
Abstract
Objective:
Tuberculosis (TB) is a public health problem, especially among people experiencing homelessness (PEH). The Advisory Council for the Elimination of Tuberculosis issued recommendations in 1992 for TB prevention and control among PEH. Our goal was to provide current guidelines and information in one place to inform medical and public health providers and TB programs on TB incidence, diagnosis, and treatment among PEH.
Methods:
We reviewed and synthesized diagnostic and treatment recommendations for TB disease and latent TB infection (LTBI) as of 2022 and information after 1992 on the magnitude of homelessness in the United States, the incidence of TB among PEH, the role of public health departments in TB case management among PEH, and recently published evidence.
Results:
In 2018, there were 1.45 million estimated PEH in the United States. During the past 2 decades, the incidence of TB was >10 times higher and the prevalence of LTBI was 7 to 20 times higher among PEH than among people not experiencing homelessness. TB outbreaks were common in overnight shelters. Permanent housing for PEH and the use of rapid TB diagnostic tests, along with isolation and treatment, reduced TB exposure among PEH. The use of direct observation enhanced treatment adherence among PEH, as did involvement of social workers to help secure shelter, food, safety, and treatment for comorbidities, especially HIV and substance use disorders. Testing and treatment for LTBI prevented progression to TB disease, and shorter LTBI regimens helped improve adherence. Federal agencies and the National Health Care for the Homeless Council have helpful resources.
Conclusion:
Improvements in TB diagnosis, treatment, and prevention among PEH are possible by following existing recommendations and using client-centered approaches.
Tuberculosis (TB) is a public health problem in the United States, especially among people experiencing homelessness (PEH). An individual or family who lacks a fixed, regular, and adequate nighttime residence is generally defined as experiencing homelessness. 1 The rate of TB is higher among PEH than among people not experiencing homelessness.2-4 TB transmission can occur in congregate settings (eg, shelters, correctional facilities), especially in crowded shelters and when outside ventilation is diminished.5-7 PEH often have a greater risk than people not experiencing homelessness of developing TB or having comorbidities that increase TB risk, if infected with latent TB infection (LTBI). 8
The Advisory Council for the Elimination of Tuberculosis (ACET) issued recommendations in 1992 for TB prevention and control among PEH. 9 Since 1992, guidelines for TB diagnosis, treatment, and prevention among adults and children have been updated. For up-to-date recommendations on TB disease and LTBI diagnosis, treatment, and prevention among PEH, the audience, who might not be public health practitioners, would need to review multiple documents. Our objective was to review and synthesize the current TB guidelines that are relevant to PEH. Specifically, we assessed and reported the current magnitude of homelessness in the United States, the TB incidence among PEH, the applicability of current diagnostic and treatment guidelines for TB disease and LTBI to PEH, the role of public health departments in TB case management among PEH, and the recently published evidence for each of these topics. Our goal was to inform medical and public health providers, TB programs, and other service providers on the present TB incidence among PEH and on updated diagnosis and treatment protocols for TB among PEH.
