
Abstract
Reproductive interconception care provided at maternal postpartum visits may help reduce unintended pregnancies and elongate birth intervals for women experiencing homelessness. To improve interconception care uptake, this qualitative study aimed to identify barriers and facilitators to reproductive interconception care from the perspectives of women who were recently pregnant and homeless. A semi-structured interview guide and demographic survey were developed based on epidemiological findings, Information-Motivation-Behavioral Skill framework components, and a review by community health workers for content validity. After conducting 12 interviews with women recently pregnant and homeless in a local continuum of care in 2022, audio-recorded interviews were transcribed, iteratively coded using a priori and emerging codes, and thematically analyzed. Key themes were identified to determine implications and next steps to improving reproductive interconception care uptake. Interrelated themes focused on information (e.g., knowledge and misconceptions about pregnancy, birth intervals, contraception), motivation (e.g., attitudes about interconception care experiences, perinatal social influences), behavioral skills (e.g., objective ability to obtain interconception care and perceived self-efficacy related to attending maternal postpartum visits and increasing birth intervals), and macro-level factors (e.g., obtaining housing, contextualizing socioeconomic factors, navigating COVID-19). The findings suggest the need for flexible, streamlined, and personalized interconception care delivery that acknowledges pressing housing and relationship considerations and supports women’s autonomy. Improvements to reproductive interconception care may reduce future unintended pregnancies, increase birth intervals, and improve birth outcomes among women experiencing homelessness.
According to the American College of Obstetricians and Gynecologists (ACOG), maternal wellbeing should be reassessed 6–12 weeks postpartum (McKinney et al., 2018). Maternal postpartum visits are associated with improved screening and treatment for key maternal mortality-related concerns, such as postpartum hemorrhage, hypertensive disorders, gestational diabetes, and postpartum depression (Paladine et al., 2019). Interconception care (ICC), a period of perinatal health promotion focused on care between pregnancies, typically occurs at maternal postpartum visits and consists of several behaviors that overlap with postpartum and preconception care (Rosener et al., 2016). ICC also comprises several reproductive behaviors, allowing women to control the timing of their pregnancies and improving birth outcomes of subsequent pregnancies (Rosener et al., 2016).
In a study of reproductive ICC behaviors among a large U.S. sample, 89.3% had a maternal postpartum checkup, 89.0% received contraceptive use counseling, and 85.1% were using contraceptives (D’Angelo et al., 2007). In another large ICC study, within 12 months of getting pregnant with their most recent child, 13% of women had a previous preterm birth, and 16% had a miscarriage, fetal death, or stillbirth (Richards et al., 2011). ACOG recommends that postpartum women learn about the potential risks and benefits of interpregnancy intervals before 18 months and avoid interpregnancy intervals shorter than 6 months, based on an increased risk of perinatal death (Louis et al., 2019; Regan et al., 2020). ICC reduces birth-related risks associated with short interpregnancy birth intervals, such as prematurity, low birthweight, and congenital anomalies (Cox et al., 2011; Goyal et al., 2017; Shannon et al., 2014). Given these disparities in maternal and child outcomes between women who receive ICC and women who do not, ICC provision is an important tool to improve life course trajectory.
While ICC is important for all women desiring or open to having children in the future, reproductive ICC may be especially beneficial for women with conflicting needs and priorities, such as women experiencing homelessness. Several cross-sectional and longitudinal studies have demonstrated worse health outcomes for people with unstable housing versus similar low-income participants who are stably housed (Bassuk et al., 1996; Cutts et al., 2015; Meadows-Oliver, 2003; Weinreb et al., 1998; Wood et al., 1990). Women experiencing homelessness are also at an increased risk of sexually transmitted infections, sexual coercion, exchange sex, and a lack of preventive screenings, compared to the general population of reproductive-aged women (Chau et al., 2002; Teruya et al., 2010). ICC behaviors also differ between postpartum women experiencing homelessness versus stably housed women: in a 33-state study, experiencing homelessness was associated with lower odds of attending a postpartum maternal visit (adjusted odds ratio [aOR] = 0.45, 95% confidence interval [CI] = [0.37, 0.56]) and higher odds of having a conversation about birth intervals with a health care provider (aOR = 1.30, 95% CI = [1.07, 1.57]), compared to women who did not experience homelessness (Galvin et al., in press). While improving access and promoting the uptake of maternal postpartum visits are important, these visits must include adequate screening and ICC counseling, especially regarding reproductive care and family planning. Qualitative analysis is one method for identifying specific barriers and facilitators to attending maternal postpartum visits, including counseling topics that would be beneficial such as birth interval spacing and pregnancy prevention.
Current Study
This qualitative study of reproductive ICC among women experiencing homelessness builds on previous quantitative findings that established a baseline for reproductive ICC behavior prevalence among this population (Galvin et al., in press). To elicit barriers and facilitators related to key reproductive ICC behaviors such as maternal postpartum visits and birth interval conversations, theoretical constructs of the Information-Motivation-Behavioral Skills (IMB) model (Fisher & Fisher, 1992) were incorporated based on successful utilization in previous studies with similar populations and sexual and reproductive behaviors (Chang et al., 2014). Therefore, this study explored the salient reproductive ICC barriers and facilitators related to information (e.g., knowledge), motivation (e.g., personal attitudes), and behavioral skills (e.g., perceived self-efficacy) among women recently pregnant and homeless to potentially improve ICC, reduce unintended pregnancy, elongate birth intervals, and reduce adverse birth outcomes.
