
Abstract
Objectives:
For decades, there have been calls to action to change the status quo of public health education in the United States to respond to workforce needs and help reinforce capacity. During the last 10 years, schools and programs of public health have planned and implemented programmatic and curricular changes. This study explored the focus of master of public health (MPH) education in the United States today.
Methods:
We used a 3-phase mixed-methods study to compile data to describe the current state and focus of MPH education in the United States via survey data collection (November–December 2019), semistructured interviews (January–February 2020), and document reviews.
Results:
Survey responses represented at least 43% (93/215) of eligible MPH programs in the United States. Most respondents (86%, 99/115) reported that the primary focus of MPH education in the United States is to prepare graduates for public health practice and employment linked to public health, and 54% (59/109) reported that their MPH programs adopted this focus in the last 5 years. MPH programs invested in student learning, competence development, and supporting workforce readiness, including a focus on leadership abilities. Programs noted that they seek to develop strategic thinkers and engaged leaders with abilities to understand and address emergent public health needs.
Conclusions:
Public health education in the United States is in a period of change. MPH programs reported responding to workforce needs by closing gaps in workforce capacity and developing compassionate and professional leaders who can understand needs, collaborating with communities, and facilitating action that will ameliorate health disparities and promote social injustice by practicing public health in new ways.
For more than a century, schools and programs of public health (SPPH) have helped capacitate the public health workforce by equipping graduates to enter the workforce, including positions in government, nonprofit, health care, education, and other sectors.1,2 SPPH in the United States were established to develop a cadre of interdisciplinary professionals able to prevent disease and support population health. 3 As of 2022, there were >200 accredited SPPH in the United States 4 ; the master of public health (MPH) is the most common degree awarded by SPPH, which produce some 17 000 MPH graduates each year. 5
Despite this investment in education, public health workforce capacity needs persist.6 -8 For 30 years, calls have been made to adapt public health education to current needs as one of many ways to ensure a robust workforce.8 -13 Specifically, SPPH have been encouraged to “transform their public health education, training, research, and practice endeavors—embracing new approaches in new settings with new partners to address current and emerging public health challenges” 14 because the “strategies and tactics of the past are not sufficient to meet the challenges of the future.” 15
To support these shifts, new standards for public health education were introduced by the Council on Education for Public Health (CEPH) in 2016. The new accreditation standards emphasize acquisition of foundational public health knowledge and development of workforce-defined competencies.16,17 These areas of educational focus emerged from government public health workforce initiatives led by the Council on Linkages Between Academia and Public Health Practice (Core Competencies for Public Health Professionals) 18 and the de Beaumont Foundation (Public Health Workforce Interests and Needs Survey)6,7,13 and from general public health workforce–focused initiatives led by the Association of Schools and Programs of Public Health (ASPPH; Blue Ribbon Employer Advisory Board and Framing the Future: Public Health Trends and Redesigned Education)19,20 and the National Board of Public Health Examiners (Job Task Analysis).16,21 The shift in standards was important because it moved SPPH from a model of teaching in siloed areas to one that prioritizes development of competence in cross-cutting areas in the workforce.8,10,16,17,22 -26
During the last 10 years, prompted by CEPH and these other initiatives, SPPH have planned and implemented adaptations to their MPH programs. 9 We hypothesized that amid the shifts, MPH programs may have refined or redefined the focus of their education and the outcomes sought. Prior research on competence-based education for health professions suggested that, as a part of these shifts, MPH programs would focus on various types of learning (informative, formative, and transformative) to foster competence,3,8,22,24 developing graduates who are ready to enter the workforce with desirable skills and attributes3,6 -8,13,16,22 -25 and supporting high rates of graduate employment (Table 1).13,16,17,20 We set out to understand whether those 4 constructs are the focus of MPH programs in the United States today.