Methods
To state the problem, we summarized the magnitude of homelessness by reviewing US Department of Housing and Urban Development (HUD) publications. To describe TB among PEH, we summarized statistics from reports on the US National TB Surveillance System, which includes data on homelessness within the past year. 10 We identified and reviewed current recommendations as of 2022 relevant to PEH on diagnosis, treatment, and prevention of TB and LTBI for US populations. We then searched PubMed for publications published from January 1993 through April 2022 that provided evidence supporting the recommendations by using the following terms: “homeless or homelessness” AND “tuberculosis or latent tuberculosis infection” AND “treatment” AND “United States.” Among 260 results, we found 55 articles after excluding recommendation documents and duplicate articles from the same study or those included in systematic reviews. We selected systematic reviews that included ≥1 US study rather than single-site US studies. We retained some references prior to 1992 from the 1992 ACET recommendations. 9
Results
Homelessness
For the most recent year (2018) for which estimates were not adversely affected by the COVID-19 pandemic, HUD reported an estimated 1.45 million PEH in the United States. 11 HUD also estimated that the number of PEH on a single night (“point-in-time”) in January 2020 was 580 466, of whom 61% were sheltered. 12
The ACET 1992 recommendations advised health care and social service providers to ask their clients if they are experiencing homelessness or if they lack a fixed, regular, and adequate nighttime residence. 9 To facilitate TB diagnosis and treatment of PEH, public health departments are recommended to maintain, and regularly update, listings of single-room occupancy hotels and homeless shelters so that addresses of PEH can be checked against these listings. Shelters should maintain lists of people staying in their facilities and share clinical data on PEH. 9 The National Health Care for the Homeless Program of the Bureau of Primary Health Care at the Health Resources and Services Administration (HRSA) funds health centers serving PEH and collects and shares health services data on PEH. 13
TB Among PEH
ACET recommends assessment of the incidence of TB among PEH, which requires accurate PEH population estimates. 9 In 2020, 290 TB cases among PEH (4.3% of TB cases in the United States) were reported to the US National TB Surveillance System. 10 From 2007 through 2016 in the United States, the number of TB cases was 11 times greater among PEH (36 per 100 000 PEH) than among people not experiencing homelessness (3.1 TB cases per 100 000 US population).3,10 In 2021, estimates of TB incidence among PEH from 2011 through 2016 were also published for large HUD continuum of care program areas. 3
Although data have not been systematically collected among all PEH, the estimated LTBI prevalence from individual studies ranged from 18% to 54% among PEH,14-16 which is 7 to 20 times higher than the estimated 2.7% to 5.0% LTBI prevalence in the general US population. 17 This higher LTBI prevalence places PEH at greater risk for TB progression than the general population.
From 2009 through 2015, 8 of 21 TB outbreaks involved overnight facilities for PEH. 18 Of 457 people included in these TB outbreaks, 204 (45%) had experienced homelessness in the year before diagnosis. 18 Large genotypic clusters of TB cases gathered from data from 2009 through 2018 disproportionately included PEH, suggesting recent TB transmission. 19
TB Diagnoses Among PEH
Rapid diagnosis of pulmonary TB, isolation, and treatment can reduce transmission in crowded congregate settings such as shelters, hospitals, and correctional facilities. The diagnostic process starts by determining whether TB disease symptoms are present, performing chest radiographs and, if results are abnormal, conducting additional tests. 20 Diagnostic tests for TB include analysis of sputum for acid-fast bacilli by microscopy and nucleic acid amplification testing (NAAT), which have turnaround times averaging 24 to 48 hours.20-23 Current American Thoracic Society/Infectious Diseases Society of America/Centers for Disease Control and Prevention (CDC) guidelines for diagnosis of TB disease among adults and children recommend performing diagnostic NAAT on the initial respiratory specimen from people with suspected pulmonary TB and on specimens collected from sites of suspected extrapulmonary TB. 20 One multisite study found that incremental cost savings occurred with NAAT (vs no NAAT) among PEH to diagnose or rule out TB. 24 Chest radiography has also been used as a screening tool in shelters with a low incidence of TB. 25
Because shelter residents and staff (including volunteers) are at increased risk of TB infection and disease, the American Thoracic Society/Infectious Diseases Society of America/CDC and the US Preventive Services Task Force (USPSTF) guidelines recommend targeted testing and treatment for LTBI in this setting and population26-28 in accordance with updated TB diagnostic guidelines. 20 Among tests for TB infection, interferon-gamma release assays (IGRAs) performed on blood samples have been found to be more efficient than tuberculin skin tests (TSTs) in improving test completion and retention in LTBI treatment among PEH.29-31 Testing frequency could range from one-time testing among PEH who are at low risk for TB exposure to annual testing among PEH who are at continued risk of exposure. 28 CDC and the USPSTF recommend that people with LTBI be evaluated and considered for treatment.28,32
A study in a low-income US community concluded that mandating LTBI testing and treatment along with education and outreach decreased TB cases, transmission, deaths, and costs. 33 Parriott et al 34 conducted a systematic review of TB screening among PEH and found high proportions of PEH who had been successfully tested, with most PEH with LTBI successfully referred for treatment.
