
Abstract
Objective:
Medicare beneficiaries in rural areas may face challenges in access to dental care. This study assessed rural–urban differences in the use of dental services and dental procedures by Medicare beneficiaries.
Methods:
We obtained data from the 2018 Medicare Current Beneficiary Survey cost and use files. Outcome variables examined in this study were (1) dental visits (yes/no), whether the Medicare beneficiary had ≥1 dental visit in the past year, and (2) dental procedures—preventive (yes/no), restorative (yes/no), and surgical procedures (yes/no)—whether the beneficiary had the procedure in a dental visit. The independent variable was the beneficiary’s residence (rural vs urban). We used multiple logistic regression to analyze data and accounted for the survey design of the Medicare Current Beneficiary Survey. The analytic sample included 7377 respondents aged ≥65 years.
Results:
Approximately 57.0% (95% CI, 54.9%-59.0%) and 46.4% (95% CI, 41.6%-51.2%) of Medicare beneficiaries in urban and rural communities in the United States had a dental visit in 2018, respectively. Rural beneficiaries were significantly less likely than their urban counterparts to have preventive procedures (adjusted odds ratio = 0.51; 95% CI, 0.36-0.72) but significantly more likely to have restorative procedures (adjusted odds ratio = 1.30; 95% CI, 1.05-1.62).
Conclusion:
We found significant disparities in use of dental services by Medicare beneficiaries in rural communities. When Medicare beneficiaries in rural areas used dental care, they were less likely than beneficiaries in urban areas to have preventive procedures but more likely to have restorative procedures, suggesting a greater burden of oral health needs among them. Policy research is needed to identify models that can incentivize prevention and improve access to dental care for Medicare beneficiaries in rural communities.
Traditional Medicare does not provide dental benefits except under limited circumstances, such as during hospitalization when dental care is an integral part of a covered procedure (eg, reconstruction of the jaw following accidental injury) or for extractions done in preparation for radiation treatment for neoplastic diseases involving the jaw. 1 The lack of dental coverage, combined with low income for more than half of Medicare beneficiaries, puts adults aged ≥65 years at risk for oral health problems, including tooth decay, periodontal disease, and tooth loss, which could be prevented or treated with timely dental care.2,3 For Medicare beneficiaries in rural areas, access to dental services is an important policy issue.4-6
Rural–urban disparities in utilization of health care services,7,8 including dental services,5,9-11 have been documented. Prior research12,13 examined utilization of dental services and procedures by Medicare beneficiaries before 2006. However, the rural–urban gap in patterns of dental visits has not been assessed recently. Specifically, utilization of various types of dental services by beneficiaries in rural areas is not well known. Beneficiaries in rural areas may be more likely to see a dentist to treat an oral health problem (eg, restorative care or tooth extraction) than for routine preventive care (eg, dental cleaning). Thus, type of dental service (eg, preventive vs treatment procedures) can be an indicator of quality of care.14,15 To date, no studies have assessed rural–urban differences in the types of dental procedures utilized by Medicare beneficiaries.
This study aimed to assess rural–urban disparities in dental visits and types of dental services utilized by Medicare beneficiaries. We used Andersen’s Behavioral Model of Health Services Utilization as the conceptual framework, which has been used to identify facilitators and barriers to health care. The model proposes that the use of health services is associated with 3 factors: predisposing characteristics, enabling factors, and health needs.16,17 Our study provides important information for the current debate on improving access to dental care for Medicare beneficiaries.
Methods
Data were from the 2018 Medicare Current Beneficiary Survey (MCBS). 18 The MCBS is a continuous annual series of nationally representative surveys conducted by the Centers for Medicare & Medicaid Services (CMS) of Medicare beneficiaries aged ≥65 years and people aged <65 years but eligible for Medicare because of certain disabilities or conditions (eg, end-stage renal disease). It collects information about the beneficiary, including demographic characteristics, health status and functioning, access to care, health insurance coverage, costs, and out-of-pocket expenses. In this analysis, data for dental procedures were from the Dental Events segment in the 2018 Cost Supplement File; data for total number of dental visits were from the Service Summary segment. Details of the MCBS can be found elsewhere. 18 We limited the study sample to community-dwelling people aged ≥65 years who were enrolled in Medicare during the entire year (ie, 365 days) of 2018 and whose data on dental service utilization were available. The analytic sample included 7377 participants. Because the data used in this analysis are in the public domain, the study was exempted from institutional review board review.
