
Abstract
Background:
Graduate-level licensed addiction counselors are a critical component of the substance use disorder workforce, yet their scope of practice, education and training requirements, and credentialing varies in the U.S.
Objectives:
To better understand the roles and functions of the graduate-level addiction counselor workforce across the U.S., this state-by state analysis sought to identify the titles, minimum education and training requirements, scope of practice, and supervisory opportunities for graduate-level addiction counselors.
Design:
This project conducted systematic abstraction and descriptive analysis of U.S. state Practice Acts, certification board rules, materials from behavioral health professional organizations, and state Medicaid plans, fee schedules, and provider manuals.
Methods:
Descriptive summaries were produced to describe trends across states. Tables synthesized aggregated data across the workforce domains of education and training, regulation and credentialing, supervision, and payment for graduate-level addiction counselors only.
Results:
Forty-one states offer a graduate-level addiction counselor credential, 18 of which offer multiple credentials for a total of 69 credentials. States varied in services permissible by scope of practice definition, including assessments (41 states), psychotherapy (28 states), telehealth (28 states), and diagnosis (16 states). Only 26 states allow for independent practice. States required an average of 2,887 practice hours and 143 post-graduate supervision hours. Sixteen states permitted all tiers of graduate-level addiction counselors to supervise others, and 10 states specifically offer a graduate-level supervisory credential.
Conclusion:
State graduate-level addiction counselor credentials widely vary, suggesting that states utilize this workforce differently based on differing training criteria, required competencies, scope of practice, and supervision. Strategies to support growth of this workforce include alignment of training competencies, additional substance use disorder training in behavioral health graduate programs, and expansion of supervisory pathways and credentials.
Keywords
Introduction
The United States (U.S.) is increasingly facing a substance use disorder (SUD) crisis, and accessing treatment for SUD remains a persistent challenge given longstanding addiction care facility and clinician shortages. The prevalence of SUDs is widespread: among individuals aged 12 or older, 46.3 million people (16.5% of the U.S. population) met DSM-5 criteria for having a SUD in the past year. 1 Additionally, drug overdoses are the leading cause of injury deaths of U.S adults,2,3 and over 105,000 drug overdose deaths were reported in 2023. 4 Despite increased demand for SUD treatment, gaps in access persist and few people receive the addiction treatment services they need.5,6 It is estimated that less than 10% of individuals who need access to SUD care receive it, 7 even less so for minoritized populations,8,9 those living in rural areas, 10 and medically underserved communities lacking the health infrastructure and workforce to address SUD needs. 11
Addiction counselors comprise a broad workforce inclusive of paraprofessional, bachelor’s-level, and graduate-level professionals who provide SUD treatment. The graduate-level addiction counselor workforce continuum serves complementary functions within communities, including culturally relevant formal and informal education that supports substance use prevention and the SUD recovery process. 11 Graduate-level addiction counselors not only vary by education and training, but also by state-level certification and licensure requirements that determine scope of practice, supervision criteria, and ability to be reimbursed by insurance.12,13 Despite the importance of this workforce, the current supply of addiction counselors is not adequate to meet demand. Recent projections from the Health Resources and Services Administration (HRSA) estimated only 53% adequacy in meeting current U.S. SUD needs, 14 a predicted shortage of nearly 88,000 addiction counselors through 2036.
The existence of a graduate-level addiction counselor workforce in the U.S. is of growing importance given increased rates of SUDs and cooccurring mental health disorders, the diagnosis and treatment of which often require advanced knowledge and training. Graduate-level programs in addiction counseling are more likely than their non-graduate training counterparts to provide more extensive and complex training in addressing SUD challenges. Advanced training likely prepares graduate-level addiction counselors to operate more effectively in settings where they work alongside other behavioral health provider types, such as in integrated and collaborative care settings. Additionally, advanced training in SUD treatment provides a foundation for addiction counselors to practice independently and thereby help address nationwide behavioral health provider shortages.