Case Management of PEH With TB
A timely public health department outreach visit to PEH with possible TB disease can facilitate access to housing and other health care resources (eg, treatment for mental health, substance use disorders, HIV) and development of a TB treatment plan, including scheduling the patient’s first TB care visit. 9 Adding details about a patient’s physical description, activities, friends, and frequent gathering places in the medical record assists case managers in locating patients.
ACET recommends providing appropriate housing of PEH with infectious TB disease to allow directly observed initial TB therapy and to stop TB transmission in the community. 9 Without housing, PEH often experience long hospitalizations for TB at significant cost to society.35-40 The Community Preventive Services Task Force and the US Interagency Council on Homelessness recommend Housing First programs to decrease homelessness, increase housing stability, and improve quality of life among PEH.41,42 Providing housing during treatment is also critical to ensuring TB treatment completion, prompting ACET to recommend the establishment of special shelters or other long-term care arrangements for PEH with TB disease. 9
An analysis of TB cases from 1994 through 2003 found that, compared with TB patients not experiencing homelessness, PEH with TB had a higher prevalence of substance use (54% excess alcohol use, 29.5% noninjecting drug use, and 14% injecting drug use), with 34% of PEH tested having coinfection with HIV. 8 Shelter, food, safety, and comorbidities are likely to be top concerns for PEH; involvement of social workers (or other staff) on the treatment team to assist in solving these other problems is important for achieving successful TB treatment. 9
TB and LTBI Treatment of PEH
TB disease treatment of PEH should follow CDC guidelines. 43 The use of shorter regimens (eg, 4-month drug-susceptible TB treatment) might facilitate treatment completion, 44 especially among people such as PEH who experience barriers to completion of longer 6- or 9-month regimens. Health care providers can assess interactions of TB medications with those for comorbidities to inform TB regimen choices. 45 Failure to take TB medications as prescribed can result in TB relapse, drug resistance, further TB transmission, and death. To facilitate adherence, the 1992 ACET recommendations stated that all TB treatments of PEH should be free of charge and transportation to clinics provided if needed. 9 A patient-centered treatment approach that uses incentives and directly observed therapy, the standard of practice, allows careful monitoring for treatment adherence and drug side effects and results in high treatment completion rates.43,46-48 In-person directly observed therapy might reduce the likelihood of robbery or assault of PEH compared with self-administered treatment because TB medications might be mistaken by others to have street value. 9 With adequate medical supervision, treatment can be given and observed by designated workers at the shelter or at another location. 9 Directly observed therapy by mobile telephone or web-based video is feasible, has high uptake, has adherence rates similar to in-person directly observed therapy,49,50 including among PEH, 51 and costs less than in-person directly observed therapy.52,53 If a patient with infectious TB disease (regardless of residential status) refuses treatment, temporary enforced isolation should be instituted in accordance with state and local public health laws and regulations. 9 Medicaid reimbursement for some services might be available, depending on state regulations.
