
Abstract
Objectives:
Limited data are available on how the closure of pediatric dental clinics because of the COVID-19 pandemic affected hospital pediatric emergency department (ED) visits in the United States. We evaluated changes in dental-related visits at a pediatric ED and associated urgent care centers (UCCs) after the shutdown of a large pediatric dental clinic because of the COVID-19 pandemic.
Methods:
We conducted a single-center retrospective medical record review of 811 patients aged 0 to 17 years who presented to a pediatric ED or associated UCC at Rady Children’s Hospital–San Diego for dental-related concerns from March 19, 2019, through January 17, 2021. Patients were classified into 3 periods: before shutdown, during shutdown, and after shutdown. We collected data on demographic characteristics; International Classification of Diseases, Tenth Revision codes; dental diagnosis; treatment; and COVID-19 test results. We compared the frequency and proportion of patients seen for dental-related concerns, dental diagnosis, and treatment during the 3 periods.
Results:
The proportion of dental-related concerns in the ED doubled during the shutdown (0.7%) and was 1.5 times higher after the shutdown (0.6%) compared with before the shutdown (0.4%; P < .001). Significantly more patients were seen in EDs than in UCCs during and after the shutdown than before the shutdown (P = .005). During and after the shutdown, admission to the hospital for antibiotic treatment increased significantly to 6.5% and 7.9%, respectively, compared with before the shutdown (2.8%; P = .022), and nonaerosolized procedures and ED/UCC discharge increased to 13.4% and 9.3%, respectively, compared with before the shutdown (6.2%; P = .015).
Conclusions:
Mitigating future closures of dental offices is important given the shifted burden of dental care to the ED.
On March 11, 2020, the World Health Organization declared the novel SARS-CoV-2 (the virus that causes COVID-19) a worldwide pandemic. 1 On March 16, 2020, the American Dental Association (ADA) released a statement asking all dentists in the United States to postpone elective dental treatment for 3 weeks. 2 The ADA further refined this recommendation by asking dentists to focus on emergency treatment to mitigate the spread of COVID-19 and ease the burden that dental emergencies would place on emergency departments (EDs). 2 Because most procedures in dentistry are aerosol-generating, dentists were theorized to be at high risk of contracting COVID-19. 3 As a result, many dental offices chose to close temporarily.
Based on the ADA’s recommendation to limit dental procedures to emergencies only, our pediatric dental clinic, a federally qualified health center in California, closed from March 19 through August 17, 2020. This dental clinic is co-located on the campus of San Diego County’s only children’s hospital, Rady Children’s Hospital–San Diego, which provides tertiary-level pediatric medical care to more than 250 000 patients annually. 4 Because of the location of the dental clinic and its proximity to the hospital, the clinic provides regular dental visits as well as critical service for dental emergencies and urgent dental follow-up visits for hospitalized patients and serves more than 12 000 patients annually. California issued guidance for dental offices to reopen and resume deferred and preventive dental care on April 27, 2020. 5 However, because of multiple factors, this pediatric dental clinic remained closed until August 17, 2020.
While the pediatric ED remained open throughout this time, some of the hospital’s associated urgent care centers (UCCs) closed or reduced their hours. Of the 6 UCCs, 1 closed on March 25, 2020, and another closed on March 30, 2020; both remained closed at the time of this writing. A third UCC closed on March 30, 2020, and reopened on November 11, 2020. The other 3 UCCS remained open.
The impact of dental facility closures during the COVID-19 pandemic on emergency dental visits has been studied. A retrospective study by the Department of Dental Emergency of West China Hospital of Stomatology, Sichuan University, found a 29.7% increase in patients seen for dental emergencies from January 20 through March 8, 2020, compared with the same period the previous year. 6 This increase in dental emergencies coincides with that region’s reduction in dental services. 6 The University Center of Dental Medicine Basel in Switzerland also found an increase in dental emergency visits during the 6-week COVID-19 pandemic lockdown period following the country’s mandated restrictions related to delivery of dental care. 7 In addition, a Canadian study reported that while overall outpatient dental clinic visits decreased during the COVID-19–related lockdown period, visits for oral infections and lesions increased during the same period. 8
Limited data are available on how the closure of pediatric dental clinics because of the pandemic affected hospital pediatric ED visits in the United States. We evaluated changes in the use of our pediatric ED and its associated pediatric UCCs for dental-related visits after the shutdown of our primary pediatric dental clinic. We hypothesized that use of the ED and UCC for dental-related concerns would increase during the shutdown of a large pediatric dental clinic.
