had the lowest AADR (0.4). By urbanization, the largest AADR was among residents living in large central metropolitan areas (3.6).
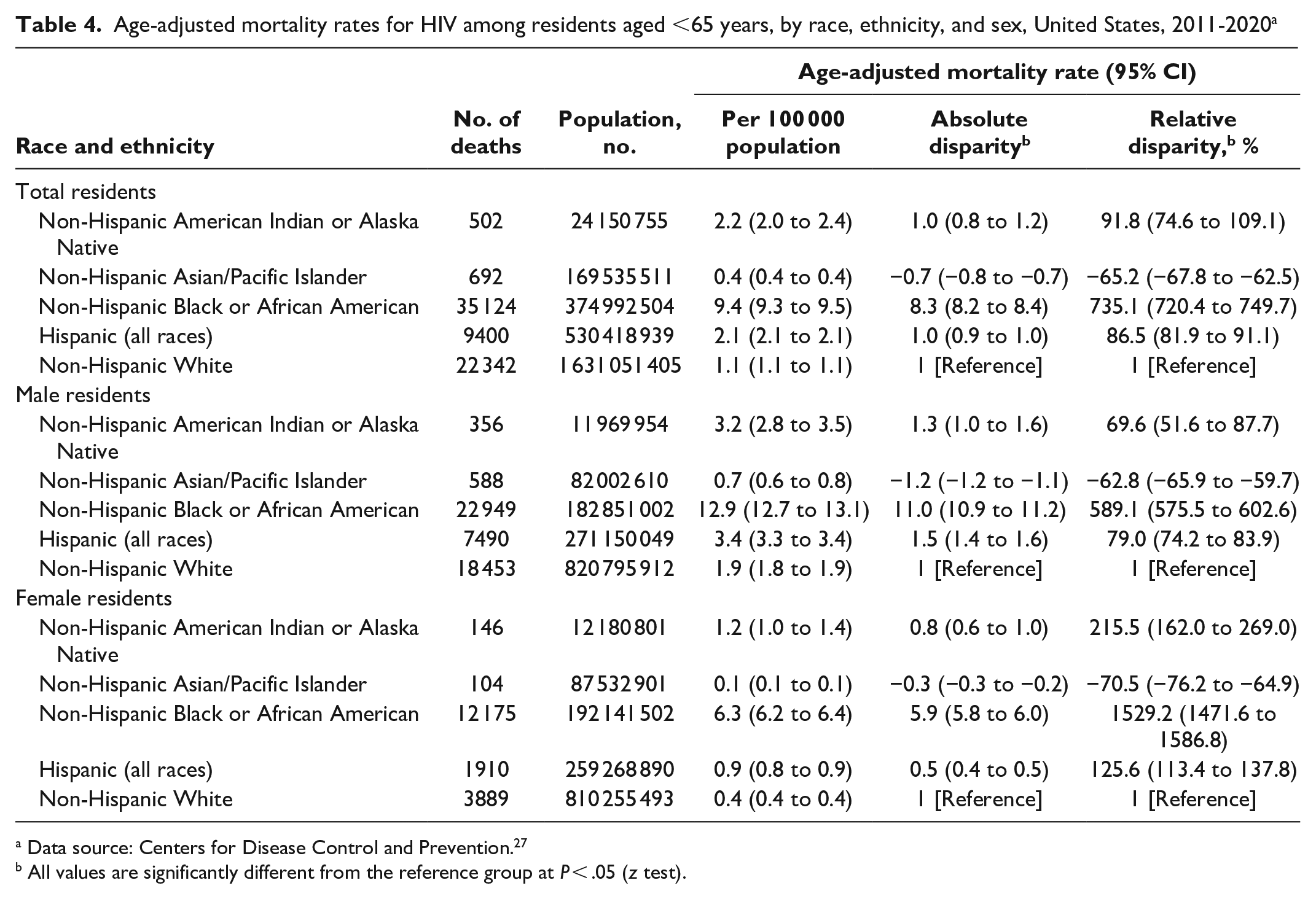
AADRs and relative disparity for death from HIV differed significantly between White residents and those from other racial and ethnic groups (Table 4). Black residents, with a relative disparity of 735.1%, had the largest disparity for death from HIV as compared with White residents. Asian or Pacific Islander residents had a lower AADR than White residents, overall and by sex, and the lowest relative disparity (−65.2%). The AADR per 100 000 population was higher among Black male residents (12.9) than among White male residents (1.9). Similarly, the AADR was significantly higher among Black female residents (6.3) than among White female residents (0.4); in addition, Black female residents had the largest relative disparity for death from HIV (1529.2%) as compared with White female residents.
