
Abstract
Objectives:
Paraprofessional substance use disorder counselors (SUDCs) are an important component of expanding access to substance use disorder treatment, but little research on SUDC training currently exists. We evaluated knowledge and self-efficacy gain from brief in-person and virtual workshops for paraprofessional SUDC student-trainees.
Methods:
Student-trainees (N = 100) enrolled in an undergraduate SUDC training program completed 6 brief workshops from April 2019 to April 2021. Three in-person workshops during 2019 covered clinical assessment, suicide risk and evaluation, and motivational interviewing, and 3 virtual workshops during 2020-2021 covered family engagement and mindfulness-oriented recovery enhancement, as well as screening, brief intervention, and referral to treatment for expectant mothers. Pretest and posttest online surveys measured student-trainee knowledge gain related to all 6 SUDC modalities. Results of paired sample t tests evaluated changes in knowledge and self-efficacy from pretest to posttest.
Results:
All 6 workshops showed a significant gain in knowledge from pretest to posttest. Four workshops showed a significant gain in self-efficacy from pretest to posttest. Hedges g ranged from 0.70 to 1.95 for knowledge gain and from 0.61 to 1.73 for self-efficacy gain across workshops. Common language effect sizes indicating the probability that a participant increased one’s score from pretest to posttest ranged from 76% to 93% for knowledge gain and from 73% to 97% for self-efficacy gain across workshops.
Conclusions:
Results of this study add to the limited research base on training for paraprofessional SUDCs and suggest that in-person learning and virtual learning are both viable brief training tools for students.
The Centers for Disease Control and Prevention estimated that >92 000 drug overdose deaths occurred in 2020 in the United States, a 30% increase from the previous 12 months. 1 The prevalence of substance use disorders (SUDs) also increased, with >40 million people reporting a diagnosable SUD in 2020. 2 Experts highlight consistent reports that the stressors of the COVID-19 pandemic began exacerbating substance misuse in early 2020. 3 At that time, the United States was facing 2 intersecting public health crises: a multidecade epidemic of substance abuse and the COVID-19 pandemic. 3
Before 2020, the supply of SUD counselors (SUDCs) in the United States was not sufficient to meet the nation’s demand for SUD treatment. 4 SUDCs may come from multiple professions, including psychology, social work, or medicine. To address this workforce shortage, many states have enlisted paraprofessional SUDCs to provide SUD treatment–related services under the supervision of licensed SUDCs. Paraprofessional SUDCs, while not independently licensed to provide counseling services, are typically trained in a range of evidence-based SUD treatments. Paraprofessional SUDCs often support many central features of SUD treatment, including screening, intake, assessment, case management, and documentation. As such, paraprofessional SUDCs are well positioned to work in tandem with licensed SUDCs to increase treatment capacity. 5 The Health Resources and Services Administration estimates that growth in the demand for licensed SUDCs will outpace training and education of new SUDCs by 12% by 2030, leaving the SUDC workforce at a shortfall of at least 13 600 licensed counselors. 6 As states and communities attempt to meet treatment demands amid the increasing prevalence of SUDs and the anticipated shortages of licensed SUDCs, paraprofessional SUDCs are likely to see greater utilization in the coming decade.
Research focusing on paraprofessional SUDCs is limited. Most current research has considered paraprofessional SUDCs on the path to clinical licensure. These studies have largely shown similar SUD treatment outcomes across paraprofessional and licensed SUDCs. 7 Many paraprofessional SUDCs, however, choose not to pursue clinical licensure and instead provide a range of services important for SUD treatment. Little research has examined the additive impact of paraprofessional SUDCs on the effectiveness of standard SUD treatment approaches. During a 3-year period, one study found that home visitation services provided by paraprofessional SUDCs resulted in improved SUD outcomes as compared with treatment as usual. 8 A study testing the additive effect of paraprofessional-delivered SUD screening services in primary care settings reported a reduced need for intensive inpatient SUD treatment services across 2 years. 9 A systematic review of 14 empirical studies examined the effect of case managers, a role often occupied by paraprofessional SUDCs, on SUD treatment outcomes. 10 Only one-third of studies, however, found that case management services were associated with improvements in SUD outcomes; half of studies reported improvements in general functioning. Beyond treatment outcomes, few recent studies have evaluated education or training specific to paraprofessional SUDCs in the United States. One study among nursing students trained in SUD screening found that screening services were more likely to be deployed in clinical settings when students reported increased self-efficacy after training. 11 Given the current roles occupied by paraprofessional SUDCs and the likely increase in their utilization in the coming decade, further understanding of paraprofessional SUDC training can provide important information for the field.
