
Abstract
Objective:
Understanding the challenges public health workers have faced is critical to reinforcing, revitalizing, and strengthening the public health workforce. We measured and identified the level and causes of psychological distress among public health workers during the COVID-19 pandemic in New York State.
Methods:
We used a knowledge, attitudes, beliefs, and behaviors survey to ask public health workers at local health departments about their experiences working in public health during the pandemic, including questions relating to harassment from the public, workload, and work/life balance. We used the Kessler-6 scale to measure participants’ psychological distress using a 5-point Likert scale, with higher scores indicating greater psychological distress. We calculated descriptive statistics and conducted a regression analysis to determine the factors associated with public health worker psychological distress, and we coded open-ended comments for qualitative analysis.
Results:
During September 7-20, 2021, 231 public health workers from 38 local health departments completed the survey. Respondents were predominantly non-Hispanic White (89.6%), female (82.1%), full-time employees (95.1%), and located in Upstate New York. On a bivariate level, the strongest predictor of distress was job satisfaction (–0.388), followed closely by COVID-19 fatigue (0.386) and feeling bullied or harassed by the public (0.331). In the regression analysis, 2 additional factors were associated with distress: considering leaving their job due to the pandemic and concerns about exposure. Themes from the qualitative analysis strongly supported these findings.
Conclusions:
Understanding the challenges public health workers have faced during the pandemic is critical to inform the actions needed—stronger state laws protecting against harassment, workforce incentives, and commensurate funding—to reinforce and revitalize our frontline public health workforce.
The impact of the COVID-19 pandemic far exceeds the physical health of those infected. It has eroded individuals’ mental health, particularly those providing essential services on the frontlines.1-3 This increase in psychological distress, especially among patient-facing health care workers, is well defined in the literature.4,5 Although health departments have led the public health response in mitigating the pandemic, few studies in the United States have explored the effects of COVID-19 on the mental health of public health workers (PHWs).
In New York State, local health departments (LHDs) are responsible for responding to disease outbreaks, enforcing public health measures, and issuing county health orders to protect the health of their communities. 6 During the COVID-19 pandemic, LHDs in New York State have conducted case investigations and contact tracing, enforced isolation/quarantine orders, and established testing and vaccine clinics. They have worked to keep their communities informed as the pandemic has evolved, with guidance and collaboration from the New York State Department of Health (NYSDOH) and the Centers for Disease Control and Prevention. 6
These efforts have been met with substantial challenges, including public criticism and backlash. 7 PHWs have experienced publication of private information, angry and armed protesters at their homes, death threats, vandalism, and harassing telephone calls and social media posts.8-11 The impact of these attacks, as well as the pandemic-related strain of overwork, on the health and well-being of this workforce is slowly being recognized.
A 2021 survey of 26 174 regional and local PHWs revealed that 53% had symptoms of at least 1 mental illness, including depression (30.8%), anxiety (30.3%), posttraumatic stress disorder (36.8%), and suicidal ideation (8.4%). 12 Respondents who were aged <29 years, identified as transgender or gender-diverse, and worked ≥41 hours per week reported the highest symptom prevalence. Symptom severity increased with time dedicated to the COVID-19 response. 12 Another national survey of PHWs (n = 44 732) found that 56% reported ≥1 symptom of posttraumatic stress disorder and 22% described their mental health as fair or poor. 13
Researchers have attributed the stress and struggles of PHWs during the COVID-19 pandemic to problems that predate the pandemic. Public health has been chronically underfunded, 14 constituting only 3% of US health care expenditures. 15 A National Association of County & City Health Officials research brief noted that, in 2019, most LHDs (67%) experienced flat funding, with either stagnant (52%) or reduced (15%) budgets, despite inflation, population growth, and prepandemic public health challenges. 16 In New York State, from 2011 to 2015, state-allocated funding for LHDs decreased by 40%. 17
US LHDs are substantially understaffed, staffing 153 000 workers in 2022, compared with 184 000 before the 2008 recession.15,18 Gaps in critical roles are common, especially in rural areas. 15 In New York State, the LHD workforce outside New York City decreased by 33% from 2011 to 2017. 17
The pandemic has exacerbated funding and workforce shortages. In the United States, hundreds of PHWs have left their positions.8,19-22 In a cross-sectional survey of 225 PHWs in August 2020, 66% reported burnout. Compared with their January 2020 plans, in August 2020, 24% fewer respondents planned to still be working in public health for ≥3 years. 23 A 2021 qualitative study of the experiences of state and local PHWs concluded that constrained hiring capacity and burnout were key intertwined themes. 24 Staffing shortages have intensified the workload among PHWs, who have had to balance the pandemic response with their essential public health functions, despite these functions being limited during the pandemic. 25 These shortages have led to substantial overtime that has negatively affected the mental health of PHWs. 24
Understanding the challenges PHWs have faced is critical to reinforcing, revitalizing, and strengthening the public health workforce. The objective of this study was to measure the level and identify the causes of psychological distress during the COVID-19 pandemic among PHWs in New York State.