State-based differences exist in the ability of graduate-level addiction counselors to diagnose, practice independently, supervise others, and be reimbursed for services. Graduate-level addiction counselors have varied educational training across behavioral health disciplines, supervision criteria, and often hold different titles, making it difficult to compare this workforce across states. Additionally, scope of practice—the range of services that a qualified health professional is legally permitted to perform in keeping with professional licensure or "certification”—impacts the capacity of this workforce to serve in SUD treatment. 15 As such, each state has varying scope of practice regulations and credentialing requirements for this workforce. Prior work reports on training, licensure, scope of practice, and other factors related to the addiction counselor workforce continuum, 13 specifically among non-graduate-level addiction counselors.13,16 However, the differences between graduate-level addiction counselors and those without graduate SUD-focused education warrants further discernment. While no consistent estimates as to what percentage of addiction counselors have a graduate degree are presently available, exploring the training and regulatory requirements for this workforce can elucidate education trends across states. Recent work has attempted to distil the nuances of the non-graduate workforce, 16 but to our knowledge, this study is the first of its kind to assess only graduate-level addiction counselors.
To better understand the roles and functions of the graduate-level addiction counselor workforce across the U.S., study researchers conducted a state-by state analysis to explore: (1) graduate-level addiction counselor titles; (2) minimum education and training requirements for credentialing at the state level; (3) scope of practice; and (4) opportunities to obtain a supervisory credential. These findings can help inform policy recommendations to expand the workforce’s capacity to meet SUD service and treatment needs throughout the U.S.
Methods
This project conducted systematic abstraction and comparative policy analysis of U.S. state Practice Acts, certification board rules, materials from behavioral health professional organizations, and state Medicaid documents (state plans, fee schedules, and provider manuals) for graduate-level addiction counselors across all 50 states and the District of Columbia. First, an abstraction guide that encompassed four domains was created: (1) title of addiction counselor credential; (2) minimum education and training requirements to be credentialed as a graduate-level addiction counselor; (3) scope of practice; and (4) opportunities for addiction counselors to obtain a supervisory credential. If states did not have a graduate-level addiction counselor title or role or specify the minimum education and training requirements as a graduate-level behavioral health degree, they were excluded from this analysis. For the purposes of this analysis, the term credential includes both certifications and licenses. Second, two members collected and abstracted data from the aforementioned state-specific documents and certification board materials between December 2023 and March 2024. Lastly, the information was reviewed and checked for accuracy by the study team. Information on scope of practice domains was identified through review of state regulations, licensing boards, and the Substance Abuse and Mental Health Services Administration (SAMHSA) SUD counseling competency framework.17,18
Descriptive summaries were produced to describe trends across states. Tables synthesized aggregated data across the workforce domains of education and training, regulation and credentialing, supervision, and payment for graduate-level addiction counselors only. Data for this study were built on prior efforts by the University of Michigan Behavioral Health Workforce Research Center Scope of Practice Tracker for behavioral health occupations in the U.S. 19 Study data collection met criteria for non-human subject research and did not require university IRB approval.
