
Abstract
Objectives:
Women experiencing homelessness have higher rates of unintended pregnancy than stably housed women and may benefit from reproductive interconception care. How reproductive interconception care differs between women who did and did not experience perinatal homelessness is not known. We estimated prevalence ratios of reproductive interconception behaviors among US women experiencing homelessness during the perinatal period.
Methods:
We used data from the 2016-2019 Pregnancy Risk Assessment Monitoring System to calculate the prevalence of 5 reproductive interconception care outcomes: attending a maternal postpartum checkup, participating in a conversation with a health care provider about birth intervals, receiving family planning counseling, obtaining a prescription for short-acting contraception, and having a long-acting reversible contraceptive inserted. We used complex survey weights, stratified by perinatal homelessness, and converted adjusted logistic regression odds ratios between housing status and outcome variables to adjusted prevalence ratios (aPRs) and 95% CIs.
Results:
Among participants, approximately 2.4% (weighted percentage; unweighted 2953 of 100 706) experienced homelessness sometime in the 12 months before their children were born; the majority were non-Hispanic (83.2%) and White (69.4%), were not married (82.2%), and had public health insurance (56.8%). Perinatal homelessness was significantly associated with a lower prevalence of attending a postpartum maternal visit (aPR = 0.90; 95% CI, 0.87-0.94) and a higher prevalence of having a conversation about birth intervals with their health care providers (aPR = 1.13; 95% CI, 1.03-1.21).
Conclusions:
Findings suggest that improving attendance at postpartum visits and evaluating birth interval conversations may strengthen interconception care practices while contextualizing social determinants such as housing stability. Improving uptake of postpartum visits may reduce unintended pregnancy, short birth intervals, and adverse birth outcomes in future pregnancies among women experiencing homelessness.
Homelessness is a critical public health issue. The US Department of Housing and Urban Development defines homelessness as having a shelter or place not suitable for residency as a primary nighttime residence. 1 The 2020 US Point-in-Time count, which includes sheltered and unsheltered homelessness, estimated that 580 000 people experienced sheltered homelessness and, of them, 223 578 (39%) were women. 1
In a longitudinal study of homelessness comparing women and men, women were younger and had more children, and they were more likely to be unemployed, less educated, less empowered, more psychologically stressed, and more victimized. 2 Moreover, women experiencing homelessness have several health disparities as compared with women who are stably housed, potentially resulting in a greater financial burden and sustained homelessness, which may explain an increase in homelessness rates from previous years. 3 When compared with women in the general population, women experiencing homelessness have an increased risk for sexual and reproductive health problems, such as sexually transmitted infections, sexual coercion, exchange sex, and lack of preventive screenings (eg, sexually transmitted infection screenings, mammograms, prenatal care, and Papanicolaou tests).4,5 Additionally, women experiencing homelessness have twice the rate of unintended pregnancy (10%) than women who are stably housed (5%). 6
Unintended pregnancy (ie, mistimed or unwanted) may be especially problematic for women experiencing homelessness, exacerbating financial constraints and potential intergenerational homelessness.7,8 The American College of Obstetricians and Gynecologists recommends assessment of maternal well-being in a postpartum visit, typically around 6 weeks and no later than 12 weeks, 9 given the associations of such visits with improved screening and treatment for key maternal mortality-related concerns, such as hemorrhage, endometritis, thromboembolic disease, hypertensive disorders, gestational diabetes, thyroid disorders, depression, and intimate partner violence. 10 The interconception period (ie, the interval between pregnancies) can also be an opportune time to reduce the potential for unintended pregnancies and promote healthy ones.
Interconception care (ie, care between pregnancies) includes conversations and screenings for several health conditions affecting maternal and child health, such as maternal depression, folic acid intake, smoking, and family planning. 11 Reproductive interconception care (ie, care related directly to reproductive family planning) is associated with reduced rates of prematurity, low birthweight, and congenital anomalies, conditions that are frequently associated with short birth intervals (<24 months).12 -14 For women experiencing homelessness, interconception care that either reduces the potential for unintended pregnancy and short birth intervals (eg, use of contraception) or promotes healthy pregnancies before subsequent pregnancies (eg, family planning discussions with a health care provider) may reduce the potential for cyclical homelessness and improve quality of life.15,16 Knowing the prevalence of reproductive interconception care for women (including all pregnant people, regardless of gender) who are experiencing homelessness can establish whether certain social determinants of health (eg, housing) can create a unique obstacle to the uptake of interconception care, which then can help to determine what to prioritize when developing health promotion interventions for populations vulnerable to poor reproductive health outcomes.