Methods
In September 2021, we partnered with the New York State Association of County Health Officials to survey PHWs in New York State. We modified the knowledge, attitudes, beliefs, and behavior survey, designed to measure the relationship between behavior and mental health during the COVID-19 pandemic, 26 for PHWs to include questions on pandemic-related interactions with the public. The New York State Association of County Health Officials emailed the invitation 3 times to 160 officials at 58 LHDs in New York State. Recipients were asked to complete the survey and forward it to their employees. During September 7-20, 2021, PHWs consented and completed the survey via Qualtrics. The study was approved by the State University of New York Oneonta Institutional Review Board (STUDY00002542, MOD00001627).
Survey Elements
We used the 6-item version of the Kessler Psychological Distress Scale to measure psychological distress among respondents. 27 Each question began with, “During the past 30 days, how often did you feel . . .” to assess the frequency with which respondents perceived the following 6 indicators: “nervous,” “hopeless,” “restless or fidgety,” “so depressed that nothing could cheer you up,” “that everything was an effort,” and “worthless.” Responses for each item were on a 5-point Likert scale, where 0 = never, 1 = rarely, 2 = sometimes, 3 = often, and 4 = almost always; higher composite scores indicate higher levels of distress. This scale is valid in US and international contexts.28,29
We measured job satisfaction using a series of statements from the Utrecht Work Engagement Scale 30 that were rated by respondents on a 7-point scale, from never (0) to always (6). Statements included: “At my job, I feel strong and vigorous; I am enthusiastic about my job; My job inspires me; When I get up in the morning, I feel like going to work; I feel happy when I am working intensely; I am proud of the work that I do; I am immersed in my work; and I get carried away when I’m working.”
We measured COVID-19 fatigue using a series of statements derived with minimal modification from the 6-item HIV Prevention Fatigue Scale. 31 These statements were: “I am burned out thinking about COVID-19; I am less careful about avoiding COVID-19 today because I am tired of being safe; I have heard so much about COVID-19 that I often tune out messages about it; I do not want to hear any more about COVID-19; Sometimes I do things where I might get COVID-19 because I am tired of being careful; and COVID-19 is really not my problem, it’s somebody else’s.” We used a 4-point Likert scale in which 1 = strongly disagree, 2 = mildly disagree, 3 = mildly agree, and 4 = strongly agree.
We determined whether respondents were bullied or harassed by asking a simple yes/no question: “During the past year, have you felt bullied or harassed because of work by members of the public (clients and/or community members)?”
We determined whether respondents were worried about exposure to COVID-19 at work and considered leaving their job as a result of the pandemic by asking the following yes/no question: “During the past year, which of the following has happened personally to you?” with 2 scenarios, “Worried about workplace exposure to COVID-19” and “Considered leaving my job as a result of the pandemic.”
Quantitative Analysis
PHWs responded to survey questions with closed-ended responses. The dependent variable, the Kessler-6 scale, combines 6 areas of distress into a single index. 28 The independent variables included items that measured the extent to which PHWs felt bullied or harassed, worried about exposure, or considered leaving their job. Job satisfaction and COVID-19 fatigue indices were included given their relevance to the research questions.
Ordinary least squares (OLS) regression analysis provides a method for examining the prediction of the dependent variable as a function of several independent variables, while controlling for other variables in the model. Per convention, we considered α = .05 to be significant. The unstandardized coefficients indicate the effect of each variable on the overall predicted Kessler-6 score.
Qualitative Analysis
PHWs were presented with an open-ended question at the end of the survey: “Please feel free to share your experiences with the researchers here.” Two researchers (E.L., E.S.), using ATLAS.ti 8 and NVivo, conducted inductive coding to pre-identify a code list. We then coded all responses independently. Analytic memos were written on the major themes that emerged from reviewing the coded data.
Results
Of 58 LHDs surveyed, 38 (65%) responded and 231 PHWs completed the survey. Because of the methodology, we could not calculate a precise rate of return for PHWs. Only 1 respondent was from New York City.
Quantitative Analysis
PHWs in the sample were predominantly non-Hispanic White (n = 198, 85.7%), were female (n = 183, 79.2%), were working full-time (n = 212, 91.8%), and had a bachelor’s degree (n = 95, 41.1%) (Table 1).
