
Abstract
COVID-19 vaccine misinformation is a global threat, and digital and social media support its spread. Addressing Spanish-language vaccine misinformation is critical. In 2021, we began a project to increase vaccine confidence and uptake in the United States by assessing and opposing Spanish-language COVID-19 vaccine misinformation circulating in the United States. Analysts identified trending Spanish-language vaccine misinformation each week, and trained journalists provided communications guidance for addressing the misinformation, which we delivered to community organizations via a weekly newsletter. We identified thematic and geographic trends and highlighted lessons learned to inform future efforts to monitor Spanish-language vaccine misinformation. We collected publicly available Spanish- and English-language COVID-19 vaccine misinformation across various media sources (eg, Twitter, Facebook, news, blogs). Analysts identified top trending vaccine misinformation in the Spanish query and compared it with vaccine misinformation in the English query. Analysts examined misinformation to identify its geographic source and dominant conversation themes. From September 2021 through March 2022, analysts flagged 109 pieces of trending Spanish-language COVID-19 vaccine misinformation. Through this work, we found that Spanish-language vaccine misinformation is easily identifiable. Linguistic networks are not distinct, and vaccine misinformation often circulates across English and Spanish queries. Several websites have outsized influence in promoting Spanish-language vaccine misinformation, suggesting that it may be important to focus on a handful of hyperinfluential accounts and websites. Efforts to address Spanish-language vaccine misinformation must incorporate collaboration with local communities and emphasize community building and empowerment. Ultimately, addressing Spanish-language vaccine misinformation is not an issue of data access and knowledge of how to monitor it; it is an issue of prioritization.
The infodemic of misinformation about the COVID-19 pandemic and vaccines has decreased vaccine uptake and increased disease transmission globally. 1 Since the start of the COVID-19 pandemic, misinformation has eroded trust in health authorities and science. 2 Addressing COVID-19 vaccine misinformation is a priority in ensuring long-term vaccine acceptance. Much of the research and reporting on misinformation has focused on English-language misinformation, even though more than 41 million people speak Spanish at home in the United States. 3 Misinformation in Spanish-language content routinely evades social media fact-checking protocols; for example, in one analysis, 70% of Spanish-language content flagged as misinformation by third-party moderators had no warning label to inform readers of falsehood and potential harms, compared with 29% of English-language content flagged as misinformation.4,5
Addressing Spanish-language vaccine misinformation is critical, given that Hispanic/Latinx populations are at a higher risk of COVID-19–related morbidity and mortality than non-Hispanic/Latinx populations are.6-8 In one US study, nearly 40% of Hispanic/Latinx adults, compared with 18% of non-Hispanic White adults, said a friend or family member had died of COVID-19. 9 COVID-19 vaccine confidence has been widely studied across racial and ethnic groups in the United States. In a systematic review, the pooled prevalence rate of vaccine hesitancy among Hispanic/Latinx adults was 30.2% compared with 26.3% among all adults. 10 Differences by country of origin are less studied; one study showed no difference in vaccine hesitancy among non–US-born Hispanic/Latinx adults and US-born non-Hispanic/Latinx White adults. 11 Although Hispanic/Latinx adults comprise 19% of the US population, 21% of the US population vaccinated against COVID-19 is Hispanic/Latinx. 12 It is critical to understand the COVID-19 vaccine misinformation to which the Hispanic/Latinx population is exposed to reach those who are unvaccinated and encourage uptake of boosters.
Monitoring vaccine misinformation is an important basic function of public health. 13 Various retrospective studies have analyzed media data to understand vaccine misinformation in English.14-19 Among studies that examined vaccine misinformation in various languages, only a handful focused exclusively on Spanish.20,21 To our knowledge, the most thorough review of vaccine misinformation among Hispanic/Latinx communities was published in 2021, highlighting top narratives, including misinformation about COVID-19 vaccine safety and alternative COVID-19 treatments. 22 The evidence base for vaccine misinformation in Spanish is still in its infancy compared with the evidence base for vaccine misinformation in English.
In 2021, the Public Good Projects (PGP), the Hispanic Communications Network, and World Voices Media/Pinyon Foundation partnered to support efforts to increase COVID-19 vaccine confidence and uptake in the United States by assessing and opposing vaccine misinformation geared toward Hispanic/Latinx communities. The project had 3 objectives: (1) identify vaccine misinformation reaching Hispanic/Latinx populations, (2) intervene on misinformation through local influencers and Spanish media, and (3) distribute tailored content via newsletters and community-based organizations.