Measurement
Outcome Variables
The outcomes examined in this study were dental visits and dental procedures. We extracted data for the total number of dental visits from the 2018 MCBS Cost Supplement File. In this analysis, we treated this variable as a binary outcome—whether the Medicare beneficiary had a dental visit in the past year (yes, ≥1 dental visit; no, no dental visit). For dental procedures, the 2018 MCBS asked participants about the dental procedures they had in a dental visit, including the following categories: dental examination, cleaning, x-ray, fluoride treatment, sealants, fillings, inlays, crowns, root canal, periodontal procedure, periodontal recall visits, extraction, implants, abscess/infection treatment, surgery, bridges, dentures, denture/bridge repair, orthodontia, bonding/whiten/bleach, treatment for temporomandibular disorders/temporomandibular joint, and other.
Following prior research, 19 we categorized these procedures as follows: diagnostic procedures (examination and radiographs), preventive procedures (cleanings, fluoride treatments, dental sealants, and recall visits), restorative (fillings and inlays), oral surgery (oral surgery and extraction), prosthetic (crowns, bridges, fixed and removable dentures, denture repairs, and dental implants), periodontic (periodontal services only), endodontic (root canal), orthodontic, and other procedures (abscess/infection treatment, bonding/whiten/bleach, treatment for temporomandibular disorders/temporomandibular joint, and other). All were assessed as binary outcomes (yes/no).
We conducted bivariate analyses for the 9 procedures to assess rural–urban differences. We conducted multivariate model analyses for only 3 procedures: preventive, restorative, and oral surgery. We did not conduct model analyses for diagnostic procedures because they are often provided before other procedures in a dental visit. For other procedures, we conducted no model analyses because of small sample sizes and/or nonsignificant bivariate analysis results in rural–urban comparisons.
Independent Variable
The independent variable in this analysis was participants’ residential location, an enabling variable, classified as rural or urban by the county of residence of Medicare beneficiaries. The measure for rurality is provided in the MCBS demographics segment and used the Core-Based Statistical Area designations according to the definition of rurality by the Office of Management and Budget. 18
Covariates
We selected covariates according to Andersen’s Behavioral Model of Health Services Utilization16,17 and prior research on the topic.12,13 Andersen’s model proposes that the use of health services is associated with 3 factors: predisposing characteristics, enabling factors, and health needs. Predisposing characteristics are factors that may predispose people to use health services. Enabling factors refer to factors that facilitate health services utilization. Health needs are related to the perceived health conditions of the individual.16,17 Predisposing factors include age (categorized as 65-74, 75-84, and ≥85 years), sex, race and ethnicity (non-Hispanic White, non-Hispanic Black, Hispanic, and “other” [American Indian/Alaska Native, Asian, other racial groups, and unknown]), and marital status (married and not married). Enabling factors include education level (<high school, high school, some college, and ≥college), income level relative to the federal poverty level (FPL; ≤135%, 136% to ≤200%, and >200% FPL), and participation in a Medicare Advantage plan (yes/no). We used self-rated health status (excellent, good/very good, and poor/fair) as the factor for health need.
Statistical Analysis
We used descriptive statistics to characterize 2018 MCBS participants by rural–urban residence. We conducted Pearson χ2 tests to assess differences in the prevalences of the 9 dental procedures used by rural and urban Medicare beneficiaries. We ran 4 multiple logistic regression models to assess rural–urban differences in having ≥1 dental visit (model 1) and preventive (model 2), restorative (model 3), and surgical (model 4) procedures, controlling for other covariates. We conducted all analyses using Stata version 14.0 (StataCorp LLC) and accounted for the complex survey design of MCBS. We set significance at P < .05.