The Health Resources and Services Administration’s shortfall projections for licensed SUDCs by 2030 were released prior to the COVID-19 pandemic and the subsequent disruption to education and training systems across the United States. With the onset of the COVID-19 pandemic, most colleges, universities, and postsecondary training programs shifted from traditional, classroom-based instruction to online platforms to help mitigate the spread of disease. 12 Most education systems were largely unprepared for the scope of this emergency move to online education. 13 Specific to SUDC training, the projected shortfall of licensed SUDCs during the next decade may be an underestimate because of these disruptions. Given the risk of drug overdose during the COVID-19 pandemic, 1 the increasing demand for SUD treatment services, 6 and the likelihood that paraprofessional SUDCs will be enlisted to help meet this demand in the coming decade, evaluations of paraprofessional SUDC training before and after the COVID-19 pandemic are warranted.
The current study was designed to provide information on 2 overlapping research questions. First, what are the effects on SUD treatment knowledge and self-efficacy of brief training in evidence-based approaches for paraprofessional SUDCs? Second, do in-person and virtual brief trainings in evidence-based approaches produce similar effects on SUD treatment knowledge and self-efficacy among paraprofessional SUDCs?
Methods
Members of the research team recruited participants for this study from 2019 to 2021 from a pool of students enrolled in an in-person undergraduate SUDC certificate program at a public university in the Intermountain Western region of the United States. The certificate program consists of 9 semester-length didactic courses, field training under the direct supervision of a licensed clinician (250-400 hours), and at least 3 brief specialized workshops. Student-trainees could participate in workshops at any point while enrolled after entry into the certificate program. As such, some virtual workshop participants had previously attended in-person workshops. The research team recruited workshop instructors with specialty knowledge in evidence-based SUD treatment approaches to provide SUDC content not covered in semester-length courses. Informed consent for participation in this study was collected prior to workshop attendance, and approval for this study was granted by the institutional review board at the University of Utah.
We examined pretest and posttest data from 6 workshops: 3 held in person during 2019 and 3 held virtually from 2020 to 2021. In-person workshops covered 3 evidence-based SUD treatment approaches. The Clinical Assessment workshop covered biopsychosocial assessment across multiple dimensions for clients in SUD treatment. 14 The Suicide Risk and Evaluation workshop provided information on the interplay of SUD and suicidality and focused on assessment of co-occurring SUD and suicidality among clients. 15 The Motivational Interviewing workshop covered the core tenets of motivational interviewing and trained students on coding motivational interviewing–based communication in SUD treatment. 