Results
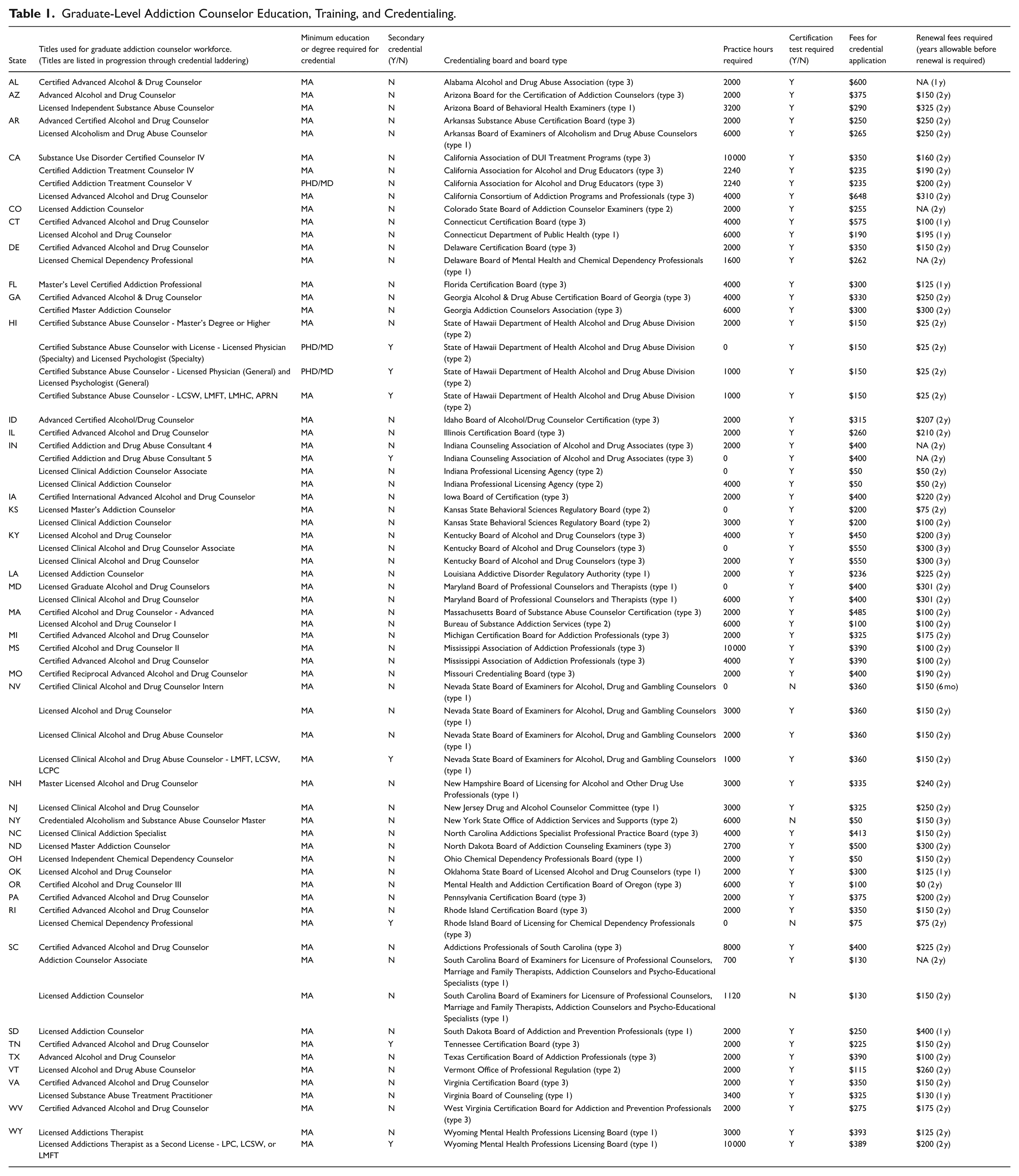
Forty-one U.S. states currently offer a graduate-level addiction counselor certification or license, and 18 of those states have more than one license or certification. A total of 69 graduate-level addiction counselor credentials were identified and analyzed. Thirty-one states (76%) relied on only one type of credentialing body to recognize addiction counselors, while 10 states (24%) allowed multiple types of organizational bodies to provide credentialing. Table 1 provides a summary of how states identified graduate-level addiction counselor titles, minimum education and training requirements, and scope of practice allowances.
Graduate-Level Addiction Counselor Education, Training, and Credentialing.
Addiction Counselor Credential Titles
The most common titles across the 41 states were Certified Advanced Alcohol and Drug Counselor (23%; n =16), followed by Licensed Alcohol and Drug Counselor (7%; n =5) and Licensed Clinical Alcohol and Drug Abuse Counselor (7%; n =5) titles. Twenty-five states required licensure for graduate-level addiction counselors, 27 states articulated a certification for graduate-level addiction counselors, and 12 states offered both licenses and certifications. Eighteen states (44%) offered multiple credential types. For example, California offered four levels: (1) SUD Certified Counselor IV (California Association of DUI Treatment Programs credential); (2) Certified Addiction Treatment Counselor IV (California Association for Alcohol and Drug Educators credential); (3) Certified Addiction Treatment Counselor V; and (4) Licensed Advanced Alcohol and Drug Counselor (California Consortium of Addiction Programs and Professionals credential).
