
Abstract
Objectives:
We conducted a survey to understand how people’s willingness to share information with contact tracers, quarantine after a COVID-19 exposure, or activate and use a smartphone exposure notification (EN) application (app) differed by the person or organization making the request or recommendation.
Methods:
We analyzed data from a nationally representative survey with hypothetical scenarios asking participants (N = 2157) to engage in a public health action by health care providers, public health departments, employers, and others. We used Likert scales and ordered logistic regression to compare willingness to take action based on which person or organization made the request, and we summarized findings by race and ethnicity.
Results:
The highest levels of willingness to engage in contact tracing (adjusted odds ratio [aOR] = 1.74; 95% CI, 1.55-1.96), quarantine (aOR = 1.91; 95% CI, 1.69-2.15), download/activate an EN app (aOR = 1.30; 95% CI, 1.16-1.46), and notify other EN users (aOR = 1.43; 95% CI, 1.27-1.60) were reported when the request came from the participant’s personal health care provider rather than from federal public health authorities. When compared with non-Hispanic White participants, non-Hispanic Black participants reported significantly higher levels of willingness to engage in contact tracing (aOR = 1.32; 95% CI, 1.18-1.48), quarantine (aOR = 1.49; 95% CI, 1.37-1.63), download/activate an EN app (aOR = 2.19; 95% CI, 2.01-2.38), and notify other EN users (aOR = 1.63; 95% CI, 1.49-1.79).
Conclusions:
Partnering with individuals and organizations perceived as trustworthy may help influence people expressing a lower level of willingness to engage in each activity, while those expressing a higher level of willingness to engage in each activity may benefit from targeted communications.
During a pandemic with rapid person-to-person spread, quarantine of recently exposed and, thus, potentially infected people can prevent transmission. Delays between exposure and quarantine, as well as the inability to identify contacts, contribute to further spread. Traditional and technology-assisted contact tracing has been used across the United States during the COVID-19 pandemic to aid contact identification, notification, and quarantine requests.
The COVID-19 pandemic has revealed difficulties in identifying, locating, and quarantining exposed people.1-6 With traditional case investigation and contact tracing, people diagnosed with COVID-19 need to answer a telephone call, as well as remember and provide details (eg, names, telephone numbers) of people with whom they have come into close contact. If people do not answer the telephone, a contact tracer has the option to call back or even visit their homes. 1 However, the rapid spread of SARS-CoV-2 had impeded traditional contact tracing.2,3 Exposure notification (EN), a technology-based intervention designed to augment traditional techniques, uses smartphone proximity sensors and modern cryptographic techniques to safeguard user identities while capturing interactions with others. 7 However, EN communications are restricted to what can be sent via text message or viewed in an associated application (app), limiting the interaction with public health. Infected people must also manually upload a positive test verification code upon receiving a positive SARS-CoV-2 test result, so their close contacts can be notified to take recommended public health actions. While downloading and activating this technology is a prerequisite, subsequently notifying others and following public health guidelines are crucial to realize the benefits of EN. 8
Our work is informed by prior research linking willingness to download/activate smartphone apps with trust in the individuals or organizations recommending or associated with the technology.4,5,9,10 We also considered research that reported on willingness to engage with contact tracing efforts1 -4,11 and EN,4 -6,9,10,12 as well as research comparing aspects of contact tracing with EN4,9,10 and comparing initially downloading an EN app with later using EN to notify others.10,12 We extend previous research by surveying a representative sample of the US population and systematically comparing actions related to contact tracing, quarantine, downloading/activating an EN app, and using EN to notify others. In particular, we examined the effect of individuals or organizations recommending and requesting engagement and compliance, as well as differences by race and ethnicity to provide an overview of willingness to engage with COVID-19 contact tracing efforts. We conducted a survey to investigate people’s willingness to engage with contact tracing efforts, including quarantine guidance. We also measured how that willingness was affected by the person or organization recommending engagement or compliance.
Methods
Study Design
We designed a survey to investigate participant willingness to engage in different aspects of traditional contact tracing, quarantine, and EN. Each scenario was presented as though the request or recommendation came from the participant’s doctor or health care provider; any doctor or nurse; city, county, or state public health department; federal public health authorities; the participant’s employer or school; where applicable, the participant’s smartphone provider; “on your own” (ie, without anyone asking the person directly); and the participant’s state governor’s office (only for the quarantine scenario).
