
Abstract
Background:
Despite prophylactic pharmacotherapy being ranked as the best intervention yet, poor treatment adherence tempers tuberculosis preventive therapy (TPT) efficacy.
Objectives:
This study aimed to investigate TPT non-adherence among household contacts and its determinants following the rollout of the 3HP regimen in northwest Ethiopia.
Design:
A facility-based multicenter retrospective study was conducted in selected hospitals of northwest Ethiopia from October 17 to February 21, 2024.
Methods:
Target populations were TPT-eligible household contacts (⩽15 years old) based on the national tuberculosis treatment guideline. Univariate and multivariate binary logistic regression model was fitted to identify potential predictors. p-Value < 0.05 was employed to adjudicate the significance level.
Results:
Among 494 household contacts (HHCs) enrolled in this study, 27.94% were non-adherent. Age (5–10 years: adjusted odds ratio (AOR) (95% CI): 1.92 (1.05–3.19); 10–15 years: AOR (95% CI): 2.04 (1.01–4.12)), parental status (AOR (95% CI): 1.87 (1.02–5.24)), comorbidity (AOR (95% CI): 2.92 (1.08–5.69)), poor nutritional status (AOR (95% CI): 1.30 (1.06–2.43)), adverse drug reactions (AOR (95% CI): 4.01 (1.03–8.20)), adherence support (AOR (95% CI): 1.56 (1.08–6.69)) and TPT regimen type (AOR (95% CI): 4.23 (1.85–6.53)) predicts non-adherence.
Conclusion:
Altogether, this study revealed a high level of non-adherence among HHCs in northwest Ethiopia, falling short of the national 2025/26 TPT targets. TPT should be accompanied by firm counseling and routine supervision to improve adherence.
Plain language summary
Tuberculosis (TB) is a serious disease. To stop it from developing in people who have been exposed, a prophylactic therapy is applied. While this medicine is the best available, it only works if people take it as directed. This study looked at the prevalence of TPT non-adherence and its predictors among children and teenagers in northwest Ethiopia. Over one-quarter (27.94%) of the children and teens did not adhere to their preventive treatment. In brief, this study discovered that the following groups had a higher likelihood of not following their treatment plan: Older children and teens (ages 5-15), those who had lost one or both parents, had other comorbid health conditions, with poor nutritional status, experienced adverse drug reactions from the medicine. The specific type of treatment regimen also played a role. This study concludes that the rate of household contact children adherence to TB prevention treatment in northwest Ethiopia is too low to meet national health goals. To mitigate this, clinicians should prefer to initiate 3HP-based TPT with firm counselling to them and their families, and ongoing support and vigilant for ADRs.
Introduction
Tuberculosis (TB) has been recognized as a silent epidemic in children and adolescents recently. 1 There were 10.8 million new TB cases in 2023, of which 12% were children and adolescents (0–14 years). 2 Based on a study by Villavicencio and his colleges approximately 6·5 million children and adolescents (<20 years) died globally in 2021, of which about 3.14% were TB-related. 3
A regional analysis study based on Global Burden of Disease 2021 revealed that Eastern Sub-Saharan Africa had the highest age-standardized incidence rate of TB. 4 The overall prevalence of TB among children and adolescents (0–14 years old) in Ethiopia was 9.35%.5,6
Pediatric patients (younger than 15 years) are at high risk of contracting TB after close contact with an adult household member diagnosed with pulmonary TB (PTB).7–9 The global prevalence of latent TB infection (LTBI) in the general population, according to a systematic review and meta-analysis study by Cohen et al., was 21.2% to 24.8% globally. 10 In addition, an analytical study based on GBD-2019 revealed that the global burden of LTBI was 23.67%. 11 In India, the prevalence of LTBI among pediatric HHCs (<15 years) was 15.4%. In Ethiopia, a study by Smith et al. involving adult diabetic and pre-diabetic HHCs in Addis Ababa revealed that 71% were diagnosed with LTBI. 12 In addition, a study in southern Ethiopia revealed that the epidemiology of active TB among adult household contacts of patients with smear-positive PTB was 6.9% (95% CI 4%–10%). 13 Latent TB infections are the major source of TB disease.14,15