Methods
Participants
Individuals were eligible if they (1) were assigned female at birth, (2) were aged 18 years or older, (3) had delivered a child in the past 4 years, and (4) experienced homelessness (i.e., sheltered, unsheltered, extended motel/hotel stay, or doubled-up/couch surfing) in the past 12 months or while pregnant. Participants were recruited at local shelters, homeless camps, homelessness service and resource centers, Early Head Start programs, and food pantries. Flyers were distributed at these local organizations, and the research team actively recruited on site. Eighteen women were eligible from screening, and 12 of the eligible women were interviewed. Of the six women not interviewed, one opted to no longer participate, and five were lost to follow-up.
Procedure
Screenings were performed via telephone, email, or on site. Interviews were conducted either via telephone or in person at a preferred location by the primary author, who identifies as an Asian, heterosexual, cis-gendered woman pregnant at the time of data collection and analysis. Screening criteria were re-verified at the interview. After informed consent and Health Insurance Portability and Accountability Act authorization were obtained, eligible, consenting participants completed a 30- to 60-minute audio-recorded interview. Participants completed a brief demographic survey prior to the interview. Participants received compensation ($45 grocery gift card) either in person or via email. Interviewer notes reflecting on potential bias or vicarious trauma were also documented.
Instruments
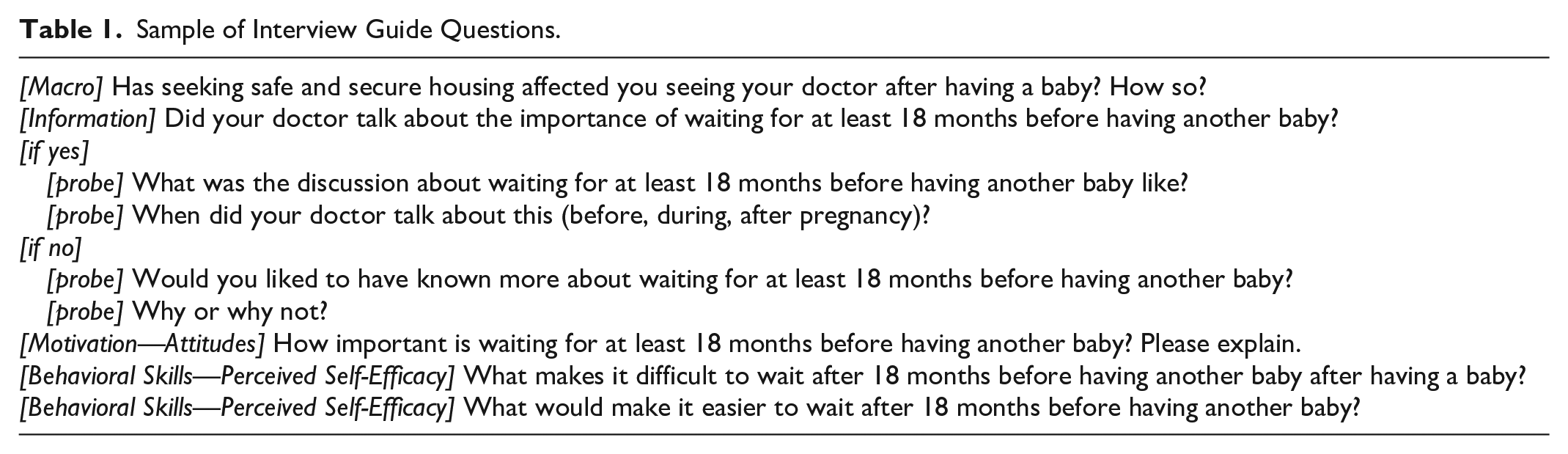
Semi-structured qualitative interview guides (Table 1) were developed, with questions that assessed IMB constructs related to maternal postpartum visits and birth intervals: information knowledge, motivational attitudes, social influences, perceived vulnerability, behavioral skill objective ability, perceived self-efficacy, and other broad, macro-level factors. The demographic survey assessed maternal demographics, homelessness status (current living situation, past living situation while homeless, homelessness history), and pregnancy history (prenatal care, pregnancy and birth history, unintended pregnancy history). The survey and interview were reviewed for content validity and readability by an affiliated organization of health care and social service providers that facilitates partnerships between researchers and community members. The final interview guide, demographic survey, and the study protocol were approved by the North Texas Institutional Review Board for the protection of human participants.
Sample of Interview Guide Questions.
Data Analysis
Interviews were transcribed by the primary author and a professional transcription service. Deidentified transcriptions were repeatedly read and coded by the first two authors in MAXQDA v. 22 (VERBI Software, Berlin, Germany) using coding, filtering, and sorting features. Initial codes were developed a priori based on the theoretical IMB constructs, used to formulate the semi-structured interview guide, and then assigned to passages in the transcripts. The initial phase of coding involved open coding, assessing segments of the interview, and assigning discrete, meaningful interpretations of the passage. Codes were iteratively reviewed, and changes and the addition of pertinent emergent codes were incorporated into the codebook and coding process.
