
Abstract
Background:
Despite increased demand, few people receive the addiction services they need, and substance use disorders (SUD) workforce shortages persist. Addiction counselors are a workforce that can help address SUD needs. However, recent projections highlight national shortages of nearly 88 000 addiction counselors through 2036. Given state variations, it is difficult to discern how high school- and bachelor’s-level (HS/BA) addiction counselors are defined based on education and training, state credentialing requirements, and Medicaid reimbursement allowances.
Methods:
A state policy analysis across all 50 states and Washington, DC was conducted from November 2023 to June 2024. A systematic review of state Practice Acts, credentialing rules, and guidance documents from licensing bodies and state organizations was conducted to extract: (1) titles and degree classifications, (2) credentialing and examination requirements, (3) supervision, and (4) Medicaid state plans.
Results:
There are 160 credentials offered across all 50 states and DC across high-school (n = 56; 35%), associate’s (n = 25; 16%), and bachelor’s (n = 59; 37%) degrees. Only 3 states (AZ, NY, TX), offer addiction counselor credentials across all degree types. Thirteen states do not specify a degree but instead require training hours. However, the number of credentials offered per state ranges (1-16), and there is wide variability in how HS/BA addiction counselors are credentialed. Forty states allow some type of Medicaid reimbursement for HS/BS addiction counselors, while 11 states do not.
Conclusion:
Addiction counselors are a critical workforce tasked with addressing SUD. To do so, they require clear training pathways, regulations, and payment mechanisms. Findings highlight wide variability within the addiction counselor workforce at the HS/BA level, including inconsistencies in minimum educational requirements and training hours, as well as an overall lack of uniformity across states. Clearly articulating addiction counselor career pathways is necessary to simplify and enhance states’ SUD workforce. Identifying Medicaid and other reimbursement mechanisms is an important way to further expand how the SUD workforce is deployed to meet increased addiction-related needs.
Highlights
Significant variation in how high school- and bachelor’s-level (HS/BA) addiction counselors are defined based on state credentialing requirements, education, and training criteria, as well as Medicaid reimbursement.
The number of addiction counselor credentials (N = 160) offered across all 50 states and DC varies and differs by education. Addiction counselors can be those with a high-school degree or equivalent (n = 56 credential types); associate’s degree (n = 25); or bachelor’s degrees (n = 49). Thirteen states do not specify the type of education/degree but instead require training from none to 360 hours.
Seventeen states have multiple types of organizational bodies for HS/BA addiction counselors.
Introduction
The United States continues to face a national behavioral health crisis related to drug use and substance use disorders (SUD). Among individuals 12 or older in 2023, more than 70 million—nearly 25% of the US population—used illicit drugs in the past year, and 48.5 million people aged 12 or older (17.1% of the US population) met DSM-5 criteria for having a SUD in the past year. 1 The severity of drug use and drug-related deaths has risen precipitously and can be attributed largely to synthetic opioids. From 2013 to 2019, the age-adjusted rate of death involving synthetic opioids increased by more than 1000%. 2 In addition, deaths related to excessive alcohol use are also concerningly high, with an estimated 1 in 8 deaths among individuals 20 to 64 years old being attributed to it. 3 As a result of the prevalence and severity of alcohol and drug use nationwide, attention to the SUD treatment workforce has become a national priority. 4 Despite increased demand for SUD treatment, gaps in access persist, and few people receive the addiction treatment services they need.5-7 Treatment barriers are even worse for people from minoritized backgrounds,8,9 rural areas,10,11 and in communities with high social and economic needs.12,13
The Addiction Counselor Workforce