As per the sustainable development goal 3.3.2, established to eradicate infectious diseases such as TB by 2030, preventing it arising from the large reservoir is pivotal.16,17 However, TB preventive therapy (TPT) is often neglected.14,16 Globally, TPT coverage among eligible HHCs, including both children and adults, remained low at 21% in 2023, far below the WHO target of 90% by 2027, indicating a substantial unmet need. 2 Furthermore, fewer than one in five were successfully completed TPT. 14
According to Ethiopian guidelines for clinical and programmatic management of TB, TPT is prioritized for children and adolescents who are HHCs of bacteriologically confirmed PTB cases. 18 In addition, adults and adolescent patients living with HIV who do not report any of the symptoms of current cough, fever, weight loss, or night sweats are unlikely to have active TB and should receive TPT. Despite a significant advancement in its approach in 2018, TPT coverage was 22% among ⩽15 years old HHCs of PTB in Ethiopia.19–21
Non-adherence to TPT among HHCs in Ethiopia is a healthcare concern.22,23 A key strategy used to increase treatment adherence in Ethiopia is initiating TPT with a treatment supporter, in accordance with WHO guidelines. 24 Ethiopia plans to achieve an 80% of TPT completion by 2025/26. 19
Common barriers to TPT adherence include age (2–15 years), 25 female gender, low education and income levels, poor patient acceptance, limited drug access, stigma, undernutrition, 26 inadequate awareness of caregivers,27,28 adverse drug reactions, 29 and regimen types. 30 The World Health Organization (WHO) heralds a new era in TB prevention policy by endorsing the 3HP regimen. 31 Ethiopia was an early adopter of it, since 2018, 32 and rapidly scaled up its implementation by 2020, aiming to improve adherence with a shorter and safer regimen.
Following 3HP, as far as the authors’ knowledge is concerned, no study exists on the initiation and non-adherence rate of TPT in Ethiopia. Consequently, this study evaluates ongoing programs, sheds light on the development of evidence-based policies, and targeted interventional strategies to improve public health outcomes in settings with high TB burden.
Methodology
Study design, setting and period
A multicenter retrospective study was conducted through medical record reviews. It was done in the TB clinics of five public teaching University hospitals of northwest Ethiopia selected purposively (Figure 1). These hospitals serve more than 12 million people in aggregate. They were selected purposively due to their high patient flow and located in urban settings characterized by a dense population.

Study area map employing ArcGIS Pro version 3.4 (Esri; Redlands, California, USA).
Study population
Target population was children and adolescents (<15 years of age) in contact with households of bacteriologically confirmed pulmonary-drug-susceptible TB patients (index cases) and eligible for TPT at those selected hospitals during August 2023 to July 2024. Children and adolescents who were referred to other health facilities and had incomplete medical records were excluded. Five public teaching University hospitals providing TB diagnostic and treatment services in northwest Ethiopia were selected for this study. In those TB clinics’ TB registration book, 878 drug-susceptible PTB index cases were identified. From them, 654 HHC target populations were screened (Figure 2).

Involvement procedure of study participants at TB clinics of teaching University hospitals in Amhara region, Northwest Ethiopia (N = 878).
Study variables
Non-adherence rate to TPT among HHCs was the principal dependent variable. Explanatory variables include sociodemographic, healthcare system, clinical, and treatment-related variables.
Operational definitions
Assessment of TPT adherence status of pediatric HHCs in Amhara comprehensive specialized hospitals, northwest Ethiopia, based on the national TB treatment and control guideline, 2023/24.

6H, 6 months isoniazid; HHC, household contact; 3HP, 3 months isoniazid and rifapentine; 3RH, 3 months rifampicin and isoniazid; TPT, tuberculosis preventive therapy.