16 Virtual workshops covered 3 evidence-based SUD treatment approaches as well. The Family Engagement workshop presented on community reinforcement and family training with a focus on facilitating the involvement of concerned significant others. 17 The Mindfulness-Oriented Recovery Enhancement (MORE) workshop provided information on the role of mindfulness in SUD treatment and focused on facilitating mindfulness-based exercises among SUD clients. 18 The Screening, Brief Intervention, and Referral to Treatment workshop for expectant mothers (Prenatal SBIRT) trained students on screening, assessment, and referral for SUD during pregnancy. 19
Measures
Six surveys were designed and administered by each workshop instructor directly before and after each workshop via Qualtrics. All 6 surveys measured knowledge in that modality at pretest and posttest, and 4 surveys measured self-efficacy in that modality at pretest and posttest. The Clinical Assessment survey consisted of 10 multiple-choice or text-entry knowledge-based items. For example, one knowledge-based question asked respondents to identify the standardized clinical interview for determining medical necessity for an SUD. The Suicide Risk and Evaluation survey consisted of 10 multiple-choice or text-entry knowledge-based items. For example, one knowledge-based question asked respondents to identify which substance is most often linked to a suicide attempt. The Motivational Interviewing survey consisted of 6 multiple-choice or text-entry knowledge-based items and 1 self-efficacy item. For example, one text-entry knowledge-based question asked respondents to define the open question, affirmation, reflective listening, and summary reflection skills. A self-efficacy question asked participants to rate their comfort in using motivational interviewing principles in practice. The Family Engagement survey consisted of 14 multiple-choice knowledge-based questions and 4 multiple-choice self-efficacy questions. For example, one knowledge-based question asked participants to identify barriers to concerned significant other involvement in recovery. Four self-efficacy questions with Likert-scale response options ranging from strongly agree to strongly disagree asked about knowledge, skills, and confidence in engaging concerned significant others in treatment. The MORE survey consisted of 10 multiple-choice knowledge-based questions and 1 multiple-choice self-efficacy question. For example, one knowledge-based question asked participants to identify the goals of mindful reappraisal in SUD treatment. A self-efficacy question with Likert-scale response options ranging from very uncomfortable to very comfortable asked about comfort in facilitating MORE-based exercises with clients. The Prenatal SBIRT survey consisted of 8 multiple-choice knowledge-based questions and 2 multiple-choice self-efficacy questions. For example, one knowledge-based question asked participants to identify first steps after an individual meets the criteria for an SUD during pregnancy. Two self-efficacy questions with Likert-scale response options ranging from strongly disagree to strongly agree asked about the level of comfort working with pregnant women who use substances. Knowledge-based scores for all 6 surveys were calculated by summing the number of correct answers. Surveys with >1 self-efficacy question measured self-efficacy as the mean of Likert-scale items. The survey questions are available upon request.