Methods
Study Design and Analytic Sample
We conducted a single-center retrospective electronic health record review at a university-affiliated tertiary care pediatric ED and its associated UCCs from March 19, 2019, through January 17, 2021. We obtained institutional review board approval for this study from the University of California San Diego Human Research Protection Program. The study period was divided into 3 periods: before shutdown (the same period 1 year prior to the closing of the pediatric dental clinic because of COVID-19, which included patient encounters from March 19 through August 17, 2019), during shutdown (the period when the dental clinic was closed for all dental care, from March 19 through August 17, 2020), and after shutdown (the 5 months after reopening the dental clinic, which included August 18, 2020, through January 17, 2021). We reviewed data from 1013 patients aged 0 to 17 years who had a dental International Classification of Diseases, Tenth Revision (ICD-10) diagnostic code for both traumatic dental injuries (TDIs) and nontraumatic dental conditions (NTDCs). 9 We subdivided NTDCs into dental diagnosis of caries, reversible pulpitis, irreversible pulpitis, localized abscess, acute facial swelling, third molar impaction with or without facial swelling, viral infections, unable to determine, and other. Patient medical records were excluded if the dental diagnosis was not related to the chief concern, if the diagnosis was not dental-related, or if the patient left without being seen by a physician or dentist. For patients who presented with the same dental-related concern within the first 30 days of the initial visit, we excluded subsequent visits.
Data Collection and Variables
Patients were identified through a data query from the electronic medical record (Epic Systems Corporation). Two investigators (F.W., W.Y.C.) manually collected data from the medical record review, and any discrepancies were reconciled by consensus of all 5 authors. All data were coded, deidentified as a limited dataset on a password- and firewall-protected server, and stored in REDCap (Vanderbilt University). Primary outcomes included ED and UCC utilization for TDIs and NTDCs; secondary outcomes included dental diagnosis and treatment rendered. Additional covariates included demographic information such as age (0-5, 6-10, 11-17 years), sex (male, female), race (White, Asian, Black/African American, American Indian/Alaska Native, Other Asian, Native Hawaiian/Other Pacific Islander, Chinese, Filipino, Japanese, Korean, Vietnamese, Asian Indian, Guamanian or Chamorro, Samoan, multiracial, other, decline to answer, unknown), ethnicity (Hispanic, non-Hispanic, unknown, refused to answer), primary health insurance type (commercial, Medi-Cal, TriCare), department where patient presented (ED, UCC), ICD-10 codes, and whether a COVID-19 test was ordered and results, if available.
Exclusion Criteria
A total of 1013 patient encounters met the initial inclusion criteria. Excluded patients included those with a dental diagnosis that was not related to the chief concern or with a diagnosis that was not dental-related (n = 162) and patients who left without being seen by a physician or dentist (n = 8). For patients who presented with the same dental-related concern within the first 30 days from the initial visit, subsequent visits were excluded (n = 32). The final analysis included 811 patients who met inclusion criteria. Overall, sample sizes for the 3 periods were 323 before the shutdown, 247 during the shutdown, and 241 after the shutdown.
Statistical Analysis
We calculated rates for all categorical variables. We compared demographic characteristics, department where patient presented, dental diagnoses, and treatments by period (before shutdown, during shutdown, and after shutdown) using Pearson χ2 analyses. We performed all analyses using Vassarstats, an online computational program (VassarStats), and SPSS version 27.0 (IBM Corp). We considered P < .05 to be significant.
We limited analysis of ethnicity to those who identified as non-Hispanic and Hispanic because of small sample size for unknown and refused to answer categories. For analyses involving race, we excluded the categories of Pacific Islander, American Indian/Alaska Native, Asian Indian, declined, and missing because of small sample sizes.
Results
The median age of patients was 7.5 years, and 435 (53.6%) patients identified as male (Table 1). Four hundred twenty-four (52.3%) patients identified as Hispanic, and most (n = 541, 68.8%) patients listed Medi-Cal as their primary health insurance. We found no significant differences in demographic or other characteristics among patients presenting to the ED or UCC by period (before, during, or after shutdown).