Data management
Data collection and quality assurance
To meet our objectives, secondary data were extracted from patient medical records between 17 October and 21 February 2024. Data were gathered by utilizing a standardized data abstraction tool adapted from the Ethiopian Federal Ministry of Health TB clinic intake and follow-up form and from previous literature.20,35-37 Initially, it was pretested in a pilot study at Woreta primary hospital TB clinic on 17 sample medical records. In light of this study, the tool was refined accordingly for clarity and comprehensiveness. Fifteen trained health professionals: five physicians as supervisors, five pharmacists, and five nurses who were experienced in working in TB clinics were selected as data collectors. A 1-day training was given to both supervisors and data collectors. The data retrieval process was closely supervised by strict supervisors, and the overall quality of the data collection was also monitored by the principal and co-investigators. The collected data were checked for completeness and consistency.
Statistical analysis
The data were entered into EpiData version 4.7 and exported to Stata version 17 software (STATA corp., College Station, TX, USA) for analysis. The study participants were characterized using descriptive statistics using measures such as frequency, percentage, and mean value with standard deviation were all included in this analysis.
At last, adherence status to TPT was dichotomized into adherent or nonadherent. The bivariable logistic regression model was fitted for each potential predictor variable. Moreover, those variables having a p-value ⩽0.25 in bivariate analysis were fitted into a multivariable logistic regression model to control the impact of confounders. Adjusted odds ratios with 95% confidence intervals and p-values were used to measure the strength of association and to identify statistically significant determinants. Factors were deemed significantly associated with the outcome variable if their p-values were <0.05 at 95% confidence interval. The Shapiro-Wilk normality test revealed that our data were not normally distributed. The model’s fitness was verified using the Hosmer-Lemeshow goodness-of-fit test and it revealed that the model was adequately fit (p-value = 0.07). The variance inflation factor (VIF) was used to diagnose the presence of multicollinearity among predictor variables. There is no collinearity among the independent variables in the model, as seen by the mean VIF of 2.33. The discriminative ability of this model was assessed employing c-statistics, revealing that 81% of children and adolescents were correctly classified into adhering versus non-adhering (c statistic = 0.81).