Analysis
We used paired sample t tests with 1000 bootstrapped samples to compare pretest and posttest scores for each workshop. We conducted statistical analyses using SPSS Statistics version 27 (IBM Corp) and produced figures using R version 4.1 (R Core Team). We calculated Cohen d, Hedges g, and common language (CL) effect sizes based on formulas and recommendations provided by Lakens. 20 We applied Hedges correction to calculations of Cohen d average to produce an unbiased Hedges g average.20,21 We calculated 95% CIs based on the approach provided by Hedges and Olkin. 21 Hedges g represents a change in mean scores from pretest to posttest expressed in pooled SD units. The CL effect size compares the standardized distribution of mean score differences from pretest to posttest with a normal distribution to estimate the probability that the score of any single workshop participant increased from pretest to posttest.
Results
Of 100 workshop participants, 51 (51%) attended 1 workshop, 41 (41%) attended 2 workshops, 7 (7%) attended 3 workshops, and 1 (1%) attended 1 workshop (Table 1). No participants attended >4 workshops.
Demographic characteristics of in-person and virtual participants in SUDC workshops at a university in the Intermountain Western region, United States, 2019-2021
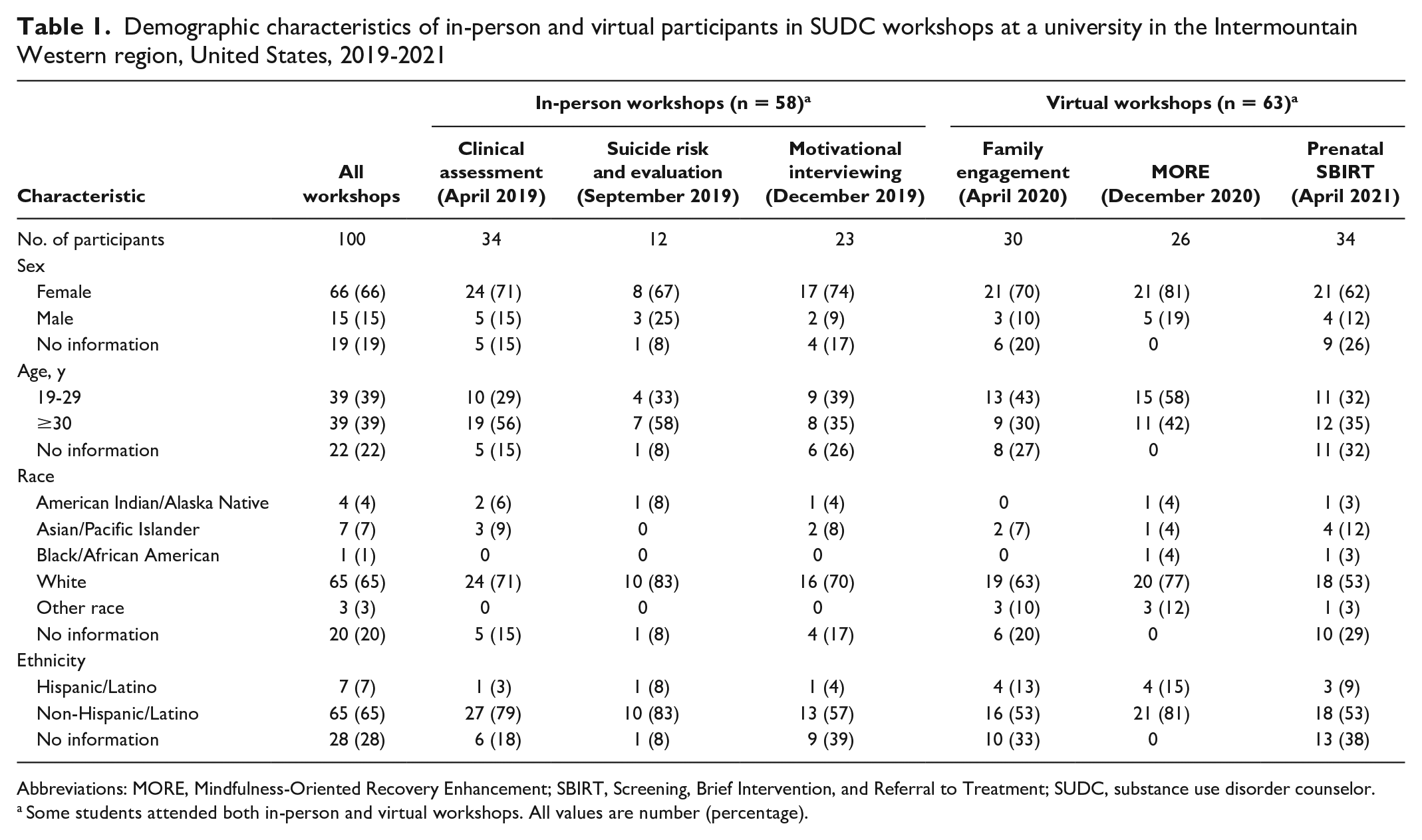
Abbreviations: MORE, Mindfulness-Oriented Recovery Enhancement; SBIRT, Screening, Brief Intervention, and Referral to Treatment; SUDC, substance use disorder counselor.
Some students attended both in-person and virtual workshops. All values are number (percentage).
Participants showed significant gains in knowledge in each of the 6 workshops and significant gains in self-efficacy in each of the 4 workshops that measured it (Table 2). For in-person workshops, the one on clinical assessment had the strongest effect on knowledge gain (Hedges g = 1.96; 95% CI, 1.38-2.53), followed by the workshops on motivational interviewing (Hedges g = 1.61; 95% CI, 0.94-2.27) and suicide risk and evaluation (Hedges g = 0.92; 95% CI, 0.08-1.76) (Figure 1). CL effect sizes indicated that student-trainees in the Clinical Assessment, Motivational Interviewing, and Suicide Risk and Evaluation workshops had a 93%, 92%, and 77% probability of increased knowledge from pretest to posttest, respectively, after controlling for individual differences (Table 2). Only the workshop on motivational interviewing assessed self-efficacy (Hedges g = 1.73; 95% CI, 1.04-2.43) (Figure 1), and CL effect sizes indicated 93% of reporting increased self-efficacy from pretest to posttest after controlling for individual differences (Table 3).