Characteristics of patients at a pediatric emergency department and urgent care centers before, during, and after shutdown of a large pediatric dental clinic because of COVID-19 (N = 811), California, March 19, 2019–January 17, 2021 a
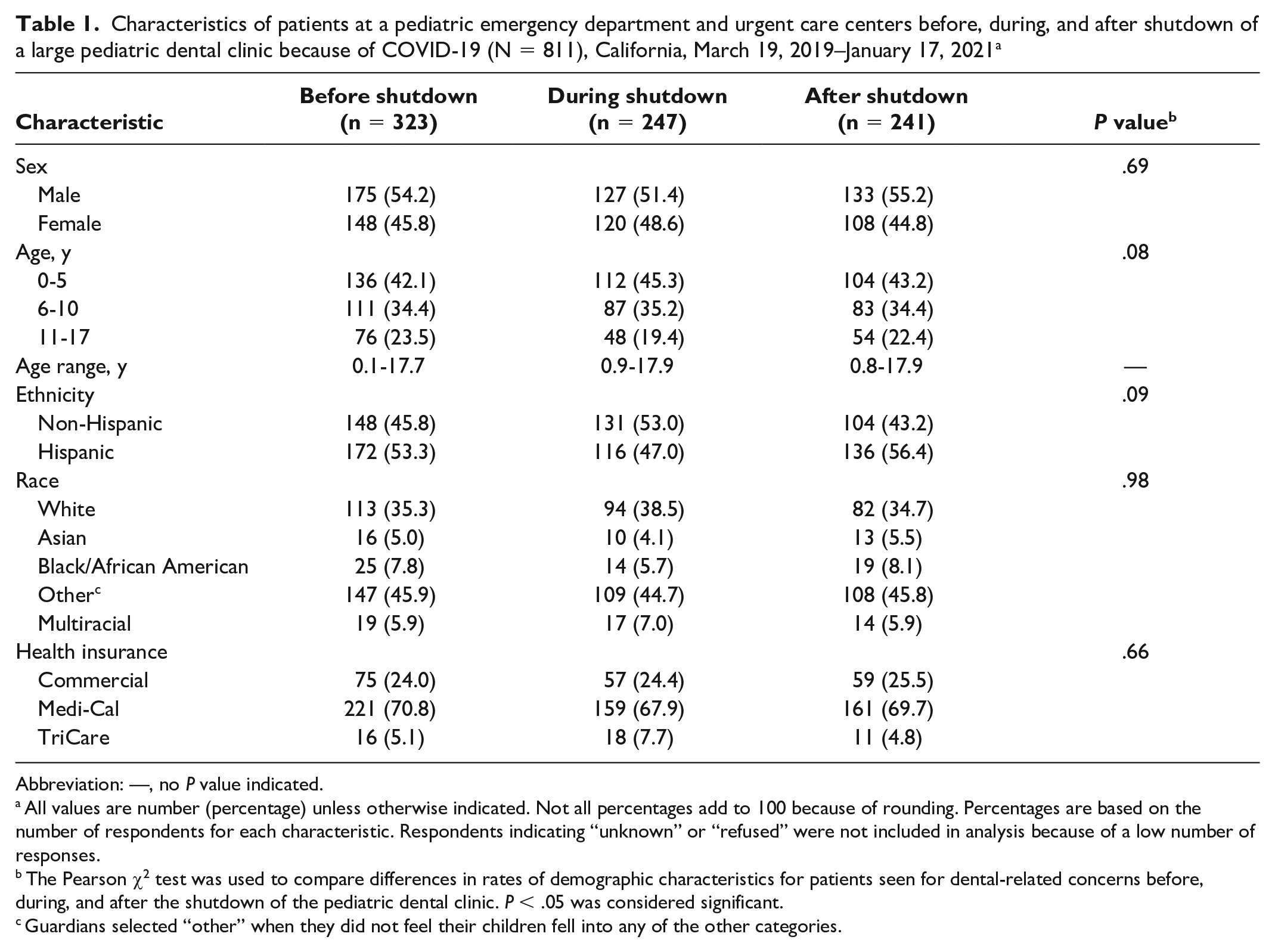
Abbreviation: —, no P value indicated.
All values are number (percentage) unless otherwise indicated. Not all percentages add to 100 because of rounding. Percentages are based on the number of respondents for each characteristic. Respondents indicating “unknown” or “refused” were not included in analysis because of a low number of responses.