Furthermore, upon performing an in-depth expert review, some factors might be included in the multivariate analysis even though their p-value was above the cut-point value in bivariate analysis based on existing knowledge and evidence.
Results
Tuberculosis preventive therapy pathway of care
Upon a retrospective clinical audit on the TB clinic contact investigation registration book, a total of 2250 HHCs were claimed from 502 index cases. The mean age of HHCs was 31.9 years (standard deviation 5.31). Among the total HHCs identified, 654 were declared eligible for TPT. Of them, 493 were asymptomatic, whereas 161 were symptomatic. Five hundred forty one (82.72%) of them were successfully initiated TPT (Figure 3).
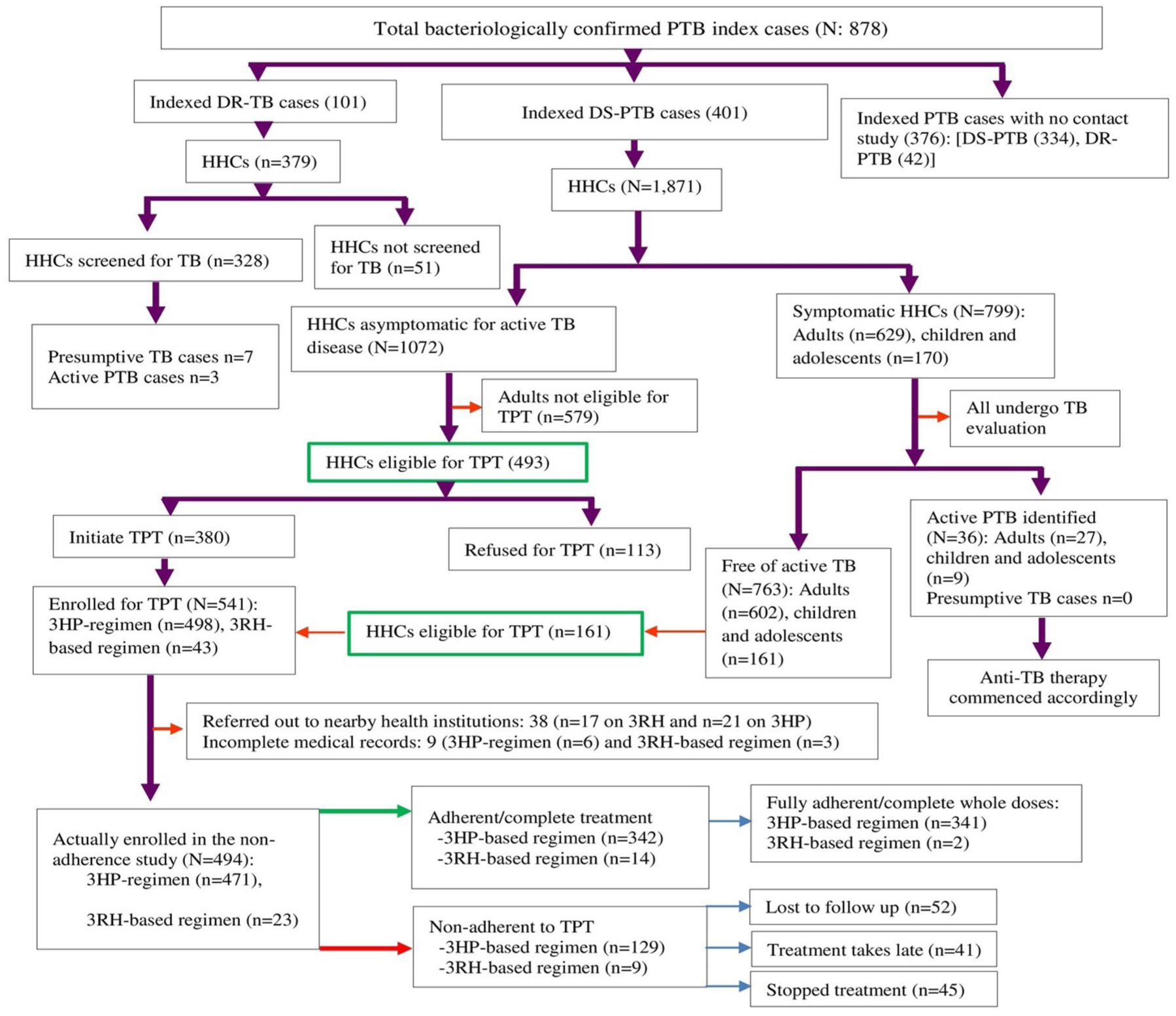
LTBI care pathway: screening and TPT enrollment among pediatric HHCs in Amhara comprehensive specialized hospitals, northwest Ethiopia, 2023/24 (n = 494).
Healthcare system and sociodemographic-related features of participants in non-adherence study
Among 541 HHCs initiating TPT, only 494 have been enrolled in the non-adherence study due to incomplete medical records and referral to other health institutions. The majority of the study participants were females (59.31%), 5–10 years old (48.78%), and had attained only a primary school level of education (65.38%). Furthermore, 29 (5.87%) children and adolescents in the study population were identified as orphanhood. A little over half (51.21%) of the caregivers do not have formal education (Table 2).
Sociodemographic profile of pediatric household contacts on TPT with their caregivers and healthcare system-related features in Amhara comprehensive specialized hospitals, northwest Ethiopia, 2023/24 (N = 494).

Guragie, Afar.
CBHI, community-based health insurance; TPT, tuberculosis preventive therapy; HHC, household contact.
Clinical profile of the study population
Almost a quarter of children and adolescents did not have a history of Bacillus Calmette-Guérin (BCG) vaccination. More than a quarter 181 (36.64%) of them had poor nutritional status. Comorbidities, primarily central nervous system disorders led by attention deficit hyperactivity disorder (ADHD), were observed in 4.25% (n = 21) of contacts. Adverse drug reaction (ADR) occurrence rate in these patients was high, 26.52% (n = 131), where flu-like cutaneous reactions were the predominant (Table 3).
Clinical characteristics of pediatric HHCs on TPT in Amhara comprehensive specialized hospitals, northwest Ethiopia, 2023/24 (N = 494).