Addiction counselors can help address behavioral health and SUD workforce shortages.14-17 Recent projections from the Health Resources and Services Administration (HRSA) forecasted a shortage of nearly 88 000 addiction counselors through 2036, reflecting only 53% adequacy in meeting demand. 18 However, there is currently no standardized definition or title for an addiction counselor. The Substance Abuse and Mental Health Services Administration defines addiction counselors as those who work with and advise people on issues related to substance use in a variety of settings, 19 while HRSA (2018) defines addiction counselors as those who provide treatment and support to persons who suffer from addiction to alcohol and other drugs, or other behavioral health issues. 20 These differing definitions have resulted in various titles being used to identify the role of addiction counselors, including drug counselors, opioid agonist treatment counselors, and alcohol and drug counselors.15,21 This has led to observed variability across states in how addiction counselors are understood and defined. Because the workforce providing SUD treatment includes a continuum of occupations with varying levels of training and educational backgrounds, 17 it is difficult to discern state-by-state variations within this workforce. Additional factors complicating the addiction counselor workforce landscape include variations in degree and education requirements which range from completion of high-school (HS) to graduate degrees; Medicaid reimbursement eligibility; employment settings; state scope of practice regulations14,17; and credentialing bodies. 15
National behavioral health workforce estimates largely represent those addiction counselors who practice with a graduate degree and/or within licensure regulations. However, addiction counselors practicing with solely HS, associate’s level (AA), bachelor’s-level (BA) degrees make up a large proportion of the total addiction counselor workforce and serve in roles that may address different patient population needs or challenges than licensed, graduate-level addiction counselors. For the purposes of this article, the term “addiction counselors” is used to describe members of the SUD workforce who received an HS to BA education only as they are an understudied workforce that receives minimal attention in policy and research despite filling roles providing important clinical services. Concurrent regulation of training, licensure, certification, and payment for this workforce is critical for ensuring its effective deployment to meet growing behavioral health needs.22,34
Given the nuances involved in defining this workforce, the first step—and the primary purpose of this study—is to better understand the variations in training, regulation, and compensation that exist within it. This analysis sought to identify how and where differences occur and identify gaps in training requirements through 3 aims:
Identify and describe state-level credentials (ie, certifications and licensure) for HS/BA-level addiction counselors.
Define training requirements for HS, AA, and BA-level addiction counselor workforce (ie, required supervised practice hours and examinations); and
Identify opportunities for laddering addiction counselor credentials for professional advancement within the workforce.
Knowing how addiction counselors are classified can help determine what regulatory factors and payment mechanisms may be helpful to enhance SUD service delivery for the workforce that is available. This analysis specifically focuses on Medicaid because it is the nation’s largest payer for behavioral health services and because nearly 12% of Medicaid enrollees aged 18 and older have SUD. 23 In addition, findings from this descriptive analysis may help illuminate gaps and clarify entry points into the SUD workforce. Findings may illuminate gaps and clarify entry points into the SUD workforce at varying levels of education and training. In addition, this analysis may assist in identifying ways to better retain addiction counselors and more clearly define career laddering—a workforce term for the steps within a job classification used to demarcate increases in knowledge or responsibility—for the addiction counseling profession. 24
Methods
Data for this project were compiled by the study team in spring 2024 using data collected across all 50 states and the District of Columbia. This work was built on prior efforts by the University of Michigan Behavioral Health Workforce Research Center, 25 which developed a Scope of Practice Tracker that compiled publicly available information on state statutes and rules, education and training requirements, and permitted services for practice for each state. The current project required systematic abstraction and extraction of state Practice Acts, certification board rules and guidance documents, and professional association materials, as well as state Medicaid plans, fee schedules, amendments, and provider manuals. Two members of the study team extracted data and completed checks of collected data to ensure consistency, and all data were reviewed by all study team members. This study was a policy analysis utilizing publicly available, non-human subject research and therefore did not require university IRB approval (see Table 1).
Data Extraction Strategy.