Pretest and posttest knowledge scores among paraprofessional SUDC student-trainees at in-person and virtual SUDC workshops at a university in the Intermountain Western region, United States, 2019-2021
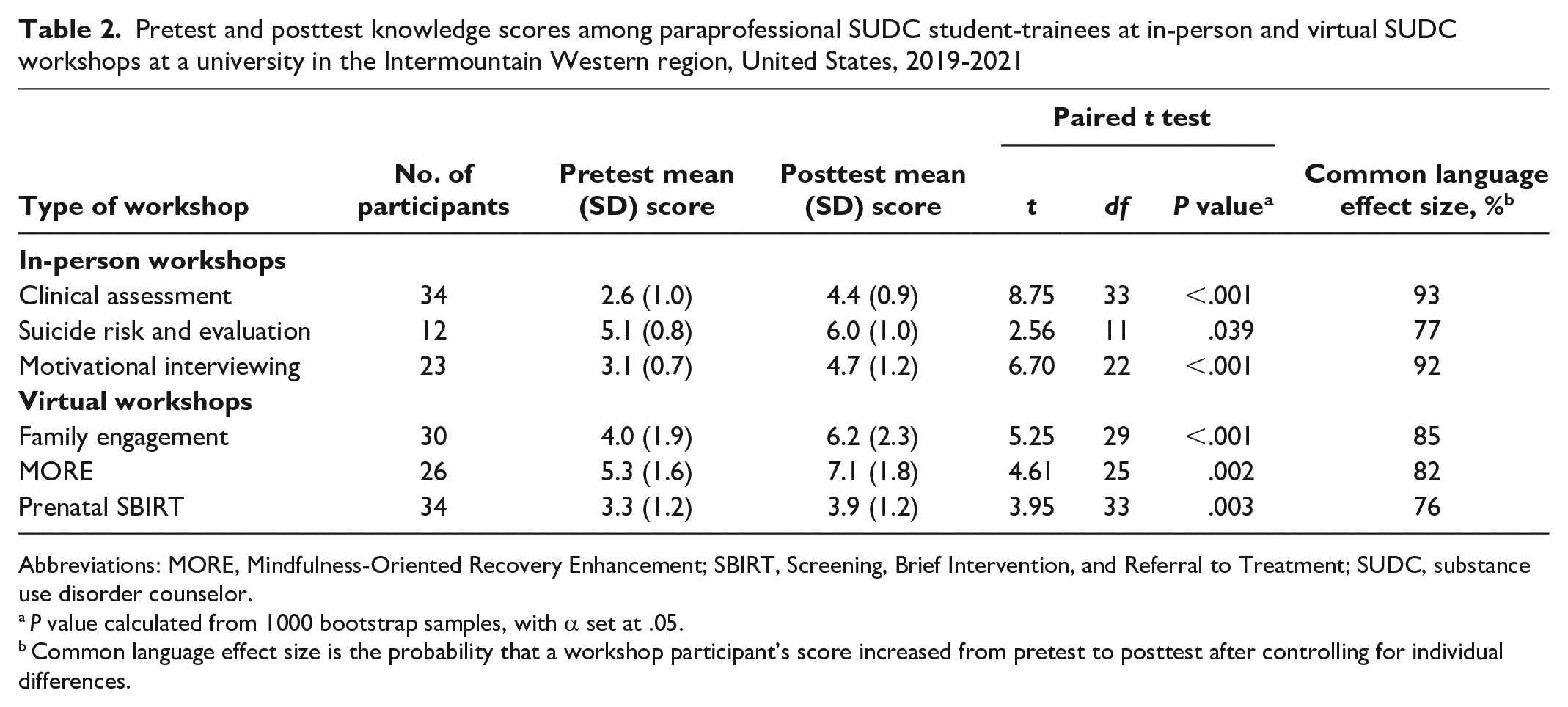
Abbreviations: MORE, Mindfulness-Oriented Recovery Enhancement; SBIRT, Screening, Brief Intervention, and Referral to Treatment; SUDC, substance use disorder counselor.
P value calculated from 1000 bootstrap samples, with α set at .05.
Common language effect size is the probability that a workshop participant’s score increased from pretest to posttest after controlling for individual differences.