Using MAXQDA, chance-corrected Rädiker & Kuckartz Kappa (Delgado & Tibau, 2019; Kuckartz & Rädiker, 2019) demonstrated sufficient (above 81%) interrater reliability (McHugh, 2012). Coding discrepancies were reviewed by the research team to achieve consensus. Themes were identified, and saturation was evaluated during the coding process. Recently collected demographic data on housing duration and type were also calculated for additional macro-level context.
Results
Among the 12 participants interviewed (Tables 2 and 3), the average age was 28.5 years (standard deviation [SD] 7.0, range 20–42 years), the average number of lifetime pregnancies was 4.2 (SD 4.0, range 1–13), and the average number of lifetime births was 2.7 (SD 1.8, range 1–8). The majority of women (58%) reported that all their pregnancies and children were unplanned. Most women were either currently doubled-up (33%) or in transitional housing (33%). The majority (67%) reported that their most recent homelessness episode lasted 1–3 years. In the past 3 years, most participants (52%) had experienced homelessness more than once. All participants experienced some form of homelessness during the postpartum period, whereas 83% experienced homelessness during their most recent pregnancy, and 75% experienced homelessness prior to their most recent pregnancy. Of the 235 total person-months of perinatal housing (Figure 1), 48.1% of person-months were doubled-up (i.e., couch-surfing, staying with friends/relatives), 20.0% person-months were in stable housing, 10.6% person-months were in hotels/motels, 10.6% person-months were in transitional housing, 6.8% person-months were spent in an emergency shelter, and 3.8% person-months were spent unsheltered (Figure 2).
Sample Demographics Among Participating Women Recently Pregnant and Homeless (n = 12), 2022.
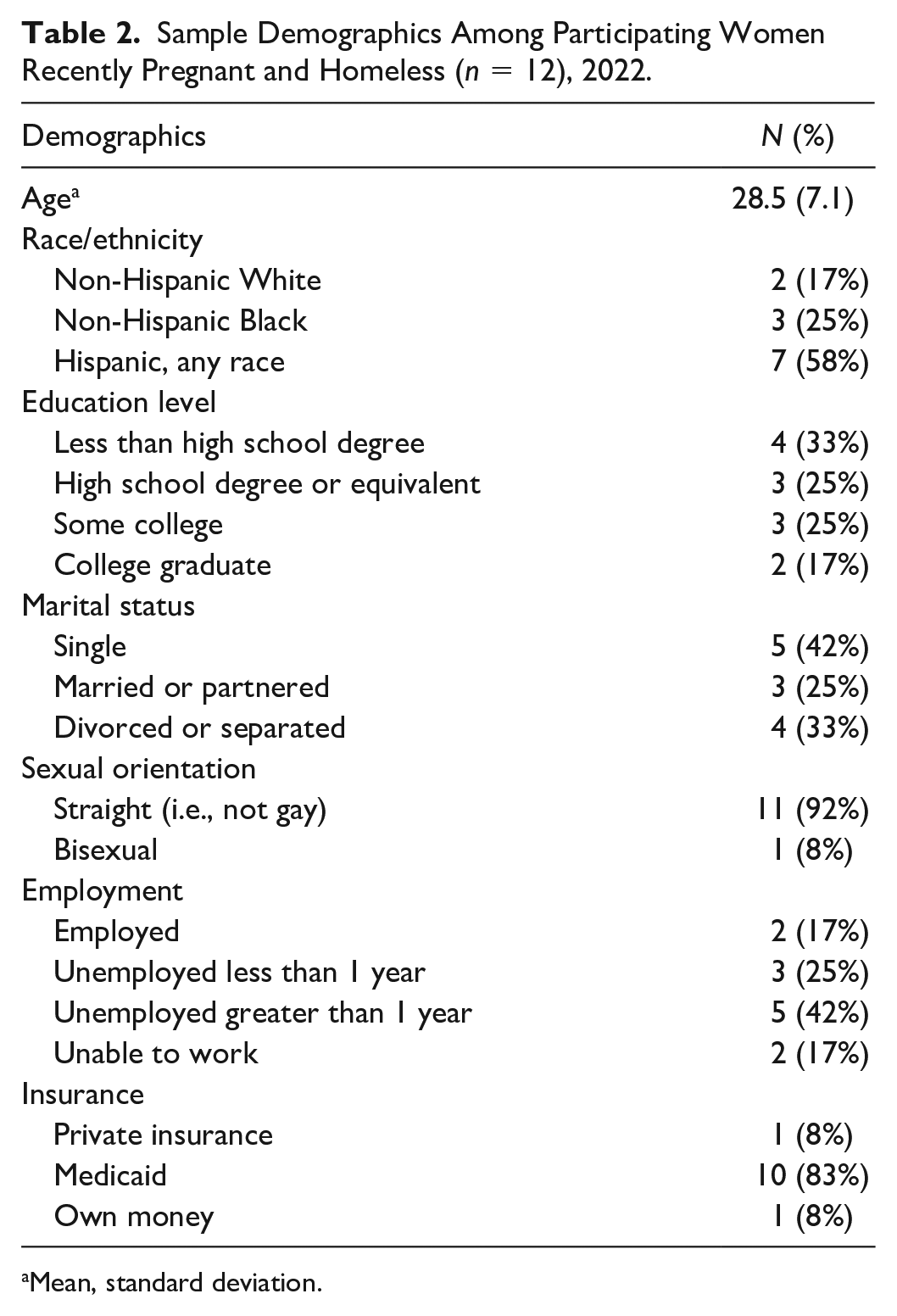
Mean, standard deviation.