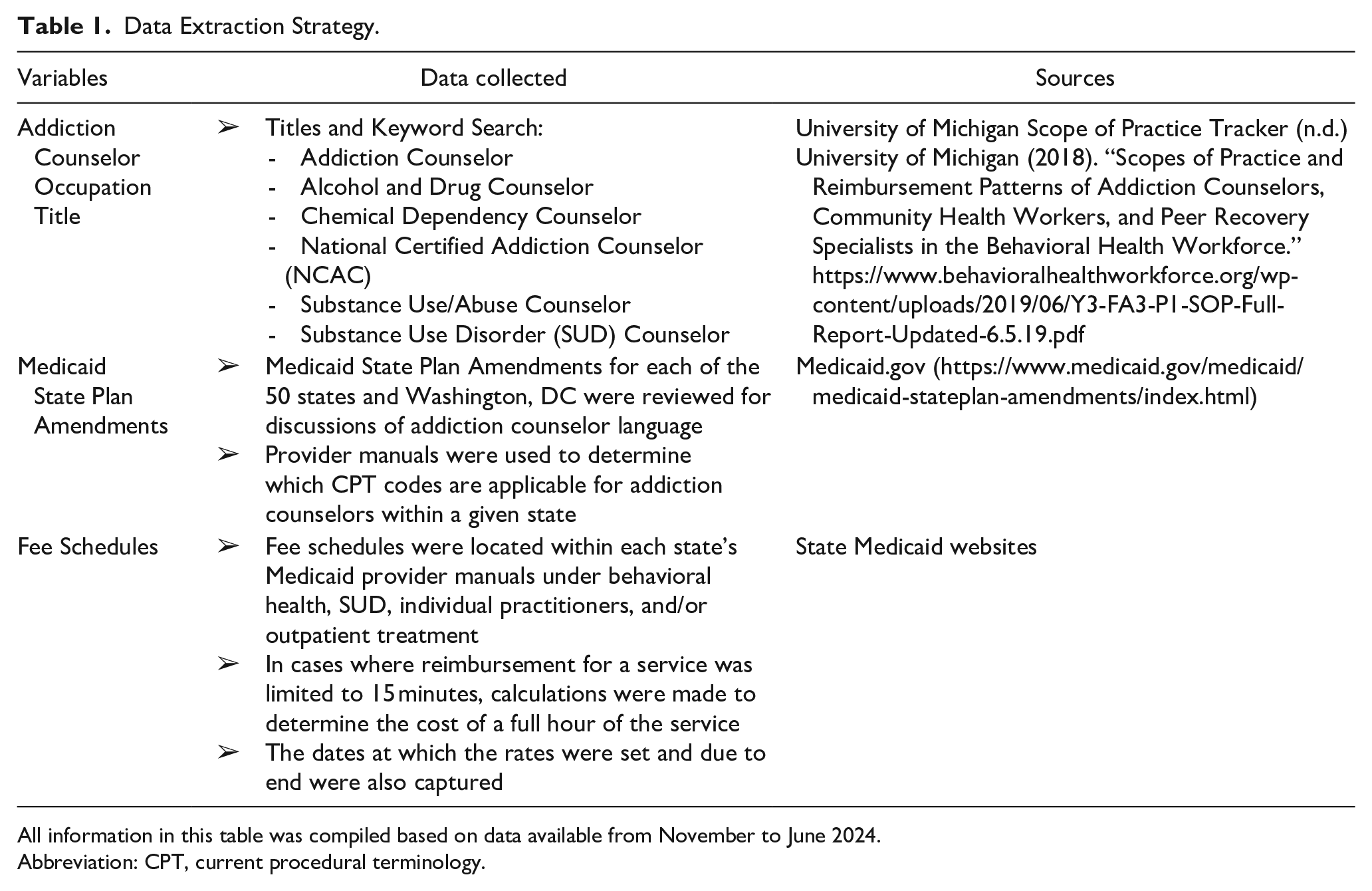
All information in this table was compiled based on data available from November to June 2024.
Abbreviation: CPT, current procedural terminology.
The study team obtained education, training, and practice requirements for each state’s specific addiction counselor credential types through an internet search. Fee schedules for mental health and SUD services were identified for each state using Medicaid provider manuals to determine reimbursement rates for services provided by addiction counselors. Instances of reimbursement rates limited to 15-minute increments were multiplied by 4 to manually calculate the total cost per hour. The start and expiration dates for each rate were recorded to ensure consistency. Current procedural terminology (CPT) codes addiction counselors are permitted to bill for were identified for each state in addition to allowable provider types, definitions of each CPT code, and whether telehealth services billed using each code are covered.