Minimum Education, Training, and Supervision Requirements to Obtain Credential
States had varied educational degree requirements to obtain an addiction counselor credential (Table 1). All states included in this study required completion of a master’s degree or higher, yet the type of degrees varied. About a quarter of credentials (23%; n =16) specified any “behavioral science” as the required degree, with an additional 17% (n =12) specifying a “clinical behavioral science” degree. However, the majority (31%; n =22) of credentials required a degree in a “relevant field.” Some states provide examples of “relevant field,” with the most common including counseling, clinical counseling, human services, clinical human services, and clinical mental health counseling.
States also varied in the number of supervised practice hours required for credentialing. The average number of required supervised practice hours was approximately 2,887 hours, though 2000 hours was the most common in 26 states. States did not specify supervised practice hours as having to be completed pre- or post-awarding of a graduate degree.
Distinct from practice hours, 36 states required post-graduate degree supervision hours for at least one of the credentials offered in each respective state. Hourly requirements ranged from zero (e.g., Colorado) to 400 (e.g., Hawaii) hours. The average amount of required supervised time across these 36 states was 143 hours, though the most commonly set hourly requirement was 300 hours observed in 17 of the 36 states. Only five states (Colorado, Georgia, Kansas, Nevada, Oregon) did not specify a minimum number of supervised hours to be completed.
States did not define differences between practice hours and supervision hours; however, these hour requirements were sometimes described differently. For example, the practice hours requirements for licensed addiction counselors in North Carolina specified that prospective addiction counselors must have completed two years of post-graduate supervised SUD counseling experience, while the supervision hours requirement for this occupation specified needed documentation of a minimum of 300 completed supervised practical training hours as well as a board-approved supervision contract between the applicant and an applicant supervisor.
Almost all the 41 total states (95%; n =39) that offer a graduate-level addiction counselor credential require passage of a certification exam for at least one credential, with the exceptions being New York and Nevada. The average cost of pursuing a graduate-level addiction counselor credential, including application and exam fees, was approximately $305 (range $50-$648). Credentialing exams were not standardized across states, and no two state examinations were from the same credentialing body. Organizations offering credentialing opportunities were all at the state level and included addiction professional-specific, behavioral health (including counseling and mental health), and general state credentialing boards offering certifications across non-addiction occupations. Opportunities for dual certification are available in some states. Most states do not specifically require a base certification (e.g., an entry-level or introductory addiction counselor-specific credential) for master’s degree-holding individuals to obtain an addiction counselor credential. Some states, such as Hawaii and Wyoming, utilize a secondary credential model whereby licensed behavioral health professionals (e.g., psychologists, physicians) can use their existing license as a base credential to obtain an addiction counseling credential without having to accrue additional practice hours. Only one state (New York) requires addiction counselors to have maintained initial addiction counselor-specific certification for a set duration before becoming eligible to pursue an advanced credential.