Shelter operators may accept hospitalized PEH with TB who have bacteriologic and clinical evidence of response to therapy (ie, 3 consecutive daily negative sputum smears and asymptomatic status).9,20
Although homelessness has been associated with noncompletion of LTBI treatment, the use of short rifamycin-based 3- or 4-month regimens compared with 6- or 9-month isoniazid-monotherapy regimens can facilitate successful completion of LTBI treatment, including among PEH,54-57 as does LTBI treatment from nurse-led community health workers. 58 Several studies have estimated that LTBI treatment is cost-effective compared with no LTBI treatment of PEH.59,60
The following populations may be disproportionately represented among PEH and are recommended for TB prevention through TB infection testing and treatment: people with HIV, people who inject drugs, people who had recent contact with patients with infectious TB disease, people with medical conditions that increase the risk of TB disease, and people with chest radiographs consistent with old, healed prior TB disease.9,20,61
TB Prevention Among PEH
In addition to the treatment of LTBI and inadequately treated prior TB disease, identification of early or active cases, including the use of NAAT for diagnosis, and effective treatment of TB disease are the most important measures for preventing TB transmission.21,22,27,62-65 Staff workers and others who provide services at homeless shelters can assist in case finding by identifying people with productive, persistent cough (ie, lasting ≥3 weeks) and fever and ensuring that PEH with suspected TB disease are quickly evaluated by a health care provider. PEH with suspected TB disease should wear a surgical mask, be instructed to observe cough etiquette, and be transferred to respiratory isolation at a health care facility. 26
Public health departments should conduct thorough contact investigations of every infectious TB case. 66 Location-based investigations are the most successful among PEH, because naming of contacts by PEH often yields few names. 66 Contact investigations are usually based on TST or IGRA testing, followed by chest radiographs for those with TST reactions ≥5 mm or positive IGRA results. Because of the increased risk of TB in congregate settings and the high prevalence of immunosuppression among PEH, and because PEH are unlikely to return for the TST to be read, IGRAs are strongly recommended; however, TSTs are acceptable. 20 Screening PEH for TB using chest radiographs might be useful during outbreak investigations. The anticipated challenges for contact investigations involving PEH include difficulty locating patients and their contacts if they are mobile, have episodic incarceration, migrate between jurisdictions, have psychiatric illnesses (including substance use disorders) that hinder communication or participation, or have preexisting medical conditions (especially HIV). 9
The number and density of people sharing the same breathing space in congregate settings are important factors influencing the likelihood of TB transmission. 5 Supplemental upper room germicidal ultraviolet air disinfection may be useful to reduce ongoing transmission.67-72 Shelter operators can consult with air quality experts to determine the adequacy of ventilation and to obtain recommendations for improvements.
Administrators of shelters for PEH are recommended to undertake the following actions (similar to those for outpatient health care settings) to prevent TB26,73,74: (1) assign responsibility for TB infection control; (2) conduct periodic TB risk assessments; (3) develop and institute a written TB infection control plan to ensure prompt detection, airborne precautions, and treatment of people who have suspected or confirmed TB disease; (4) implement effective work practices for the management of staff and residents with suspected or confirmed TB disease; (5) ensure proper cleaning and sterilization or disinfection of potentially contaminated surfaces; (6) train and educate shelter staff on TB, with a focus on prevention, transmission, and symptom identification; (7) maintain bed maps and track bed assignments, ideally in a searchable electronic format (eg, a spreadsheet) to facilitate contact investigations if a TB case is identified; (8) maintain as much space as possible between beds and position beds head to toe to reduce the possibility of transmission; (9) post signs and informational posters for client awareness and cough monitoring 75 ; (10) use a cough log to document people who are coughing, particularly at night, so that they can be referred for medical evaluation 74 ; and (11) coordinate efforts with the local or state public health department.