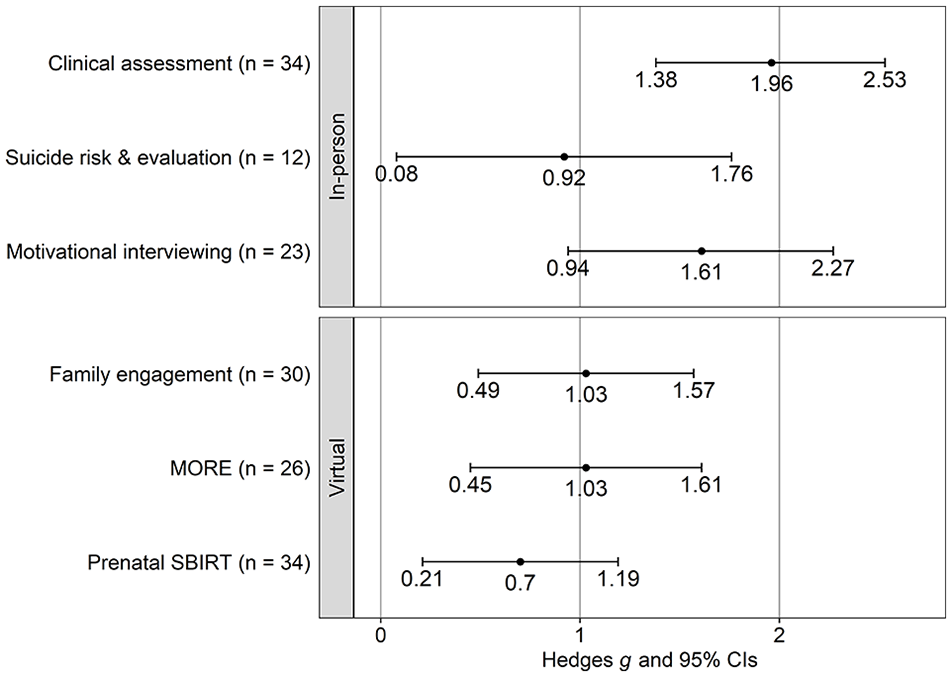
Standardized mean difference in knowledge scores from pretest to posttest among paraprofessional SUDC student-trainees at in-person and virtual workshops at a university in the Intermountain Western region, United States, 2019-2021. Error bars indicate 95% CIs. Abbreviations: MORE, Mindfulness-Oriented Recovery Enhancement; SBIRT, Screening, Brief Intervention, and Referral to Treatment; SUDC, substance use disorder counselor.
Pretest and posttest self-efficacy scores among paraprofessional SUDC student-trainees at in-person and virtual SUDC workshops at a university in the Intermountain Western region, United States, 2019-2021
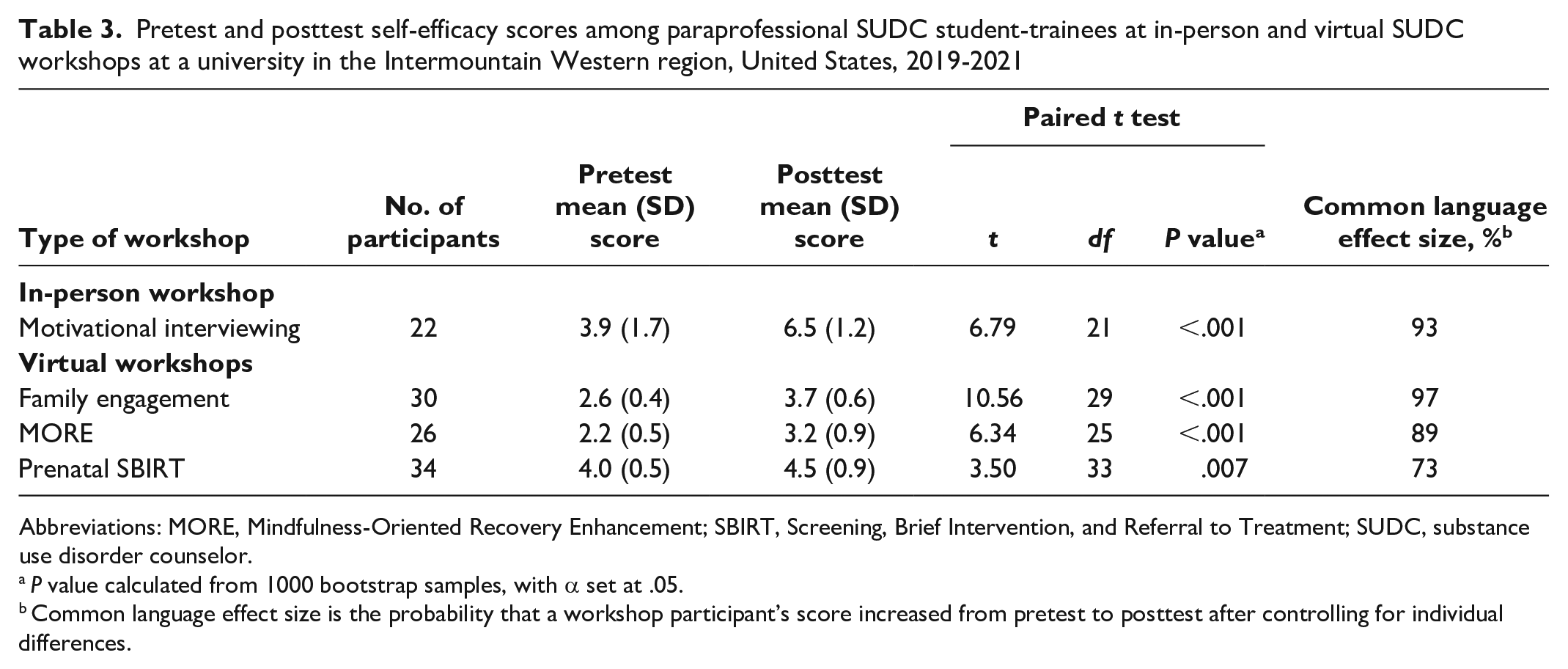
Abbreviations: MORE, Mindfulness-Oriented Recovery Enhancement; SBIRT, Screening, Brief Intervention, and Referral to Treatment; SUDC, substance use disorder counselor.