Scope of Practice
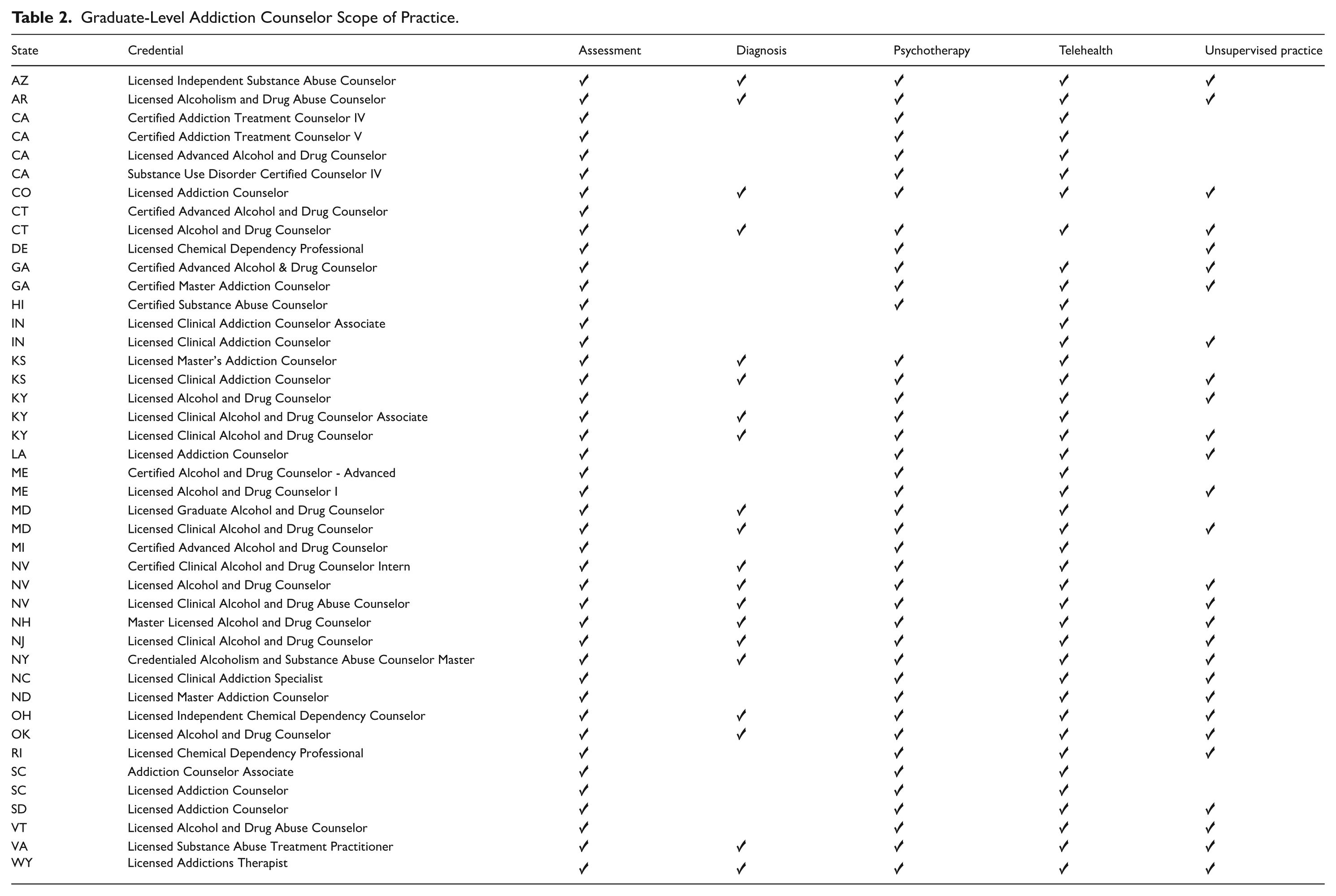
Findings indicate that the services that graduate-level addiction counselors are permitted to provide differ by state and credential. Out of the 41 states offering graduate-level addiction counselor credentials, 29 states have scopes of practice in their statutes or administrative code associated with at least one of their credentials, encompassing a total of 43 distinct credentials with scopes of practice. While licenses included in state statutes or administrative codes have a defined scope of practice, not all certifications do. Seventy-one percent of states permit at least one addiction counselor credential to provide assessments in their statute or administrative code (n =29); 68% of states permit at least one addiction counselor credential to provide psychotherapy (n = 28); 66% of states permit at least one addiction counselor credential to provide telehealth (n =27); 61% of states permit at least one addiction counselor credential to practice independently (n = 25), and 39% of states permit at least one addiction counselor credential to diagnose (n = 16; Table 2). Some states with multiple addiction counselor credentials provide multiple scopes of practice. For example, Connecticut’s Licensed Alcohol and Drug Counselor is permitted to provide assessments, telehealth, psychotherapy, diagnoses, and practice independently, while the state’s Certified Advanced Alcohol and Drug Counselor is only permitted to provide assessments.
Graduate-Level Addiction Counselor Scope of Practice.