The study team created an abstraction table to house identified and systematically collected information obtained from each state’s reviewed documents. Data collection included the following 4 domains based on available state data through July 2024: (1) addiction counselor titles and minimum educational requirements to be credentialed; (2) credentialing information, including credentialing body, exam requirements, and associated fees; (3) supervision requirements; (4) Medicaid reimbursement allowances. Once the data was extracted across all 50 states and Washington, DC, the study team produced descriptive data to synthesize findings. Data regarding fees, education, and supervision requirements were systematically calculated by the study team through a review of credentialing body websites. Tables were created to aggregate data across the workforce domains of education and training, regulation and credentialing, and payment for addiction counselors with HS, AA, and BA-level degrees.
Results
Education and Training
Overview by State and Degree
There were 160 total credentials found to be offered across all 50 states and DC, of which 56 were at the HS level, 25 at AA, and 49 at BA. Thirteen states did not specify the type of degree but instead required training hours of up to 360 hours. More than half of all states (n = 29, 57%) offered at least one type of addiction counselor credential for individuals with an HS degree; one-third of states (n = 17) offered at least one credential for those with an AA degree, and 30 states (59%) offered at least one type of credential for those with a BA degree (see Table 2). Only 3 states (AZ, NY, and TX), have addiction counselor credentials across HS, AA, and BA-level degrees. The number of credentials offered in each state ranged from 1 to 16. For example, 10 states, including DE, KS, MI, MT, NC, NH, NJ, OK, SC, and WV) each only offered one type of addiction counselor credential, whereas CA offered 16.