Purpose
This case study describes the process of identifying COVID-19 vaccine misinformation reaching Hispanic/Latinx groups in the United States. We determined whether we could find thematic and geographic trends in Spanish-language vaccine misinformation identified in this project.
Methods
Spanish Monitoring
Since 2019, PGP has collected publicly available English media data on vaccines across various sources, including social media (eg, Facebook, Instagram, Twitter), news websites, blogs, video websites, and emerging websites. For this study, we adapted methods to collect additional data on conversations in Spanish. We collected data into an artificial intelligence–powered media monitoring software platform provided by Zignal Labs, Inc. Data collection was based on a Boolean query constructed by Spanish-speaking analysts, using hundreds of Spanish keywords (eg, vacuna, inmunizacion, #yonomevacuno) that we programmed into the software platform. The platform ingested any instance of a post, article, or comment that used that term. We programmed exclusion terms to remove references to animal vaccines (eg, #cuidadodemascotas).
To identify vaccine misinformation, 2 analysts created lists of terms or hashtags that were commonly used in references to vaccine opposition or misinformation (eg, muertes, tóxico). The analysts established these terms based on a review of the data, their expertise in public health and Spanish communications, and a prior publication on vaccine misinformation. 15 We programmed this list into the software platform and applied it to the entire dataset. This process produced a query that aggregated Spanish references to vaccine misinformation circulating in the United States, similar to PGP’s existing query containing vaccine misinformation in English. These methods are replicated from prior work that PGP has published; in-depth information on the process is available elsewhere.14,15 The Advarra Institutional Review Board determined that this study was exempt from review because we used preexisting, publicly available data.
From September 1, 2021, through March 30, 2022, each week the analysts used the media data collected through this process to identify vaccine misinformation trending in the Spanish-language query. The analysts determined trending vaccine misinformation by various factors, including the amount of engagement or the importance of the topic, and made decisions on whether to address vaccine misinformation using various tools.23,24 To determine whether the vaccine misinformation was also circulating in English, the analysts compared findings with the English-language query, noting which topics were circulating only in the Spanish query and which showed crossover to the English query. Each week, at least 2 analysts reviewed each piece of vaccine misinformation to determine that it met the criteria of misinformation. All analysts had received prior training on misinformation monitoring and identification. Trained public health journalists then reviewed vaccine misinformation to provide strategic communications guidance for community organizations that received the weekly newsletter (objectives 2 and 3). A sample newsletter is available (Supplemental Material).
Data Analysis
For this study, 2 Spanish-speaking analysts further reviewed vaccine misinformation to identify the country source of the misinformation, which was defined in 2 ways. If vaccine misinformation was shared via a website link, analysts searched a domain identification website to identify the country of domain registration. If vaccine misinformation was shared via a post directly, analysts examined the social media biography of the person sharing the content, reviewed historical posts to identify a geotag placed on their content, or reviewed references to a likely country of origin. Using this process, analysts classified all vaccine misinformation as originating from a specific country.
To understand trends in vaccine misinformation, 1 analyst thematically coded misinformation, using Crabtree and Miller’s 25 process for qualitative coding. Analysts generated themes until reaching data saturation, defined as the point at which analysts found themes in <5 pieces of misinformation. Analysts inductively coded vaccine misinformation to examine references to specific populations mentioned within misinformation. One analyst double-checked coding to ensure accuracy to the coding scheme, and discrepancies were resolved until 100% agreement was reached (Figure). We analyzed data in SPSS Statistics version 25 (IBM Corp). Because of small sample sizes, we did not conduct tests of significance.