Results
The proportion of Medicare beneficiaries who were aged ≥75 years, were non-Hispanic White, self-reported health status as poor/fair, had less than a college education, and had a family income ≤135% FPL was higher among rural than among urban Medicare beneficiaries, and a smaller proportion of rural than among urban beneficiaries had Medicare Advantage plans (all P < .05) (Table 1).
Characteristics of Medicare beneficiaries (N = 7377) participating in the Medicare Current Beneficiary Survey, overall and by rural–urban county residence, United States, 2018 a
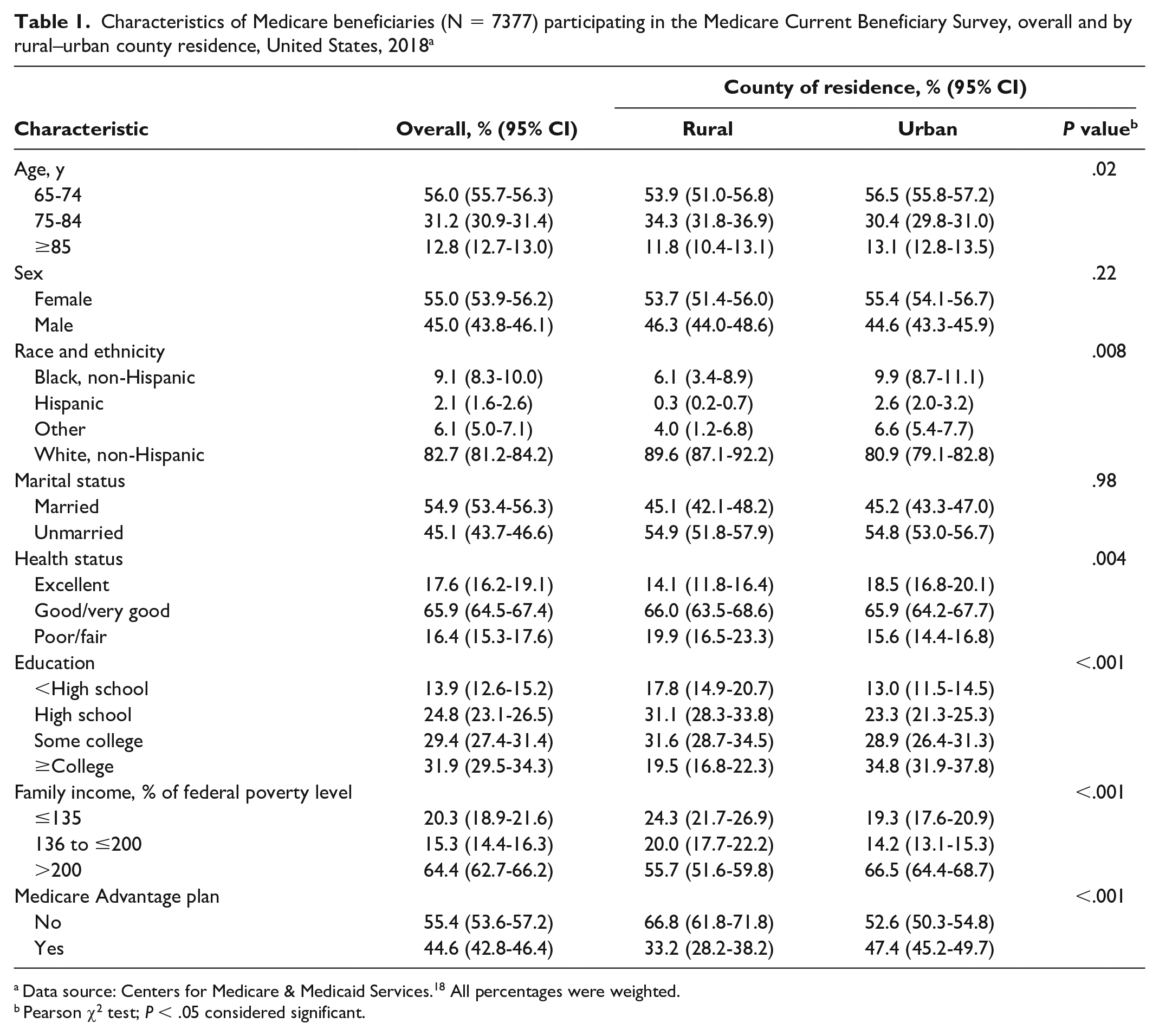
Data source: Centers for Medicare & Medicaid Services. 18 All percentages were weighted.