Age-adjusted mortality rates for HIV among residents aged <65 years, by race, ethnicity, and sex, United States, 2011-2020 a
Data source: Centers for Disease Control and Prevention. 27
All values are significantly different from the reference group at P < .05 (z test).
Discussion
We described AADRs from HIV or TB as underlying or contributing causes of death by using death certificate data of all deaths in the United States. The use of mortality data to monitor health disparities in deaths from HIV or TB is well established.35-37 Previous studies have highlighted the need to continually measure and monitor health disparities.36,39 From 2011 through 2020, although the TB-related AADR stabilized at 0.1 deaths per 100 000 population, deaths associated with HIV declined by 34% to an AADR of 2.3 per 100 000 population. Despite the stabilization of and decrease in TB- and HIV-associated mortality, substantial health inequities and disparities remain.40,41
Timely and effective health care options are needed to reduce morbidity and mortality associated with TB and HIV. 41 For example, the proportion of people aged <65 years with health insurance coverage increased significantly from 83.2% in 2008 to 86.7% in 2014, 42 which may have contributed to the overall stabilization of TB-associated deaths and the decrease in HIV-related deaths that we observed. Similarly, the widely documented disparities in timely access to and use of effective health care 18 might explain the disparities in mortality that we observed. For example, higher levels of access to health care among White people as compared with people in other racial and ethnic groups might explain their lower mortality rates. High TB-related AADRs among AI/AN people, particularly females, is concerning given the availability of the Indian Health Service to deliver health care to this population. 43 Relative and absolute disparities were highest among male and female AI/AN people than among people in other racial and ethnic groups, particularly White people. Specific reasons for this observation warrant further exploration.
Although many health inequalities affect people who are Black, the Black population in our study had a significantly lower TB-related AADR than the AI/AN population, a nonsignificantly lower AADR than the Asian or Pacific Islander population, and a significantly higher AADR than the White population. Efforts have been made to improve health outcomes in all racial and ethnic populations, including Black populations, and in non–US-born populations.44,45 More effective community-based efforts could help improve health outcomes among AI/AN populations. However, unlike the TB-related AADR, the HIV-related AADR among Black people in our study group was significantly higher than among all other racial and ethnic groups. The relative and absolute Black–White disparities in the HIV-related AADR among Black females were particularly striking: in absolute number of deaths, 3 times more deaths occurred, and the AADR was 16 times higher among Black female residents than among White female residents. Reasons are unclear why Black people had different experiences with TB or HIV disparities from 2011 through 2020, and our findings may reflect differences in patterns of exposure. The differences highlight the need for enhanced research, monitoring, and interventions to reduce residual disparities in TB- and HIV-related death rates among Black people.
