
Abstract
Objectives:
How Right Now (HRN) is an evidence-based, culturally responsive communication campaign developed to facilitate coping and resilience among US groups disproportionately affected by the COVID-19 pandemic. To inform the development of this campaign, we examined patterns in emotional health, stress, and coping strategies among HRN’s audiences, focusing on differences among racial and ethnic groups.
Methods:
We used a national probability panel, AmeriSpeak, to collect survey data from HRN’s priority audience members in English and Spanish at 2 time points (May 2020 and May 2021). We conducted statistical testing to examine differences between time points for each subgroup (Hispanic, non-Hispanic Black, and non-Hispanic White) and differences among subgroups at each time point.
Results:
We found disparities in COVID-19–related mental health challenges and differences in coping strategies. Non-Hispanic Black respondents were more likely than non-Hispanic White respondents to report challenges related to the social determinants of health, such as affording food and housing (26.4% vs 9.4% in May 2020) and experiencing personal financial loss (46.6% vs 29.2% in May 2020). In May 2021, 30.6% of Hispanic respondents reported being unable to meet basic food or housing needs versus 8.2% of non-Hispanic White respondents, and 51.6% reported personal financial loss versus 26.5% of non-Hispanic White respondents.
Conclusions:
Our study further illuminates what is needed to build emotional well-being pathways for people who historically have been economically and socially marginalized. Our findings underscore the need for public health interventions to provide culturally responsive mental health support to populations disproportionately affected by COVID-19 during the pandemic and into the future, with a focus on racial and ethnic disparities.
Keywords
As a result of the COVID-19 pandemic, millions of people in the United States have experienced emotions such as anxiety, fear, and loneliness. 1 By the end of 2020, reports of anxiety and depression symptoms were 6 times higher than rates recorded in 2019. Non-Hispanic Black and Hispanic people were more likely than non-Hispanic White people to experience such mental health disorders.2,3 COVID-19 has negatively impacted mental health in communities of color, in part due to the disproportionate disease and death rates in these communities.4,5 The pandemic has also intensified the need for social and economic resources, which have historically been unavailable to them.3,6,7
The How Right Now (HRN) campaign, which is made possible with support from the CDC Foundation and conducted in partnership with the Centers for Disease Control and Prevention (CDC), aims to help people cope, adapt, and be resilient throughout the COVID-19 pandemic. HRN prioritizes communities that have been disproportionately affected by COVID-19 (adults aged ≥65 years and their caregivers, people living with preexisting mental/physical health conditions, people experiencing economic distress, and people experiencing violence), with a particular emphasis on racial and ethnic minority populations. HRN has been implemented in partnership with national organizations, health- and mental health–focused partners, and community leaders, and it encourages audiences to access the campaign page on the CDC website (cdc.gov/howrightnow), which features resources to support mental health and emotional well-being.