The 4 scenarios of interest were whether the participant would be willing to (1) share information with a contact tracer, (2) quarantine if notified about a SARS-CoV-2 exposure, (3) download or activate EN on the participant’s smartphone, and (4) allow the anonymous notification to other EN users if the participant were to have a positive COVID-19 test result. Participants were asked to rate each scenario and person/organization pair using a 5-point Likert scale 13 (1 = very unlikely, 2 = somewhat unlikely, 3 = neither likely nor unlikely, 4 = somewhat likely, and 5 = very unlikely), indicating their willingness to perform that action after considering the person or organization making the request or recommendation.
Sample and Procedure
During April 30–May 24, 2021, NORC at the University of Chicago, an independent research organization, provided a nationally representative US sample of its AmeriSpeak-recruited probability panel aged ≥18 years (Table 1). This established survey methodology uses stratified random sampling according to age (18-24, 25-34, 35-44, 45-54, 55-64, 65-74, ≥75 years), sex (male, female), race and ethnicity (non-Hispanic White, non-Hispanic Black, Hispanic, and other [non-Hispanic Asian, another race or ethnicity, or ≥2 races or ethnicities]), and education (<high school, high school/equivalent, vocational/some college, bachelor’s degree, postgraduate study) and adjusts final weights for nonresponse by age, sex, race and ethnicity, and education.14,15 Participants could choose to take the survey in English or Spanish.
Characteristics of participants in a survey on willingness to engage in contact tracing, quarantine, and exposure notification, by race and ethnicity, United States, April 10–May 24, 2021 a
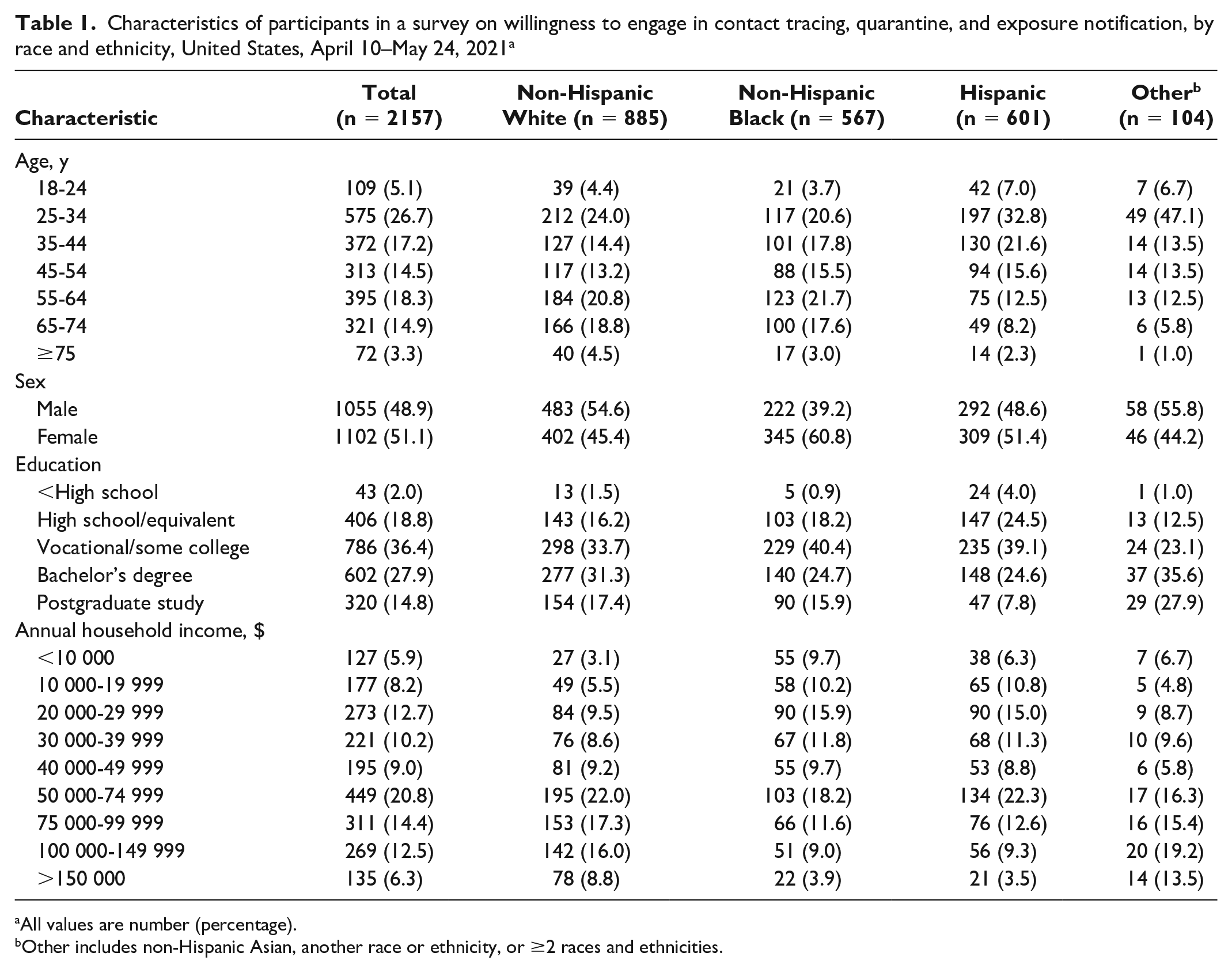
All values are number (percentage).