A workshop that included TB program staff, health care and social service providers for PEH, other health agency staff, and shelter administrators convened in 2015 and provided input to improve infection control in overnight shelters for PEH. 76 The group stated that addressing stigma (associated with poverty, experiences of discrimination or exclusion, and HIV) is also essential for optimizing TB prevention efforts among PEH. 76
HIV and TB
HIV is a major risk factor for the development of TB disease.77,78 An association among TB disease, HIV, and homelessness has been documented.27,43 The National Alliance to End Homelessness estimated that 3.4% of PEH were HIV positive in 2006, 79 compared with CDC’s estimate of 0.4% of adults and adolescents in the general population 80 or an 8.5 times higher prevalence among PEH than among the general population. Among TB patients with HIV, PEH had higher odds of TB being attributed to recent transmission compared with TB patients not experiencing homelessness. 81 Several studies have shown higher odds of TB-related mortality among people with HIV than among people without HIV.81,82
The annual risk of TB disease due to reactivation of LTBI among people with untreated HIV has been estimated as 3% to 16% per year, which approximates the lifetime risk of TB for people with LTBI who are HIV negative.83,84 The advent of highly active antiretroviral therapy resulted in a reduced incidence of TB disease among people who are HIV positive. 85 Health care providers should implement routine HIV testing of PEH who are suspected to have TB, which can reduce mortality among immunosuppressed patients with TB and HIV if antiretroviral therapy is implemented.86,87
People with HIV are recommended to be tested after diagnosis of HIV and annually if they have TB exposure risk. 78 Among people with HIV, rapid TB diagnosis using NAAT is essential, given the quick clinical progression to TB disease and risk of mortality among patients with advanced immunodeficiency. 78 With increasing immunodeficiency in people with HIV, chest radiographs are often atypical, or TB is extrapulmonary or disseminated, which makes TB diagnosis difficult and further increases the importance of NAAT. 78