Development of the campaign was guided by a conceptual model of emotional health resiliency and thriving, as informed by multiple psychological and behavioral theories. The Emotional Health Resiliency and Thriving Conceptual Model (Figure) draws from the extended parallel processing model, 8 information processing theory, 9 the transtheoretical model, 10 the theory of planned behavior, 11 and published data. 12
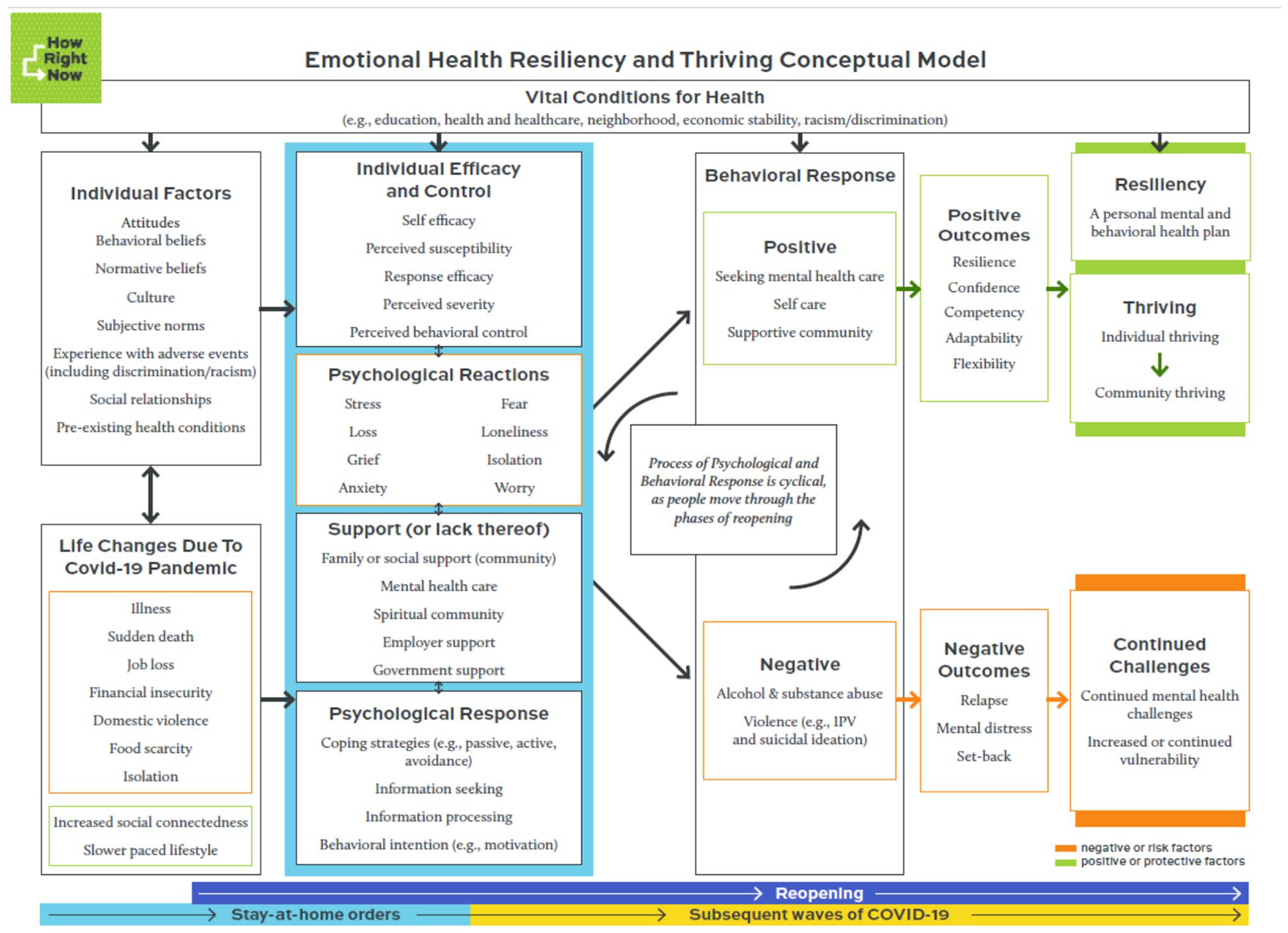
The Emotional Health Resiliency and Thriving Conceptual Model, developed by NORC at the University of Chicago, the Centers for Disease Control and Prevention (CDC), and the CDC Foundation, guided the development of the How Right Now campaign; it draws from numerous health communication theories8 -11 and published data. 12 Abbreviation: IPV, intimate partner violence.
The model builds on CDC’s definition of emotional well-being (“judging life positively and feeling good”) by focusing on resilience and thriving as key to mental health in the context of COVID-19 and its negative impacts (eg, disease, economic shutdowns, social isolation).13 -15 As such, the model delineates how adverse events (including experiences with discrimination and racism), self-efficacy, risk appraisal, stress, coping, and support, among others, shape resilience and thriving in a context where social determinants affect health. These constructs were the focus of exploration in the formative research, which was a crucial step in developing HRN.
In the model, individual factors are primary because they exist in the absence or presence of COVID-19. These factors include behavioral beliefs, culture, and preexisting health conditions (eg, asthma, heart disease, depression, anxiety), but they also influence, and are influenced by, the life-changing factors introduced by the pandemic (eg, illness, job loss). This combination of individual and pandemic-driven factors impacts perceptions of self-efficacy and control, psychological reactions and responses, and social support, and together, these factors lead to positive or negative behavioral responses with positive or negative outcomes. These outcomes ultimately lead to associated recovery or challenges. This process is cyclical because factors and responses ebb and flow over time, and it is time oriented as the United States moves through subsequent phases of the pandemic.
The development of HRN was also based on audience research that used an interrupted time series design to explore the mental health, emotional well-being, and coping needs of people in the United States. Nationally representative survey data were collected in English and Spanish at 2 time points: May 2020 and May 2021. The current study expands on previous work16 -18 by examining how members of 3 racial and ethnic groups—non-Hispanic White (White), non-Hispanic Black or African American (Black), and Hispanic or Latino (Hispanic)—experienced stress and implemented coping strategies during COVID-19.