Other includes non-Hispanic Asian, another race or ethnicity, or ≥2 races and ethnicities.
Invited panel members who reported owning a smartphone were provided a link to a Qualtrics survey with a description of the study and consent information. After consenting to participate, users were directed to the full survey, which took a median of 13 minutes to complete. Survey responses were excluded from analysis if a participant skipped ≥10 questions or completed the survey in 3.5 minutes (ie, quality control exclusions).
Data Analysis
We performed an analysis on the frequency of each response choice within each scenario, weighted according to the sampling weights provided for each participant. We then built predictive models of willingness to engage or comply by regressing the proportional odds of reported willingness on indicator variables for each independent variable. Because our data are weighted to better represent the demographic composition of the United States, we performed a weighted ordinal logistic regression analysis and report results as adjusted odds ratios (aORs), corresponding 95% CIs, and P values, with P ≤ .05 considered significant.
Ethics Approvals
The Massachusetts Institute of Technology Committee on the Use of Humans as Experimental Subjects approved this study, with concurrence from the institutional review board of NORC and the Air Force Medical Readiness Agency Human Research Protection Official. The Centers for Disease Control and Prevention (CDC) reviewed this activity to ensure that it was conducted consistent with applicable federal law and CDC policy (45 CFR part 46, 21 CFR part 56; 42 USC §241[d]; 5 USC §552a; 44 USC §3501 et seq).
Results
Of the 9941 AmeriSpeak panel members invited, 2356 responded to the invitation (23.7% response rate). The 36 respondents who indicated not owning a smartphone were not directed to the survey. We removed another 163 responses from the analysis where respondents failed the predetermined quality control exclusions, leaving 2157 participants who consented and completed the survey successfully.
Of the 2157 survey participants, 885 (41.0%) described themselves as non-Hispanic White, 567 (26.3%) as non-Hispanic Black, 601 (27.9%) as Hispanic, and 104 (4.8%) as non-Hispanic other (Table 1).
We grouped participants’ self-reported willingness to participate in the desired public health activities by the person or organization recommending that action (Table 2) and demographic characteristics (Table 3).