The Pearson χ2 test was used to compare differences in rates of demographic characteristics for patients seen for dental-related concerns before, during, and after the shutdown of the pediatric dental clinic. P < .05 was considered significant.
Guardians selected “other” when they did not feel their children fell into any of the other categories.
The proportion of ED visits for all dental-related concerns increased significantly during (0.7%) and after (0.6%) the shutdown compared with before the shutdown (0.4%; P < .001) (Table 2). While we found no significant differences in rates of dental diagnoses during the 3 periods (Figure 1), the types of treatment rendered differed significantly among the 3 periods (Figure 2). A significant increase occurred in admissions for NTDCs (6.5%) and antibiotics used (7.9%) during and after the shutdown, respectively, compared with before the shutdown (2.8%; P = .022). Likewise, the percentage of nonaerosolized procedures and discharges directly from the ED/UCC increased during (13.4%) and after (9.3%) the shutdown for all dental-related concerns (ie, total TDIs and NTDCs) compared with before the shutdown (6.2%; P = .02).
Patients seen in the emergency department (ED) for dental-related and non–dental-related concerns before, during, and after shutdown of a large pediatric dental clinic because of COVID-19 (N = 811), California, March 19, 2019–January 17, 2021 a
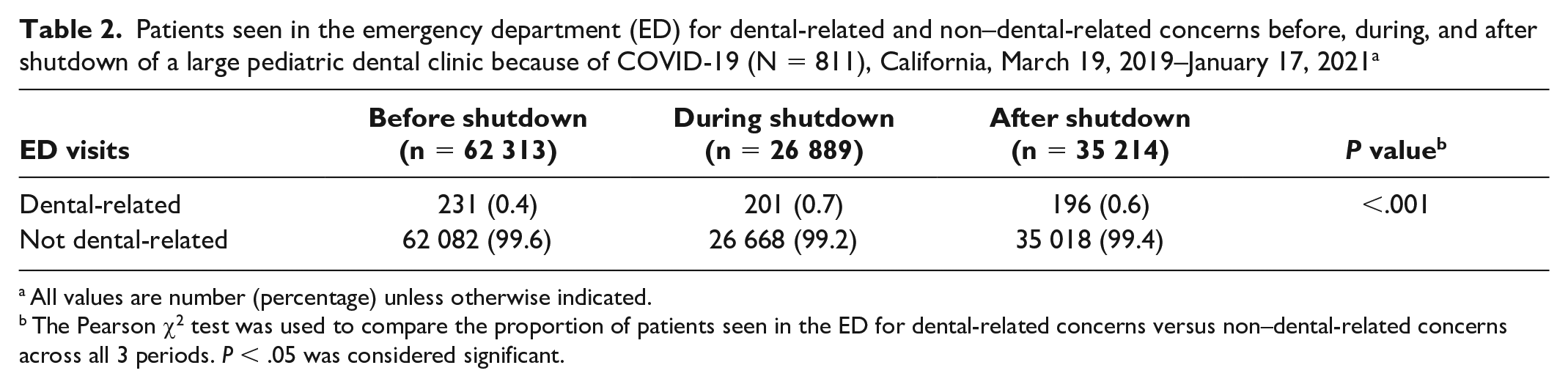
All values are number (percentage) unless otherwise indicated.
The Pearson χ2 test was used to compare the proportion of patients seen in the ED for dental-related concerns versus non–dental-related concerns across all 3 periods. P < .05 was considered significant.