In addition to differences in service provision, states also vary in their policies regarding the supervision of other addiction counselors. In some states, graduate-level addiction counselors are not required to hold a separate credential specifically for supervisory roles. For example, 16 of the 41 states with graduate-level addiction credentials permit all types and tiers of graduate-level credentials (e.g., entry-level, advanced) to supervise others, 9 of the 41 (22%) permit at least one, but not necessary all, graduate-level addiction counselor credential to supervise others, and 16 of the 41 (39%) do not specifically allow graduate-level addiction counselors to serve in a supervisory capacity.
Opportunity for Supervision Credential
Eleven states offer one or more graduate-level supervisor credentials (California, Iowa, Indiana, Michigan, North Carolina, New Jersey, Ohio, Rhode Island, South Carolina, Virginia, Wyoming; Table 3). The range of practice hours required to become a supervisor in these states ranges significantly from zero to 10,000 hours (five years), with an average amount of 5,467 hours. In most of these states with a supervisory credential (55%; n = 6), passing a certification exam is required for all supervisory credentials in the state. Two states (North Carolina and South Carolina) require passing a certification test for at least one supervisory credential in their state, and three states (Indiana, Virginia, and Wyoming) do not require examination for any supervisory credentials in their state.
Graduate-Level Supervisor Addiction Counselor Education, Training, and Credentialing.

Non-graduate level credential.
Discussion and Policy Implications
Addiction counselors are a critical workforce tasked with addressing chronic, serious behavioral health issues that require a trained, skilled, and compensated workforce who can continue to do this work with clear training, regulation and payment mechanisms. Despite this, there are inconsistencies in the type of educational requirements, credentialing criteria including examination and training hours, and an overall lack of uniformity across states. To date, few studies have explored the education and training pathways to becoming an addiction counselor at the graduate level. Further, there is a paucity of work examining the role of supervision required for becoming a graduate-level addiction counselor, or for being able to provide supervision for others in the addiction field. This study contributes to the body of research by addressing knowledge gaps around state-level differences in education/training requirements and scope of practice allowances/restrictions for the graduate-level addiction counselor workforce. The following policy and institutional recommendations are potential strategies to help strengthen the graduate-level addiction counselor workforce and expand the accessibility of a workforce who can address SUD.
SUD Training in Requisite Graduate Degree Programs
Although most states had a graduate-level addiction counselor credential, eight states did not—suggesting that in these states, professionals with other licenses are serving in the graduate-level workforce to treat addiction (i.e., licensed clinical social workers or licensed mental health counselors). Though it is unclear if states with a credentialed graduate-level workforce have better access to SUD treatment, graduate-level addiction counselors represent a workforce that is easily identifiable for serving in this role. Relatedly, although other professional licenses can work in addiction care, there is no formal requirement for training in SUD and addiction content being included within these programs or licensure exams—including those occupations such as mental health counselors and social workers for whom diagnosis and independent practice are in their scope of practice. 20 Resultingly, completion of a graduate-level behavioral health degree does not guarantee exposure—if at all—nor depth of SUD training in coursework or clinical internships. Prior work examining SUD content in Master of Social Work (MSW) education has noted how little SUD content is included,21,22 with one study reporting that only 64% of the 58 MSW programs reviewed offered a substance use elective. 23 Another noted that 14.3% of accredited schools of social work offered a specialization in SUD at the time of the study, and less than 5% of accredited schools had one or more required SUD-related courses in their curricula. 24 In contrast, a study assessing SUD content in graduate behavioral health programs identified 67 of 97 (69%) master’s-level counseling programs reviewed required at least one course in SUD with only 12 offering at least one elective in SUD. 23 A review of this literature suggests that, in the U.S., behavioral health training differs across program types, curriculum, and/or accreditation standards.
Competencies to Clarify Role and Scope of Practice
Addiction counselor roles, permitted services, and titles vary across states, and the core functions of the occupation are not clearly defined at a national level. The creation of new competencies, understood as those criteria intended to serve as an empirically based blueprint to guide trainee occupational development, 25 could help clarify for prospective trainees what addiction counselor professions will encompass. While some credential programs require completion of SUD-specific coursework, training in addiction treatment is not universally present in program curricula. Credentialing bodies might consider developing new or expanding existing competencies for addiction counselors and addiction counseling education and training programs to help ensure more uniformity.