Establishing the prevalence of reproductive interconception care behaviors among women experiencing homelessness is necessary to determine whether additional or improved reproductive care during the interconception period is warranted for these women and their children. This study aimed to establish the prevalence of reproductive interconception care behaviors among women experiencing homelessness and determine whether the prevalence of this care differs significantly by housing status. We hypothesized that the prevalence of reproductive interconception care behaviors among women experiencing homelessness would be significantly lower than among women who are stably housed, when adjusting for demographic and perinatal covariates.
Methods
Study Population
The data source was 2016-2019 Phase 8 data from the Pregnancy Risk Assessment Monitoring System (PRAMS). 17 PRAMS is a population-based, site-specific surveillance system partnership between the Centers for Disease Control and Prevention and local, state, and regional health departments to identify women and infants at risk of poor health outcomes and to track progress toward improving mother and infant health. 18 PRAMS uses birth certificate files to randomly sample women with a live birth 2 to 6 months postpartum. 18 Women respond to the survey by submitting a mailed PRAMS questionnaire or participating in a telephone interview (if they do not respond to the mailing), both of which could be completed up to 9 months after delivery. 18
Eligibility criteria for this study were (1) participation in PRAMS and (2) a response of yes or no to whether homelessness was experienced 12 months before delivery, a standard (state-optional) question asked in 34 sites. In addition, we set a response rate threshold for PRAMS sites (55% in 2016-2017 or 50% in 2018-2019). Thirty jurisdictions had a ≥50% response rate in 2018-2019 or ≥55% response rate in 2016-2017: Alabama, Alaska, Colorado, Connecticut, Delaware, Florida, Georgia, Illinois, Indiana, Iowa, Kansas, Kentucky, Louisiana, Maine, Massachusetts, Michigan, Minnesota, Mississippi, Missouri, Nebraska, New York City, New York State, North Carolina, North Dakota, Oregon, Pennsylvania, South Dakota, Utah, Wisconsin, and Wyoming. Because this study used deidentified data, it was deemed non–human subjects research by the North Texas Regional Institutional Review Board; thus, full review was waived.
Measures
All variables came from responses to the PRAMS survey. Our primary independent variable was housing status based on whether the participant was homeless or had to sleep outside, in a car, or in a shelter during the 12 months before her newborn was born (yes/no). Five primary outcomes assessed reproductive interconception care behaviors. The first outcome assessed whether participants attended a maternal postpartum checkup at 4 to 6 weeks (yes/no). If the answer was yes, we assessed 4 additional dichotomous outcomes (yes/no), including whether the postpartum care provider (1) talked about how long to wait before getting pregnant again, (2) discussed birth control methods to use postpartum, (3) prescribed a short-acting contraceptive method (eg, pill, patch, shot, ring), and (4) inserted a long-acting reversible contraceptive (LARC; eg, intrauterine device or implant).
We identified potential confounding covariates on the basis of a literature review and the availability of survey questions with at least 70% of valid responses among the study’s eligible sample.19 -23 Preconception covariates were whether the respondent, at a health care visit 12 months before becoming pregnant, had a conversation with a health care provider about the desire to have children or not (yes/no) or the use of birth control to prevent pregnancy (yes/no). The question about pregnancy desire asked participants how they felt about the idea of becoming pregnant just before they became pregnant with their most recent infant. Response options were as follows: (1) “I wanted to be pregnant later,” (2) “I wanted to be pregnant sooner,” (3) “I wanted to be pregnant then,” (4) “I didn’t want to be pregnant then or any time in the future,” and (5) “I wasn’t sure what I wanted.” The survey determines the timing of the participant’s first prenatal care visit, which is initially assessed by the number of weeks pregnant at the first visit and is then categorized by trimester (first, second, or third) with a fourth category (none) for participants with no prenatal care visit. The survey also assessed whether contraception and family planning were discussed during the prenatal period (yes/no).
Demographic covariates were as follows:
Maternal age: <18, 18-24, 25-29, 30-34, ≥35 years
Health insurance: private (any employer provided, nongovernmental), public (Medicaid, Children’s Health Insurance Program [CHIP or state CHIP], or other government-offered insurance with no private insurance), other (another insurance type that is not private or public), no insurance
Maternal education: <9th grade, 9th-12th grade (no degree), high school degree or GED (General Educational Development), some college/2-year degree, ≥4-year degree
For maternal race and ethnicity, demographic descriptive data included Hispanic or Latinx for ethnicity (yes/no) and the following race categories: American Indian/Alaska Native, Asian/Pacific Islander, Black or African American, White, other race (for any race not previously listed), and mixed race (reporting ≥2 races). In adjusted analysis, to account for small cell sizes, we operationalized race and ethnicity into 4 categories: Hispanic (any race), non-Hispanic Black, non-Hispanic White, and non-Hispanic other race (for any race not White or Black) or mixed race.