P value calculated from 1000 bootstrap samples, with α set at .05.
Common language effect size is the probability that a workshop participant’s score increased from pretest to posttest after controlling for individual differences.
For virtual workshops, the one on MORE showed the strongest effect on knowledge gain (Hedges g = 1.03; 95% CI, 0.45-1.61), followed by the workshops on family engagement (Hedges g = 1.03; 95% CI, 0.49-1.57) and prenatal SBIRT (Hedges g = 0.70; 95% CI, 0.21-1.19) (Figure 1). CL effect sizes indicated that student-trainees in the MORE, Family Engagement, and Prenatal SBIRT workshops had an 85%, 82%, and 76% probability of increased knowledge from pretest to posttest, respectively, after controlling for individual differences (Table 2). The workshop on family engagement showed the strongest effect on self-efficacy gain (Hedges g = 1.97; 95% CI, 1.35-2.58), followed by MORE (Hedges g = 1.26; 95% CI, 0.66-1.85) and prenatal SBIRT (Hedges g = 0.61; 95% CI, 0.12-1.10) (Figure 2). CL effect sizes indicated that student-trainees in the workshops on family engagement, MORE, and prenatal SBIRT had a 97%, 89%, and 73% probability, respectively, of reporting increased self-efficacy from pretest to posttest, after controlling for individual differences (Table 3).
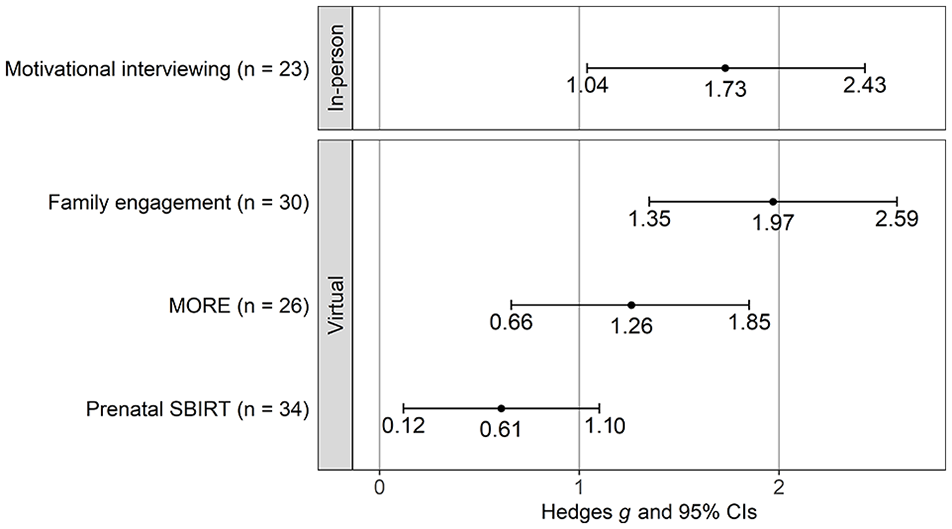
Standardized mean difference in self-efficacy scores from pretest to posttest among paraprofessional SUDC student-trainees at in-person and virtual workshops at a university in the Intermountain Western region, United States, 2019-2021. Error bars indicate 95% CIs. Abbreviations: MORE, Mindfulness-Oriented Recovery Enhancement; SBIRT, Screening, Brief Intervention, and Referral to Treatment; SUDC, substance use disorder counselor.