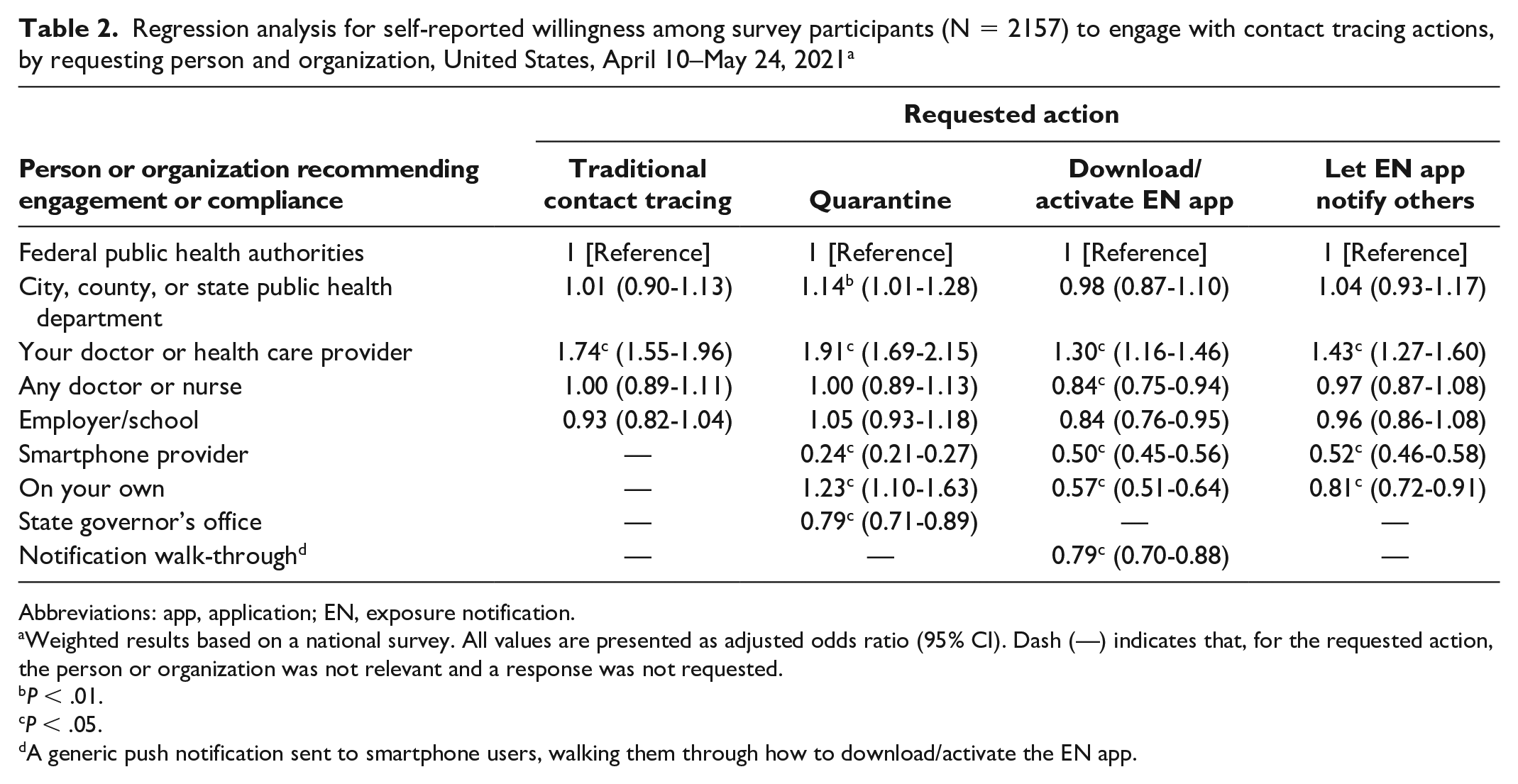
Regression analysis for self-reported willingness among survey participants (N = 2157) to engage with contact tracing actions, by requesting person and organization, United States, April 10–May 24, 2021 a
Abbreviations: app, application; EN, exposure notification.
Weighted results based on a national survey. All values are presented as adjusted odds ratio (95% CI). Dash (—) indicates that, for the requested action, the person or organization was not relevant and a response was not requested.
P < .01.
P < .05.
A generic push notification sent to smartphone users, walking them through how to download/activate the EN app.