Overview of Addiction Counselors by Title, Education, Training, Regulation, and Medicaid Reimbursement.
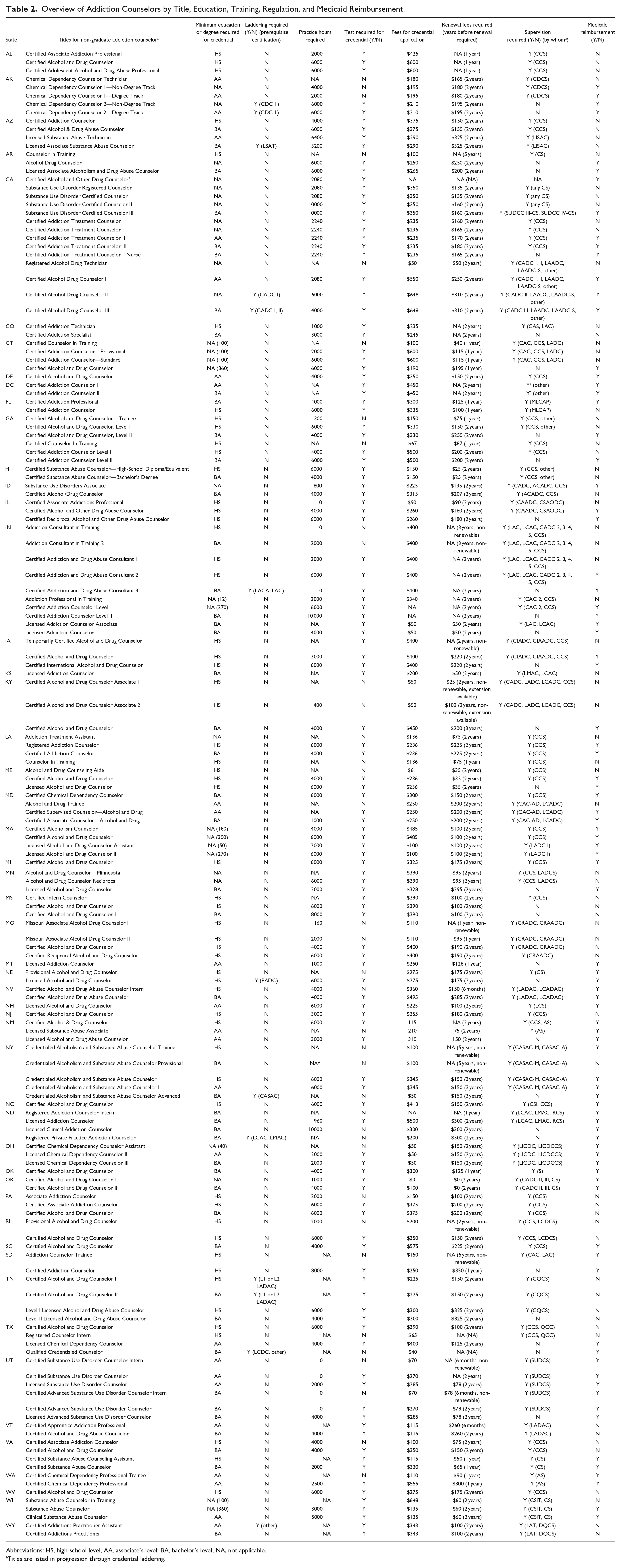
Abbreviations: HS, high-school level; AA, associate’s level; BA, bachelor’s level; NA, not applicable.
Titles are listed in progression through credential laddering.
Laddering and Career Progression
Most states offered a ladder of addiction counselor credentials, indicating the opportunity to progress within the addiction counselor workforce. For some states, each step on the addiction counselor career ladder reflected the attainment of a higher degree or additional practice hours required to obtain more advanced credentials. For example, laddering of credentials was observed in the Georgia Alcohol and Drug Abuse Certification Board’s 3 Certified Alcohol and Drug Counselor (CADC) credentials offerings (see Table 2): CADC Trainee, CADC Level I, and CADC Level II. The CADC Trainee credential requires an HS degree and 300 practice hours. The CADC Level I credential requires an HS degree and 6000 practice hours. Finally, the CADC Level II credential requires a bachelor’s degree and 4000 practice hours.
Regulation and Credentialing
Regulatory Body and Fees
Two-thirds of states (67%, n = 34), relied on only one type of credentialing body to recognize addiction counselors, while 17 (33%) allowed multiple types of organizational bodies to provide credentialing (see Figure 1). Of the states that employed only one type of credentialing body, 14 (41%) used on occupational licensing boards (eg, KY and ME); another 13 states (38%) were state affiliates of a national organization such as the International Certification and Reciprocity Consortium and the National Association for Alcoholism and Drug Abuse Counselors (eg, MO, NC, SC, and FL), and 6 states (18%) credentialed addiction counselors through state agency licensing boards (eg, WI, NY, and WA). Alaska was the only state that relied on a state-wide professional association to credential addiction counselors.