Data Analysis
We used SAS version 9.4 (SAS Institute Inc) to estimate the prevalence of the 5 reproductive interconception care outcomes among women experiencing homelessness and women who were stably housed. All statistical calculations incorporated complex survey analysis including standardized weights and strata. To account for missing data, we used the SAS option NOMCAR, which instructs SAS to perform a domain analysis of missing and nonmissing values. 24 We used the Taylor series variance estimation method for survey analysis. 24 Bivariate Rao–Scott χ2 tests determined whether each reproductive interconception care outcome was significantly associated with homelessness; we considered P < .05 to be significant. 25
Five adjusted logistic regression models estimated the odds ratios (ORs) with covariate-adjusted associations between housing status and each of the 5 reproductive interconception care outcomes, using complex survey analysis including standardized weights and strata. We selected all covariates on the basis of past associations with homelessness and birth outcomes19 -23 and entered these covariates into models for model selection. We systematically assessed each covariate for inclusion in the final model on the basis of confounding (using direct acyclic graphs to examine potential confounding relationships between exposure and outcomes), biological plausibility, extent of missingness, and overall model fit. Model fit comparisons using direct acyclic graphs and change in estimation criterion ensured that final models had the best fit without overcorrection. We then converted adjusted ORs (aORs) into prevalence ratios by using the following formula: prevalence ratio = OR/[(1 – P0) + (OR × P0)], where P0 is the risk of the outcome (eg, attending maternal postpartum visits) in the unexposed population (ie, unexposed to homelessness). 26 We calculated 95% CIs accordingly. All descriptions of the sample are reported as unweighted sample sizes and weighted percentages.
Results