Discussion
Before 2020, the supply of licensed SUDCs in the United States was insufficient to meet the current and projected demand for SUD treatment by 2030.4,6 As a result, states and communities have enlisted paraprofessional SUDCs to provide many SUD treatment–related services under the direction of licensed SUDCs to expand access to SUD treatment. The COVID-19 pandemic has intensified the need for SUD treatment in the United States1,3 while disrupting educational programs that prepare new SUDCs to enter the workforce.12,13 The current study describes the effectiveness of 6 evidence-based trainings for paraprofessional SUDCs enrolled in an undergraduate SUDC certificate program: 3 occurring in person prior to COVID-19 and 3 occurring virtually after the onset of COVID-19. All workshops showed significant improvements in knowledge related to 6 evidence-based SUD treatment approaches. Four workshops also measured self-efficacy in delivering services related to specific SUD treatment modalities, and all showed significant improvements. Effect sizes for improvement in knowledge and self-efficacy were similar for workshops held in person and workshops held virtually. On average, in-person and virtual workshop participants had a 90% and 81% probability, respectively, of increased knowledge after the workshop. On average, in-person and virtual workshop participants had a 93% and 86% probability of increased self-efficacy after the workshop. These results indicate that workshops designed to train paraprofessional SUDCs in evidence-based SUD treatment modalities were not substantially derailed by challenges during the COVID-19 pandemic. Results also support sustained efforts to train paraprofessional SUDCs in diverse treatment approaches via in-person and online platforms.
To our knowledge, this study is the first to describe the effects of SUDC training before and during the COVID-19 pandemic. Prior to 2019, virtual training for SUDC students outside the United States had been shown to significantly improve knowledge related to a range of SUD treatment approaches. 22 These students, however, had knowingly enrolled in a virtual training program. Accounts from students enrolled in in-person health services education programs prior to the COVID-19 pandemic have signaled a strong dislike for the shift to online learning. 23 As such, it is encouraging to find that the SUDC students in the current study maintained similar knowledge and self-efficacy gains across the shift to online learning. Prior research suggests that self-efficacy is a particularly salient factor in supporting paraprofessional SUDCs’ willingness to deploy evidence-based SUD treatment. 11
Limitations
This study had several limitations. First, students were recruited for this study from a single certificate program at a single university. As a result, the effect sizes should be generalized to other universities or student groups with caution. Second, the current study did not compare SUDC classroom-based learning or field training before and during the COVID-19 pandemic. Given the results of the current study, we would expect similar knowledge gains across in-person and virtual classroom-based learning for SUDC students. However, challenges with safely completing the field education components of the SUDC certificate during COVID-19 were likely profound. 24 Further research is needed to understand the potential impact of disruptions to field education on the practice competency and self-efficacy of paraprofessional SUDCs entering the workforce. Finally, pretests and posttests for each workshop were yet to be validated as measures of knowledge or self-efficacy in each modality. While instruments were designed by practicing experts in each modality to match the content of each workshop on content validity, further examination of these measures in large samples is needed to establish statistical validity, refine these measures, and minimize measurement error. Future research should seek to establish validated instruments specific to paraprofessional SUDC education. Additionally, skill-based observational measures, whereby student-trainees demonstrate learning obtained via each workshop, can provide important evaluative information. Given the pressing need for paraprofessional SUDC support in SUD treatment, the results presented here should be interpreted as an incremental improvement upon current research. We encourage future researchers to conduct multisite investigations including multiple measures for effectiveness of SUDC education.
Conclusions
The results of the current study highlight the promise of in-person and virtual training to educate and expand the SUDC workforce. Given current and expected shortfalls in the supply of SUD treatment providers by 2030, innovative approaches to increasing training for licensed and paraprofessional SUDCs are necessary. Virtual training for SUDCs may also inherently support shifts to virtual SUD treatment modalities necessitated by the COVID-19 pandemic.25,26 Current shifts to technology-based SUD treatment services are likely to become an integral part of paraprofessional SUDC training in the near future and can increase the capacity of SUD treatment services in the United States. 26
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received the following financial support for the research, authorship, and/or publication of this article: This project was supported by the Health Resources and Services Administration of the US Department of Health and Human Services under M01HP31280 and the Behavioral Health Workforce Education and Training Program. This information or content and conclusions are those of the authors and should not be construed as the official position or policy of, nor should any endorsements be inferred by, the Health Resources and Services Administration, US Department of Health and Human Services, or the US government.