Attention deficit hyperactivity disorder, Autism Spectrum Disorder, and Epilepsy. bGIT disorders and Cancer.
ADR, adverse drug reaction; BCG, Bacillus Calmette-Guérin; HHC, household contacts; TPT, tuberculosis preventive therapy.
Adherence status to TB preventive treatment
Non-adherence to TPT among children and adolescents was 27.94% (138/494). The non-adherence rate was higher among the 3RH regimen, 39.13% (9/23), than among HHCs who were on 3HP, 27.39% (129/471). Among children and adolescents on TPT, 343 (69.43%) achieved full adherence by completing all doses. HHCs on the 3HP regimen has higher rate of completing TPT fully (341/471 = 72.4%) as compared to HHCs on the 3RH regimen (2/23 = 8.7%; Figure 3).
Regarding treatment retention rate per each dose of TPT, the maximum number of participants who lost their treatment was during tenth week of therapy (n = 83; Figure 4).
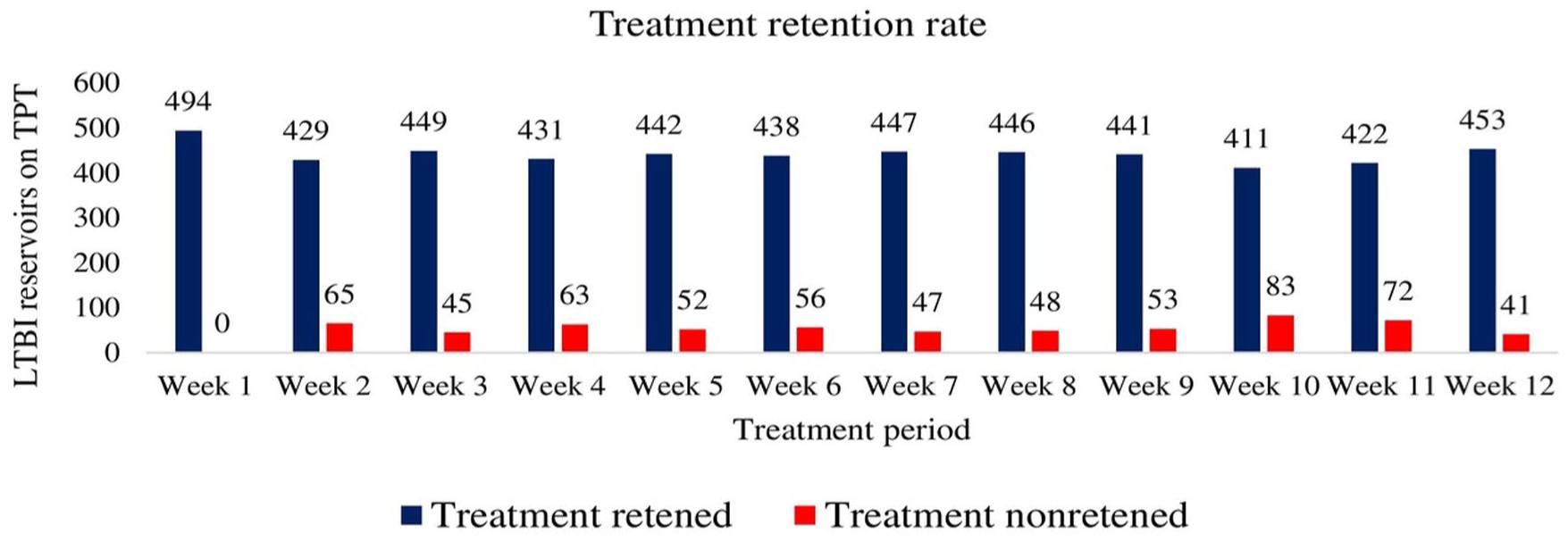
Weekly treatment retention rate among pediatric household contacts by dose in Amhara comprehensive specialized hospitals, northwest Ethiopia, 2023/24 (N = 494).