The study sample consisted of 100 706 participants, with 2953 (2.4%) experiencing homelessness (Table 1). Most were aged 25-29 years (29.2%) or 30-34 years (29.6%). Most (83.2%) reported non-Hispanic/Latinx ethnicity, and the majority (69.4%) self-identified as White, as compared with 15.6% Black, 5.3% Asian/Pacific Islander, 0.9% American Indian/Alaska Native, 5.9% other race, and 2.8% mixed race. The proportion that reported having any private health insurance was 59.4%. By education level, the largest proportion (37.0%) had ≥4-year degree, followed by some college/2-year degree (27.3%), high school degree or GED (24.1%), and less than a high school degree (11.6%). All demographic characteristics except Hispanic ethnicity were significantly different (P < .05) between women experiencing homelessness and women who were stably housed.
Prevalence of women experiencing homelessness during the perinatal period and characteristics of participants (n = 100 706) in 30 sites in the Pregnancy Risk Assessment Monitoring System, United States, 2016-2019 a
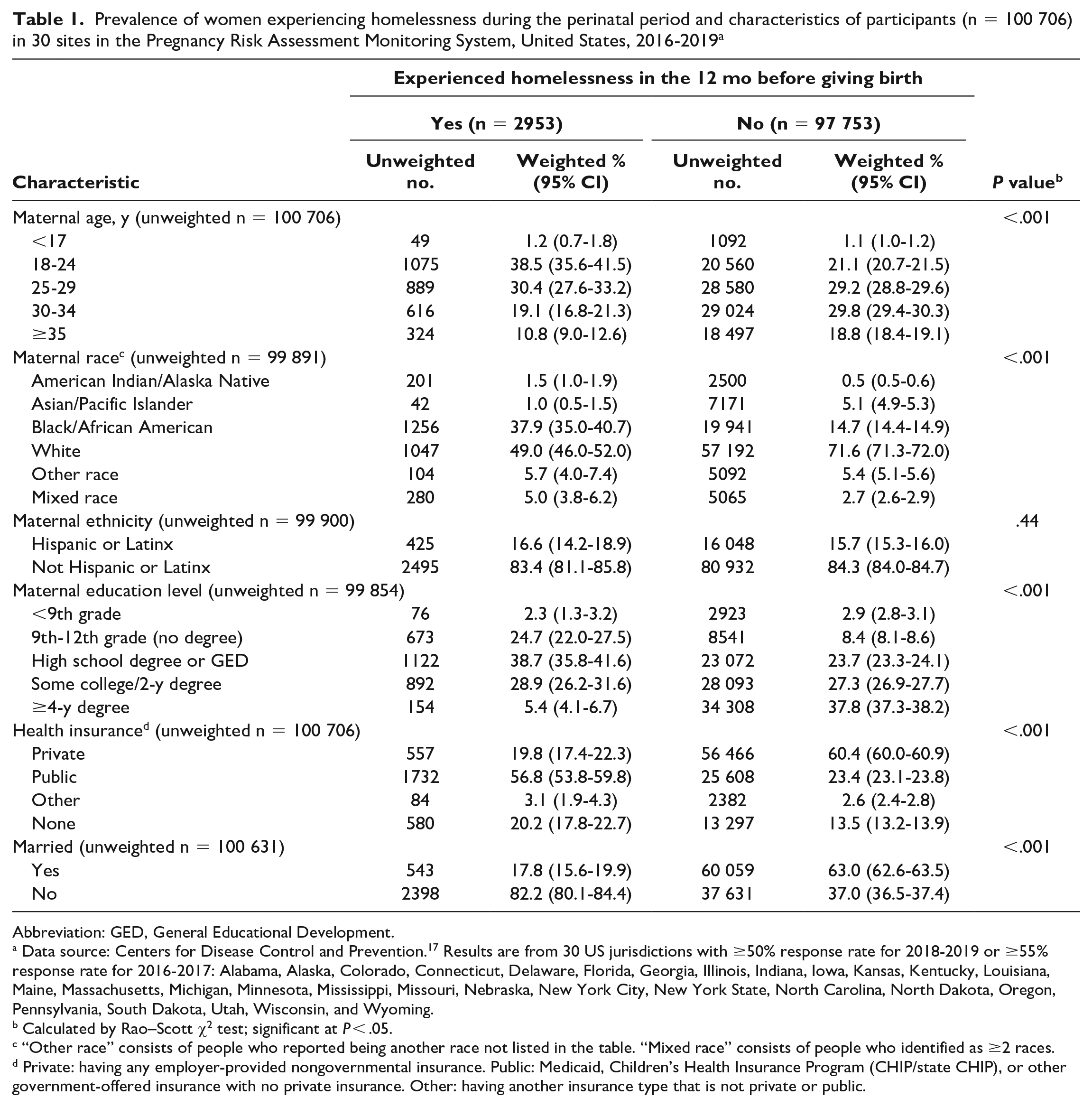
Abbreviation: GED, General Educational Development.
Data source: Centers for Disease Control and Prevention. 17 Results are from 30 US jurisdictions with ≥50% response rate for 2018-2019 or ≥55% response rate for 2016-2017: Alabama, Alaska, Colorado, Connecticut, Delaware, Florida, Georgia, Illinois, Indiana, Iowa, Kansas, Kentucky, Louisiana, Maine, Massachusetts, Michigan, Minnesota, Mississippi, Missouri, Nebraska, New York City, New York State, North Carolina, North Dakota, Oregon, Pennsylvania, South Dakota, Utah, Wisconsin, and Wyoming.
Calculated by Rao–Scott χ2 test; significant at P < .05.
“Other race” consists of people who reported being another race not listed in the table. “Mixed race” consists of people who identified as ≥2 races.
Private: having any employer-provided nongovernmental insurance. Public: Medicaid, Children’s Health Insurance Program (CHIP/state CHIP), or other government-offered insurance with no private insurance. Other: having another insurance type that is not private or public.
Bivariate Analysis
There were 3 significant reproductive interconception care outcomes: (1) having attended a maternal postpartum visit, (2) having a postpartum conversation about pregnancy intervals, and (3) having a postpartum LARC inserted (Table 2). A significantly larger proportion of women who were stably housed reported attending a maternal postpartum visit as compared with women who experienced homelessness (91.2% vs 73.7%; P < .001). Conversely, the proportion of women receiving counseling on birth intervals and insertion of LARC was larger among women experiencing homeless than among women who were stably housed (58.3% vs 49.7% [P < .001] and 25.2% vs 20.2% [P < .001], respectively).