Resources
Tables 1 and 2 list current US guidelines and recommendations6,9,20-22,26,28,32,41,43,44,46,61,65,77,86 relevant to TB diagnosis, treatment, and prevention among PEH. We list the recommendations in Table 1 and the recommendation documents chronologically in Table 2. CDC provides information and links to resources for TB programs, homeless shelters, and other service providers for PEH.88,89 CDC-funded Tuberculosis Centers of Excellence for Training, Education, and Medical Consultation (TB COEs) are resources for public health departments and other entities to access expert TB medical consultation for providers caring for PEH. 90 The TB COEs have also developed educational materials and shelter staff training on TB.74,91,92
Summary of recommendations for tuberculosis (TB) diagnosis, treatment, and prevention among people experiencing homelessness (PEH), United States, 2022
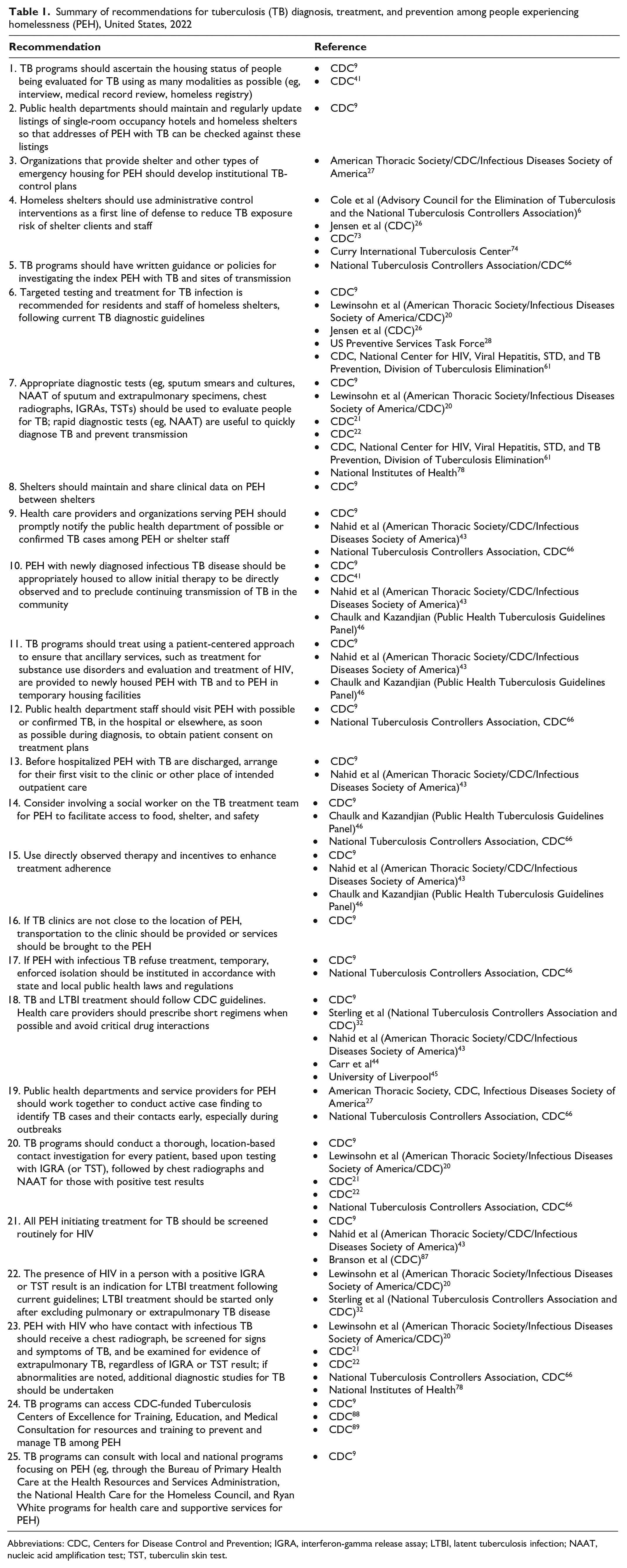
Abbreviations: CDC, Centers for Disease Control and Prevention; IGRA, interferon-gamma release assay; LTBI, latent tuberculosis infection; NAAT, nucleic acid amplification test; TST, tuberculin skin test.
Summary of recommendations for tuberculosis diagnosis, treatment, and prevention among people experiencing homelessness, United States, 2022, in chronological order of publication
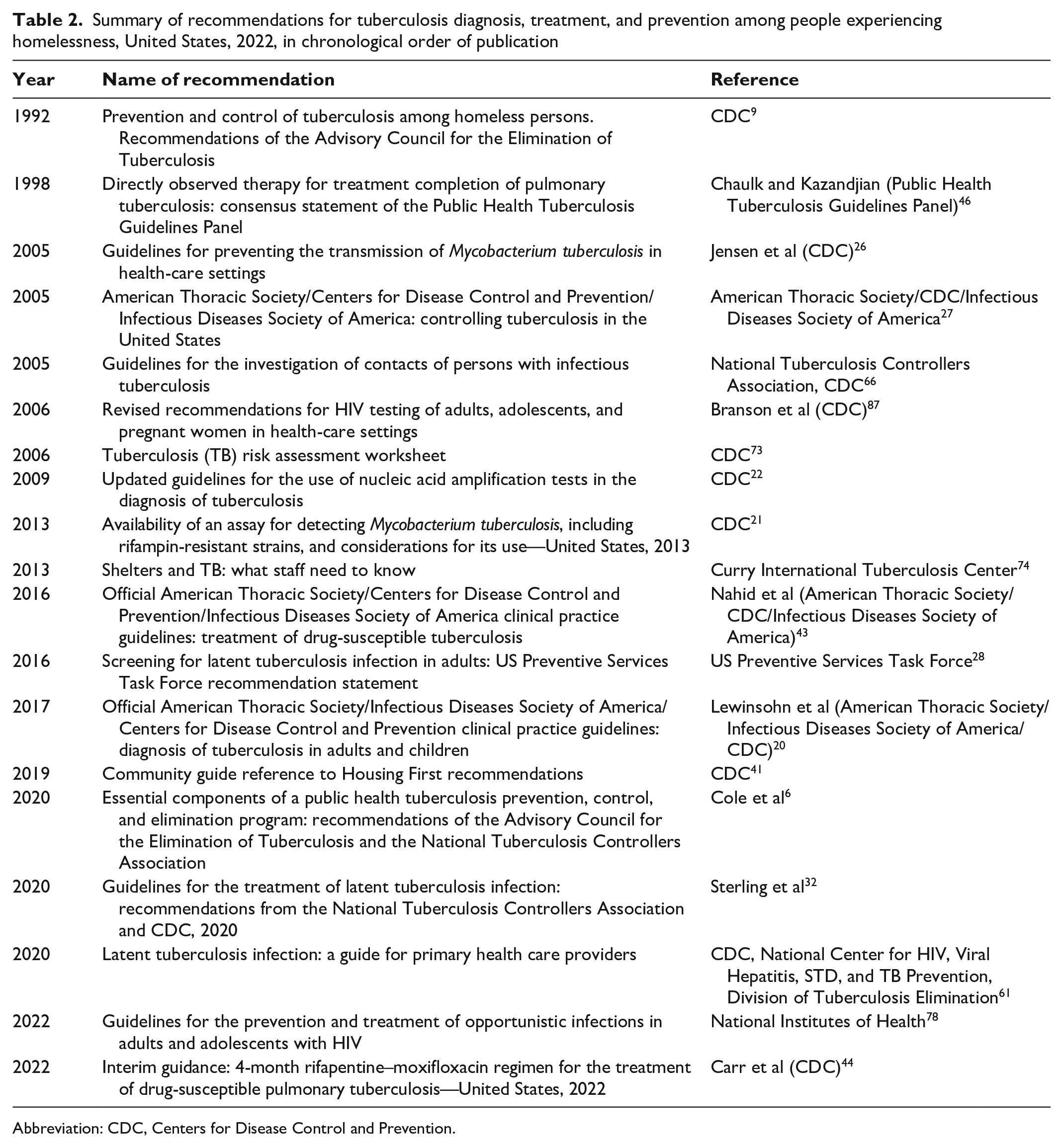
Abbreviation: CDC, Centers for Disease Control and Prevention.
The McKinney Homeless Assistance Act led to a national network of primary health care programs for PEH. 93 Community programs supported by HRSA’s National Health Care for the Homeless Program of the Bureau of Primary Health Care are appropriate partners for public health departments in preventing TB among PEH. 94 The National Health Care for the Homeless Council is a network of >10 000 physicians, nurses, social workers, patients, and advocates providing support to >200 health centers and Health Care for the Homeless programs. The Council provides links to health care resources in each state for PEH. 95 Health care and supportive services are also available for people with HIV through HRSA’s Ryan White Comprehensive AIDS Resources Emergency Act. 96