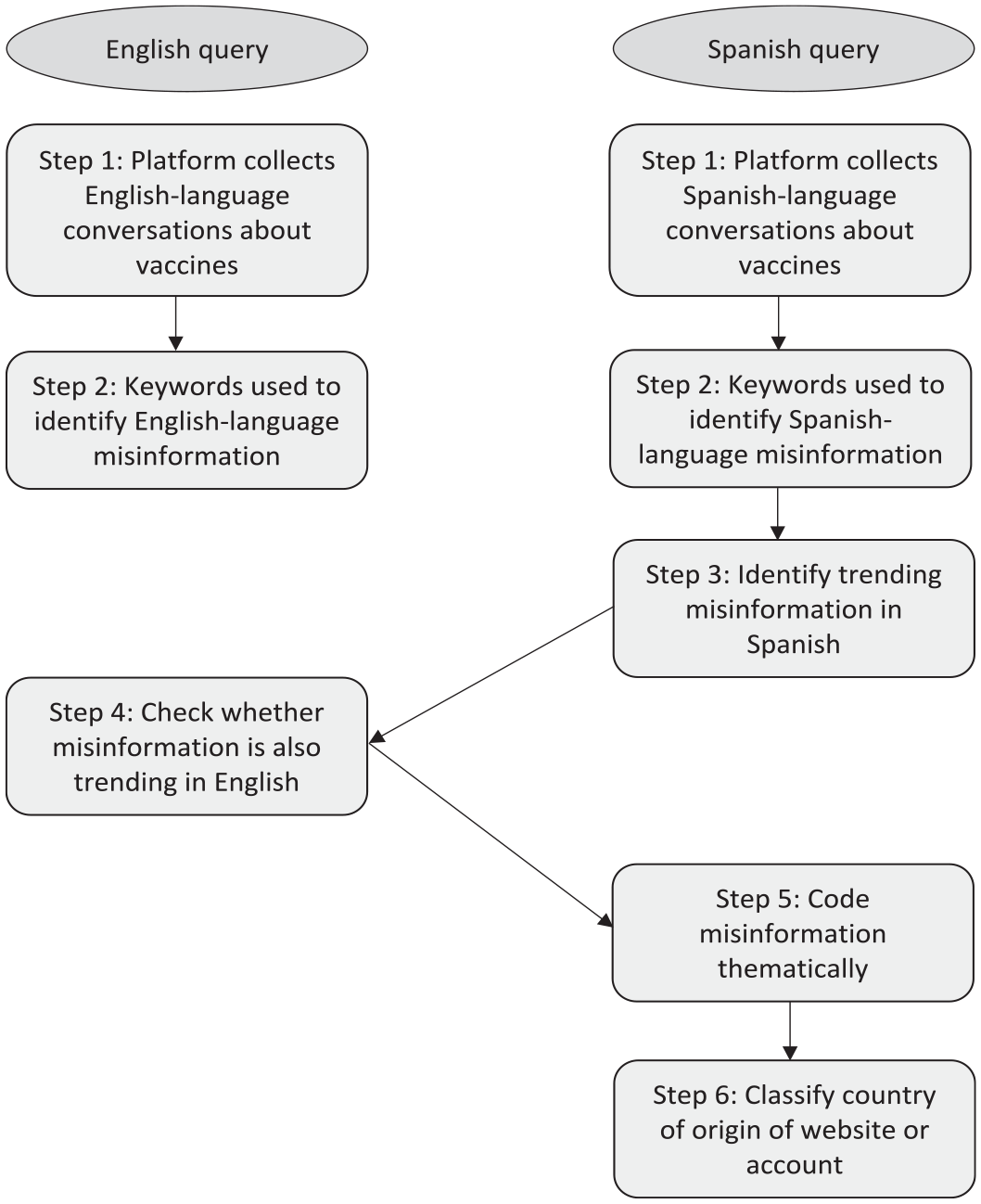
Data collection and analysis process for identifying online COVID-19 vaccine misinformation in English and Spanish, September 2021–March 2022.
Outcomes
During the data collection period, analysts flagged 109 pieces of Spanish-language COVID-19 vaccine misinformation circulating in the Spanish query (Table 1). Most posts (n = 68, 62.4%) were found only in the Spanish query, while fewer (n = 41, 37.6%) were found circulating in both English and Spanish queries. Of all misinformation identified, 29 (26.6%) posts shared a website link from 1 of 4 websites. Three of these 4 websites provided translations in English and Spanish for articles on the websites: 2 provided professional translations and 1 provided automatic machine translations.