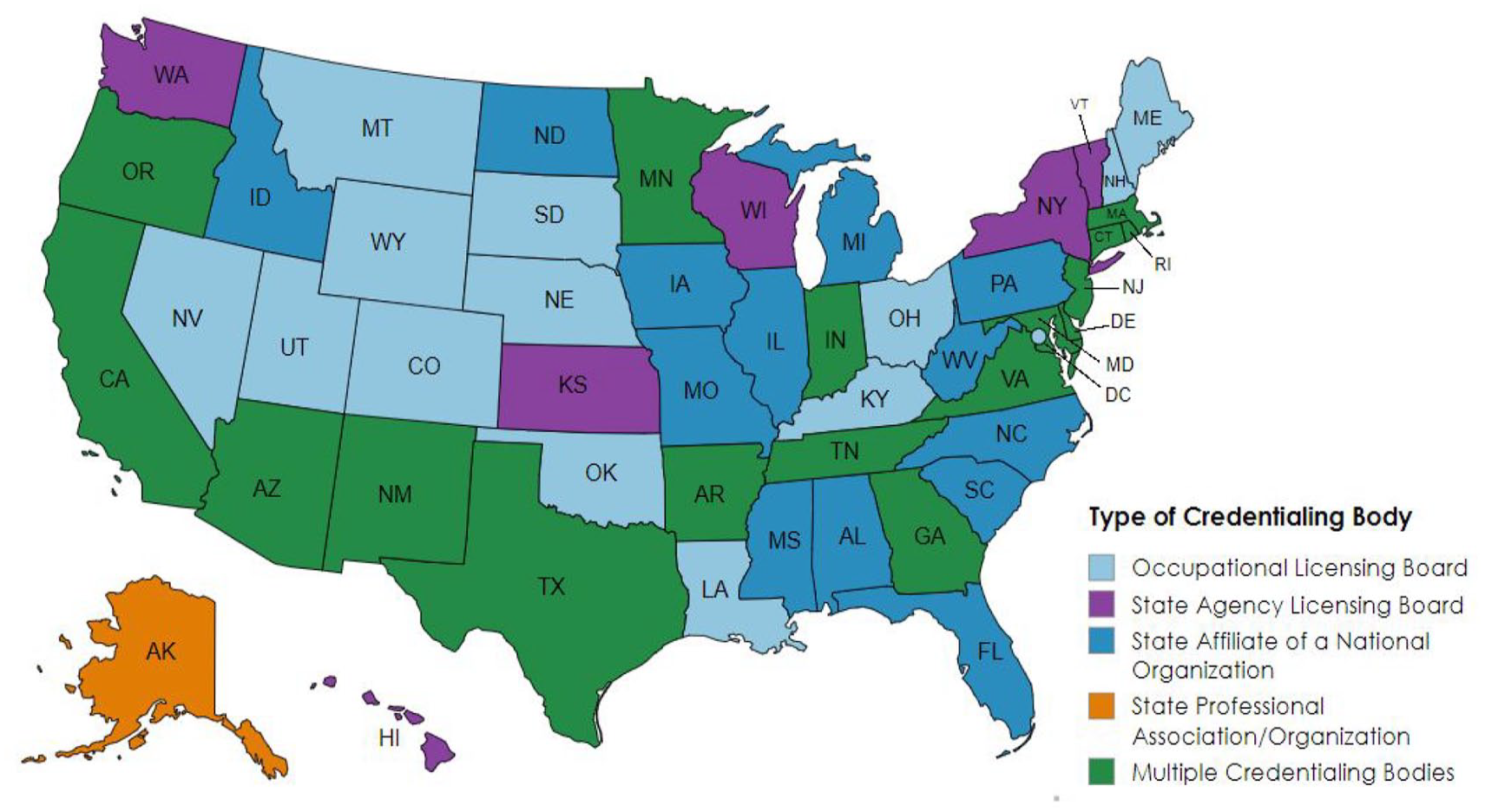
Credentialing bodies for non-graduate-level addiction counselors.
Credentialing Requirements: Exam, Practice Hours, Fees
In 27 states (53%), all credentials, regardless of education, required a certification exam. There were 24 states (47%) where some credentials require a certification exam but not all (eg, RI). The number of practice hours required for HS/BA-level addiction counselors ranged from 0 in DC to 6000 in NC. The average was 3164 hours or roughly the equivalent of 1.6 years of work in the addiction field. In cases where no specific degree was required, addiction counselors had to complete more practice hours on average (3566 hours) than when an HS, AA, or BA degree was specified. On average, HS- and BA-level credentialed addiction counselors were required to complete 3319 practice, respectively, while AA-level credentialed addiction counselors had the lowest average amount of practice hours requirement at 2169 hours.
The cost of application and exam fees for addiction counselor credentialing averaged $278, ranging from $50 in Oregon to $575 in South Carolina. Credentialing costs were similar across all degree levels but were slightly higher for credentials not associated with a specific degree ($311) while credentialing costs for AA-level credentials were the lowest at $265. In addition to the cost of examination and application fees, the average cost of credential renewal was $126, ranging from $0 in Connecticut to $260 in Vermont. Renewals were typically required after 2 years, but the duration of addiction counselors’ credentialing ranged from as little as 6 months (eg, VT’s Certified Apprentice Addiction Professional) to as long as 5 years (eg, SD’s Addiction Counselor Trainee).