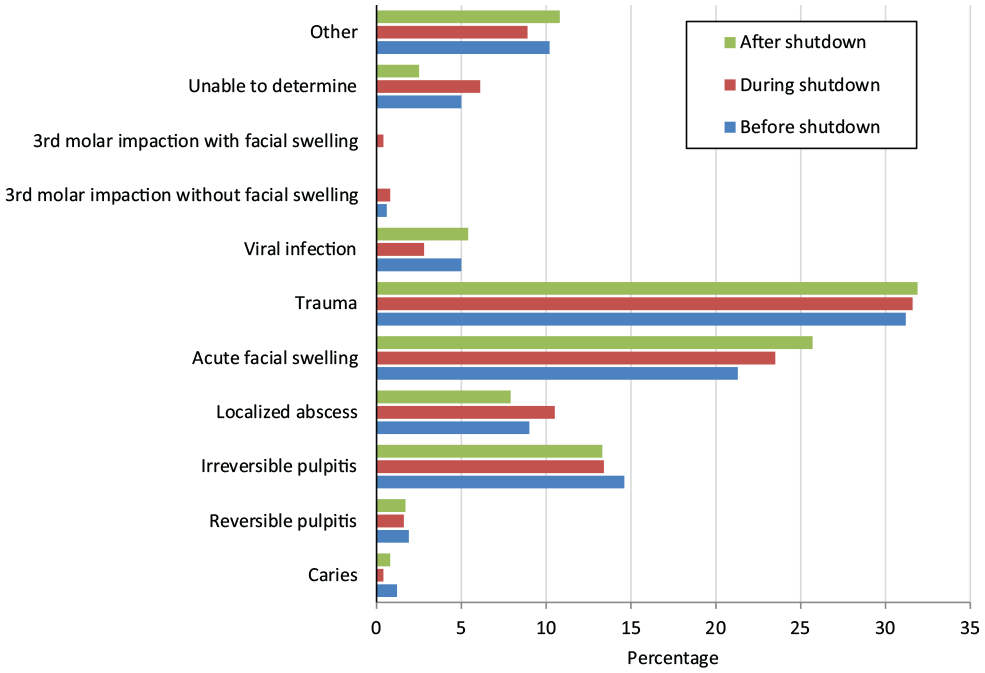
Diagnosis of dental-related concerns seen in the emergency department or urgent care center before, during, and after shutdown of a large pediatric dental clinic because of COVID-19 (N = 811), California, March 19, 2019–January 17, 2021. The Pearson χ2 test was used to compare rates of each diagnosis of dental-related concerns before, during, and after the shutdown periods; it showed no significant differences for any dental diagnoses (P = .83). Diagnoses with low numbers (caries, reversible pulpitis, third-molar impactions with and without facial swelling, unable to determine) were not analyzed. Other includes exfoliating tooth, orthodontic appliance, neonatal tooth, postdental procedure bleeding, temporomandibular joint pain, loose stainless steel crowns, suture removal, tooth eruption, ranula, parotiditis, lip laceration, oral ulcer, and postoperative dental pain.
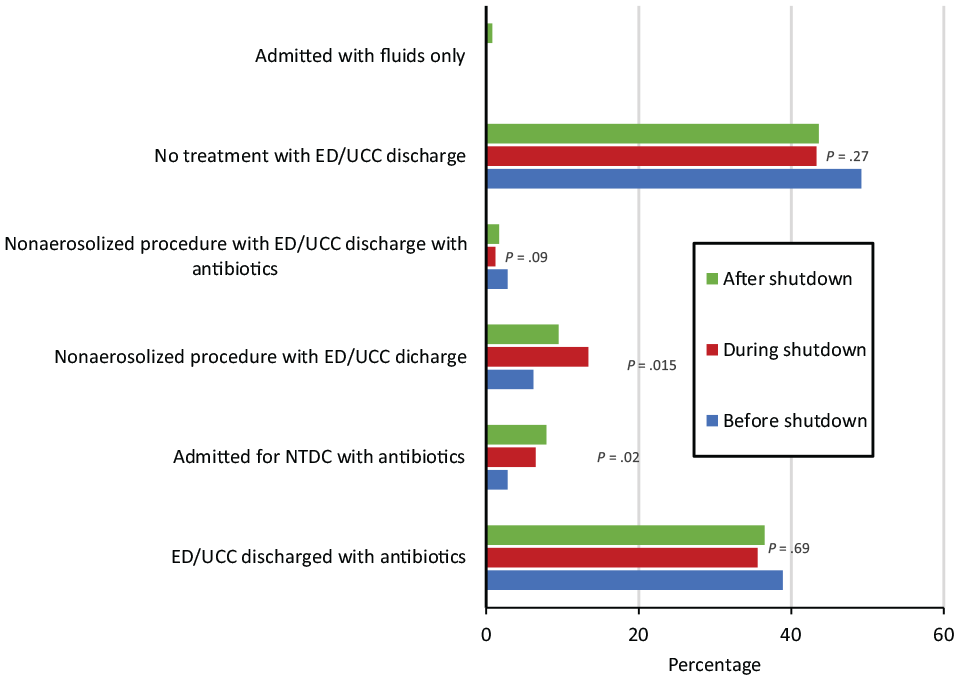
Treatment rendered for all dental-related concerns seen in the emergency department (ED) or urgent care center (UCC) before, during, and after shutdown of a large pediatric dental clinic because of COVID-19 (N = 811), California, March 19, 2019–January 17, 2021. The Pearson χ2 test was used to compare rates of treatment rendered for dental-related concerns during the 3 periods. P < .05 was considered significant. Treatment modalities with very small numbers (eg, admitted with fluids only) were not analyzed. Abbreviation: NTDC, nontraumatic dental condition.