Pearson χ2 test; P < .05 considered significant.
In 2018, approximately 54.9% (95% CI, 53.2%-56.6%) of Medicare beneficiaries had ≥1 dental visit in the past year; the prevalence was lower in rural areas than in urban areas (46.4% vs 57.0%; P < .001) (Table 2). Among Medicare beneficiaries who had ≥1 dental visit in the past year, 82.9% (95% CI, 81.2%-84.7%) had preventive dental procedures; the prevalence was lower in rural areas than in urban areas (74.3% vs 84.6%; P < .001). Approximately 82.3% (95% CI, 80.2%-84.3%) had diagnostic procedures and, similarly, the prevalence was lower in rural areas than in urban areas (74.6% vs 83.8%; P < .001).
Weighted prevalence of having ≥1 dental visit and dental procedures among Medicare beneficiaries participating in the Medicare Current Beneficiary Survey, overall and by rural–urban location, United States, 2018 a
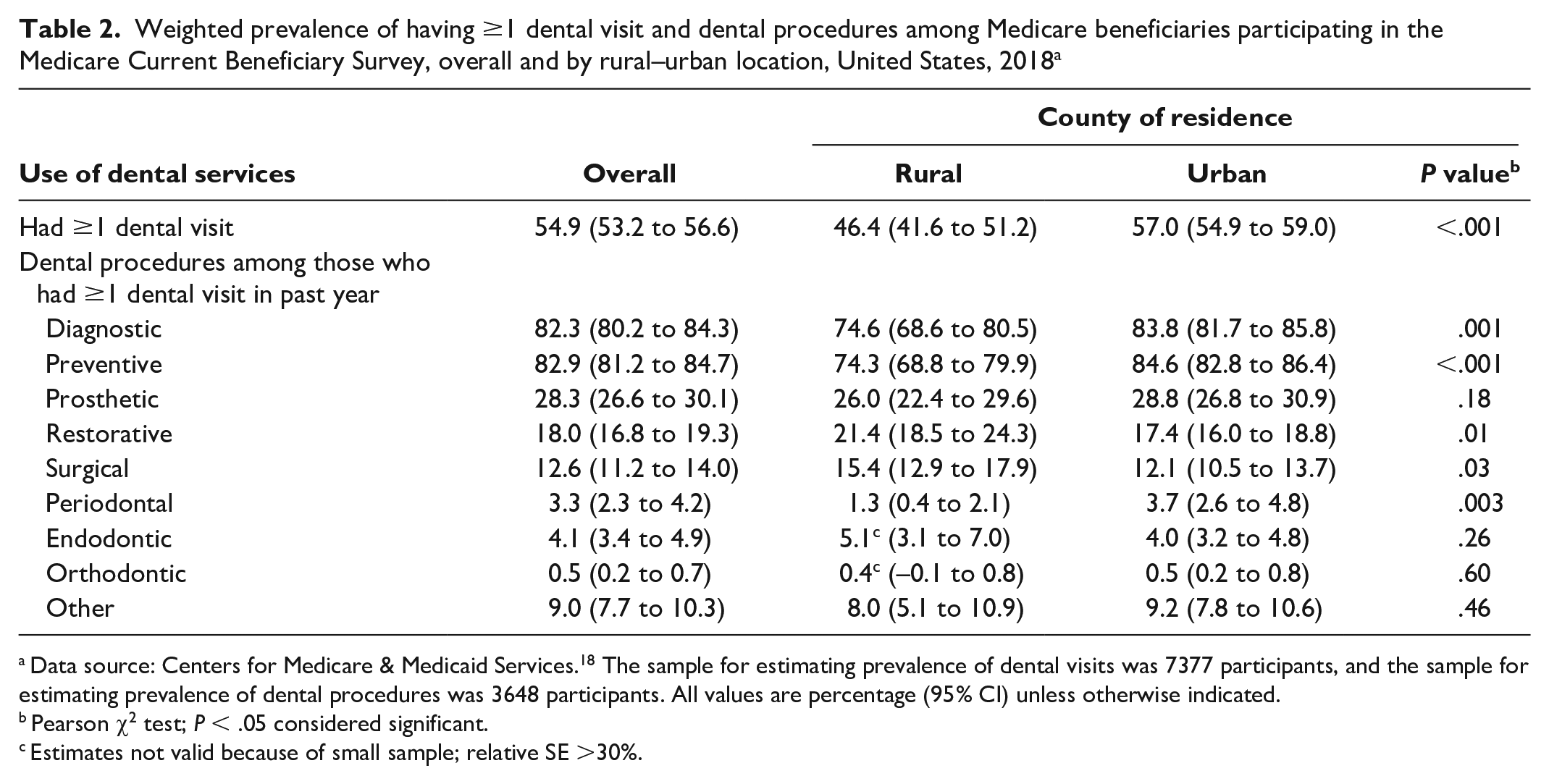
Data source: Centers for Medicare & Medicaid Services. 18 The sample for estimating prevalence of dental visits was 7377 participants, and the sample for estimating prevalence of dental procedures was 3648 participants. All values are percentage (95% CI) unless otherwise indicated.
Pearson χ2 test; P < .05 considered significant.
Estimates not valid because of small sample; relative SE >30%.
For other dental procedures, the highest prevalence was for prosthetic procedures (28.3%), followed by restorative (18.0%), surgical (12.6%), endodontic (4.1%), periodontal (3.3%), and orthodontic (0.5%) procedures. The prevalence was higher in rural areas than in urban areas for restorative procedures (21.4% vs 17.4%; P = .01) and surgical procedures (15.4% vs 12.1%; P = .03) but lower for periodontal procedures (1.3% vs 3.7%; P = .003). In addition, a higher proportion of beneficiaries in rural areas than in urban areas had endodontic procedures, but the estimate for rural beneficiaries was not valid because the small sample size resulted in relative SEs >30%.