Themes in online COVID-19 vaccine misinformation, by linguistic query, September 2021–March 2022 a
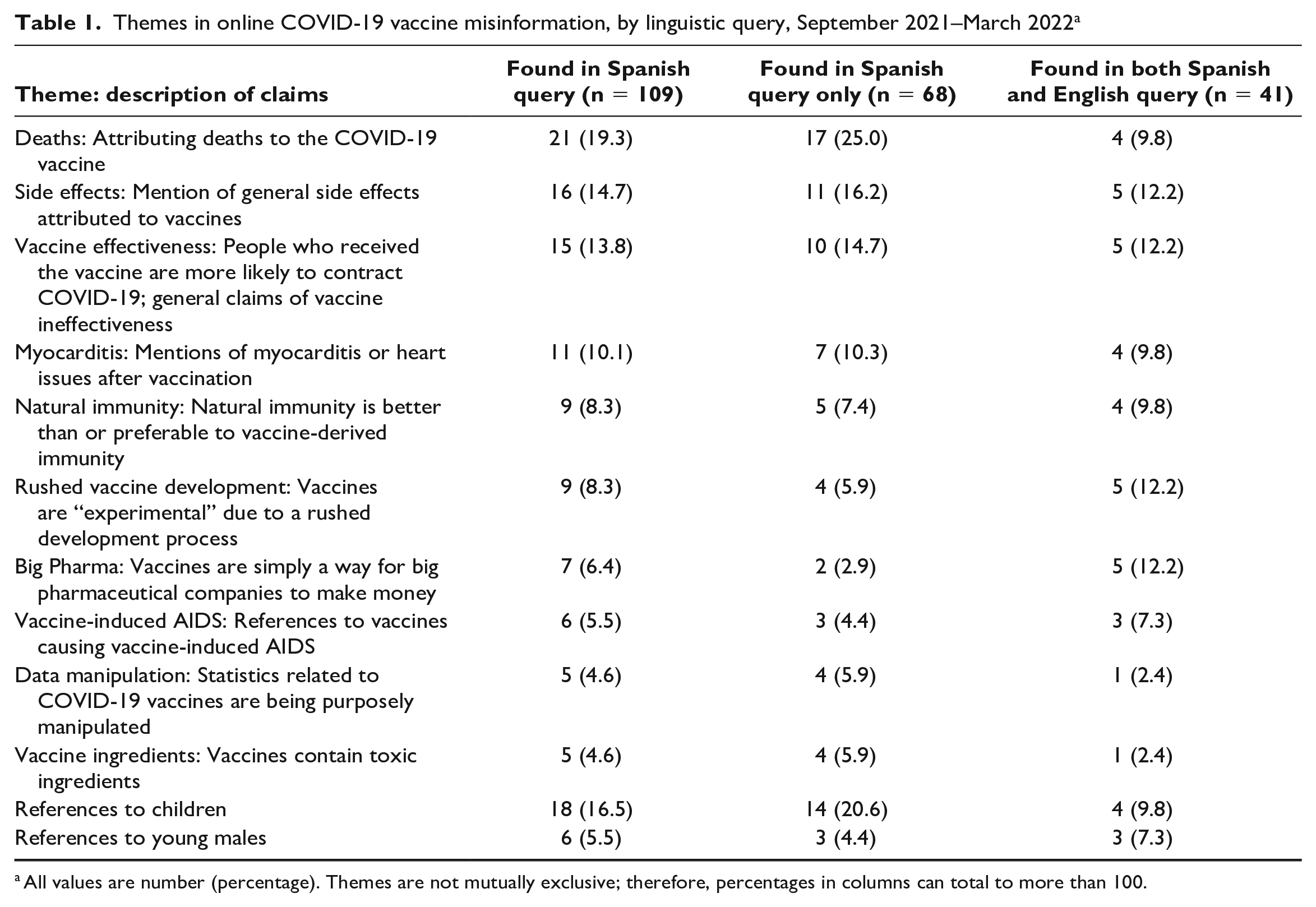
All values are number (percentage). Themes are not mutually exclusive; therefore, percentages in columns can total to more than 100.
When analyzed thematically, we identified 10 themes (Table 1). The largest theme comprised references to deaths attributed to COVID-19 vaccination (n = 21, 19.3%), followed by side effects after vaccination (n = 16, 14.7%), questioning vaccine effectiveness (n = 15, 13.8%), and references to myocarditis (n = 11, 10.1%). The remaining 6 themes comprised <10% of posts: natural immunity, rushed vaccine development, influence of big pharma, vaccine-induced AIDS, data manipulation, and vaccine ingredients.