Discussion
The current US guidelines and recommendations relevant to TB diagnosis, treatment, and prevention call for health care providers serving PEH to (1) assess the magnitude of homelessness in their jurisdictions, (2) test PEH and shelter staff for TB and LTBI and treat those diagnosed using short treatment regimens, (3) identify TB among PEH rapidly through the use of TB diagnostics that can detect TB in 24 to 48 hours, (4) immediately report possible TB among PEH to the local public health department, (5) implement routine HIV testing of PEH who have LTBI or are being evaluated for TB disease, (6) provide temporary housing of PEH during TB treatment and link PEH to opportunities for permanent housing, and (7) conduct location-based contact investigations of infectious cases among PEH.
There is a paucity of recent studies on TB and PEH. More studies are needed to inform best practices in TB diagnosis, treatment, and prevention among PEH.
Recent improvements in health care access through the Affordable Care Act have provided greater health insurance coverage through Medicaid to people with low incomes in 39 US states. 97 These advancements enable greater access to primary health care for PEH, including LTBI testing and treatment. 98
Public Health Implications
PEH disproportionately have chronic and infectious diseases, including TB. Detection, treatment, and prevention of TB among PEH can benefit not only PEH but also society at large. Assessing homelessness among people suspected of having TB, providing housing to PEH with TB during treatment, using short 3- to 4-month regimens for LTBI, and providing directly observed therapy for TB treatment can increase successful treatment of TB among PEH. TB prevention among PEH is challenging but can be achieved.
Footnotes
Disclaimer
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of CDC.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.