Supervision Requirements
At the time of analysis, 38 out of all 50 states and DC (75%) allowed HS/BA-level addiction counselors to receive a supervisor credential. Among these, 16 supervisor credentials were available at the HS level. The average number of practice hours required for a supervisor certification was 6800 hours and the average cost was $192. Twelve states (CO, FL, KS, MI, MO, NC, NV, NY, OH, SC, VT, and WY) and DC did not offer a supervisory credential (see Table 2).
Payment
Medicaid Reimbursement
Assessing whether the HS/BA-level addiction counselor credential is cited in states’ Medicaid billing manual, fee schedules, state plans, or statute/regulations, yielded mixed results. Specifically, 21 states (41%) incorporated all addiction counselor credentials, including those with HS/BA degrees and those with graduate degrees; 19 states cited some, but not all, of their state’s HS/BA-level addiction counselor workforce within their Medicaid reimbursement documents; 11 states (22%) did not include any HS/BA-level addiction counselors in their Medicaid reimbursement policies. Most BA- and AA-level credentials were able to bill Medicaid for their services (78% and 80%, respectively), while less than half of HS- and no-degree-specified credentials could bill Medicaid (38% and 43%, respectively). Of the 10 states that had not adopted Medicaid expansion, 6 allowed some or all addiction counselor credentials to bill Medicaid for their services (TX, KS, GA, SC, WI, FL).
Discussion
This up-to-date, comprehensive assessment identifies education, regulation, and payment factors that are critical components for effectively employing the addiction counselor workforce throughout the United States. Although the complexities of this workforce have been examined in prior research,14-17,27 such efforts included both graduate-level addiction counselors and those practicing with an HS/BA degree, making comparisons difficult. Findings from the current analysis confirm that variations across the addiction counselor workforce persist even within the smaller subset of workforce members practicing without graduate degrees. Training, regulation, and reimbursement implications are described below to assist policymakers, credentialing bodies, professional associations, researchers, and SUD service providers to determine how to build and maintain an adequate workforce to meet increasing addiction and SUD demands.
Implications for Training and Regulation
Overall, differences in the educational and credentialing requirements for addiction counselors highlight issues of equivalency across states and jurisdictions. As evidence-based practices within the addiction field evolve, it becomes increasingly difficult to know where and how new evidence-based models are being implemented across different curricula, training, and practice requirements.17,26,27 This variability also impacts reciprocity between states and the transferability of an HS, AA, and BA-level addiction counselor credential from one state to another.14,28 The variation in training hours and minimum educational requirements may perpetuate a misconception that addiction counselors are a type of behavioral health profession that does not require or have rigorous training standards in contrast to other clinical specialties (with graduate-level degrees) where skill acquisition is tightly linked to nationally accredited academic programs.15,28 More research is needed to determine the training adequacy across addiction counselor programs and ease of reciprocity in transferring an HS, AA, or BA-level addiction counselor credential between different states and regions.
Implications for Payment
The payment variations described in this study underscore some of the challenges HS, AA, and BA-level addiction counselors may face in providing SUD services. Given the limited information that was collected and the aims of this study, it remains unclear if Medicaid reimbursement is impacted by supervisory credentials. Further investigation is also required to determine what incentives—such as financial compensation, professional development, or increased responsibilities, among others—exist to motivate addiction counselors at the HS/BA level to pursue a supervisor credential or other type of credentialing advance. Findings from this state-by-state analysis highlight a misalignment that could exist between Medicaid reimbursement for SUD treatment and the workforce that is able to provide these services. Specifically, 11 states do not mention HS, AA, or BA-level addiction counselors in their Medicaid reimbursement policies, while 6 states that have not adopted Medicaid expansion do mention these types of addiction counselors in their current fee schedules. Ideally, states would examine education and training criteria for their SUD workforce and align these credentialing requirements and payment mechanisms. Although prior research has identified how Medicaid expansion has increased insurance coverage for SUD treatment and access among enrollees, 29 more attention is needed on the workforce who are essential to policy implementation.