Furthermore, the benefits of role and scope of practice consistency reach beyond the workforce itself. This clarity is equally as important for the consumers of care provided by graduate-level addiction counselors as it is for addiction counselors themselves. Clear guidelines on core functions and competencies graduate-level addiction counselors are required to master is an important method of standardizing the types of services and quality of care that individuals receive from addiction counselors regardless of jurisdiction.12,17, 26 Efforts to standardize the training and education of graduate-level addiction counselors would help to ensure that reliable evidence-based information is being conveyed, especially given the wide variability that currently exists across training programs. It is important to note that exiting standards were not explicitly created for graduate-level addiction counselor programs, contributing to inconsistency of SUD content within graduate-level training programs.
Existing competencies could serve as a base for guiding the development of new training program competencies. For example, the Council for Accreditation of Counseling and Related Educational Programs (CACREP) published updated guidance in 2024 on standards for the eight specialty areas it recognizes, 13 standards of which are specific to addiction counselors. 27 This guidance was intended to simplify and clarify accreditation requirements for programs and to promote a unified counseling profession. 27 Additional resources such as the SAMHSA “TAP 21,” a frequently updated list of more than 120 competencies, could be used to develop and evaluate addiction counselor curricula, advise trainees and students, and assess counseling proficiencies. 17 Per the TAP 21 competency framework, SUD counselors should achieve proficiency in 8 practice dimensions: clinical evaluation; treatment planning; referral; service coordination; counseling; client, family, and community education; documentation; and professional and ethical responsibilities. 18 Similarly, SAMHSA’s “TIP 22” is a treatment improvement protocol and professional development guide for substance use counselor supervisors that can be utilized for its focus on counselor development, professional and ethical standards, program development and quality assurance, performance evaluation, and administration. 28 Lastly, SUD curricula piloted in countries outside the U.S., such as the European Prevention Curriculum (EUPC) designed for professionals involved in shaping prevention decisions and policies and Europe, could function as a model for implementing a standardized prevention training curriculum across states. 29
Expansion of Supervisory Pathways and Credentials
The importance of including quality supervisory training in behavioral health programs cannot be overstated. Prior work demonstrates the effectiveness of clinical supervision in systematically developing trainee skills and improving work satisfaction. 28 Additionally, a study of individuals with direct care responsibilities in drug treatment units found that individuals working in a managerial or supervisory position were more likely to endorse evidence-based practices than did support staff. 30 The availability of competent clinical supervisors is critical as demand for SUD services continues to increase, particularly for those clients who experience complex comorbidities and psychosocial constraints and may require specialized care. 31 However, prior work indicates that counselors may sometimes be promoted to supervisory roles with little or no training. 28 This study identified that opportunities to achieve a supervisory role are limited or nonexistent in some states—as only 11 states currently offer supervisor credentials and, among these, the respective practice hour requirements for earning a supervisor credential vary dramatically. It is possible that the current wide variation in state-level practice hour requirements may create incongruence on the significance, purpose, and meaning of attaining a supervisory credential. This variability may impact the portability of graduate-level addiction counselor credentials as efforts to obtain a supervisory credential may not be transferable across state-lines.