Prevalence of reproductive interconception care outcomes among women, by experience of homelessness during the perinatal period, in 30 sites in the Pregnancy Risk Assessment Monitoring System, United States, 2016-2019 a
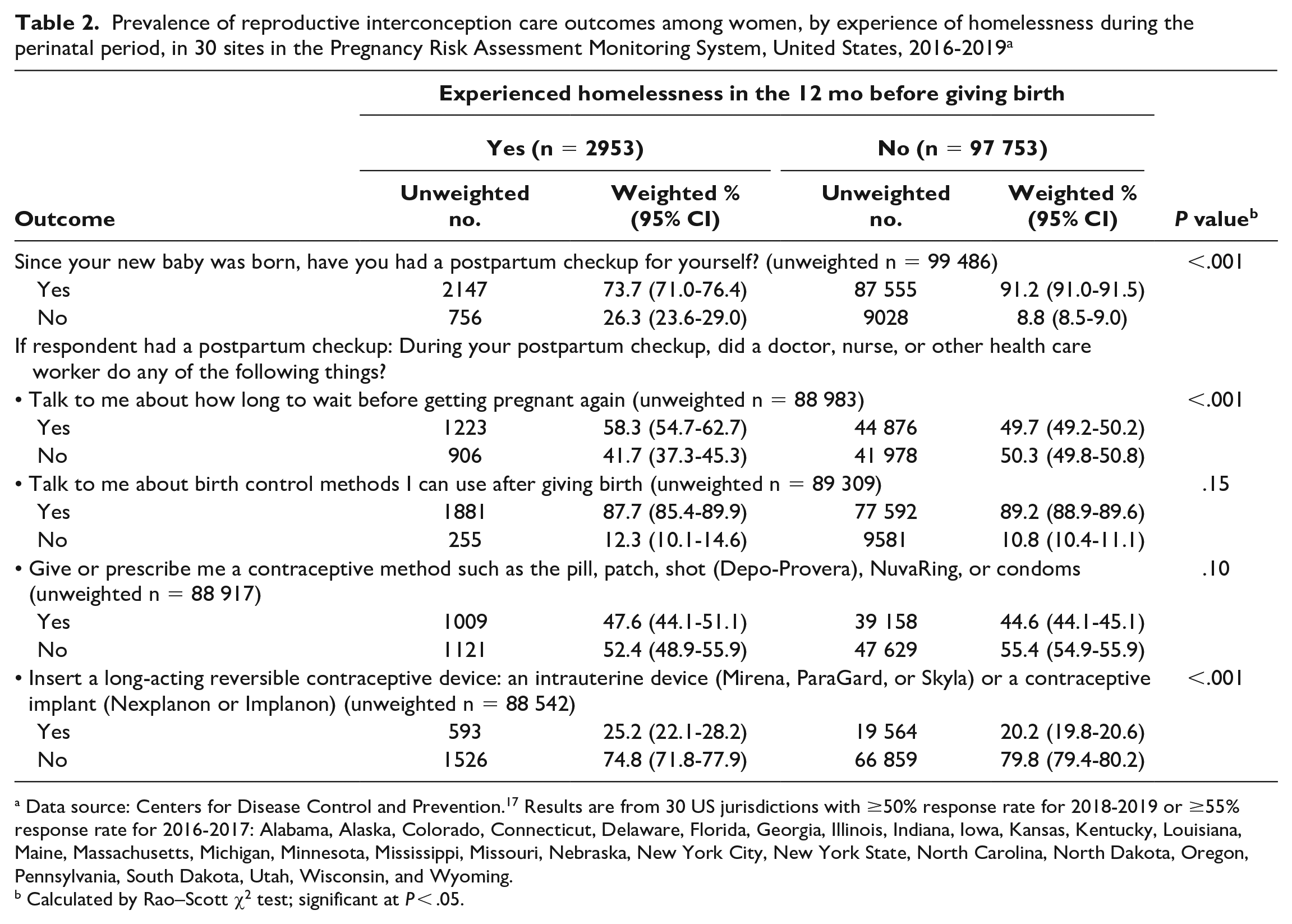
Data source: Centers for Disease Control and Prevention. 17 Results are from 30 US jurisdictions with ≥50% response rate for 2018-2019 or ≥55% response rate for 2016-2017: Alabama, Alaska, Colorado, Connecticut, Delaware, Florida, Georgia, Illinois, Indiana, Iowa, Kansas, Kentucky, Louisiana, Maine, Massachusetts, Michigan, Minnesota, Mississippi, Missouri, Nebraska, New York City, New York State, North Carolina, North Dakota, Oregon, Pennsylvania, South Dakota, Utah, Wisconsin, and Wyoming.
Calculated by Rao–Scott χ2 test; significant at P < .05.
Adjusted Models
Like the bivariate results, the adjusted models showed that attending a maternal postpartum visit and having a postpartum conversation about pregnancy intervals were significantly associated with experiencing perinatal homelessness (Table 3). When compared with women who were stably housed, women experiencing homelessness had a lower prevalence of attending a maternal postpartum visit (aPR = 0.90; 95% CI, 0.87-0.94). Among those who attended a maternal postpartum visit, women experiencing perinatal homelessness had a higher prevalence of having a conversation about birth intervals with their health care providers than women who were stably housed (aPR = 1.13; 95% CI, 1.03-1.21). Having a postpartum LARC inserted was no longer significantly associated with experiencing perinatal homelessness after adjusting for covariates (aPR = 0.98; 95% CI, 0.76-1.08). Similarly, postpartum contraception or family planning counseling (aPR = 0.97; 95% CI, 0.93-1.01) and prescription of short-acting contraception (aPR = 0.97; 95% CI, 0.87-1.08) were significantly associated with experiencing perinatal homelessness.
