
Abstract

Moral injury has been defined as the combined psychological, social, and spiritual impact of events involving violation of personal moral beliefs and values, especially in high-stress situations. 1 For centuries, this phenomenon has been experienced by military service members who perpetrated, witnessed, or failed to prevent acts that transgressed their own moral values or code of conduct. Examples include causing the deaths of civilians, following illegal or immoral orders, or failing to provide needed medical assistance. General mechanisms of moral injury include acts of commission, acts of omission, and betrayal. 2
At the individual level, moral injury may manifest as a crisis of conscience: feelings of guilt, shame, disgust, anger, and inability to forgive oneself. Commonly associated maladaptive coping behaviors include increased alcohol or substance use, aggressive behavior, and social isolation. 3 While moral injury is not yet recognized as a distinct diagnosis in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), 4 in the context of posttraumatic stress disorder (PTSD), DSM-5 does refer to exposure to details of trauma in the course of professional duties among medical and nonmedical first responders. Moral injury overlaps with PTSD in its clinical presentation but may be recognized separately from or in combination with PTSD and other related conditions, including adjustment disorders, depression, and burnout. 5 Biological mechanisms underlying PTSD and moral injury appear to differ. 6 Key distinctions exist between PTSD and moral injury, but behavioral symptomatology is shared (Figure). 7
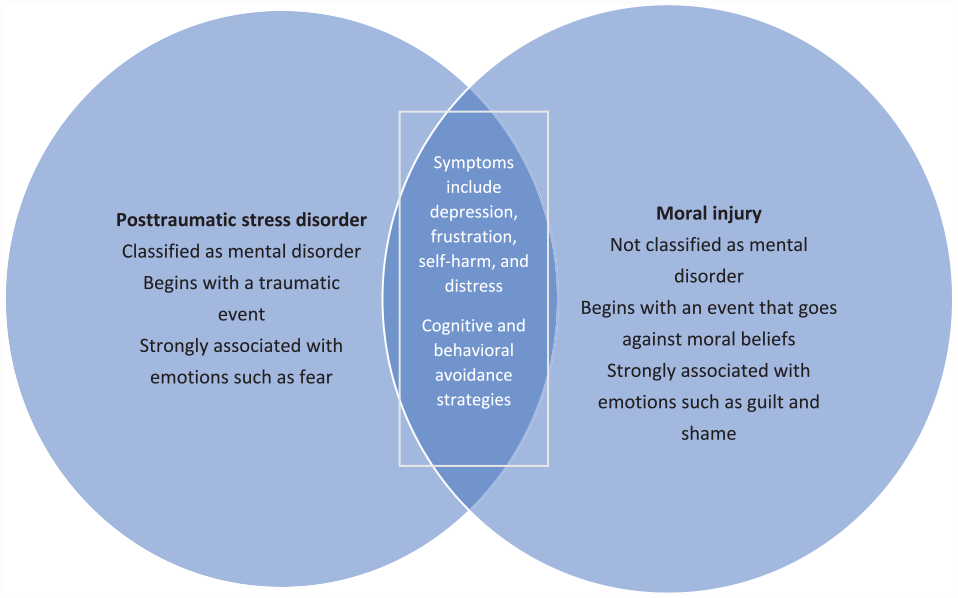
Posttraumatic stress disorder and moral injury: differences and similarities. Modified from moral injury in child exploitation investigators. 7
The existing literature on moral injury among health care workers, in terms of authorship and target audience, primarily addresses the moral injury experienced by physicians8,9 and nurses10,11 serving in clinical roles rather than public health workers. The COVID-19 pandemic has clearly demonstrated that moral injury can be experienced by frontline public health responders, most of whom do not work in traditional clinical roles.
In the context of the COVID-19 pandemic, moral injury must be viewed not solely from the individual point of view but in terms of public health. Both the pandemic itself 12 and coincident large-scale social movements 13 have resulted in an increased occurrence of moral injury. Writing from our perspective as active-duty United States Public Health Service (PHS) officers who deployed during the pandemic, we describe in this commentary risk and contextual factors associated with moral injury among PHS first responders during the pandemic and propose a set of mitigation strategies that can provide a path toward individual and collective healing for public health first responders at large.