In model 1 of the logistic regression, Medicare beneficiaries in rural areas were less likely than those in urban areas to have ≥1 dental visit (adjusted odds ratio [aOR] = 0.77; 95% CI, 0.62-0.95). Women (aOR = 1.71; 95% CI, 1.48-1.99) and beneficiaries who were married (aOR = 1.64; 95% CI, 1.43-1.87) were more likely to have ≥1 dental visit than men and beneficiaries who were not married, respectively. Non-Hispanic Black beneficiaries (aOR = 0.59; 95% CI, 0.46-0.76) were less likely than non-Hispanic White beneficiaries to have ≥1 dental visit. Beneficiaries with more than a high school education (vs <high school) and income levels ≥136% FPL (vs ≤135% FPL) were significantly more likely to have ≥1 dental visit (both P < .001). Self-reported health status was a significant factor: beneficiaries with less-than-excellent self-rated health were less likely than those reporting excellent health to have ≥1 dental visit.
In model 2, beneficiaries in rural areas were less likely than those in urban areas to have preventive dental procedures (aOR = 0.51; 95% CI, 0.36-0.72) (Table 3). Non-Hispanic Black beneficiaries were less likely than non-Hispanic White beneficiaries to have preventive dental procedures (aOR = 0.56; 95% CI, 0.34-0.95). Beneficiaries with income ≥136% FPL were more likely than those with income ≤135% FPL to have preventive dental procedures (P < .001). Other significant variables were female sex and self-reported health status (all P < .01).