The lack of opportunities for career advancement and professional growth in the field presents a significant challenge to retaining addiction counselors in the behavioral health workforce. 27 Expanding opportunities for graduate-level addiction counselors to pursue a supervisory role and increasing availability of supervisor credentials in states currently lacking them will be necessary for ensuring a well-prepared workforce. Greater availability of supervisor training and credentialing could also support the workforce more broadly by increasing trainees’ interest in continuing a career in SUD treatment, allowing them to highlight their advanced training and specialization in addiction. Working toward a supervisory credential could help increase a worker’s sense of responsibility, expertise, and professional development, though further investigation is required to determine how to best incentivize pursuing a supervisor credential. 16
Recruiting Future Trainees
Lastly, continued growth of the graduate-level addiction counselor workforce is integral for addressing SUD treatment needs. Presently, there are few resources available to outline what degrees and training programs prepare prospective trainees for graduate-level addiction counseling, and it is unclear what degree concentration or type will transfer to a licensed role. State-level credentialing bodies might consider developing educational and training guidelines for prospective addiction counselors, with an emphasis on bachelor’s to master’s degree pathways, supervisory credential opportunities, and any dual certification options. Additionally, reduced-cost training for prospective graduate-level addiction counselors could also help increase this workforce. To enhance recruitment efforts, policymakers and training institutions might consider developing scholarships and grant funding opportunities for graduate-level entrants to help offset education and training costs across behavioral health programs. Support to develop evidence-based SUD curricula and evidence-based education on addiction could help ensure minimum standards and perhaps expand SUD content. Further, funding mechanisms, such as the former Opioid Workforce Expansion Program (OWEP) to enhance community-based training for students preparing to become behavioral health professionals, are one strategy to grow the opioid-focused workforce and expand the behavioral health workforce trained in addiction. However, this mechanism was only available for one funding cycle (2019-2023) and has not been reinstated. 32
Limitations
Findings from this U.S. based state-by-state analysis should be considered in light of identified limitations. First, the analysis relied on state-level data, which varied in accessibility, quality, completeness, and reporting standards across U.S. states. Such variability may affect the comparability of results as the research team might have inadvertently included outdated or missing data. Second, the study design is observational and descriptive in nature, and the data do not allow for more in-depth analysis on per/population ratios of the addiction counselor workforce adequacy in each state. Relatedly, a power analysis was not performed because the sample was determined by state regulations and documents, rather than through a probabilistic or random sampling process and as such, the focus was on completeness and relevance instead of statistical power. Third, unmeasured confounding variables—such as differences in state-level health and social investment (i.e., Medicaid expansion, opioid settlement funding), economic conditions, SUD and health care infrastructure, or public attitudes about addiction services—may influence both the adoption of addiction counselor workforce policies, potentially biasing the results. The heterogeneity in how policies are implemented and enforced across states complicates direct comparisons, as nominally similar policies may differ substantially in practice. Additionally, temporal and geographic differences may not fully capture the long-term effects of workforce policies, or the potential effects of addiction services that are accessed and serviced by workers who may live in one state but work in another. Future work is needed to assess the portability of addiction counselor credentials and training across state lines. Finally, we recognize this study is U.S.-based and these workforce issues may not be generalizable to other country and health system contexts.
Conclusions
This state analysis highlights the wide variability of graduate-level addiction counselor titles, education and training requirements, scope of practice, and supervision. As states work to increase the SUD workforce, clearly articulating and understanding the way in which graduate-level addiction counselors are prepared and trained is necessary to meet current SUD treatment demands. Given only a small number of states offer supervisory role opportunities, limiting the potential for career advancement within the addiction counselor profession, expanding opportunities for becoming a graduate-level supervisor is important.
Supplemental Material
sj-docx-1-sat-10.1177_29768357251390304 – Supplemental material for Understanding the Graduate-Level Addiction Counselor Workforce: Differences in Educational Standards, Scope of Practice, and Supervisory Opportunities Across the United States
Supplemental material, sj-docx-1-sat-10.1177_29768357251390304 for Understanding the Graduate-Level Addiction Counselor Workforce: Differences in Educational Standards, Scope of Practice, and Supervisory Opportunities Across the United States by Maria Gaiser, Lisa de Saxe Zerden, Libby Daberko and Brianna M. Lombardi in Substance Use: Research and Treatment
Footnotes
Author Contributions
LZ and BM conceived and designed the study. Data collection and analysis were performed by MG and LD. LZ and BM supervised the project. All authors discussed the results and contributed to the final manuscript. All authors provided critical feedback and helped shape the research, analysis and manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Substance Abuse and Mental Health Services Administration (SAMHSA) and the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) under grant number U81HP46529 Cooperative Agreement for a Regional Center for Health Workforce Studies for $1,121,875. This information or content and conclusions are those of the author and should not be construed as the official position or policy of, nor should any endorsements be inferred by SAMHSA, HRSA, HHS or the U.S. Government.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.