Demographic characteristics of public health workers (n = 231) at 38 local health departments in a survey on psychological distress during the COVID-19 pandemic, New York State, September 2021
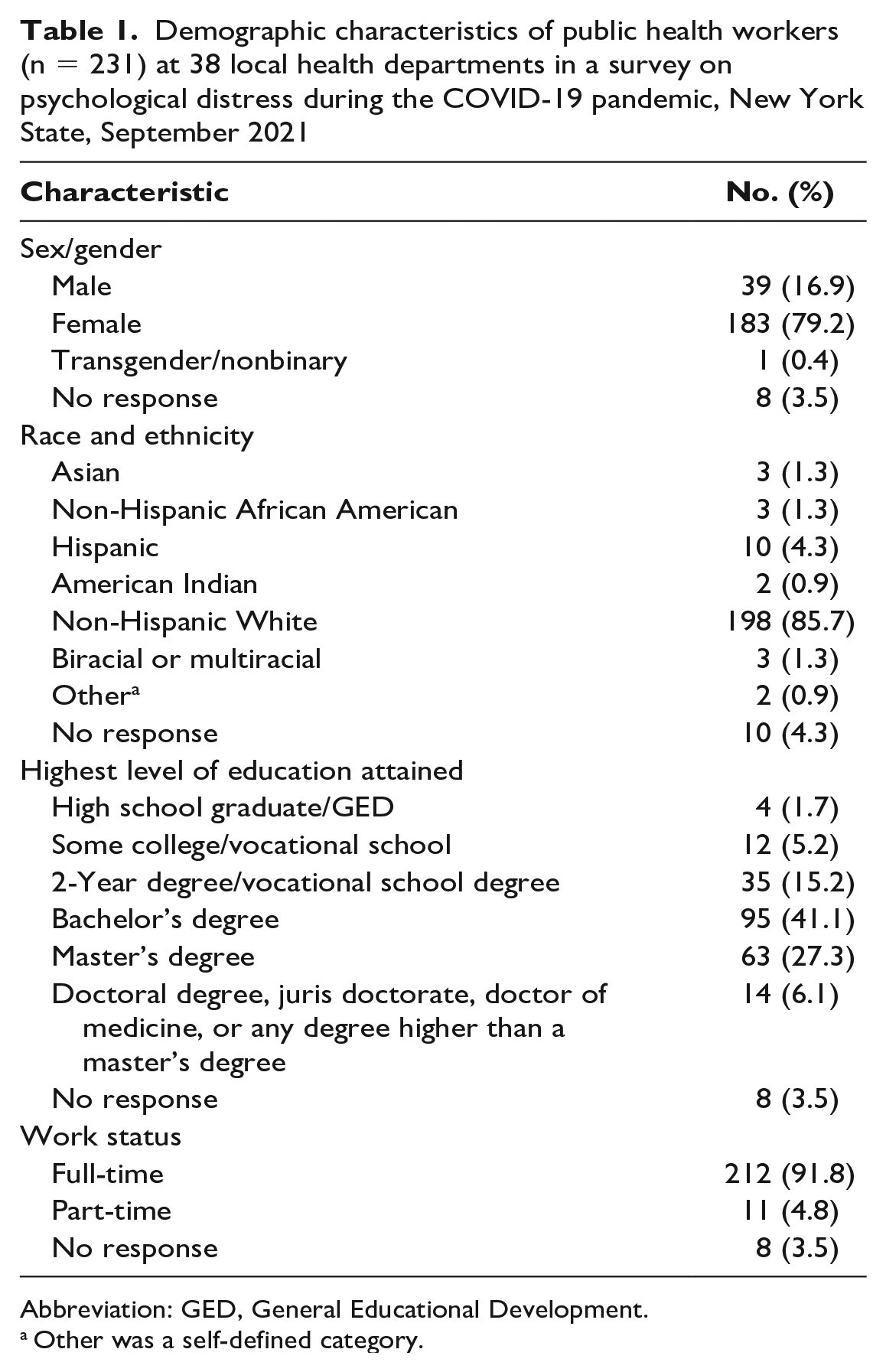
Abbreviation: GED, General Educational Development.
Other was a self-defined category.