When examined by primary language of the query (English vs Spanish), we found several notable differences. Analysts found references to deaths after vaccination and mentions of children more frequently in the Spanish query than in the English query (25.0% vs 9.8% and 20.6% vs 9.8%, respectively). In comparison, analysts found references to pharmaceutical companies and rushed vaccine development equally in both Spanish and English queries (12.2% and 12.2%, respectively). All other themes showed comparable percentages.
In the analysis of data on the country from which the COVID-19 vaccine misinformation originated, misinformation predominantly originated from 8 countries (Table 2). The United States and Spain were the top countries (50.5% and 13.8%, respectively), followed by the United Kingdom (11.0%). About one-third of vaccine misinformation found only in the Spanish query originated from 4 Spanish-speaking countries (Spain; 20.6%; Argentina, 7.4%; Dominican Republic, 2.9%; and Mexico, 2.9%). In addition, 7 pieces of vaccine misinformation found only in the Spanish query originated from predominantly non–Spanish-speaking countries (Germany, Iceland, Italy, Japan, Peru, Russia, and Scotland). Vaccine misinformation found in both English and Spanish queries mostly originated from English-speaking countries (United States, 56.1%; United Kingdom, 22.0%; Canada, 7.3%; and Australia, 4.9%).
Geographic location of website link shared or account posting online COVID-19 vaccine misinformation, by linguistic query, September 2021–March 2022 a
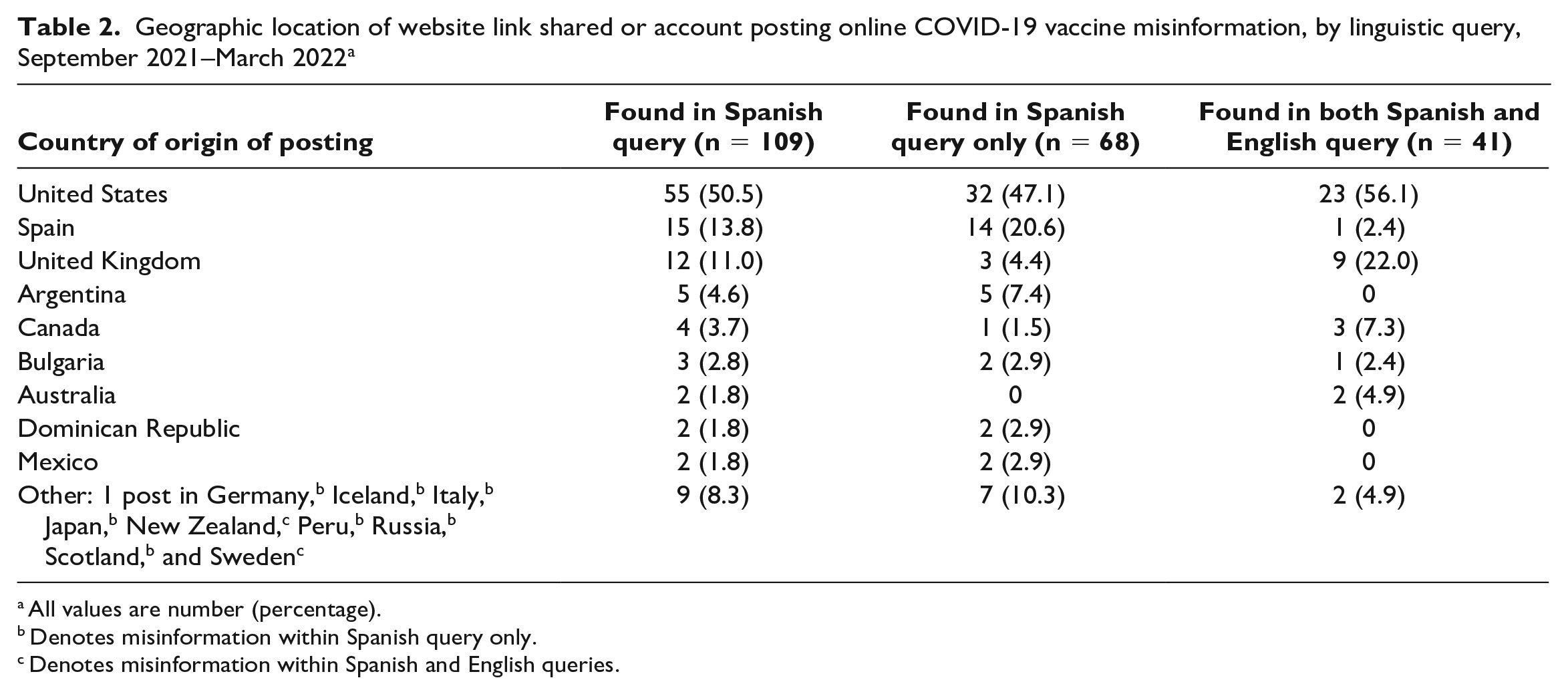
All values are number (percentage).