Results of logistic regression models to assess rural–urban differences in having ≥1 dental visit and 3 dental procedures among Medicare beneficiaries participating in the Medicare Current Beneficiary Survey, United States, 2018 a
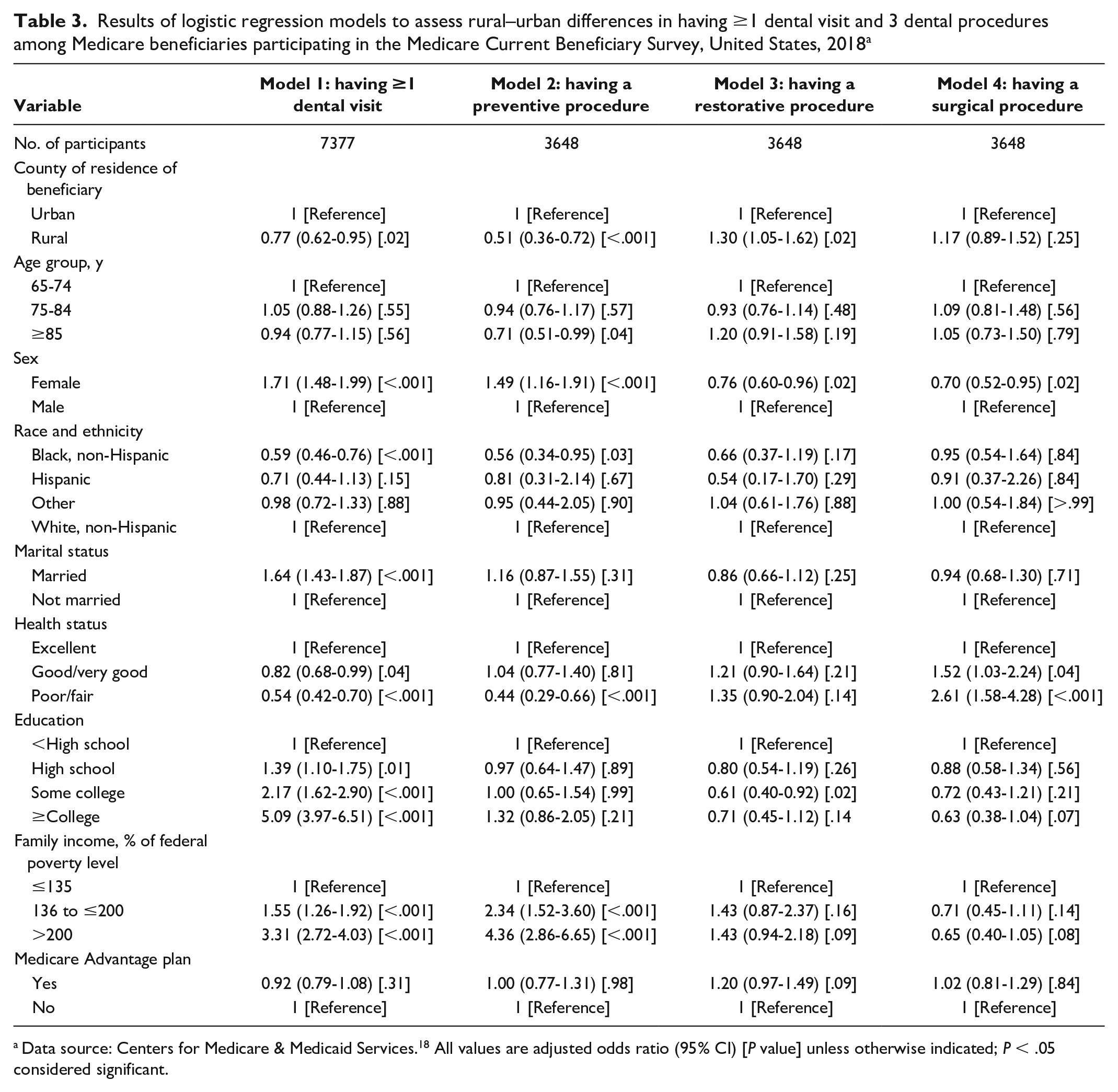
Data source: Centers for Medicare & Medicaid Services. 18 All values are adjusted odds ratio (95% CI) [P value] unless otherwise indicated; P < .05 considered significant.