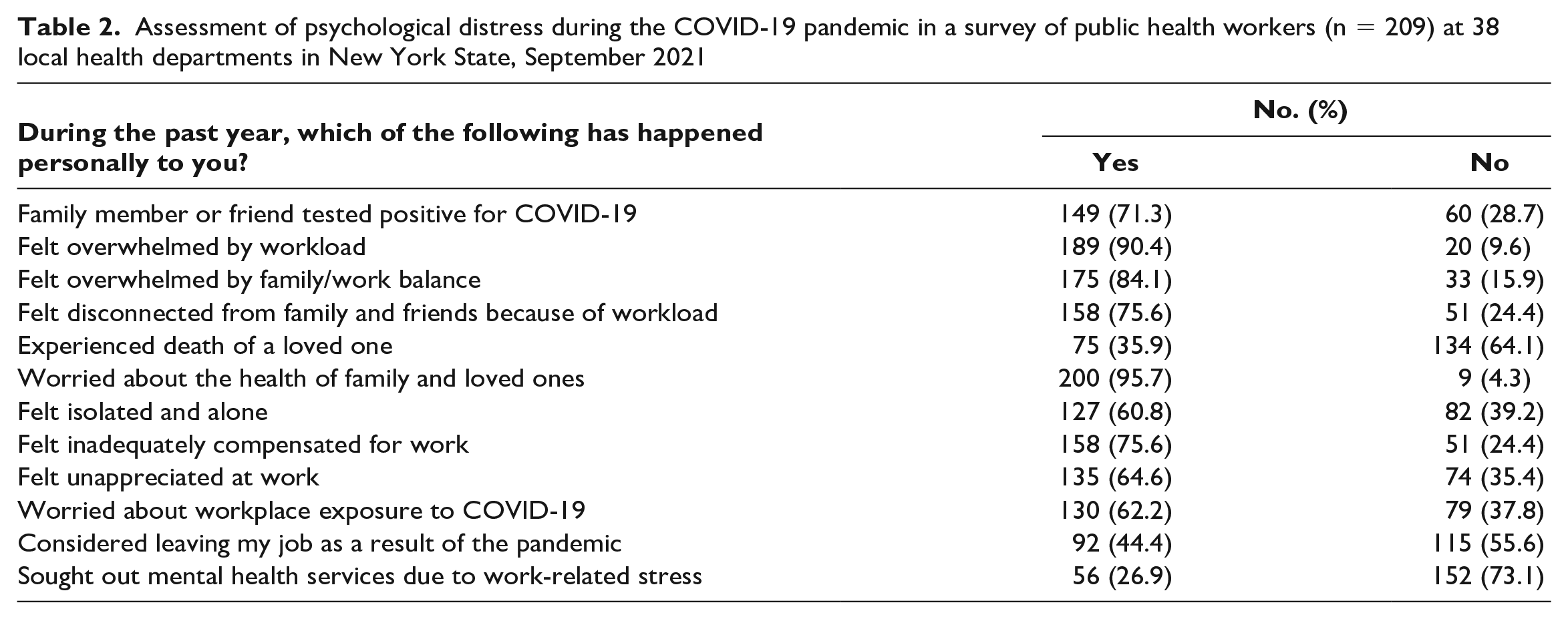
When asked about their experiences during the past year, most PHWs said they felt overwhelmed by their workload (189 of 209, 90.4%) and by family/work balance (175 of 208, 84.1%), isolated and alone (127 of 209, 60.8%), unappreciated at work (135 of 209, 64.6%), and inadequately compensated for work (158 of 209, 75.6%) (Table 2). Many PHWs had considered leaving their job because of the pandemic (92 of 207, 44.4%) or seeking mental health services due to work-related stress (56 of 208, 26.9%).
Assessment of psychological distress during the COVID-19 pandemic in a survey of public health workers (n = 209) at 38 local health departments in New York State, September 2021
According to Kessler-6 scores, the strongest predictor of distress was job satisfaction (r = –0.388) followed by COVID-19 fatigue (0.386) and feeling bullied or harassed by the public (0.331) (Table 3).