Denotes misinformation within Spanish query only.
Denotes misinformation within Spanish and English queries.
Lessons Learned
This case study reviewed the approach used to identify trends in Spanish-language COVID-19 vaccine misinformation that may affect public perceptions toward COVID-19 vaccines and insights into the top COVID-19 vaccine misinformation identified throughout the project. Through this work, we learned several lessons that can inform the future of monitoring Spanish-language COVID-19 vaccine misinformation.
Lesson 1: Spanish-Language COVID-19 Vaccine Misinformation Is Easily Identifiable
This finding supports the overwhelming evidence that Spanish-language COVID-19 vaccine misinformation is pervasive, is not well monitored, and frequently goes unchecked by platforms. In doing this work, it is critical to note that we did not create new approaches from the ground up. Rather, we adapted tested, publicly available, scientifically backed methods to monitor vaccine misinformation and refined them to be applicable to Spanish.14,15 The issue of addressing Spanish vaccine misinformation is not a problem of data access or knowledge of how to do the work.
Lesson 2: Several Websites Have Outsized Influence in Promoting Spanish-Language COVID-19 Vaccine Misinformation
Of all 109 pieces of Spanish-language COVID-19 vaccine misinformation identified, 29 originated from the same 4 websites, suggesting that a handful of easily discoverable websites and accounts have an outsized influence in spreading vaccine misinformation. This outsized influence of specific individuals and organizations has been well studied in English, with reports and studies showing that most global vaccine misinformation is spread by a handful of accounts and websites.15,26,27 Therefore, it may be less important to monitor the entire universe of vaccine conversations in Spanish and instead focus on a handful of hyperinfluential individuals and organizations. Doing so can help to make the issue of COVID-19 vaccine misinformation in Spanish more easily addressable.
Lesson 3: An Overlap in COVID-19 Vaccine Misinformation Spreads Through Spanish- and English-Language Networks
About 40% of misinformation that analysts flagged in the Spanish query was also flagged in the English query, showing that linguistic networks are not distinct and that substantial crossover exists. When we examined the country from which the website link or account originated, >70% of posts originated from non–Spanish-speaking countries. These results underscore the importance of recognizing the nuances in the Spanish-speaking population: >60% of Spanish speakers in the United States also speak English, and no concrete dividing line exists between English and Spanish speakers. 22 Efforts to monitor Spanish-language misinformation should not be restricted to accounts or websites in Spanish-speaking countries, especially given that misinformation easily spreads across borders. Tracking and identifying English- and Spanish-language misinformation should be parallel processes that draw lessons across both.
In comparing the thematic breakdown of posts circulating in Spanish and English queries, we also found similarities, with 2 exceptions. COVID-19 vaccine misinformation found only in the Spanish query had more references to deaths and to children than COVID-19 vaccine misinformation that also trended in the English query. These themes may be particularly resonant in Spanish-speaking communities. Although we found overlap in the types of vaccine misinformation that circulated between English- and Spanish-speaking communities, these similarities should not imply that responses to misinformation should be the same across groups. Cultural competence and segmenting health communications for various Hispanic/Latinx audiences still need to be front and center of addressing misinformation.28,29
Lesson 4: Public Health Needs to Value Accurate and Culturally Responsive Translations
The issue of Spanish-language vaccine misinformation is further compounded by the fact that educational Spanish-language resources on vaccines are often challenging to find. A 2021 study found that, in the top 10 most populated US cities, 5 of the major vaccine distributors did not offer COVID-19 vaccine information in Spanish and 4 did not offer vaccine scheduling in Spanish. 30 Even when Spanish-translated resources are present, the translations may be incorrect, stilted, or at a higher reading level than would be acceptable in English. 31 Automatic machine translations are frequently used to relay important vaccine information, although such services have been shown to be error prone, and Google Translate states that its services should not be used for public health translations unless verified by human translators.32,33 Investigative reporting found that, of 113 US public health websites reviewed, 60% made use of automatic machine translation. 34
Public health should place as much value on providing accurate translations as the top websites promoting vaccine misinformation. Our analysis found that 3 of the top 4 websites promoting vaccine misinformation provided Spanish translations. Spanish speakers who have valid questions or concerns about vaccines may be drawn to websites that provide well-translated materials, particularly if they are unable to get their questions answered through public health websites. These issues in providing accurate, easily accessible, and comprehensible resources in Spanish are critical to address, especially given the relatively small evidence base for understanding vaccine misinformation in Spanish.