Focus areas of health-related professional education programs, as identified through existing literature, in a study of the current state and focus of MPH education in the United States, 2019-2020
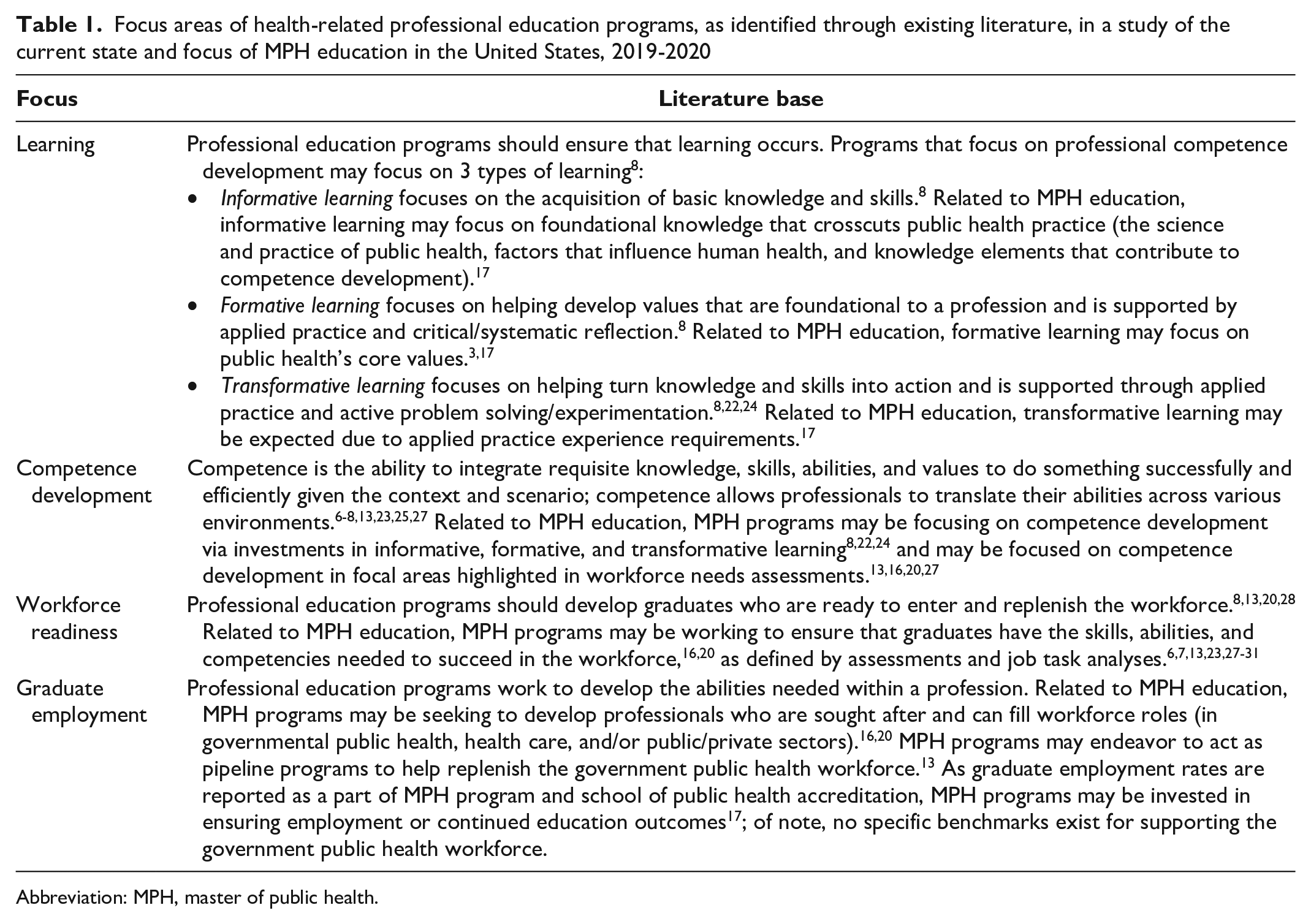
Abbreviation: MPH, master of public health.
Methods
We used a 3-phase mixed-methods study to describe the current focus of MPH education in the United States. In phase 1, we compiled data from MPH programs to depict program characteristics and their educational focus. We distributed a Qualtrics survey to all CEPH-accredited or CEPH-applicant MPH programs in the United States via personalized emails and a post to an ASPPH-managed Listserv. The survey consisted of categorical and open-text questions; it was developed from a priori themes (Table 1) and pilot tested for validity, length, and flow. We used publicly available lists (CEPH and ASPPH websites) and web searches (“program director,” “associate dean for curriculum,” “associate dean for practice,” and/or “associate dean for academic affairs”) to develop the email distribution list of 248 unique individuals at 215 institutions. The survey was accessible from November 21 through December 20, 2019. Of the 248 individuals on the distribution list, 132 (53%) opened the survey and 125 (95%) consented to participate. We removed survey responses that were not at least 80% complete (n = 10), leaving 115 valid survey responses. Of these respondents, 22 (19%) did not list an institution name; we did not exclude these 22 respondents from analysis, however, because when we reviewed the data during the data-cleaning process, the responses suggested that they were not from an institution that had already responded. We used Real Statistics Resources Pack Release 8.2.1 (Charles Zaiontz) to calculate descriptive statistics (response rates, frequencies, distributions, and means) and measures of association. We assessed associations between program characteristics (age, size, type, affiliation, and Health Resources and Services Administration region) and survey responses via cross-tabulations and tests of significance (Pearson χ2 test or Fisher exact test), and we used Dedoose version 8.1 (SocioCultural Research Consultants, LLC) to code and analyze open-ended responses.