Pearson bivariate correlation matrix from an assessment of psychological distress during the COVID-19 pandemic in a survey of public health workers (n = 197) at 38 local health departments in New York State, September 2021
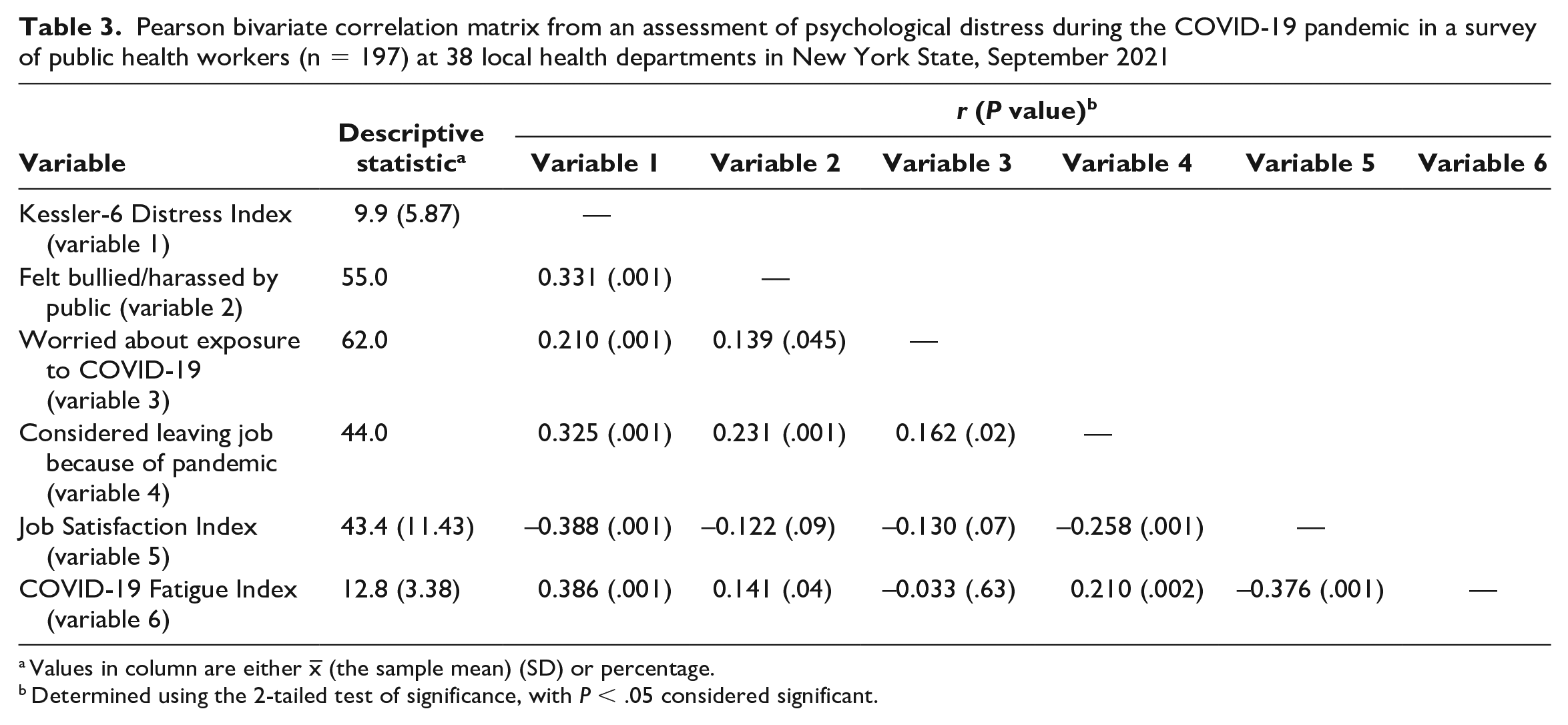
Values in column are either x– (the sample mean) (SD) or percentage.
Determined using the 2-tailed test of significance, with P < .05 considered significant.
Regression Model
In the (OLS) regression analysis predicting Kessler-6 Distress for PHWs, Model 1 was significant, per the F statistic, and explained about one-third of the variation (adjusted R 2 = 0.309) (Table 4). The model diagnostics did not reveal problems with multicollinearity.
Ordinary least squares regression predicting distress on the Kessler-6 Psychological Distress Scale during the COVID-19 pandemic among public health workers (n = 197) at 38 local health departments in New York State, September 2021
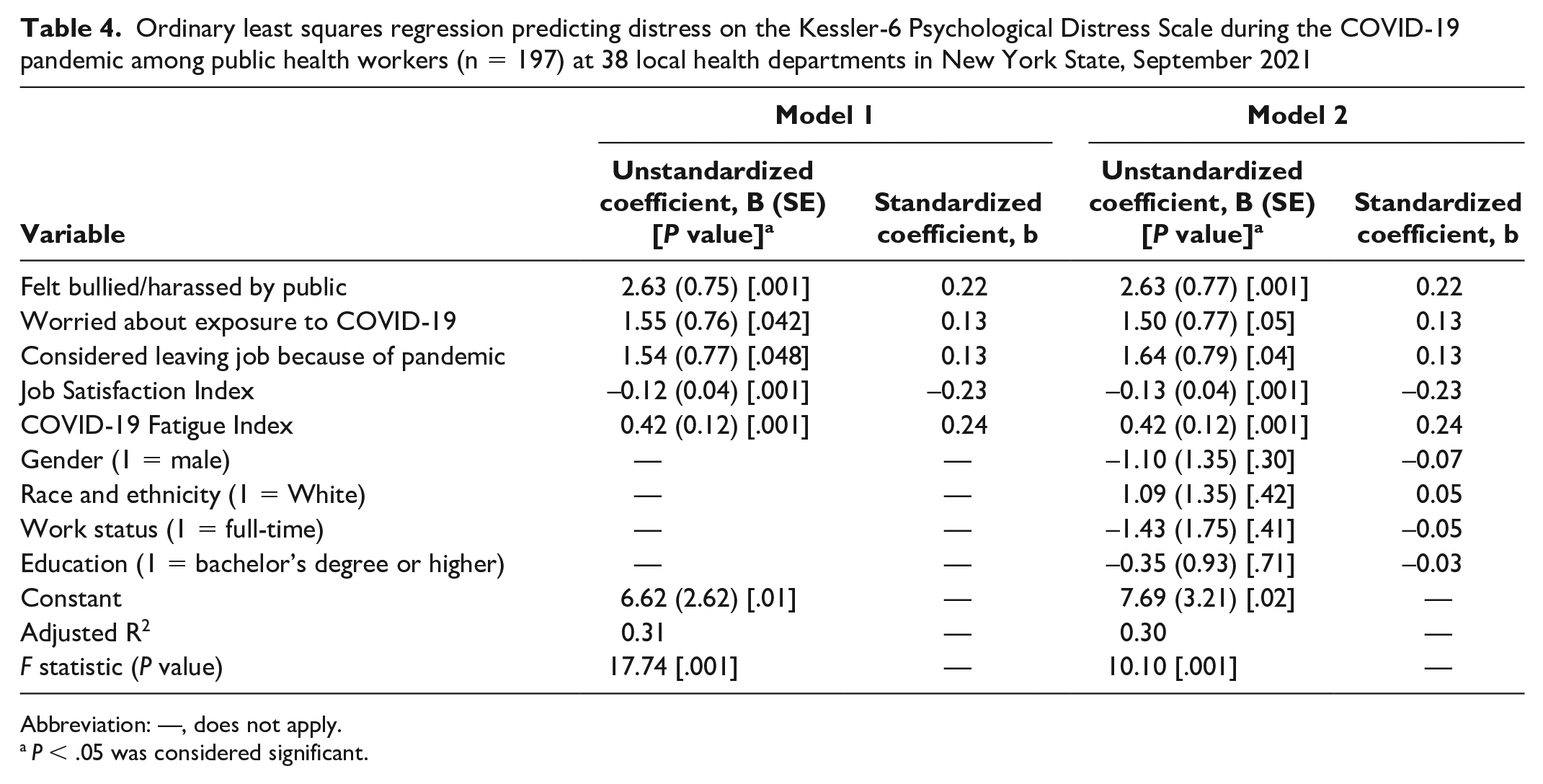
Abbreviation: —, does not apply.