Discussion: PHS First Responders and Risks for Moral Injury
The PHS, led by the US Surgeon General and organizationally part of the US Department of Health and Human Services (HHS), is one of 8 uniformed services. At a force strength of more than 6000, it is one of the smallest. While the PHS is not routinely militarized, it is subject to military principles, including the need to deploy, follow orders, and obey the chain of command. PHS officers include physicians, nurses, pharmacists, therapists, and other clinical providers, as well as scientists and other nonclinical professionals working in health-related fields. This latter category includes health scientists, laboratory technicians, and informaticians. Approximately 10% of PHS officers are physicians. 14 The PHS mission to protect, promote, and advance health and safety nationally and globally includes both clinical and scientific support for numerous federal agencies, including many outside HHS, 15 and deployment for diverse public health emergencies ranging from disease epidemics to natural disasters to large-scale migration-related events. 16 The beliefs and values of the PHS encompass an Oath of Office that indicates officers are required to serve wherever and whenever required, additional profession-specific oaths (eg, the Hippocratic Oath or the Florence Nightingale Pledge), and core values of leadership, service, integrity, and excellence.
The uniformed service members of the PHS have been deployed as frontline workers to provide both essential clinical and public health services throughout the pandemic, in settings including long-term care and temporary medical facilities. PHS officers have been deployed repeatedly; nearly 4000 officers—two-thirds of the total force—deployed nationally or internationally within the first 5 months of the pandemic. Officers provided direct care or public health support (including testing, infection control, and investigation of transmission) at long-term care facilities in Washington State; convention center–based hospitals in New York City, Michigan, and Washington, DC; and in Indian Health Service and Bureau of Prison facilities. 17 PHS officers also worked in conventional settings such as hospitals, providing direct clinical services at times when facilities were overwhelmed with COVID-19 patients. 18
Because of the potential for increased exposure to death and suffering in either combat or health care settings, being a uniformed service member or a frontline health worker confers an increased risk for moral injury. PHS officers fall into both of these high-risk categories for moral injury, and this risk is further exacerbated by working on the frontlines during a global pandemic. These frontline in-person responses by both clinical and nonclinical staff have created the opportunity for acts of commission that can contribute to moral injury, including inadvertently spreading COVID-19 infection. Early in the pandemic, inadvertent spread may have occurred due to inadequate supplies of personal protective equipment or incomplete knowledge of mechanisms of viral transmission. The early pandemic period in 2020 was also characterized by a lack of preventive and treatment interventions, contributing to responder feelings of frustration and powerlessness. Undoubtedly more important during the pandemic as a risk factor for moral injury are acts of omission (eg, the inability to treat or attend to all COVID-19 patients because of lack of resources and attrition of the health care workforce related to both staffing shortages and COVID-19–related absences caused by illness, isolation, or quarantine). For nonclinical personnel who were also subject to staffing shortages, acts of omission included the inability to investigate all reported COVID-19 outbreaks and the need to make difficult choices about which high-risk transmission settings (eg, jails, prisons, high-density work settings) could receive specific risk mitigation guidance or in-person visits and which could not. Such omissions may be especially injurious to public health personnel, for whom pursuing health equity is a core professional value.