In phase 2, we compiled data to describe the themes identified in phase 1 in depth (program focus, desired outcomes). We conducted document reviews and semistructured interviews from January 28 through February 25, 2020. Thirty-nine phase 1 respondents consented to participate in phase 2. To maximize the diversity of perspectives, 32 we used blinded stratified purposeful sampling to generate a list of 8 MPH programs that were diverse in size, age, type, affiliation, and location. We conducted interviews with the phase 1 respondent and his or her invitees (n = 12 interviewees total). Before the interview, we reviewed publicly available documents (website, CEPH self-study, student handbook) to develop interview probes, and we provided participants with a study overview, informed consent documents, and an outline of topics to be discussed. If participants requested a copy of their phase 1 survey responses, we shared it via email as a PDF report from Qualtrics. We conducted 45-minute video interviews via Zoom (Zoom Video Communications) using the semistructured interview guide. Interviews were audio recorded, transcribed, quality checked, and deidentified. We then conducted 3 rounds of coding, first with full transcripts and then with segments, using a priori codes (Table 1) and subcodes defined in the code book. We used a peer validation process to validate and improve the coding process and help decrease researcher bias.
In phase 3, we integrated categorical, thematic, and descriptive data from phase 1 (open-ended responses) and phase 2 to summarize answers to the defined research questions. If we noted divergent themes across phase 1 and 2 data, we further reviewed the primary data to explain divergence. The University of Illinois at Chicago Institutional Review Board deemed this study (protocol 2019-1203) exempt from human subjects review (category 2) based on the data collection methods (voluntary participation in survey and interview) and because the data collected would not reasonably place the participants at risk of criminal or civil liability or be damaging to the participants’ financial standing, employability, educational advancement, or reputation (45 CFR 46.104[d][2]). 33
Results
Respondent Characteristics
The 115 participants in phase 1 of the study represented at least 93 of 215 (43%) CEPH-affiliated MPH programs in the United States, including at least 29 of 64 (45%) MPH programs in schools of public health and 64 of 151 (42%) public health programs (Table 2). The 93 named institutions were geographically distributed, representing at least one-third of MPH programs in each Health Resources and Services Administration region. Phase 1 survey respondent characteristics generally mirrored those of CEPH-affiliated MPH programs by size, age, type, ASPPH affiliation, and Health Resources and Services Administration region. The phase 2 sample, consisting of 8 interviewed MPH programs, also represented characteristics of MPH programs nationally and those represented in the survey.