Housing, Pregnancy, and Childbirth Characteristics Among Participating Women Recently Pregnant and Homeless (n = 12), 2022.
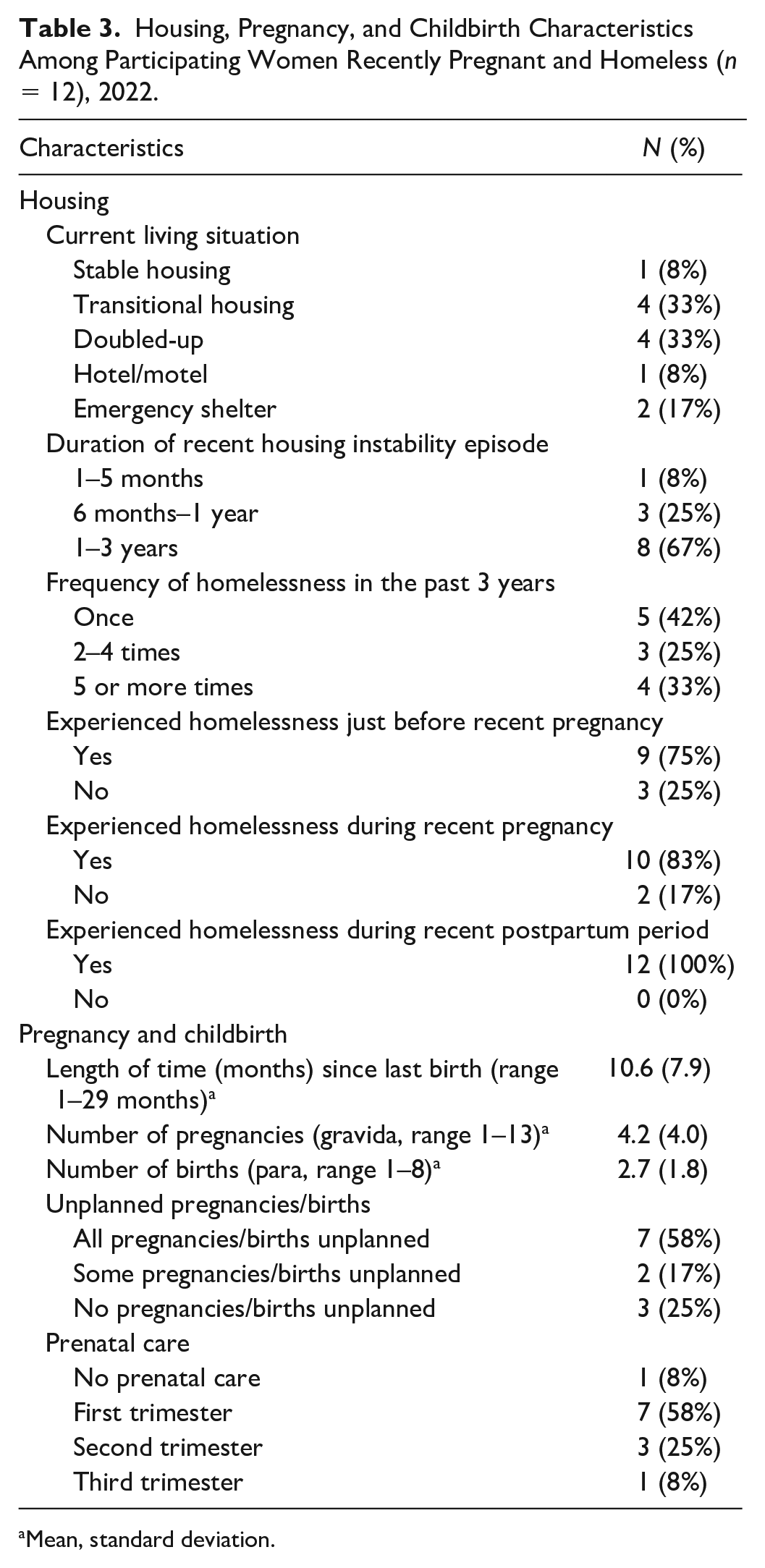
Mean, standard deviation.