While we found a decrease in total encounters for all dental-related concerns (ie, total TDIs and NTDCs) during and after the shutdown, with 231 patients seen in the ED (92 in UCCs) before the shutdown compared with 201 patients seen in the ED (46 in UCCs) during the shutdown and 196 patients seen in the ED (45 in UCCs) after the shutdown, we found a significant increase in the proportion of patients seen in the ED versus UCCs during (81.4%) and after (81.3%) the shutdown compared with before the shutdown (71.5%; P = .005).
A total of 117 COVID-19 nasal swab polymerase chain reaction tests were ordered at the time of visit, of which 5 (4.3%) were positive, 94 (80.3%) were negative, and 18 (15.4%) were indeterminate.
Discussion
In this retrospective study of a pediatric ED and its associated UCCs, the closure of a large pediatric dental office because of the COVID-19 pandemic was associated with an increase in ED utilization for TDIs and NTDCs despite lower patient volumes. This increase in ED utilization for dental-related visits persisted even after the pediatric dental clinic reopened. To our knowledge, this is the largest and only study of pediatric patients that evaluated dental-related concerns in a hospital pediatric ED/UCC setting during the pandemic. Our findings are similar to prior studies demonstrating increased dental emergency utilization during dental clinic closures.6,7
Our study showed that the proportion of all dental-related concerns in the ED more than doubled during the shutdown (0.7%) and was 1.5 times higher after the shutdown (0.6%) compared with before the shutdown (0.4%). These values were above the national average (0.5%) for patients aged 0 to 17 years in 2018, 10 possibly reflecting that while other seasonal or infectious diseases decreased during the pandemic, dental disease remained the same. The proportion of ED visits remained high even after the shutdown, possibly reflecting uncertainty among parents concerning whether dental offices and UCCs were reopened, whereas the likelihood of an ED being available for care was high. It could also reflect that the proportion increased only because of a decrease in other ED diagnoses during and after the shutdown.
Studies examining dental concerns in hospital settings prior to the COVID-19 pandemic often noted only NTDCs or TDIs, not both. Because TDIs are a common presentation in outpatient pediatric dental offices, it is important to note the effect of dental office closures on TDIs and hospital utilization. It is especially important to note because a recent study in North Carolina found that 47% of preschool-aged children have experienced dental trauma. 11 Accidental falls account for the primary etiology of TDIs among preschool-aged children, while sports and hits from other people are more common among school-aged children. 12 Physical activities, assault, and traffic accidents are the primary etiology among adolescents, while alcohol and mental distress played a key role in TDIs in a young adult population.13,14 In our study, TDIs (31.6%), acute facial swelling (23.3%), and irreversible pulpitis (13.8%) accounted for the most dental concerns, but we found no significant difference in rates observed before, during, and after the shutdown. This finding is similar to the finding of Wu et al, 6 who reported that dental trauma was the most common concern among patients aged 0 to 17 years presenting for dental emergency during the pandemic. Our study findings were surprising because many in-person events, including schools and local sporting events in our county, were suspended during the shutdown. Our findings should be examined in future studies, especially the role of alcohol and mental health in TDIs among older pediatric populations during the height of COVID-19 pandemic restrictions.
Although dental diagnoses did not vary significantly among the 3 periods, we found a significant difference in treatment rendered. More patients received nonaerosolized treatments and subsequent ED/UCC discharge during and after the shutdown than before the shutdown. It is possible that physicians and on-call dentists were aware that dental offices and UCCs were closed and, therefore, rendered more definitive treatment in the ED and UCC settings. The uncertainty of whether a dental office or UCC was open may have been a consideration by the ED/UCC provider and may explain why definitive treatment continued to be performed even after the shutdown.