Characteristics of study sample and comparison with CEPH-accredited or CEPH-applicant MPH education programs in the United States, 2019-2020
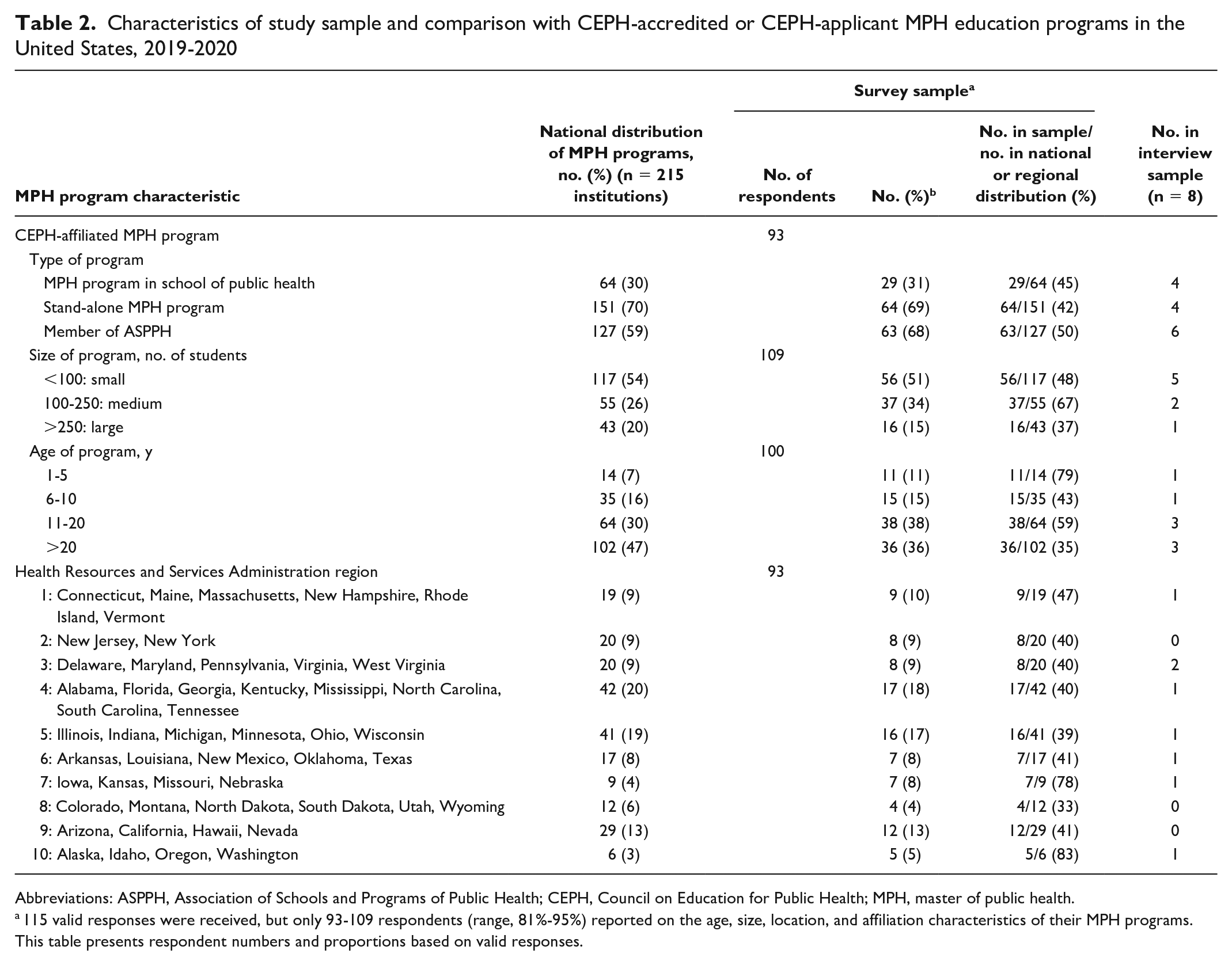
Abbreviations: ASPPH, Association of Schools and Programs of Public Health; CEPH, Council on Education for Public Health; MPH, master of public health.
115 valid responses were received, but only 93-109 respondents (range, 81%-95%) reported on the age, size, location, and affiliation characteristics of their MPH programs. This table presents respondent numbers and proportions based on valid responses.
MPH Program Focus
Most survey respondents (76%, 87 of 115) stated that the primary focus of MPH-level training in the United States should be to “train practitioners/leaders” rather than to “train researchers” (n = 1) or to “act as a steppingstone to other education” (n = 0). Seventeen percent (20 of 115) of respondents reported “all of the above,” while 6% (n = 7) listed other areas of focus, including “train graduates as independent professionals,” “evidence-based practice and good science,” “program management and evaluation,” “integration with other degrees to educate other professionals,” “complement other training/expertise,” “enhance training in other disciplines,” “prepare students for new areas of need,” and “implement/advocate for evidence-based policy and practice that impact health and social outcomes.”
When asked about the focus of their own program, 86% (99 of 115) of respondents reported that they “prepare graduates for public health practice” (eg, preparation for immediate employment linked to public health), while 2% (n = 2) noted “preparing graduates for public health research” (eg, preparation for a doctor of philosophy [PhD] program or a research fellowship); 1% (n = 1) cited “integration with other professional degrees” (eg, doctor of medicine, doctor of veterinary medicine, master of business administration, juris doctorate); and 11% (n = 13) indicated “other.” Open-ended “other” responses suggested that some MPH programs focus on all 3 areas (n = 10), while others reported their focus as developing professionals, supporting the career trajectory of students (research, doctor of medicine, or practice), and helping students be ready to tackle the world’s most pressing public health issues. Of note, 54% (59 of 109) of respondents indicated that since 2015, they have adapted their MPH program to increase emphasis on training students for public health practice (applied work at the community, county, state, local, or international level in governmental or nongovernmental sectors); 43% (47 of 109) indicated that shifts in focus were not made because they had already taken place before 2015; some (n = 3) indicated no changes. We found no significant difference in responses by program characteristic.