Growing the Addiction Counselor Workforce
Understanding the nuances of the addiction counseling workforce is important because it can help clarify credentialing pathways for those who want to enter and advance in the SUD field. It may also help states understand the practitioners who make up their SUD workforce and the levels at which they practice, as well as what changes—such as providing additional levels of training or credentialing—can be made to better enable advancement within the workforce. While most states were found to have various levels or laddering to indicate a path for career progression within their addiction counselor workforces, 24 further studies are needed to determine how addiction counselors are informed about or encouraged to pursue additional SUD training to reach more advanced levels of practice.
As states work to grow their SUD workforces to meet the intensifying demand for services, state-specific policy action will be needed to ensure clear articulation of these career advancement pathways and incentivize addiction counselors to pursue additional training opportunities or supervisory credentials. Potential methods for achieving these actions include allowing addiction counselors additional practice hours as part of a development plan, tracking and encouraging the expansion of practice hours to simplify this process, and waiving fees associated with examination and application costs. It is of particular importance that states without supervisory credentials or pathways for laddering, understand how adopting these measures can help build a robust addiction counselor workforce that is adequately compensated, 34 supported, 30 and clinically effective. 31 Monitoring and tracking the number and type of addiction counselors in the workforce is also key for understanding who is being retained in the field and understanding how potential burnout and attrition can occur within high-stress, poorly compensated behavioral health occupations.30,32-34
Limitations
This analysis should be considered within the context of its limitations. First, due to the lack of a consistent definition of addiction counselors, the data necessary for this analysis was sometimes unavailable or difficult to access, which may have resulted in missing information or the inclusion of outdated materials. In addition, although this paper focused only on Medicaid payment for addiction counselors, additional investigation should be conducted to examine the payment mechanisms and adequacy of reimbursement for addiction counselors across payers (eg, commercial plans and Medicare) is necessary. Further research should also review addiction counselors’ average earnings by state to investigate the relationship between salary and credentialing.
Conclusions
This study’s findings help fill important gaps in the literature on substance use and addiction and inform related policy and practice. A state-by-state analysis of the HS/BA-level addiction counselor workforce is necessary for more accurately understanding workforce shortages relative to increasing demand for services. Effectively harnessing the expertise of the addiction counseling workforce is key to addressing the nation’s growing behavioral health needs. However, considerable variability in how the workforce is defined, trained, regulated, and compensated complicates these efforts. Attention to and investment in the addiction counselor workforce is a vital strategy to address the nation’s behavioral health crisis and clearer pathways will help clarify potential training and policy levers to more effectively employ the workforce providing addiction treatment and services. Articulating the education and training pathways, career progression, and compensation structures for addiction counselors is essential for optimizing this workforce’s provision of addiction and treatment services. With the harmful impacts of SUD and number of lives lost to substance-related toxicity increasing, this attention to and investment in the addiction counselor workforce is a vital strategy for addressing the behavioral health crisis in the United States.
Footnotes
Acknowledgements
The authors would like to thank Scott Luetgenau, MSW, LCAS, and Michael McGuire, MSW, LCAS for sharing their practice knowledge and insights with our research team.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is supported by the Substance Abuse and Mental Health Services Administration (SAMHSA) and the Health Resources and Services Administration (HRSA) of the US Department of Health and Human Services (HHS) under grant number U81HP46529-01-01 Cooperative Agreement for a Regional Center for Health Workforce Studies for $1 121 875. This information or content and conclusions are those of the author and should not be construed as the official position or policy of, nor should any endorsements be inferred by SAMHSA, HRSA, HHS, or the US Government.
Compliance,Ethical Standards,and Ethical Approval
Institutional Review Board approval was not required.