P < .05 was considered significant.
The predictors in Model 1 were job satisfaction, COVID-19 fatigue, feeling bullied or harassed by the public in the past year, being worried about exposure to COVID-19 at work, and considering leaving their job because of the pandemic (Table 4). Each predictor was significant at the α = .05 level or better. For those who reported feeling bullied or harassed by the public in the past year, their predicted distress score increased by 2.6 points. Those who worried about being exposed to COVID-19 at work had a predicted distress score that was 1.6 points higher than those who did not.
If the respondent reported having considered leaving their job because of the pandemic, their predicted Kessler-6 score was 1.5 points higher than if they had not reported considering leaving their job (Table 4). For every 1-point increase in job satisfaction, the model predicted a decrease in the predicted distress score of 0.1. Finally, for every additional level of COVID-19 fatigue, the model predicted a corresponding increase in the Kessler-6 score of 0.4. In terms of the standardized coefficients, the best predictors of distress were COVID-19 fatigue, job satisfaction, and feeling bullied or harassed. The magnitude of these coefficients was consistent with the zero-order bivariate correlations noted previously. The main difference was for respondents who reported that they had considered leaving their job because of the pandemic—the zero-order correlation was higher than the OLS regression coefficient, suggesting that the other variables in the model accounted for some of the variation.
Model 2 includes the predictors from Model 1 along with demographic characteristics (sex/gender, race and ethnicity, education, and work status). While the F statistic in Model 2 was significant, the explained variation was slightly lower than in Model 1 (Table 4), suggesting that the addition of the demographic variables did not improve the explanatory power of the model. Reviewing the individual regression coefficients revealed these demographic variables were not significant.
Qualitative Analysis
Seventy-five respondents entered comments in the open-ended response to the statement, “Please feel free to share your experiences with the researchers here,” amounting to 8500 words. Respondents were able to enter text into an “other” category in response to questions about job-related hazards, producing 927 additional words. Key themes from the qualitative analysis supported the results of the quantitative analysis. Respondents frequently expressed frustration about how the work environment had changed because of the pandemic and the extreme burnout and exhaustion experienced (Table 5). Several PHWs expressed fears about an upcoming winter surge. Many PHWs elaborated on their stressful interactions with both the public and the state.
Key themes of written responses to an open-ended prompt in a survey of public health workers (n = 231) during the COVID-19 pandemic at 38 local health departments in New York State, September 2021