Lesson 5: Monitoring Spanish-Language COVID-19 Vaccine Misinformation Is Not a Silver Bullet to Decreasing Misinformation in Communities
Our analysis was one aspect of a larger project. This work should be accompanied by participation with local community-based organizations and individuals, a focus on delivering messages through trusted sources, and letting the community help lead the work with the populations they know best. Recent studies have shown the importance of community–academic partnerships in addressing COVID-19 vaccine hesitancy and increasing vaccine equity.35,36 To truly stop the spread of vaccine misinformation and provide accurate health messaging to Spanish-speaking communities, forming community partnerships should be a central strategy.
This study had several limitations. First, the results of thematic and geographic distributions were based on the data selected as part of a larger project, which collected data on only the most commonly circulating vaccine misinformation. It is possible that other vaccine misinformation was also circulating at the same time, and it is therefore not possible to generalize conclusions of this study to the larger field of Spanish-language vaccine misinformation. Second, this study did not provide an evaluation of effectiveness of the larger journalistic intervention, which involved intervening on misinformation and distributing tailored content via newsletters and community-based organizations. Future research should examine the efficacy of our overall model of work.
Conclusions
The problem of vaccine misinformation in Hispanic/Latinx communities is a health communications crisis with solutions. The lack of focus on Spanish-language vaccine misinformation is a result of structural inequities that deprioritize access to culturally meaningful health information. 37 The lessons that we have learned can be implemented at a large scale to monitor vaccine misinformation in Spanish, if given the prioritization it deserves. Yet, it is also important to recognize this work as one piece of the puzzle in ensuring equal access to health information. Efforts to address vaccine misinformation in Spanish should also incorporate collaboration with community-based organizations and local messengers, with an emphasis on empowerment, community building, and trust.
Supplemental Material
sj-pdf-1-phr-10.1177_00333549231168452 – Supplemental material for Lessons Learned From Monitoring Spanish-Language Vaccine Misinformation During the COVID-19 Pandemic
Supplemental material, sj-pdf-1-phr-10.1177_00333549231168452 for Lessons Learned From Monitoring Spanish-Language Vaccine Misinformation During the COVID-19 Pandemic by Erika Bonnevie, Valeria Ricciulli, Megan Fields and Ruth O’Neill in Public Health Reports
Footnotes
Acknowledgements
The authors thank the following people for their participation in this program: Megan Barber, PhD, Allison Gallegos-Jeffrey, MPH, Jaclyn Goldbarg, MPH, Megan Leibensperger, MA, Darshana Panchal, MPH, Melissa Silesky, MPH, and Joe Smyser, PhD, at The Public Good Projects; Mariana Diez, MPR, José López, BA, Mariana Nonino, BA, Ana Saraí Peña, MSL, and Alison Rodden, BA, at the Hispanic Communications Network; and Angelique Magdaleno, MA, Steph Niaupari, MA, and Patricia Fausto-Rodriguez, MA, at World Voices Media.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the Centers for Disease Control and Prevention (CDC) of the US Department of Health and Human Services (HHS) as part of a financial assistance award totaling $25 660 048, with 100% funded by CDC/HHS (grant no. 43101). The contents of this article are those of the authors and do not necessarily represent the official views of, nor an endorsement, by CDC/HHS or the US government.
Supplemental Material
Supplemental material for this article is available online. The authors have provided these supplemental materials to give readers additional information about their work. These materials have not been edited or formatted by Public Health Reports’s scientific editors and, thus, may not conform to the guidelines of the AMA Manual of Style, 11th Edition.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.