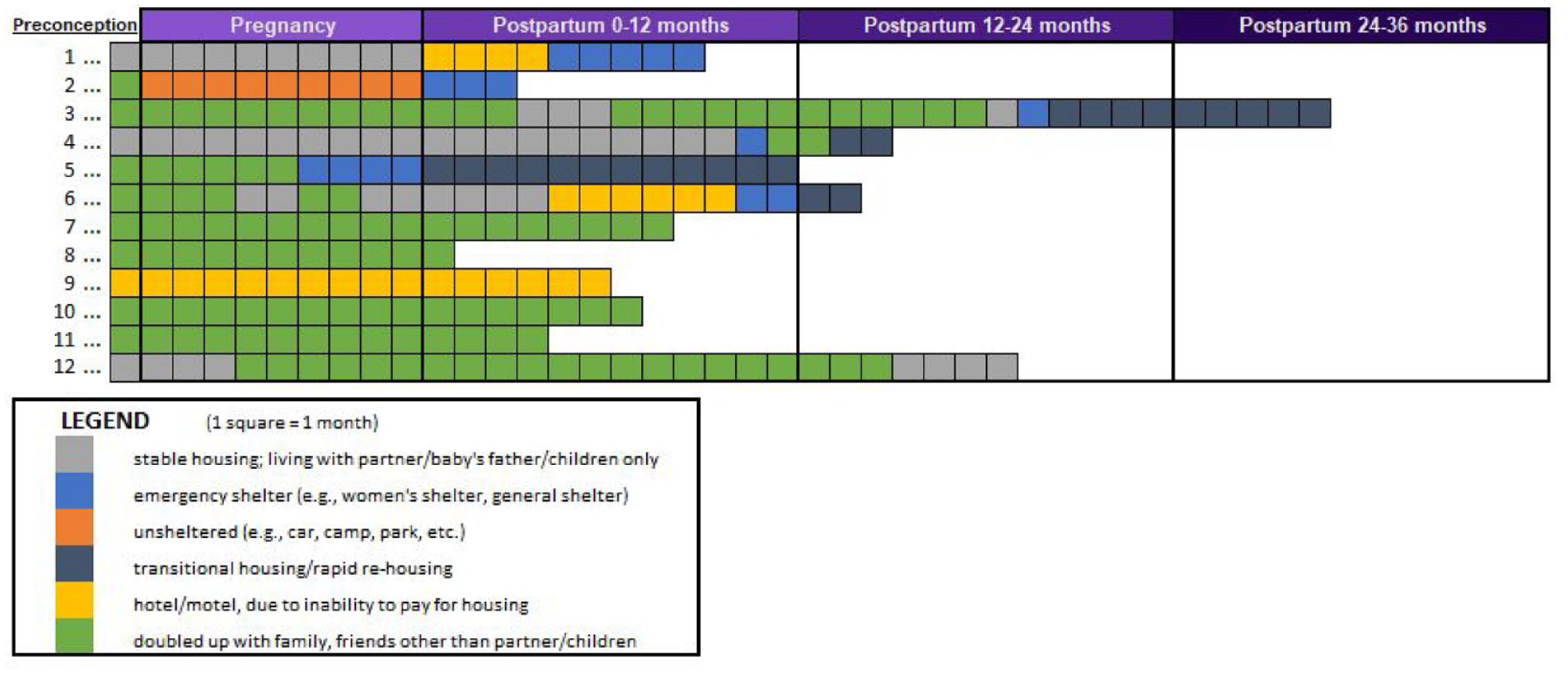
Perinatal Homelessness, by Type and Duration Among Participating Women Recently Pregnant and Homeless (n = 12), 2022.
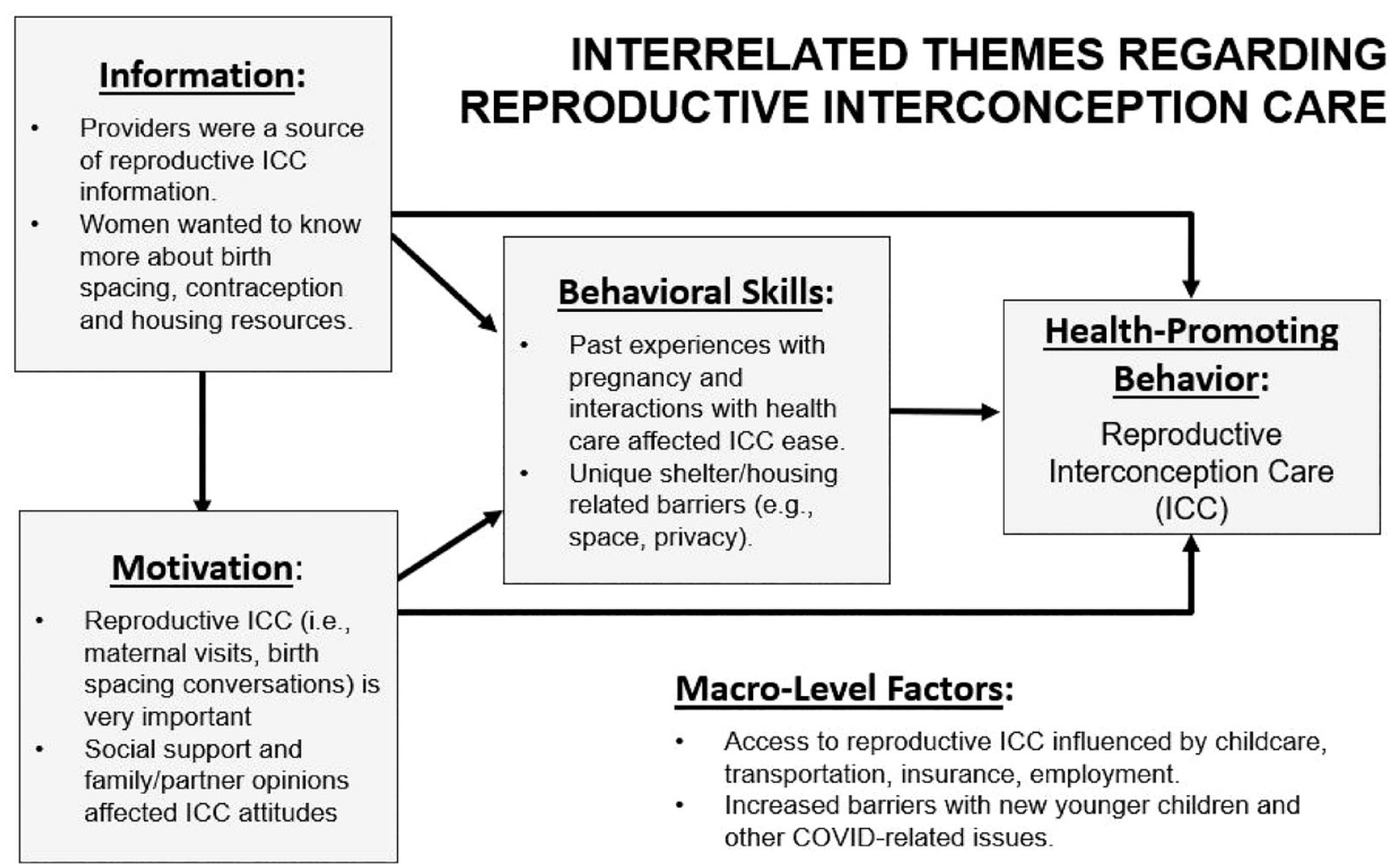
Interrelated Themes Regarding Reproductive Interconception Care.
Information
Questions related to maternal postpartum visits and birth intervals yielded overlapping themes. Information themes focused on what participants learned and what they would like to have learned more about from their postpartum visit providers. Maternal postpartum visit information was also discussed in the context of how their providers delivered the information during this visit and whether the information was consistent (e.g., recommended birth interval spacing). Women wanted to learn more about other topics like birth intervals and contraception, resources for obtaining birth control, resources for housing, and resources for healthy relationships. One participant who had recently experienced intimate partner violence stated, Also, just knowing how to have a healthy household, for sure. Because a lot of women are not in one, and they stay in bad situations, and then the kids are affected. And it doesn’t matter how old they are, they can still be babies and be affected by domestic violence and stuff. (woman—multiparous, transitional housing)
Despite these desires to learn more, the limited time of the appointment and emphasis on other priorities made these conversations seem less important to the providers. Another woman knew about reproductive ICC topics but was surprised her OB-GYN did not ask or confirm what she knew.
I think she kind of gathered that I kind of knew a lot of the basics, a lot of the things. But I would’ve liked her to just kind of say it and me have to tell her, ‘I already know’ than to just kind of wonder if she does this with everyone, kind of deal.” (woman—multiparous, transitional housing)
While one participant who engaged in telehealth postpartum visits had an overall positive experience, she acknowledged that maintaining time and engagement was difficult.