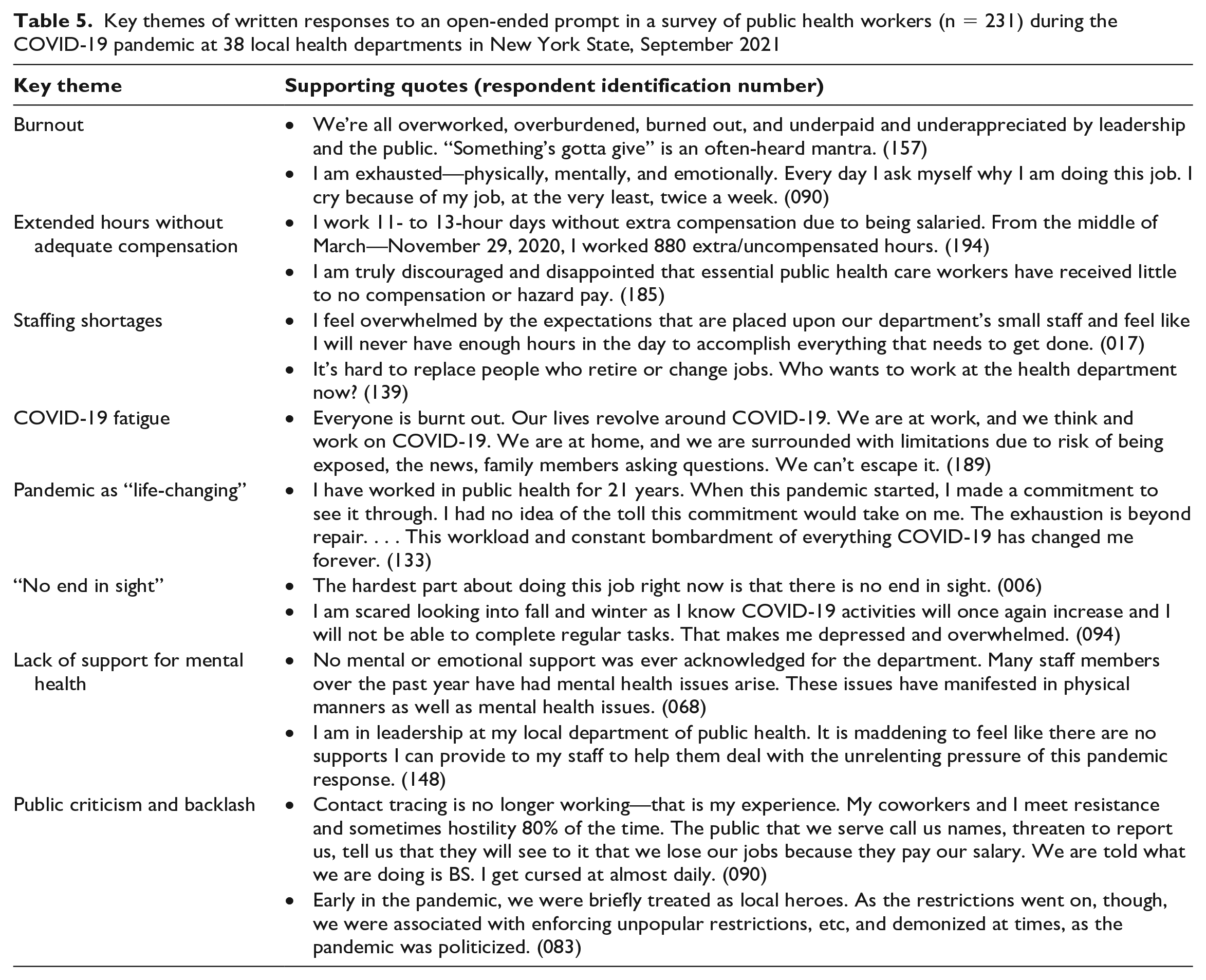
PHWs indicated they were hampered in their ability to respond to crisis because of state-level issues, including a lack of up-to-date guidance reflecting rapidly evolving pandemic mitigation strategies. PHWs at LHDs had to work within the local context and, thus, deal with sociopolitical forces in their counties that may oppose public health measures. At the same time, their authority and capacity derive from the state. Many felt their authority was undermined among local elements because of the state’s lack of communication and mixed messages leading to confusion about policy. Caught in the middle, PHWs became vulnerable. They expressed the need for adequate training, resources, experienced management, and support.
Discussion
The numerous factors associated with PHW psychological distress reflect the vast challenges facing our public health system, including workforce recruitment and retention, antipathy toward public health, a workforce that feels undervalued and overwhelmed, and restrictive funding streams. These challenges suggest that we are at the bottom of an uphill journey to revitalize the public health workforce.
Workforce Retention and Recruitment
Public health response largely depends on skilled PHWs who are tasked with protecting the health and safety of their communities. However, our findings indicate that 44% of study respondents had considered leaving their job in the past year. According to NYSDOH data, the number of full-time equivalents working on Article 6 services declined by 7% from 2015 to 2020 (NYSDOH, unpublished data, 2021), in part attributable to an aging workforce. Article 6 of the New York State Public Health Law requires counties to deliver the following 6 core services to receive state aid funding: family health; communicable disease; chronic disease; emergency preparedness/response; community health assessment; and, for 38 full-service LHDs, environmental health services. 32 In 2020, 25% of the LHD workforce in New York State was eligible to retire, with rural counties reporting a range of 20% to 50% (New York State Association of County Health Officials, unpublished data, 2020). Coupled with the challenges related to burnout, harassment, and fatigue, many PHWs are retiring earlier because of the pressures of the pandemic response, creating additional stressors for working PHWs.
LHDs nationally need approximately 54 000 new staff to provide adequate levels of public health services. 33 In New York State, more than 1000 additional full-time staff are needed to provide the same level of service. However, recruiting staff poses challenges. Only 17% of public health graduates are hired by governmental public health agencies after graduation. 34 To recruit and retain PHWs, policy makers and hiring agencies should offer competitive salaries, establish loan repayment/forgiveness programs, and promote policies that allow for a positive work/life balance, job security, retiree insurance, and benefits not offered by the private sector.