Phase 1 open-ended responses provided insight and preparation for the phase 2 interviews, including probes related to what, specifically, programs are focused on, what training for public health practice means, and what desired program outcomes are. We noted 4 clearly defined themes in the phase 2 data; 3 of the 4 themes were a priori themes: learning, competence development, and workforce readiness and success (Table 1). The fourth theme, leadership, emerged as a cross-cutting theme, in part because of the substantial focus on transformative learning. The expected theme of “ensuring graduate employment” was not prevalent in phase 2 data.
Learning
All 8 MPH programs interviewed noted a focus on supporting integrated learning and reported investment in informative learning to build MPH student knowledge and skills so that students and graduates succeed in the workforce, in their careers, and in improving public health (Table 3). To succeed as a public health practitioner, interviewees indicated that students need to have a broad education related to the tenets of public health and the structure and function of governmental public health: “I describe the MPH as getting breadth in education” (interviewee 2).
Emergent themes in focal areas of MPH education in the United States, 2020
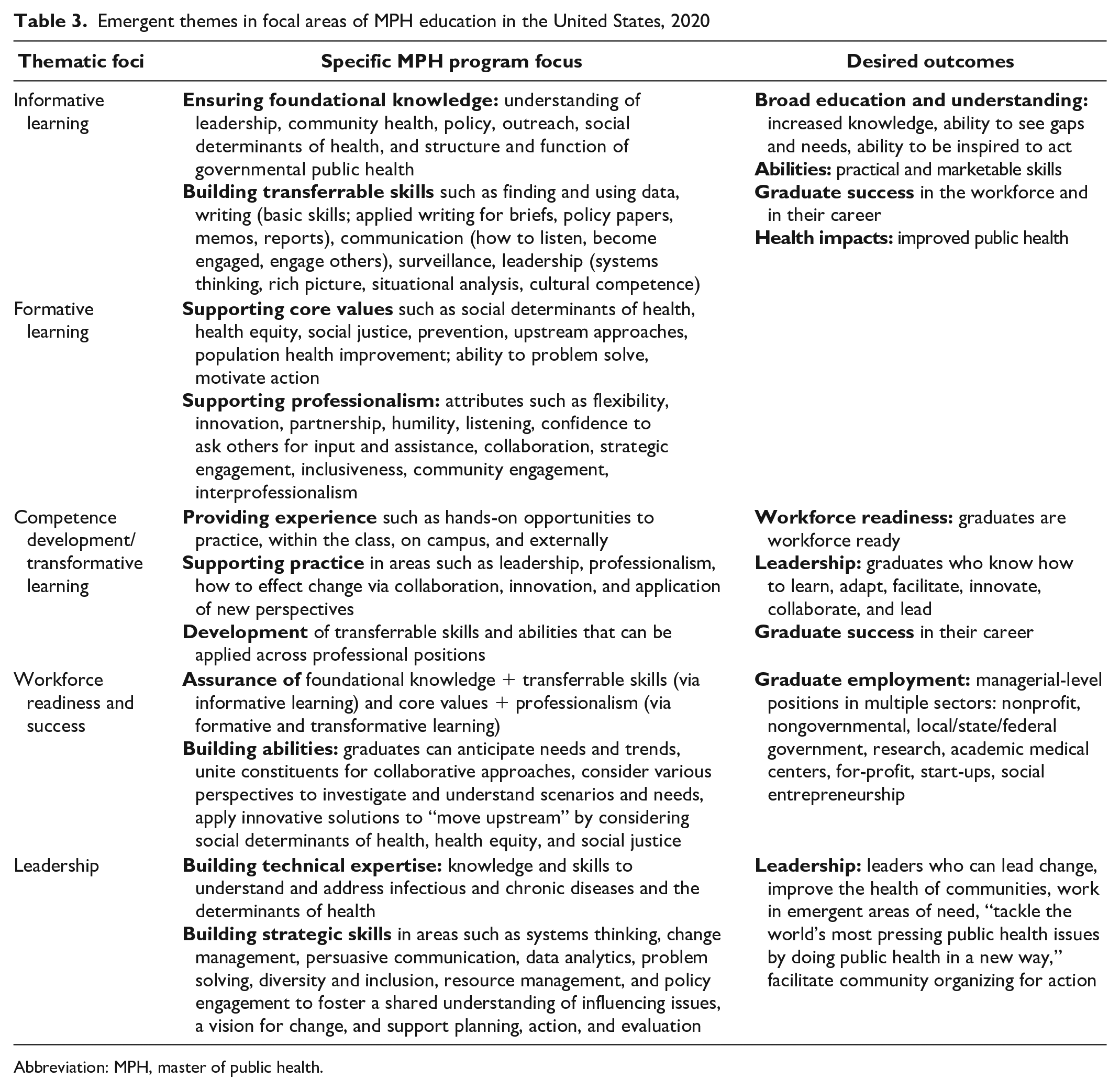
Abbreviation: MPH, master of public health.