Even when we would do the telehealth, it would be kind of just quick because I had my one-year-old and my newborn. So that really kind of put a . . . stressor on the ability to get the information or just kind of have the time . . . to really listen.” (woman—multiparous, transitional housing)
When asked about birth intervals, participants’ responses varied about the interval recommended for trying to get pregnant again (n = 4), how to use contraception to space out pregnancies (n = 2), and discussions about whether they wanted children in the future (n = 1). Some women said their providers told them to wait at least 6 months, until they were healed, at least 18–24 months, or to not have any more children at all. Some women said that their doctors did not discuss birth intervals at all (n = 4). One said, No, I didn’t get talked to about birth spacing. They just wanted me to get on something [a contraceptive] so I wouldn’t have three kids. (woman—multiparous, transitional housing)
Motivation
Most women found maternal postpartum visits and birth interval considerations very important. The majority found their maternal postpartum visit especially important, primarily to detect any abnormal bleeding, to address postpartum depression, or for guidance on Cesarean section care, healing, and body changes.
[The maternal postpartum visit]’s very important ‘cause you do, you want to make sure that things are going well. You want to make sure that you’re healing. . . .that’s when they actually go in and they look. You know, some people go back for their 6-week checkup, and they’re already back pregnant. (woman—multiparous, emergency shelter)
Although one woman said there was no reason not to go to maternal postpartum visits, others considered the visits a waste of time if they were doing well. For example, one said, [My postpartum health] didn’t bother me. I didn’t have to go see the doctor. I didn’t have no problems or nothing. I’m not a doctor person. If it’s not broken, I don’t go. I haven’t been to my primary care in 9, 8 years. (woman—multiparous, hotel)
A few women acknowledged that attending their postpartum visit was important, but they did not attend their postpartum visit because of scheduling difficulties.