In model 3, beneficiaries in rural areas were more likely than those in urban areas to have restorative procedures (aOR = 1.30; 95% CI, 1.05-1.62). Women were less likely than men to have restorative procedures (aOR = 0.76; 95% CI, 0.60-0.96). Beneficiaries with some college were less likely than those with less than a high school education to have restorative procedures (aOR = 0.61; 95% CI, 0.40-0.92). Finally, in model 4, we found no significant rural–urban difference in having surgical procedures. Women were less likely than men to have surgical procedures (aOR = 0.70; 95% CI, 0.52-0.95). Self-reported health status was also a significant variable.
Discussion
To our knowledge, no studies have assessed dental service utilization among Medicare beneficiaries since the study by Skaar and O’Connor, 13 which analyzed MCBS data for 1998-2006 and reported that 46.3% of beneficiaries had ≥1 dental visit in 2006. Our study, which analyzed MCBS data for 2018, found that 54.9% of beneficiaries had ≥1 dental visit. In addition, we found that Medicare beneficiaries in rural areas were less likely than those in urban areas to have ≥1 dental visit, and if they did have a dental visit, they were less likely to have preventive dental procedures but more likely to have restorative procedures than those in urban areas.
The 2018 MCBS data showed a gap of 10 percentage points between beneficiaries in rural and urban areas in having ≥1 dental visit. These findings are different from those in an analysis of 2016 Medical Expenditure Panel Survey data, which did not show significant differences in dental visits among adults aged ≥18 years in rural, suburban, and urban areas. 9 The different study design and study population of that analysis limit a direct comparison with our study. Still, the results from the 2018 MCBS data suggest that Medicare beneficiaries in rural areas might face greater barriers than adults aged <65 years (ie, non–Medicare beneficiaries) in access to dental services. Future research is needed to monitor rural–urban disparities in dental utilization by Medicare beneficiaries.
Lack of dental providers in rural areas may account for our findings. Approximately 37 million people in the United States reside in rural or partially rural areas designated by the Health Resources & Services Administration as Dental Health Professional Shortage Areas. 20 Only 11% of practicing dentists served rural or partially rural communities in 2018. 21 In addition to the lack of providers, other factors include rural beneficiaries not prioritizing oral health as a result of competing needs, such as food insecurity among those with low socioeconomic status, 22 as well as limited health literacy 22 or negative attitudes toward dental services and perceived lack of need.23,24 Lack of transportation could be another barrier. 25 Strategies have been proposed to address limited access to dental care in rural communities. For example, teledentistry has been shown to be an effective way of providing oral health services in Dental Health Professional Shortage Areas.26,27 In addition, several government agencies have suggested that integrating dental care with primary care can help address many oral health disparities, particularly in rural populations. 28 The use of midlevel dental providers (eg, dental therapists)29,30 has also been proposed to increase access to care for rural residents.
Dental insurance is a key enabling factor for access to dental services.31,32 Recent estimates by the Kaiser Family Foundation showed that nearly half of Medicare beneficiaries (47%) do not have dental insurance coverage. 33 Medicare beneficiaries have substantial costs for dental, hearing, and vision services. 34 Some Medicare Advantage plans are designed to address this gap in traditional Medicare, and nearly 26% of Medicare beneficiaries are estimated to have opted for a plan that may offer some form of dental benefit. 33 Nearly all Medicare Advantage enrollees with access to dental coverage have preventive dental care benefits, including oral examinations, cleanings, dental x-rays, and sometimes fluoride treatments. 33 However, our analysis did not find that enrollment in Medicare Advantage plans contributed to use of dental services. Several factors may account for our results. In addition to a lack of providers and dental services not being the priority for some Medicare beneficiaries, another reason could be cost sharing for other nonpreventive services. A limit on the number of dental visits per year and an annual cap on payments in Medicare Advantage plans may also present barriers to accessing dental services. Of note, our results also showed that beneficiaries in rural areas were less likely than those in urban areas to have Medicare Advantage plans. More research is needed to assess the impact of Medicare Advantage plans on dental care access in rural areas.