Association between experiencing homelessness during the perinatal period and 5 reproductive interconception outcomes, in 30 sites in the Pregnancy Risk Assessment Monitoring System, United States, 2016-2019 a
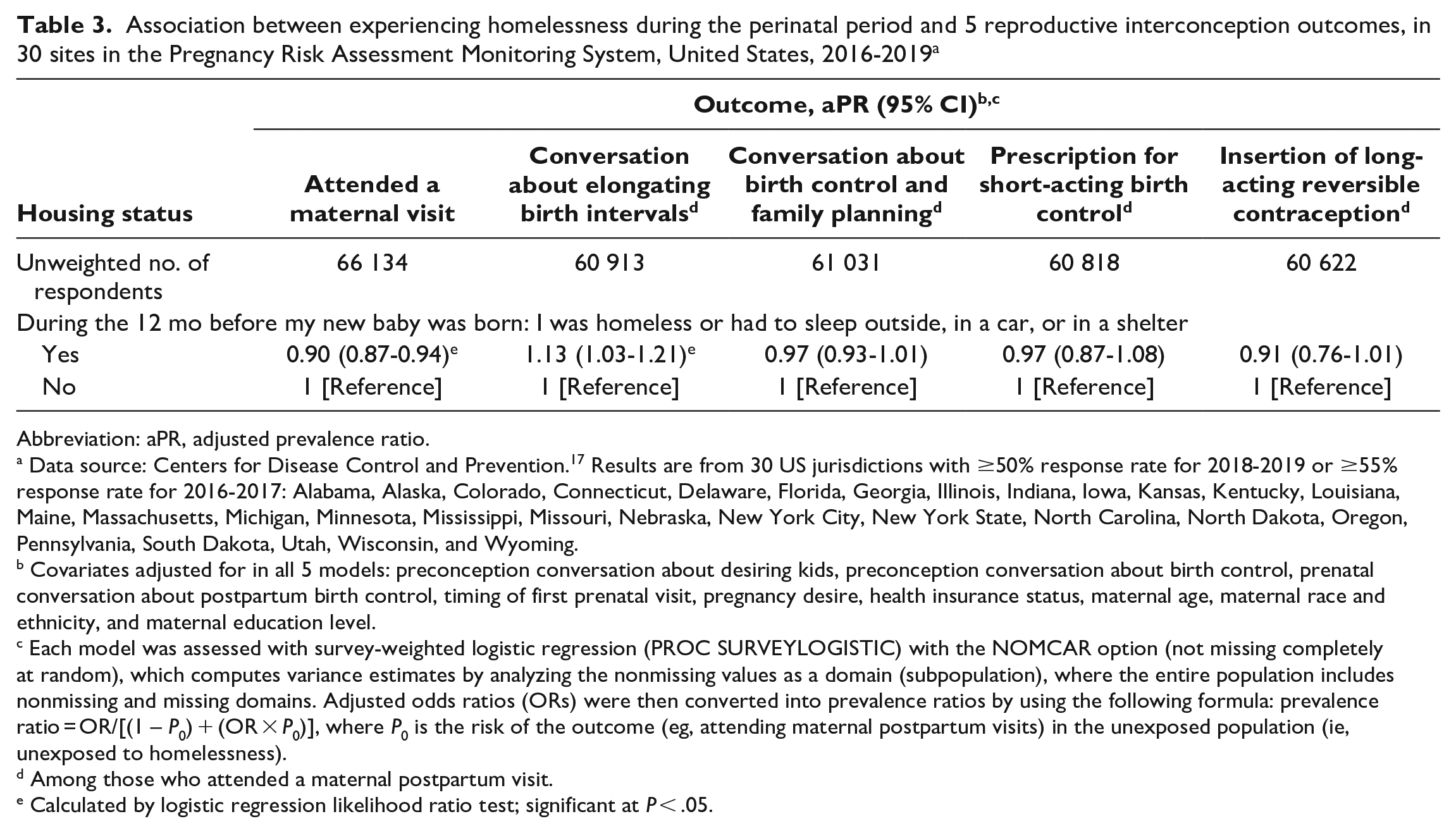
Abbreviation: aPR, adjusted prevalence ratio.
Data source: Centers for Disease Control and Prevention. 17 Results are from 30 US jurisdictions with ≥50% response rate for 2018-2019 or ≥55% response rate for 2016-2017: Alabama, Alaska, Colorado, Connecticut, Delaware, Florida, Georgia, Illinois, Indiana, Iowa, Kansas, Kentucky, Louisiana, Maine, Massachusetts, Michigan, Minnesota, Mississippi, Missouri, Nebraska, New York City, New York State, North Carolina, North Dakota, Oregon, Pennsylvania, South Dakota, Utah, Wisconsin, and Wyoming.
Covariates adjusted for in all 5 models: preconception conversation about desiring kids, preconception conversation about birth control, prenatal conversation about postpartum birth control, timing of first prenatal visit, pregnancy desire, health insurance status, maternal age, maternal race and ethnicity, and maternal education level.
Each model was assessed with survey-weighted logistic regression (PROC SURVEYLOGISTIC) with the NOMCAR option (not missing completely at random), which computes variance estimates by analyzing the nonmissing values as a domain (subpopulation), where the entire population includes nonmissing and missing domains. Adjusted odds ratios (ORs) were then converted into prevalence ratios by using the following formula: prevalence ratio = OR/[(1 – P0) + (OR × P0)], where P0 is the risk of the outcome (eg, attending maternal postpartum visits) in the unexposed population (ie, unexposed to homelessness).