All interviewees reported investing in helping students develop practical and marketable skills that they can apply immediately and across industries (Table 3) because skills help students succeed and move ahead in the workforce, even for students who are more experienced: “[Until now] the purpose [of MPH education] hasn’t matched the needed outcome. . . . We tend to forget that the MPH is the practice degree” (interviewee 7).
All interviewees also reported a focus on formative learning and teaching to develop professional values and professionalism skills (Table 3). Interviewees noted the importance of helping students learn the values of public health such that they can see gaps and needs and be inspired to act on health equity, social justice, and population health improvement and be able to use that understanding to motivate action: “[The focus is on] preparing students for community health activities and helping them learn what it is, how we can address community health, and then also how to lead” (interviewee 6).
Competence Development
All MPH programs interviewed reported a focus on transformative learning by providing hands-on learning opportunities and by focusing on transferrable skills development. Of note was the focus on professionalism and leadership practices, with goals of supporting innovation and developing graduates who know how to learn, adapt, facilitate, innovate, collaborate, and lead (Table 3). Some interviewees suggested that the current length of MPH programs (1-2 years, 42 credits) is not long enough to teach all the technical content that students may need, and so programs must focus instead on helping students have adaptable and strategic skills.
I talk to my students about collaboration because public health cannot do much if we stay in silos. We need to innovate. Thirty years ago, there were five different areas of public health and now there is like a million, and every time we turn around there is something else. We need to be prepared to react to new challenges. We need to teach flexibility, innovation. It’s like partnerships, the humility to share and to talk to other people and to lean on other experts. We cannot possibly cover all [topic areas] in an MPH program, but we need to be ready for it. . . . That’s what we need to prepare students for. (interviewee 3)
Workforce Readiness and Success
In addition to learning, all MPH programs interviewed reported a focus on ensuring that graduates are workforce ready and equipped with abilities desired by the public health workforce. Interviewees noted a number of transferrable skills and abilities that are important for success in the workforce (Table 3). “The thinking behind the public health core competencies was, these are the skills that people need in the workforce” (interviewee 7).
All interviewees stated that this focus on workforce readiness and success is linked to at least 1 national initiative: CEPH-defined competencies 17 or Council on Linkages core competencies. 18
The public workforce doesn’t receive enough training—we are thrown into the job and then it’s like, good luck to you. When I look at the core competencies for public health professionals, I’m like, this is exactly where we need to be with our graduates. (interviewee 3) We prepare public health professionals for managerial-level positions in public health practice. I think the [Council on Linkages] competency framework is useful . . . it provides a framework for what an MPH-level grad should be able to do out there in the workplace. (interviewee 8)
All interviewees indicated that they seek to develop skilled students and graduates who can practice public health–related work in the field and professionals motivated to fill current and future public health roles; government public health roles were noted, along with many other sectors. MPH education as a pathway to a PhD was not explicitly stated in any interview, although interviewees identified the strategic value of integrating public health into various professional fields via dual degrees (including PhD programs) so that graduates can apply skills across many industries, including clinical, research, and academic medical centers.
I see the [MPH] degree as the professional entrée. . . . There’s all kinds of positions that affect public health. . . . Public health graduates must be trained sufficiently in all these areas to interact with others from various disciplines and then land in a particular area that fits them. (interviewee 1)
Another participant said, “The MPH is a professional degree. You should come out of the degree with a set of marketable skills that you can use across a whole range of industries” (interviewee 4).