Our study showed substantial disparities in dental procedures. Compared with beneficiaries in urban areas, beneficiaries in rural areas were about 10 percentage points lower in having preventive procedures and 4 percentage points higher in having restorative procedures. These findings are consistent with those in our earlier study, which found that adults in rural areas were less likely than adults in urban areas to have received preventive dental procedures.9,10 In addition, we found significant differences in our present bivariate analysis, with beneficiaries in rural areas being more likely than those in urban areas to have surgical procedures but less likely to have periodontal procedures. Taken together, these findings suggest poor oral health status and poor quality of dental care among Medicare beneficiaries in rural communities: they may seek dental care only when they have dental problems. That is, poor oral health status necessitated a dental visit.
Among all the treatment procedures, the most common was prosthetic procedures (including crowns, bridges, fixed and removable dentures, denture repairs, and dental implants). This finding provides important information for geriatric dentistry. Secular trends in tooth loss indicate that edentulism (ie, complete tooth loss) will continue to decline. National Health and Nutrition Examination Survey data showed that the prevalence of edentulism was lower in 2009-2014 than in 1999-2004 (11% vs 17%) among adults aged ≥50 years. 35 The US population overall is experiencing less edentulism and greater tooth retention. Furthermore, research indicates that 64% of people aged ≥65 years with ≥1 tooth have moderate or severe periodontitis 36 and nearly 1 in 5 adults aged ≥65 years have untreated tooth decay. 37 As the population ages, the demand of dental care by older adults will be growing. By 2060, the number of US adults aged ≥65 years is expected to reach 98 million, or 24% of the overall population. 38 They may have a greater need than adults aged <65 years for regular dental services to address concerns such as root caries and dentures. Access to dental care among people aged ≥65 years in rural communities needs to be improved, and their financial burdens for dental services must be addressed to improve health and quality of life. 39
Finally, consistent with existing literature12,13,40 and Andersen’s model, 16 our study showed that higher income and higher levels of education were significant enabling factors for dental visits overall and that higher income was associated with use of preventive dental services. For Medicare beneficiaries, financial burden is among the most important barriers to use of dental services. Provision of dental insurance would improve access to dental care for Medicare beneficiaries. A recent public poll found that 90% of the public supported expanding Medicare coverage to dental, hearing, and vision. 41
Limitations
Our study had several limitations. First, information on dental procedures received is self-reported or proxy-reported and may be inaccurate. Second, multiple procedures of the same type reported during a single visit are recorded as a single procedure type in MSBS. Third, no information on the status of oral health (eg, dentition status) is available in MCBS. Data on use of dental services were from the community survey, but some data were extracted from claims by the CMS. Medicare Advantage plans may not report to CMS data on dental care services of their enrollees; thus, the data (especially dental visits) that we used in this analysis may not fully capture the use of dental services for Medicare Advantage enrollees. Nevertheless, this study contributed to the literature by updating the current status of dental utilization and procedures by Medicare beneficiaries in rural and urban areas.
Conclusion
The study findings reveal significant disparities in utilization of dental services for Medicare beneficiaries in rural communities. These disparities persisted after controlling for socioeconomic status. When rural Medicare beneficiaries utilized dental care, they were less likely to have preventive procedures but more likely to have restorative procedures than their urban counterparts, suggesting a greater burden of oral health needs among them. Policy research is needed to identify models that can incentivize prevention and improve access to dental care for Medicare beneficiaries in rural communities.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by a grant from the Health Resources & Services Administration (grant D88HP37544).