Our observation of limited variability in TB-related death rates in urban versus rural areas could indicate successful implementation of strategies such as integrated care by multidisciplinary teams with case management services.46,47 Our observation could also mean that nonurban areas are diagnosing TB as effectively as urban areas, although urban areas would be more likely than rural areas to have multidisciplinary teams and access to clinicians who know to test for TB. High rates of TB have been reported among US-born and non–US-born people living in areas identified as being low income, being densely populated, having high rates of unemployment, and having populations with low levels of education. 48 When compared with other life-threatening infectious diseases, TB is relatively rare, has nonspecific symptoms, and has diagnostic tests with limited sensitivity and specificity. Therefore, prompt TB diagnosis, which prevents TB-associated mortality, requires access to clinicians who consider TB in their differential diagnoses, particularly when symptoms persist despite treatment for other, more common conditions (eg, community-acquired pneumonia) with overlapping symptoms. However, unlike the care of patients with TB through an integrated approach, a comprehensive approach might work better for patients with HIV (eg, enhanced education, focused funding, community engagement, consideration of social vulnerability), particularly to address high rates of HIV-related deaths in the Black population.49,50
Strengths and Limitations
This study had 2 strengths. One was that the death certificate data source offers consistency in data over time, ease of use in understanding disease trends, and usefulness in developing and monitoring Healthy People objectives. Another strength was that our findings are generalizable to the general population, and the inclusion of AADRs contributes to an understanding of health disparities. 51
Our study also had some limitations. First, details of our study design, analysis, and interpretation may have affected the validity (accuracy) or precision (certainty) of the findings to the US population from 2011 through 2020. Second, we did not generate state-level analysis for HIV or TB 52 because that was not the focus of our current research. However, the urbanization index that we used (large central metropolitan, large fringe metropolitan, medium metropolitan, small metropolitan, micropolitan, and noncore) could be used to develop and enhance programs; the implications of these diseases have been documented nationally.1,2,24,26 For example, a consistent AADR for TB was found among urbanization options, whereas AADRs for HIV varied considerably among urbanization options, with rates highest among large central metropolitan areas and lowest among noncore areas. Third, racial misclassification on death certificates has been studied extensively and might have affected our findings. Racial misclassification on death certificates has implications for how we study and address health disparities and health services because mortality rates among AI/AN people have been reported to be higher than among the general population.43,53 Fourth, this research was cross-sectional and did not account for socioeconomic factors and comorbidities of decedents. Factors such as excessive alcohol consumption, smoking, injection drug use, and diabetes influence health outcomes, including those related to HIV and TB. These factors are particularly concerning among certain population groups (eg, Black, AI/AN) in the United States. In addition, the Social Vulnerability Index can identify adversely affected communities. 54 Fifth, because of the study design, we did not consider confounding of the association of race and ethnicity and AADR by US-born versus non–US-born geographic origin. 48 Lastly, this study used vital statistics data compiled by NCHS. Our study may have yielded slightly different results than studies that use surveillance programs that prospectively follow people. 48
Conclusions
AADRs associated with HIV or TB among people aged <65 years differed by race, ethnicity, and sex, with higher mortality rates among racial and ethnic minority residents than among White residents. Although our results included a small number of deaths among AI/AN residents, we found that the largest disparities in TB-related mortality rates were between AI/AN residents and non-Hispanic White residents, with large disparities between male and female AI/AN residents and their non-Hispanic White counterparts. HIV-related death rates were significantly higher among Black residents than among residents of all other racial and ethnic groups, with particularly large disparities found for Black female residents.
Thousands of TB cases are still reported annually in the United States, and clinically severe or drug-resistant TB can be life-threatening without timely and effective treatment. Moreover, people with latent TB infection can develop life-threatening disease. Addressing disparities in deaths through strategies such as access to health care, health care resources, transportation, education, comorbidity, and implementation of comprehensive prevention and treatment programs is critical to achieving health equity. Further reductions in TB deaths, especially among the groups identified in our study, will require expanding testing and treatment of latent TB infection.19,55-57
Footnotes
Acknowledgements
Dr Benedict I. Truman retired in May 2022. The authors thank Greta Tessman, MA (CDC), for editorial support and Rick Song, PhD (CDC), and Ramal Moonesinghe, PhD (CDC), for statistical consultations.
Disclaimer
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention (CDC).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.