Four of 8 interviewees worried about dilution of MPH concentration areas in biostatistics and epidemiology because of the current pressure to focus more credit hours on the development of general public health competence. There is concern that this dilution might reduce the competitiveness and success of MPH graduates in some fields; some programs are developing advanced classes and certificates to build more in-depth quantitative ability.
Leadership
A theme that was not expected but emerged via qualitative data analysis was one of leadership beyond the 2 CEPH-defined leadership competencies: (1) apply principles of leadership, governance, and management, which includes creating a vision, empowering others, fostering collaboration, and guiding decision making; (2) apply negotiation and mediation skills to address organizational or community challenges. 17 All interviewees described how their curriculum aims to develop students who are aware and curious and who are able to engage, listen, and facilitate, as well as research, envision and act, and advocate for change (Table 3). They discussed the desire to develop graduates who are invested in the health of their communities and who can facilitate change to improve health equity.
I am looking [to develop] people who can look through different lenses and have priorities around inclusiveness and collaborative leadership, because to address the issues that need to be really addressed, we can’t keep doing the same things that we’ve been doing. (interviewee 1)
To support this, interviewees described the value of helping students develop strategic skills, integrating public health into other professional fields, and supporting job placement in areas beyond traditional government public health.
“[We have] the opportunity to train folks who will get out there and work in public health and ultimately make a difference and move the needle on population health. . . . We need talented, skilled people in governmental public health. And we know that there are real deficits that are growing. . . . We want and need our grads to be in those traditional settings. But also . . . in nontraditional settings. Those who end up in the for-profit world, at startups, doing social entrepreneurship. They’re thinking about public health differently. (interviewee 8) [Our goal is to develop graduates who] will be being prepared for anything and everything that comes up in public health. And at this point, I cannot even imagine what the next challenge would be. It’s almost like there has to be an MPH in every organization. (interviewee 3)
Discussion
While the last century has been a time of rapid growth for public health education, prior research reported a disconnect between graduates’ abilities and the real-world needs of public health jobs.8,10,14 -16,23,25 In response, national initiatives have spurred changes to public health education focused on developing workforce-defined competencies. As MPH programs have shifted their curriculum, 9 this study hypothesized that SPPH may have reenvisioned the focus of their MPH programs.
Background research suggested that MPH programs would be focused on supporting learning to build knowledge, skills, and values and on developing graduates who are ready for and employed in public health jobs. Based on data collected from at least two-fifths of CEPH-affiliated MPH programs in the United States, programs are focused on this and more. Whereas the literature base suggested that MPH programs had become siloed and had educational focal areas not fully aligned with the needs of the public health workforce, 8 this study found that MPH programs are informed by workforce needs (government and broader public health workforce) and are highly invested in preparing graduates to contribute to and succeed in the public health workforce (government and other) (Figure).
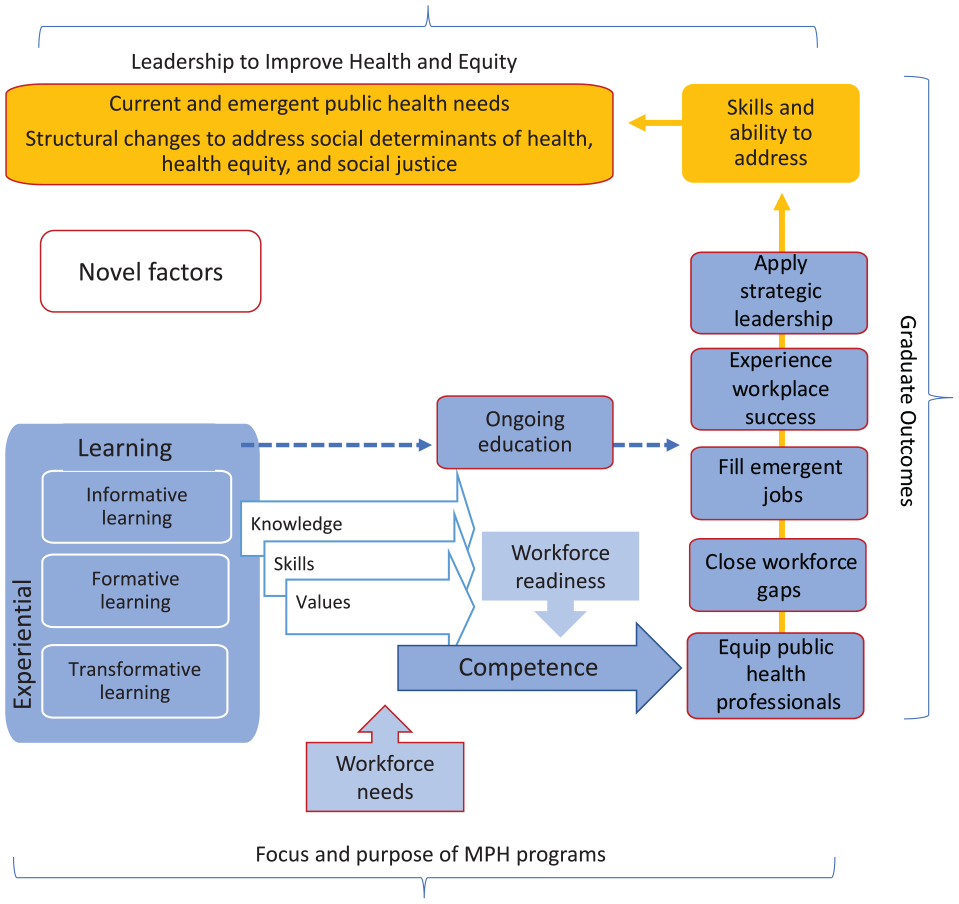