I think it’s really important, but because I had a child before, I kind of stayed home more, just because I don’t, they always go up there and stuff, and it’s kind of painful . . .. I didn’t want to go anywhere, so I just kind of stayed home a lot. But it is important to go, especially if this is your first child, I would say. But I knew I was okay, so I kind of just stopped going because I was dealing with a lot housing-wise as well, but I know I should have gone back. And I know I still need to. (woman—multiparous, transitional housing)
Motivation themes included attitudes about birth intervals and becoming pregnant now, specifically regarding the perceived importance of elongating birth intervals (e.g., wanting more time with their current baby, more time for healing) and the optimal interval before having another child, ranging from 1 to 3 years. Most women said that spacing birth intervals was important in general, but it depended on the woman.
Being a first-time mom, I would rather have experiences with my kids. And not have kids back, back-to-back, and not even know what he likes or what if he gets mad about . . . I would want experiences with my son, he’s the first baby, and you know, the feeding and crying, and he’s already going to school, getting out of that space, that you know for the next one, you know you’re prepared for it. (woman—primiparous, doubled-up) Now, I think it’s based on your health and your finances and your level of support. Because I do see benefits of having them close, but it’s kind of like a teeter. It’s like a balancing scale. They might be close, but can you afford it? Do you have the patience for it? There’s pros and cons to all of it. (woman—multiparous, transitional housing)
Participants’ partners, family, and friends affected both their ability to attend maternal postpartum visits and the timing of the next pregnancy and pregnancy desire in general. Social factors included having a support system to help them take care of children or encourage them to make visits or relying on mothers, partners, and other family members to provide transportation. One woman reflected on the need for support, I feel like it should be everybody [should help with postpartum visits]. Everybody should call that’s your friends, everybody that’s a family member. I don’t think it should be anyone that should tell you no, don’t go see the doctor. (woman—multiparous, emergency shelter)
Birth interval social themes ranged from friends wanting to have children growing up together, mothers wanting more grandchildren, and partners wanting future children of a specific gender. Some women had families and partners who supported their decision about when to have another child, while others said that family’s and partners’ opinions did not influence them.
People are always . . . “When you get remarried . . .” They want you to have more, but I don’t want it anymore because I have two boys, and they want you to have a girl, and they always want you to have something else. First it was, “I want you to have a baby.” Now, “I want you to have four or five, six.” (laughs) At a certain point, you stop letting people do that to you. And you say no, enough is enough. (woman—multiparous, transitional housing)
Behavioral Skills
For behavioral skills regarding perceived self-efficacy, women reported that child care, social support, transportation, Medicaid, employment, appointment scheduling, past health care experiences, and the COVID-19 pandemic sequelae could make attending postpartum visits and delaying or spacing pregnancies difficult. While most women (n = 10) were able to attend maternal postpartum visits, child care during COVID-19 was a significant challenge.
Childcare has been a big thing, “cause especially right now with COVID, they don’t want kids coming into the hospitals or going into clinics, and that’s another thing that we kinda have to choose: okay, does [partner] have to take a whole day off just to watch the kids at the house, you know—or here. I think childcare would be so helpful, you know, for the—especially for doctors” appointments and stuff like that. (woman—multiparous, emergency shelter)
Regarding birth intervals, women said that wanting closer-aged children, pressure from family and partners for another child, wanting to be finished with all pregnancies, worrying about future fertility, and not wanting to change behavior made it harder to space out pregnancies.
Some moms that took forever to get pregnant, or they did IVF to get pregnant, then I’d say, “Hey, if you want another baby, you want to try so fast, go ahead because your body’s not going to just say yes all the time to go ahead and have a baby.” Sometimes, some women’s bodies are like, “Nope, your body’s not ready for a baby,” and that’s when some people have miscarriages. (woman—multiparous, doubled-up)
Macro-Level Factors
Regarding larger, macro-level themes, women noted several housing transitions across the perinatal period, to which they attributed uncertainty and difficulty in planning pregnancy and postpartum reproductive ICC. Other themes included wanting to get housing-ready first, having limited resources for another child, knowing more about short-birth-interval risks, not wanting to go through pregnancy again, and lacking help and social support during previous pregnancies made it easier to space out pregnancies.