Betrayal as a mechanism of moral injury has been exacerbated during the pandemic by implementation of crisis standards of care. 19 The enactment of such standards makes more explicit the idea that care must sometimes be rationed and that care providers are expected to do the rationing. This rationing of care may trigger moral injury, as it runs counter to frameworks of ethics adopted by the health professions that compose the PHS.20,21 Officers and other frontline public health responders may also experience a sense of betrayal when they directly or indirectly experience anger and hostility directed toward public health and health care professionals. Fueled by misinformation and well-captured through the media, the COVID-19 pandemic engendered widespread antipathy, including death threats and violence directed toward public health providers. 22
In addition to experiencing general issues of commission, omission, and betrayal, PHS officers are subject to role-specific circumstances that may fuel moral injury. When attempting to adhere to professional roles and standards (eg, their Oath of Service and/or professional oath) conflicts with the need to follow orders in support of a mission, individual moral distress results. PHS officer responders have little input into policy or operational details when they deploy, and because such assignments typically last only up to 4 weeks, the ability to follow up on individual patient or community outcomes is limited. Officers on deployment, especially to long-term care facilities, frequently experienced deaths of patients coupled with a perception that there was little they could do to help. While in the field, officers may experience guilt about not fulfilling important work functions of their permanent jobs. Repeated and sometimes consecutive deployments with limited recovery time in between (“dwell time”) may exacerbate this feeling of lack of professional agency. Short but frequent deployments may result in increased personal and family stress, with little or no time to adjust back to normal life routines and less time to transition between deployed and nondeployed professional roles. While these risk factors of lack of continuity of care and repeated deployments are not unique to PHS officers, they distinguish them from most health care workers who may work at a single facility or in a limited geographic area.
While PHS deployments may have often provided a needed respite for frontline clinical workers (ie, officers serving as temporary replacements for nurses and other full-time clinical roles), the need for responders themselves to have respite care has rarely been acknowledged. Secondary or delayed impacts of moral injury can also occur after deployments, in which responders see their actions or motives publicly questioned, second-guessed, or even found professionally lacking. 23 Such after-the-fact criticism is another face of the betrayal mechanism of moral injury.
Public Health Implications: Strategies to Address Moral Injury Among the Public Health Workforce
Given the COVID-19 pandemic’s enormous contributions to moral injury among public health first responders, leaders at all government levels of public health must seek to understand this form of psychological trauma in the context of public health work and be willing to openly discuss it with their workforce. This understanding begins with acknowledging the issue’s existence and seeking to gain nonjudgmental insight into its scope and factors contributing to it through the use of questionnaires or other confidential survey instruments. PHS officers, because they have worked extensively in both clinical and nonclinical roles during the pandemic, may be important sources of data and insights on the triggers and consequences of moral injury.
Other parts of the solution include incorporating information on moral injury into both scheduled and just-in-time training prior to or during deployments. Deployment teams and their leadership should be proactively briefed on deployment stressors and potentially morally injurious events (eg, if deploying to settings that have implemented crisis standards of care), identify deployment support groups, and employ evidence-based stress management teams. 24 While care needs to be taken not to relive or trigger traumatic memories, trauma-informed care for people who have experienced moral injury must be made available in individual or group settings. Individuals in need of mental or behavioral health services as a result of moral injury should have access to care without fear of reprisal or adverse professional consequences.
Existing mental health resources for deployed PHS officers 25 should be supported and enhanced. Unlike members of other services, PHS officers, most of whom are assigned outside the US Department of Defense, do not have access to chaplains. Exploring options for wider availability of this resource, which has shown qualitative benefits in uniformed service settings, could expand access to and decrease the stigma of seeking assistance for moral injury and frequent comorbid conditions, including depression and burnout. 26 We acknowledge that interventional research on psychological health outcomes among public health professionals is limited. However, given data showing extensive mental health symptoms among COVID-19 public health responders 27 and positive process evaluations for interventions targeting the moral distress of health workers, 28 we call for practice-based evidence, focused on the public health community, related to the interventions we recommend. Perceived loss of control is an important component of moral injury and could be addressed after deployment through enforcing minimum dwell time requirements, supporting officers to develop family contingency plans, and facilitating ready availability of mental health resources.
Moral injury can be experienced by all public health responders through the shared mechanisms of commission, omission, and betrayal. Broader understanding of the scope and nature of moral injury among public health workers is needed, especially at nonfederal levels in the United States, where most public health professionals are employed. Calls for investments in public health recruitment and retention should include increased supports for public health responders.29,30
We recognize that not all of these proposed strategies are appropriate or feasible in other federal systems or at state, local, territorial, or tribal levels. However, leadership engagement, seeking quantitative or qualitative inputs from workers to develop evidence-informed policies, and promoting trauma-informed care are not service-specific recommendations, and they can form the bedrock of the path by which public health–focused organizations can begin to heal the moral injury of the public health workforce.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.