Our study also found a significant increase in patients admitted to the hospital for NTDCs during and after the shutdown, suggesting an increase in severity of disease rather than a change in disease diagnosis. This finding differs from the findings of Wu et al, 6 who reported no changes in rates of cellulitis and abscesses of the mouth before or during the COVID-19–related shutdown. That study, and other similar studies, examined university-based dental emergency clinics rather than a hospital-based ED, as evaluated in our study. Patients whose condition required admission might have a perceived need or preference for care in a hospital facility rather than a university-based clinical facility. The increase in severity of dental disease in our study is similar to the severity reported in a Canadian study; that study showed a decrease in outpatient dental visits during the COVID-19 pandemic and an increase in frequency of visits for infections and lesions during that period. 8
Another consideration is the desire to avoid seeking care for nonurgent dental needs because of concerns about contracting COVID-19, even after reopening, thus allowing dental disease to progress. A recent social media–based study found that 47.7% of adults reported delaying health care because of the pandemic, with 38.1% of the delays specific to dental care. 15 Reasons for delaying health care included fear of being infected with COVID-19 (33.7%) and health care provider unavailability (28.9%). 15 The increase in severity of disease is notable because it suggests that a possible unintended sequela of the ADA’s recommendation and subsequent closure of a major pediatric dental clinic was that because of lack of access to dental care, patients’ dental disease may have progressed and some patients may have required hospitalization and escalation in the level of care.
This study also found that significantly more patients sought care for both TDIs and NTDCs in the ED versus UCCs during and after the shutdown compared with before the shutdown. This finding is most likely attributable to 50% of the UCCs being closed for the entire period during and after the shutdown, with only 1 UCC reopening halfway through the post-shutdown period, leaving the ED as the only option to seek care.
Socioeconomic disparities in ED utilization have been demonstrated, with the highest rate of dental-related ED visits found for those in the lowest income bracket. 14 Furthermore, the rate differential between the highest and lowest income brackets was greater for dental-related concerns than for non–dental-related concerns. 16 Although 68.8% of patients in our study had MediCal as their primary health insurance, we found no significant differences in health insurance type, which was used as a proxy for socioeconomic disparity. While California has continually made changes to its Medicaid system, essential and preventive treatment services for pediatric dentistry have been federally mandated benefits for both state-based and private health insurance for years prior to the COVID-19 pandemic.17-19 Thus, any changes made to the management of the Medicaid system would not have had a major impact on ED/UCC utilization for dental-related concerns during the periods examined in our study. This insignificance in health insurance type may also be because our hospital is the only children’s hospital in the region, and it serves a large catchment area with patients from a wide range of demographic backgrounds. It may also reflect that the COVID-19 pandemic, unlike other determinants of health, affected everyone regardless of socioeconomic status.
Limitations and Strengths
This study had several limitations. First, the ICD-10 codes used in the study did not include all dental codes available but were chosen because they represented dental concerns most likely to present to a dental office. Thus, this study may not have accounted for an increase in other dental-related concerns. Second, we excluded medical records of patients seen within 30 days for the same issue, potentially leading to an underreporting of those subsequently admitted after initial treatment failed. Third, this was only a single-center retrospective review, and the findings may not be generalizable to other areas. Lastly, COVID-19 mitigation strategies were different in each state. California had some of the strictest mandates in the country, with an indoor face mask mandate remaining in place for this hospital’s county until March 1, 2022. 20 These mandates may have influenced patients’ decisions about where and when to seek dental care and may not be applicable to states with less strict measures.
This study also had several strengths. One strength was the large sample size and consistent ICD-10 coding in a hospital-based medical record system. Another strength was that medical record reviews were completed by 2 reviewers, with differences resolved by consensus. Lastly, the co-location and geographic circumstances of the facilities in this study provided a unique study condition. There is likely a more readily observable impact on ED utilization because of the pediatric dental clinic’s closure as a result of its role as a key dental care service provider in the region.
Conclusion
Considering the increased clinical burden on EDs and UCCs for TDIs and NTDCs, with the potential for increased costs of care, severity of dental disease, and evidence that dental care can be safely delivered, it is imperative that a complete shutdown of dental offices is avoided or mitigated in the future.
Footnotes
Acknowledgements
The authors thank Andrew Richardson, MS, research data manager, for his assistance with importing the charts and data into REDCap.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.