Adverse drug reaction profile of household contacts
Six hundred seventy-three ADRs were reported from 131 HHCs. The causality, severity, and preventability data of ADRs were not found. ADR occurrences in this study have been classified into six main types. Cutaneous ADRs were hypersensitivity reactions revealing angioedema, urticaria, rash, pruritus, and potentially life-threatening anaphylaxis during treatment. Flu-like symptoms encompass fever, chills, weakness, fatigue, muscle pain, aches, syncope, tachycardia (>100 bpm), palpitations, hypotension, flushing, dizziness, conjunctivitis (red eyes), or excessive sweating. Gastrointestinal ADRs include vomiting (with or without nausea) or abdominal pain. Respiratory ADRs include bronchoconstriction, cough, dyspnea, or chest pain, where presumptive TB was ruled out. Among 673 ADRs, 41.75% (281), 40.56% (273), 6.24% (42), 4.61% (31), 3.57% (24), and 3.27% (22) were flu-like symptoms, cutaneous, gastrointestinal, neurological, hepatotoxic, and respiratory ADRs, respectively. Seven participants discontinued TPT due to flu-like symptoms (n = 2), peripheral neuropathy (n = 1), and hepatotoxicity (n = 4). Among individuals who developed hepatotoxicity, 83.3% (10 of 12) were non-adherent to TPT (Figure 5).

Impact of adverse drug reactions on TPT adherence among pediatrics in Amhara comprehensive specialized hospitals, northwest Ethiopia, 2023/24 (N = 494).
Factors associated with non-adherence
In the multivariate analysis, factors with a p-value ⩽ 0.25 in the univariate analysis were qualified for and included. In addition, gender was incorporated into the multivariate analysis despite its p-value exceeding the cutoff, as previous studies identified it as a significant determinant factor of non-adherence to TPT.29,38,39 Explanatory variables such as age, relationship of children with caregiver, parental status, drug stock-out, commorbidity, ADR experience, regimen type, lack of adherence support, and poor nutritional status were significantly associated with non-adherence, and the odds were in the predicted direction. The association between regimen type and ADR with non-adherence was clear-cut. Patients who were on 3RH (AOR (95% CI): 4.23 (1.85–6.53)) and experienced ADR (AOR (95% CI): 4.01 (1.03–8.20)) were four times more likely to have failed to adhere to their medication compared to their counterparts. Among all types of ADRs, patients who revealed neurological reactions (AOR (95% CI): 6.1 (1.23–8.20)) and hepatotoxicity (AOR (95% CI): 7.2 (1.26–9.04)) were at a higher odds of being non-adherent to TPT (Table 4).
Multiple logistic regression analysis of factors associated with non-adherence to TPT among pediatrics in Amhara comprehensive specialized hospitals, northwest Ethiopia, 2023/24 (N = 494).

ADR, adverse drug reaction; aOR, adjusted odds ratio; CM, complementary medicine; ETB, Ethiopian birr; GP, general practitioner; LTBI, latent TB infection; OR, odds ratio; Ref, reference category; TPT, TB preventive therapy.
Discussion
Several preventive measures are employed, yet preventive pharmacotherapy ranked as the best intervention.40,35 However, non-adherence tempers TPT program efficacy. 41 In this study, among TPT eligibles, 82.72% initiated TPT. Despite failing to attain the national strategic plan by 2025/2026 (90%), 19 it corroborates an earlier study conducted in Ethiopia20,42-44 and Sub-Saharan Africa, such as Rwanda and Eswatini.45,46
Among the participants in the study, 27.94% were non-adherent, indicating a failure to meet the strategic goal. 19 However, this study’s finding was in accordance with earlier studies in Ethiopia.23,36 This finding also fairly aligns with an earlier study in Mozambique. 47
Herein, multiple variables predict non-adherence. Compared to HHCs under five, those older than five had a roughly twofold-increased odds of developing non-adherence to TPT. The results of this investigation mirror those of previous studies in Ethiopia, 25 and Cambodia. 42 This may be due to the fact that school-aged children are more prone to non-adherence due to a lack of firm adherence support from parents/caregivers. 48 In the contrary, a cross-sectional study in China reported that age failed to reach statistical significance threshold. 30 This discrepancy might be due to the involvement of adolescents and adults (14–52 years old), differences in TPT regimen type and study area.