Among those who attended a maternal postpartum visit.
Calculated by logistic regression likelihood ratio test; significant at P < .05.
Discussion
Using 2016-2019 PRAMS data, this study compared estimates of reproductive interconception care behaviors between women experiencing homelessness and women who were stably housed during the perinatal period. Approximately 2.4% of PRAMS participants experienced homelessness in the 12 months before their infants were born. Attending a postpartum maternal visit was less prevalent among participants who were experiencing homelessness than among those who were stably housed, while having a conversation about birth intervals with a health care provider was more prevalent among participants experiencing homelessness.
In samples of postpartum women participating in other large national cross-sectional surveys, the prevalence of postpartum visit attendance was approximately 89%.27,28 In our study, approximately 73.7% of participants experiencing homelessness and 91.2% who were stably housed attended a maternal postpartum visit. Our findings may suggest difficulty among women experiencing homelessness with making health care appointments, consistent with previous research on women and other people experiencing homelessness.29 -32 The unique experiences of unstable housing may affect maternal postpartum visit attendance; further research is needed to assess whether the interconception period may be an opportune time to facilitate improvements in maternal outcomes for this population. Future studies should integrate our quantitative findings with qualitative data to provide a perspective directly from women experiencing homelessness and pregnancy and to identify barriers and facilitators to reproductive interconception care. This information is especially important for women experiencing homelessness, who are more transient than stably housed women and who may delay or skip postpartum visits and other perinatal and contraceptive services because of competing priorities or lack of streamlined services.33,34
The American College of Obstetricians and Gynecologists recommends that all postpartum health care providers discuss the avoidance of a birth interval <6 months and the risks and benefits of repeat pregnancy earlier than 18 months. 9 In our study, conversations about birth intervals during maternal postpartum visits occurred more frequently among women experiencing homelessness than among women who were stably housed. Among the subset of PRAMS-participating women who did attend their postpartum maternal visits, women experiencing homelessness had a 1.13-times higher prevalence of receiving birth interval counseling than women who were stably housed. This finding may highlight how women who are pregnant and experiencing homelessness may benefit from attending maternal postpartum visits, where they may get birth interval counseling. Alternatively, this finding may demonstrate the perceived need for birth interval conversations in health care for all pregnancy-capable people. Future research should determine how to increase the provision of just reproductive health care for women experiencing homelessness. Health care providers may have a bias against women experiencing homelessness or assume that they do not want children or should be on a form of contraception. Future studies should also consider health care provider bias toward pregnancy during homelessness, given that conversations about birth intervals occurred more frequently among women experiencing homelessness than among women who were stably housed. It is critical for health care providers to facilitate autonomous and informed decision making.
Postpartum conversations about contraception and family planning counseling occurred among 89.2% of women who attended their postpartum visits and did not differ significantly by housing status. These findings are comparable to those in previous studies that reported postpartum interconception conversations about contraceptives and family planning at roughly 89.0%, 35 with a smaller percentage of women (86%) using short-acting birth control or LARC postpartum. 23 In our study, the provision of postpartum short-acting birth control was not significantly associated with homelessness. Although unadjusted estimates revealed significant associations between postpartum LARC insertion and homelessness, this relationship was no longer significant in the adjusted model. This finding may suggest that associations between LARC insertion and perinatal homelessness are better explained by other covariates that the model adjusted for (eg, health insurance status) rather than homelessness alone. In addition to access-related barriers, other barriers to contraception uptake are either shelter-related (storage and privacy, timing restrictions) or based on personal beliefs and misinformation about contraception (fear of side effects, effects on fertility, normative beliefs).36,37 Our study provides additional support for the need to identify barriers and facilitators to postpartum contraception for the population experiencing homelessness. Future research should examine contextualized needs from women who are recently pregnant and homeless with recent lived experiences. For organizations with sufficient funding and infrastructure, provision of reproductive interconception care through telehealth may help reach women experiencing homelessness who have internet access, but future studies should identify additional novel cost-saving ways to connect with postpartum women experiencing homelessness.
Limitations
Our study had several limitations. First, it had a cross-sectional design. PRAMS is a single point-in-time snapshot; thus, causality and temporality cannot be inferred. Second, responses were self-reported, with the possibility of recall and social desirability bias. Third, because of the way in which homelessness is assessed in PRAMS, we could not determine whether participants were pregnant before, during, or after experiencing homelessness. Fourth, the question uses a narrow definition of homelessness from the US Department of Housing and Urban Development, which does not include people who are unstably housed in doubled-up situations or staying in hotels or motels because of an inability to afford housing. 1 Fifth, although we used survey weighting to increase response generalizability, the births in the 50 jurisdictions that participate in PRAMS surveillance represent approximately 81% of all live US births, 18 so our findings cannot be generalized to the entirety of the United States. Sixth, homelessness was assessed in only 34 jurisdictions, with just 30 having at least a 50% response rate, excluding other states with notably higher rates of homelessness (eg, California). These findings may underestimate the prevalence of reproductive interconception care for people who are recently pregnant and homeless. Lastly, we excluded 2020 and 2021 PRAMS data because of the potential effect of the COVID-19 pandemic on access to reproductive care and homelessness.