Of course, I didn’t leave [my baby] with anybody, and this is kind of when COVID was going on, so a lot of daycares wasn’t opening, so I was kind of off-and-on with jobs. And, you know, I think I’m doing good, and OK, well I’m gonna try to go find somewhere to stay. OK well, when I move, will I still have the help? Well, I feel it just, it is. It’s been frustrating, you know. (woman—multiparous, emergency shelter) Yeah. I think men just feel like they just don’t understand how much it comes with. And especially, even when I was with, he was adamant, he was low-key trying to have another kid, he was even talking about it. I was like, “Why do you want another kid when you can’t even take care of these two?” It just doesn’t make sense. (woman—multiparous, transitional housing)
Discussion
This study identified barriers and facilitators to obtaining reproductive ICC among women recently pregnant and homeless. Based on this sample’s perceived risks, social support networks, available resources, and access to reproductive ICC, interventions should seek to be comprehensive and reproductively just, involving women to make autonomous decisions. Information themes related to navigating housing with other children amid intimate partner violence demonstrate the importance of holistic services that will better support beneficial reproductive decision-making (Chan et al., 2021). Traumatic birth experiences and other perinatal trauma were shown to inhibit reproductive care outcomes in this study as well as another qualitative study investigating perinatal care perceptions among women experiencing homelessness (Gordon et al., 2019). There may be a need and potential opportunity to build more congruence from ambivalence by determining whether a woman experiencing homelessness wants to attend postpartum visits, elongate subsequent births, or prevent pregnancy despite perceiving these ICC behaviors as important.
Clinicians and community health educators have opportunities to have open, acceptable family planning conversations tailored to the preferences and experiences of each woman. Women in this study lamented the timeframe when education was offered, preferring instead to receive education prenatally and potentially in a follow-up after the initial postpartum appointment. Some women who did attend visits felt rushed and unable to ask questions. Standardized guidelines from national organizations are imperative to support providers in comprehensive assessment and ensuring all content is sufficiently covered (Randel, 2019; Tully et al., 2017; Wilkes, 2016). As one interviewed woman praised the availability of telehealth during her most recent postpartum visit, other studies have shown the acceptability and feasibility of using mHeatlh programs for populations similar to postpartum women experiencing homelessness (Byrnes, 2016; McInnes et al., 2013). Even with evidence-based guidelines, implementing policies within clinics, especially among those who may not have sufficient resources or those who serve low-income or homeless populations, may be challenging.
In the current study, women preferred having earlier and additional follow-up conversations about ICC, which suggests potential benefits of screening for maternal health risks via assessing pregnancy desires and risks at every health encounter and setting possible (Frayne, 2017). This is especially important for women experiencing homelessness, who may delay or skip postpartum visits and contraceptive services due to competing priorities and a lack of streamlined services (Azarmehr et al., 2018; Cutts et al., 2015; Ovrebo et al., 1994).
Most women interviewed had Medicaid and suggested that their insurance coverage was critical for ICC and contraceptive services; thus, policies related to Medicaid coverage expansion and health care affordability should be considered. Safety net programs like the Healthy Texas Women program may help women experiencing homelessness, who typically qualify as low-income (204.2% of the federal poverty level), to receive free family planning, reproductive health, and women’s health screening services. Women in this study also noted confusion regarding Medicaid coverage, what services were covered, and how long she or her child was covered during this period. Larger local, state, and national policies focusing on housing reform, expansion of Medicaid and reproductive health care access, and additional welfare-related and poverty-alleviation supports for families should also be re-evaluated to reduce complexity, streamline care provision, and prevent additional deleterious effects of child rearing in unstable environments, during additional unintended pregnancy, and to improve maternal wellbeing and self-actualization.
Strengths and Limitations
Health care clinicians, community partners, and policy-makers can build on these findings to reduce barriers to attending maternal postpartum visits and improve supportive reproductive health outcomes. While the findings align with previous reproductive interconception findings (Galvin et al., in press), this study did not capture all forms of ICC. Although the strategy of recruiting women through community organizations facilitated data collection, women connected to these service organizations were more likely to have more resources than those who are harder to recruit and who may have additional insights that were not captured. The demographic survey data would require additional studies with larger samples to establish in-group differences. However, the sample size was appropriate for the study’s overall preliminary scope (Guest et al., 2006; Hennink & Kaiser, 2022). Based on eligibility criteria and sampling, the findings may not be generalizable to women who had different birth experiences outside of live birth (e.g., stillbirth, miscarriage, or abortion) or trans or non-gender binary persons (who met eligibility criteria but were not recruited during this study). Since eligibility criteria included women with children under the age of 4 years, some recall bias may have been introduced, especially for women beyond 1-year postpartum, who may be less able to recall attending early postpartum visits and engaging in reproductive care than women who are recently postpartum. However, because this study focused on these broader experiences versus comparative differences, the interpretation of findings is likely still appropriate.
Implications for Theory, Policy, and Practice
This article identified barriers and facilitators related to ICC information, motivation, behavioral skills, and other macro-level factors among women experiencing homelessness. The findings may also strengthen current ICC practices and augment reductions in unintended pregnancy. Providers must consider how ICC and postpartum care are provided, inclusive of women who do not want future children or cannot have children, given the tendency for health promotion during similar time periods like preconception to demonstrate gender bias (Thompson et al., 2017). Patient-centered, community-engaged health education can impact women experiencing homelessness, through personalized health conversations about the patient’s most pertinent social health determinants (Nelipovich et al., 2022). Ultimately, understanding reproductive ICC factors from the perspective of women experiencing homelessness can help inform reproductively equitable ICC services to help women experiencing homelessness make positive reproductive decisions throughout their life course.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the University of North Texas Health Science Center School of Public Health Dissertation Support fund.