This study revealed that being orphanhood increases the risk of non-adherence, possibly due to a lack of strong social support.43,44 Furthermore, child contacts whose caregivers were guardians/neighbors were twice as likely to have failed to adhere as compared to those cared for by biological relatives. In the Ethiopian context, TPT was conducted as a self-administered therapy. Therefore, biologic-relative adherence supporters achieves higher rate of adherence than their counterparts.
Chronic comorbid illnesses predict TPT non-adherence in agreement with earlier studies.49,50 This may be potentially due to the medication regimen complexity associated with the treatment of comorbidities. Poor nutritional status was also found to be a pertinent risk factor in agreement with previous studies.26,51 On the contrary, earlier studies involving patients with LTBI reported that nutritional status failed to reach a statistically significant level.30,52 This may be due to differences in study design and patients’ age group.
HHCs on the 3RH regimen were more likely to have failed to adhere than those who were on the 3HP regimen. This study finding mirrors an earlier study in Ethiopia. 25 In addition, a study in Cambodia reported that individuals who initiated 3RH or 6H were more likely to not complete the treatment compared to those on 3HP. 42 This may be due to the medication regimen complexity and treatment burden with 3RH and 6H regimens.
Children experiencing ADRs were found to have a higher odds of treatment non-adherence, consistent with other studies. 53 Among all types of ADRs, patients who revealed neurological reactions and hepatotoxicity were at a higher odds of being non-adherent to TPT in line with the earlier studies. 54 This may be due to the development of a negative attitude toward the medications as they experienced TPT-related ADRs. 55 In contrast, a study in a similar setting revealed that ADR experience was not associated with non-adherence. 56 This might possibly be due to a target population discrepancy. Finally, drug stock-out was also predict TPT non-adherence. A study in rural Delhi revealed that the primary reason for non-adherence to TPT among HHCs was the unavailability of medicine. 57
Strength and limitation of the study
Our study has several limitations. In the first place, purposive hospital selection and exclusion of participants due to referral and incomplete medical records may affect the study’s integrity. However, this is considered a low risk due to the relatively small size of the excluded group, and their characteristics were less likely to be systematically different. Despite this study trying to incorporate multiple potential predictors, it might be affected by unmeasured variables due to its retrospective nature. Although there are methodological limitations, following the adoption of the 3HP-based regimen in Ethiopia this study is the first of its kind.
Conclusion and recommendations
Non-adherence among HHCs to TPT was alarmingly high in the study area, indicating a failure to achieve the strategic plan set by Ethiopia for 2025/2026. It remains the program’s concern despite the introduction of rifamycins-based 3HP-regimen into the Ethiopian TPT algorithm.
To mitigate TPT non-adherence in the study area, the government should set focused policies on curbing risk factors. This includes access to healthcare institutions and medications, improving nutritional status, and clinicians should prefer to initiate 3HP-based TPT accompanied with firm counseling, supervision, and vigilance for ADRs. Altogether, special emphasis should be given to those who were school-aged children, orphans, comorbid, malnourished, and ADR experienced, considering them as vulnerable groups.
Supplemental Material
sj-docx-1-tai-10.1177_20499361261426969 – Supplemental material for Non-adherence and its predictors among pediatric household contacts on tuberculosis preventive therapy in the 3HP era: A multicenter observational study
Supplemental material, sj-docx-1-tai-10.1177_20499361261426969 for Non-adherence and its predictors among pediatric household contacts on tuberculosis preventive therapy in the 3HP era: A multicenter observational study by Woretaw Sisay Zewdu, Muluken Adela Alemu, Tilaye Arega Moges, Sisay Sitotaw Anberbr, Desalegn Addis Mussie, Abel Temeche Kassaw, Demewoz Kefale, Tigabu Eskeziya Zerihun, Fisseha Nigussie Dagnew and Samuel Berihun Dagnew in Therapeutic Advances in Infectious Disease
Footnotes
Acknowledgements
The authors would like to thank the data collectors, the hospitals, and the respective TB clinic staffs.
Declarations
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.