Conclusion
Health care clinicians, community partners, and policy makers can seek to reduce barriers to the attendance of maternal postpartum visits and improve supportive reproductive health outcomes. Certain strategies in promoting follow-up include health care and community organization partnerships, multisystem care coordination, and community advocacy.33,34 Systems of care in partnership with women experiencing homelessness can build support of policies that promote access to postpartum and interconception health care coupled with economic support for pregnant and postpartum women. Reducing the additional burdens and various priorities of recently pregnant women experiencing homelessness may help to empower these populations to engage in preventive care and promote health for themselves and their children.
With the narrow definition of homelessness used in our study, estimates may understate the actual picture of homelessness in the United States, especially among women and children. A study published in 2021 used American Community Survey public-use microdata to show that 3.7 million people in the United States were doubled up in 2019 (ie, living with others because of economic hardship or housing loss). 38 Identifying ways to access postpartum people who are doubled up or living in hotels or motels and who may not receive shelter services is another critical next step in facilitating postpartum and interconception care for recently pregnant women experiencing homelessness. Community organizations and health care providers who serve postpartum people who were recently pregnant and homeless can also benefit from incorporating comprehensive and streamlined screening instruments that assess homelessness or risk for homelessness. Several housing screening tools exist 39 that can further explore types of homelessness beyond sheltered and unsheltered homelessness. Other social determinants of health can be screened in conjunction with housing to ensure that holistic social care is provided to improve health outcomes.39,40
Our findings lay the groundwork for understanding how homelessness may affect attendance at maternal postpartum visits and whether the interconception period may be used to facilitate improvements in maternal outcomes for the population experiencing homelessness. Findings may strengthen current interconception practices and augment reductions in unintended pregnancy, short birth intervals, or adverse birth outcomes in future pregnancies among women experiencing homelessness.
Footnotes
Acknowledgements
The authors acknowledge the PRAMS Working Group and the Centers for Disease Control and Prevention. Thank you to the PRAMS Team of the Centers for Disease Control and Prevention (Applied Sciences Branch, Division of Reproductive Health) and the representatives of the PRAMS Working Group: Danita Crear, DrPH (Alabama), Kathy Perham-Hester, MS, MPH (Alaska), Mary McGehee, PhD (Arkansas), Alyson Shupe, PhD (Colorado), Jennifer Morin, MPH (Connecticut), George Yocher, MS (Delaware), Pamela Oandasan, MPH (District of Columbia), Jerri Foreman, MPH (Florida), Jenna Self, MPH (Georgia), Emily Roberson, MPH (Hawaii), Theresa Sandidge, MA (Illinois), Jenny Durica, MPH (Indiana), Sarah Mauch, MPH (Iowa), Jane Herwehe, MPH (Louisiana), Tom Patendaude, MPH (Maine), Diana Cheng, MD (Maryland), Emily Lu, MPH (Massachusetts), Cristin Larder, MS (Michigan), Judy Punyko, PhD, MPH (Minnesota), Brenda Hughes, MPPA (Mississippi), Venkata Garikapaty, PhD, MPH, MSc, MS (Missouri), JoAnn Dotson, PhD, MSN (Montana), Brenda Coufal (Nebraska), Paulette Valliere, MPH (New Hampshire), Lakota Kruse, MD (New Jersey), Eirian Coronado, MPH (New Mexico), Candace Mulready-Ward, MPH (New York City), Anne Radigan-Garcia (New York State), Kathleen Jones-Vessey, MS (North Carolina), Sandra Anseth (North Dakota), Connie Geidenberger, PhD (Ohio), Alicia Lincoln, MSW, MSPH (Oklahoma), Kenneth Rosenberg, MD, MPH (Oregon), Tony Norwood (Pennsylvania), Sam Viner-Brown, PhD (Rhode Island), Mike Smith, MSPH (South Carolina), Angela Miller, PhD, MSPH (Tennessee), Rochelle Kingsley, MPH (Texas), Lynsey Gammon, MPH (Utah), Peggy Brozicevic, MA (Vermont), Marilyn Wenner (Virginia), Linda Lohdefinck, BS (Washington), Melissa Baker, MA (West Virginia), Mireille Perzan, MPH (Wisconsin), and Amy Spieker, MPH (Wyoming).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.