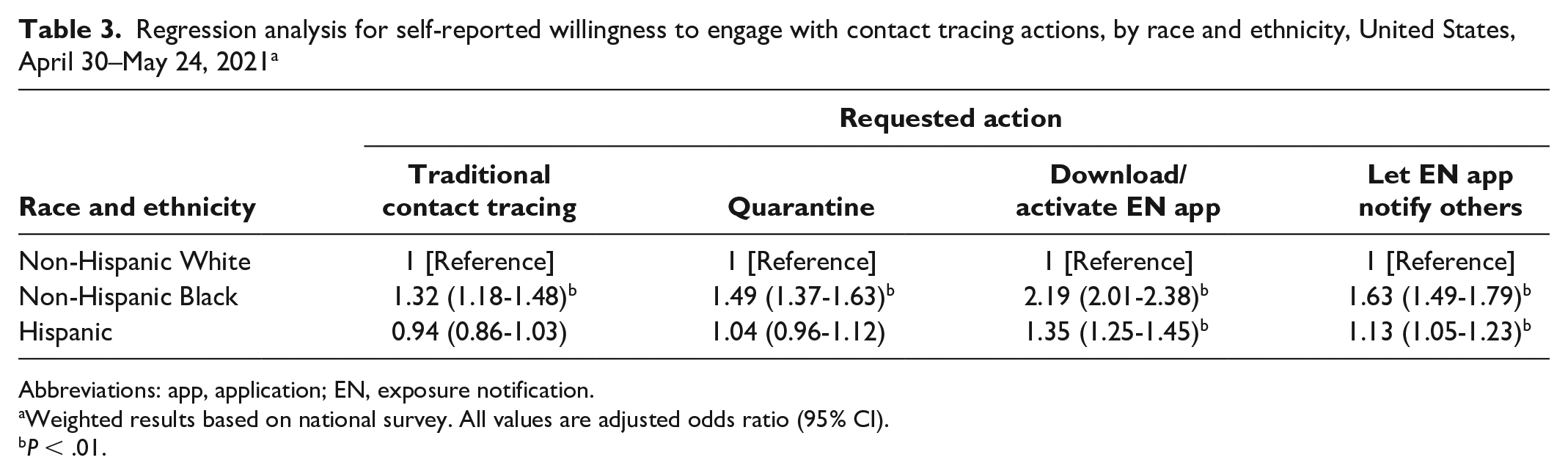
Regression analysis for self-reported willingness to engage with contact tracing actions, by race and ethnicity, United States, April 30–May 24, 2021 a
Abbreviations: app, application; EN, exposure notification.
Weighted results based on national survey. All values are adjusted odds ratio (95% CI).
P < .01.
Sharing Contact Tracing Information
In the traditional contact tracing scenario, levels of willingness to share information were significantly higher when the participant’s doctor or health care provider made the request (aOR = 1.74; 95% CI, 1.55-1.96) than when the request came from federal public health authorities (Table 2). When compared with non-Hispanic White participants, non-Hispanic Black participants expressed greater levels of willingness to participate in traditional contact tracing (aOR = 1.32; 95% CI, 1.18-1.48; Table 3).
Willingness to Quarantine
Levels of willingness to quarantine after receiving a positive test result for COVID-19 were higher when the request came from the participant’s doctor or health care provider (aOR = 1.91; 95% CI, 1.69-2.15), no one (ie, quarantined “on your own”; aOR = 1.23; 95% CI, 1.10-1.63), or public health departments (city, county, or state; aOR = 1.14; 95% CI, 1.01-1.28) than when the request came from federal public health authorities (Table 2). Levels of willingness were lower when the request came from the state governor’s office (aOR = 0.79; 95% CI, 0.71-0.89) or the participant’s smartphone provider (aOR = 0.24; 95% CI, 0.21-0.27). When compared with non-Hispanic White participants, non-Hispanic Black participants expressed a higher level of willingness to quarantine (aOR = 1.49; 95% CI, 1.37-1.63; Table 3).
Downloading/Activating EN App on Smartphone
Levels of willingness to download/activate an EN app were highest when the request came from the participant’s doctor or health care provider (aOR = 1.30; 95% CI, 1.16-1.46), lower when the request came from any doctor or nurse (aOR = 0.84; 95% CI, 0.75-0.94) or the participant’s employer or school (aOR = 0.84; 95% CI, 0.76-0.95), and lowest when the request came from the participant’s smartphone provider (aOR = 0.50; 95% CI, 0.45-0.56) or no one (ie, downloaded/activated app “on your own”; aOR = 0.57; 95% CI, 0.51-0.64), as compared with when the request came from federal public health authorities (Table 2). When compared with non-Hispanic White participants, non-Hispanic Black (aOR = 2.19; 95% CI, 2.01-2.38) and Hispanic (aOR = 1.35; 95% CI, 1.25-1.45) participants expressed higher levels of willingness to download/activate an EN app (Table 3).
Notifying Other EN Users
Levels of willingness to notify other EN users about a positive COVID-19 test result were highest when the request came from the participant’s doctor or health care provider (aOR = 1.43; 95% CI, 1.27-1.60). They were lower when the request came from the participant’s smartphone provider (aOR = 0.52; 95% CI, 0.46-0.58) or no one (ie, notified “on your own”; aOR = 0.81; 95% CI, 0.72-0.91), as compared with receiving the request from federal public health authorities (Table 2). When compared with non-Hispanic White participants, non-Hispanic Black (aOR = 1.63; 95% CI, 1.49-1.79) and Hispanic (aOR = 1.13; 95% CI, 1.05-1.23) participants expressed higher levels of willingness to use EN to notify contacts about a recent exposure.