COVID-19 Fatigue and Concern About Exposure
Although the pandemic has made its way into every aspect of people’s lives, PHWs often have “no escape,” as a survey respondent indicated. Lack of boundaries between work and home life has resulted in COVID-19 fatigue, leading to distress and burnout. 35 Perceptions of COVID-19 risk at work also play an important role. During the survey, the Delta variant was dominant and New York State was averaging 5077 cases per day (~3.0% positivity rate). 36 Fear of contracting and spreading the virus is a threat to the psychological well-being and occupational efficiency of frontline workers37-39 and has created stress and frustration, and even job departures, for employees seeking more flexible and safer work.
Communication
The stress PHWs endured as a result of inadequate communication and support from the state emphasizes the importance of improved communication and relationships between state and county agencies in future public health emergencies. LHD staff have been central to communicating state directives to the public, including liaising with schools and businesses and conducting contact tracing. 6 PHWs reported frequent harassment and threats while conducting these activities, most frequently by telephone, in person, and on social media. In the open comments, many shared experiences of being yelled and cursed at while contact tracing and discussed the lack of support from local government officials and the challenges of supporting schools. Nationally, the percentage of US adults who believe threats or harassment of PHWs to be justified has increased from 15% to 21% and 20% to 25%, respectively, from November 2020 to July/August 2021. 40
This harassment, consistent with the hostility that has hit science and related fields during the pandemic, requires broader protections and support for PHWs, whether it be legal, technological, security, or mental health.41,42 An in-progress review of the COVID-19 response has also indicated the need for increased availability of risk-communication training to better equip PHWs with the tools necessary to communicate with the public during a public health emergency. 6
Funding and Job Satisfaction
Most health spending in New York State is directed toward the Medicaid program. 43 However, to stabilize the public health system and protect and retain the dedicated workers employed by LHDs, investments must be made to improve how vital public health services are funded to ensure that these public health entities are appropriately staffed. These investments would enable PHWs to be fairly compensated for their work, feel valued in their jobs, manage work/life balance, and avoid burnout, all key factors contributing to job satisfaction. Our qualitative results suggest that job satisfaction, work effectiveness, and mental health are interconnected. Improving the working conditions of PHWs and their psychosocial support within the public health system is critical to maintaining their mental health, especially during crises.
Article 6 of the New York State public health law provides statutory authority for state aid for general public health work. 32 Article 6 also provides reimbursement for expenses incurred by LHDs for core public health areas as defined by law. Initially, localities were the safety-net providers of primary and clinical home care services in a fee-for-service payment model, to provide basic care for uninsured and underinsured populations. Over time, the emergence of new payment models and expansion of the availability of clinical care reduced the need for LHDs to act as safety-net providers. Rather than reinvesting public health dollars from clinical care to population health services, public health funding was reduced.
The key to supporting effective public health strategies is providing sustainable foundational funding to public health entities that is commensurate with the work they are tasked with providing. One participant wrote, “Public health funding, especially at the local level, has been cut and public health work has been overlooked and devalued. This has to change.” To ensure current functions and prepare for future emergencies, public health funding must be increased substantially and should not be subject to repeated cuts. During the COVID-19 response, the federal government provided several dispersions of funding, but boom-and-bust funding has a specific “use-by date,” has spending restrictions, and does not allow LHDs to hire long-term staff who contribute to local public health infrastructure. In the open comments, PHWs expressed frustration with these funding constraints.
Limitations
This study had several limitations. First, selection bias limited the generalizability of this study. Because of limited contact information, surveys were sent only to department leaders, who decided whether to send the survey to their staff. Only PHWs employed at the time of data collection were included. Respondents were predominantly located in Upstate New York, which provides an approximately equal distribution of metropolitan, micropolitan, and rural counties. Second, respondent bias could have occurred in 2 ways: bias toward overworked respondents in disproportionately burdened departments who were passionate about sharing their experiences or toward nonrespondents who did not respond because of heavy workloads.
Conclusion
The study results, combined with what we know about the New York State public health workforce, can be used to identify solutions that will support frontline PHWs. Decreasing psychological distress among PHWs starts with improving everyday working conditions, which requires adequate training, improved communication, experienced management, mental health support, and stronger legislation that protects against harassment. Adopting such measures will strengthen public health capacity and, hence, improve population health. Future research should evaluate the impact of these solutions on PHW recruitment and retention, as well as examine how the state and local context interact to enable and constrain the work of local public health organizations. As we emerge from the full-blown pandemic response, there has never been a better time to provide increased, disease-agnostic, sustainable funding to LHDs.
Footnotes
Acknowledgements
The authors thank the dedicated governmental public health workers who, despite long hours, burnout, harassment, and exhaustion, persevered throughout the pandemic response in New York State and across the nation. Their public servitude saved lives and had a direct impact on the health and safety of community members during this public health emergency. To those who responded to the survey, we thank you for taking time out of your busy schedules to share your experiences. We also thank Caroline Gomez-DiCesare, MD, of the Bassett Research Institute, and Jim Zians, PhD, of the State University of New York College at Oneonta, for early work in survey design, and Cristina Dyer-Drobnack, MS, of the New York State Association of County Health Officials, for assisting with survey distribution.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.