Conceptual frame depicting the focus of master of public health (MPH) education in the United States in 2020: deep investments in various approaches to learning to build knowledge, skills, and values (competence and readiness to meet workforce needs) such that graduates are public health professionals able to fill current and emergent roles, experience success in the workplace, and engage in strategic leadership to improve health and equity.
Respondents were almost unanimous in stating that the primary focus of an MPH program should be to develop public health professionals and leaders. Programs are not just looking to ensure graduate employment (a traditional metric of success) or employment in a specific sector (eg, government public health); they are seeking to develop well-equipped graduates who can meet workforce and community health needs. To do so, MPH programs are focused on preparing graduates for managerial-level positions (Tier II Council on Linkages Between Academia and Public Health Practice core competencies) 18 and developing professionals who can fill roles across multiple sectors and be a part of leading change and improving health outcomes.
Aligned with the focus of Public Health 3.0,15,23 MPH programs aim to develop strategic thinkers and interdisciplinary leaders who are invested in the health of their communities and who can “think on their feet” to anticipate needs and trends and unite community members and professionals for collaborative action. Study participants were aware of current public health needs and trends and suggested that public health graduates need to be able to innovate to “move upstream” to prevent or reduce ill health by considering social determinants of health, health equity, and social justice.
To support development of these professionals, MPH programs focus on workforce-informed competencies, as defined by CEPH, 17 the Council on Linkages Between Academia and Public Health Practice, 18 and constituent input (via ASPPH).19,20 Competence development is supported by investment in progressive and applied learning 8 to ensure that students have solid foundational knowledge and public health values and a transferrable skill base that can be adapted to various contexts to support professional success.
Limitations
This study had several limitations. While the response rate was strong and the sample of SPPH was representative by many criteria, those who did not respond to the survey or opt into the interview may represent a dissenting opinion. Furthermore, the results presented here represent the perspectives of a single person or a few people in each SPPH (those who oversee the MPH program curriculum and/or practice); as such, input from other SPPH leaders or faculty might differ. Future research could seek to sample a broader array of faculty to understand perspectives across different disciplinary backgrounds. Finally, these data were collected before the COVID-19 pandemic; it is possible that SPPH have further shifted focus in response to the critical workforce needs experienced since March 2020.
Conclusion
For decades, public health leaders in the United States have proposed multiple strategies to address gaps in the public health workforce, including collaboration with SPPH. This study suggests that MPH programs are focused on closing gaps by developing compassionate and professional leaders who have the ability to understand needs, collaborate with communities, and facilitate action to improve health disparities by practicing public health in a new way. This focus is encouraging as the United States seeks to build back from the effects of the COVID-19 pandemic. However, at the time of data collection (before COVID-19), it did not appear that MPH programs were focused specifically on helping to close gaps in the government public health workforce; rather, they perceived the value of ensuring public health competence being integrated into multiple fields and sectors. As state and local governments look to rebuild their workforces, there may be opportunities to forge stronger ties with MPH programs and help them connect graduates with rewarding government public health roles.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.