Discussion
We found significant differences in willingness to participate in COVID-19 contact tracing, quarantine, and EN that depended on who requested or recommended the action. When requests or recommendations originated from a personal doctor or health care provider rather than federal public health authorities, participants consistently reported higher levels of willingness to engage or comply. Requests from local public health authorities also resulted in high reported likelihood to engage in EN and to quarantine and was second only to receiving requests from personal doctors, as compared with other individuals or organizations. Participants were less willing to participate if a smartphone provider asked them to do so. A national survey conducted a year before ours found similar low willingness to use the then-in-development Google Apple Exposure Notification app.4,16
Our findings confirm prior research, which found that users rely on institutional trust when deciding whether to install a smartphone EN app, 5 but it extends that area of research to show similar institutional trust preferences across other contact investigation activities. As in previous research, Hispanic participants reported higher levels of intent to install EN apps as compared with non-Hispanic White participants. 12 Hispanic participants also reported higher intentions to use EN to notify others, whereas non-Hispanic Black participants reported the highest intention to participate in contact tracing, quarantine, download/activate an EN app, and use EN to notify others.
Our findings confirm those of a prior national poll 11 in which people reported high levels of trust in health care providers, even though the actual level of engagement was low for contact tracing efforts1 -3 and EN use 6 throughout the COVID-19 pandemic. Our results show that this lower level of engagement may be due in part to the communications coming from, or being perceived as coming from, a less trusted source. These results highlight the need for trusted people or organizations to engage in the process and to consider the perception of communications to increase public engagement.
Limitations
Our study had several limitations. First, to keep scenarios simple and focused on comparisons among people, organizations, and actions, we did not describe details of typical real-world scenarios. We expect that details would affect real-world willingness to engage, especially if the person were experiencing symptoms or the action had adverse financial consequences. Second, participants may have provided more socially desirable responses that differ from how they would actually behave. To target potential EN app users, we screened for participants who owned a smartphone, which may have excluded vulnerable populations (eg, those not able to access or use a smartphone). Lastly, our recruited probability sample did not control for bias in other areas, such as nonparticipation due to strong opposition to contact tracing efforts.
Conclusion
People expressing low levels of willingness to engage in each COVID-19 contact tracing activity could benefit from targeted communications from entities that they hold in high regard, while those expressing a higher level of willingness to engage in EN may benefit from targeted communications to ensure awareness and understanding of how to engage fully. Our research highlights differences in willingness to engage with COVID-19 contact tracing efforts across various populations. While a person’s personal doctor or health care provider appeared to be the most influential requestors, requests from federal and local public health authorities were also positively associated with reported willingness to engage in contact tracing activities. To promote public health initiatives, federal and local public health authorities should, wherever possible, consider outreach to local health care providers to coordinate messaging to their patients through existing communication channels such as patient portals, email communications, or official websites. Coordination with trusted people and organizations may also serve to reinforce recommendations about, and improve participation in, public health initiatives. Our research also shows high willingness to engage with traditional contact tracing and quarantine efforts but suggests that communications about COVID-19 public health measures during spring 2021 might not have been perceived as coming from trusted sources. Federal and local public health authorities should explore ways to ensure that public perception of communications align with public health intent.
Footnotes
Acknowledgements
The authors thank Daniel J. Weitzner, JD (MIT Computer Science and Artificial Intelligence Laboratory), Curran Schiefelbein, ScM (MIT Lincoln Laboratory), Lauren Finklea, MS (Centers for Disease Control and Prevention), and Adam Norige, MS (MIT Lincoln Laboratory), for their invaluable support and guidance and Charlie Ishikawa, MSPH (Kahuina Consulting LLC), for his advice and insights.
Disclaimer
The findings and conclusions of this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention or the Massachusetts Institute of Technology. Any opinions, findings, conclusions, or recommendations expressed in this article are those of the authors and do not necessarily reflect the views of the US Air Force. Use of product names does not imply their endorsement. Distribution statement: approved for public release; distribution is unlimited.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This material is based on work supported under Air Force contract FA8702-15-D-0001. Ilaria Liccardi was also supported by the William and Flora Hewlett Foundation.