A substantial proportion of Black (49%) and Hispanic (43%) adults have reported that COVID-19 has damaged their mental health. 19 The disproportionate impact of COVID-19 on morbidity and mortality and economic factors such as job and housing security among racial and ethnic minority populations has been a primary driver of these negative mental health outcomes. 20 For example, Hispanic adults have reported greater concern than any other racial or ethnic group about having enough food or stable housing. 20 These disparities are a direct result of the exclusionary policies that have (1) left communities of color in the United States without access to resources that would help address these needs and (2) increased psychological distress. 21
Before the onset of the pandemic, White people were more likely than their Black or Hispanic counterparts to access various forms of mental health care,22,23 with members of racial and ethnic minority groups seeking informal support (eg, help from family and friends) more often than professional mental health services.
While peer-reviewed literature on US-based behavioral health trends during the pandemic is limited, data from the Household Pulse Survey demonstrated that national estimates of people receiving counseling/therapy increased from 8.7% in August 2020 to 9.8% in April 2021, but White survey respondents generally had higher rates of receiving therapy than Black and Hispanic respondents. 24
Our study research questions were based on data collected as part of HRN’s audience research: (1) What are the differences among White, Black, and Hispanic audiences’ experiences with mental health challenges? (2) What are the differences among White, Black, and Hispanic audiences’ coping with COVID-19–related mental health challenges?
Methods
We designed and fielded 2 national probability panel surveys in English and Spanish. The first was fielded May 15-17, 2020; the second was fielded May 26–June 1, 2021. Most items on the 2 surveys were the same; however, the first survey was designed to inform campaign development, and the second had additional items that reflected pandemic-related events at that time (ie, items related to vaccines) and questions intended to evaluate HRN campaign materials. Both used NORC at the University of Chicago’s AmeriSpeak panel, a nationally representative probability panel of >30 000 US households. 25 The survey was not distributed through the HRN website. Data collection procedures and protocols were reviewed and approved by NORC’s institutional review board and were determined exempt under 45 CFR 46 102(1) by CDC.
The survey included questions to assess experiences and stressors, coping strategies, and resilience. For experiences and stressors, the survey asked, “Which of the following are you experiencing during the COVID-19 pandemic?” and provided a list of experiences that respondents could select. For coping strategies, the survey asked, “Which of the following activities are you doing to cope with the COVID-19 pandemic?” and provided a list of coping activities that respondents could choose. For resilience, the survey used items adapted from the Connor-Davidson Resilience Scale. 26 Sample items include “I will bounce back quickly from these hard times,” “I will come through these difficult times with little trouble,” and “I have the ability to get through.”
Because the goal of the surveys was to assess HRN audiences’ experiences during COVID-19 and the impact of the campaign efforts, respondents who screened into at least 1 of the campaign’s audience groups were invited to participate. Membership in each audience group was based on self-reported identification with one of our priority audiences. Additionally, this sample was constructed by various demographic attributes to ensure the inclusion of diverse perspectives.
The research team cleaned the data (eg, removed duplicates) and weighted them to national census benchmarks, balanced by sex/gender, age, education, race and ethnicity, and region. We adjusted the weights to HRN’s population totals for the final study weights. We calculated statistical weights for the study’s eligible respondents by using panel base sampling weights to start, computed as the inverse probability of selection from the NORC National Frame used to sample housing units for AmeriSpeak and other address-based samples. We raked panel weights to external population totals associated with age, sex/gender, education, race and ethnicity, housing tenure, telephone status, and census division, obtained from the Current Population Survey, and adjusted to the external population totals to develop the final panel weights. We derived study-specific base sampling weights by using a combination of the final panel weight and the probability of selection associated with the sampled panel member. We also adjusted for screener nonresponse, which decreased the nonresponse bias.
At the final stage of weighting, we trimmed extreme weights based on a criterion of minimizing the mean squared error associated with key survey estimates, and we reraked weights to the population totals such that the weighted demographic distribution of the completed surveys resembled the demographic distribution in the populations.
Analysis
We conducted analysis using SAS version 9.4 (SAS Institute Inc) and R version 4.0.2 (R Core Team). We used bivariate analyses to test the null hypothesis of independence for a pair of random variables. We conducted 2 cross-sectional analyses using t tests to detect significant differences between 2 time points 1 year apart at P < .05. We conducted another series of t tests to examine differences among the 3 groups at each time point at P < .05. We tested each group against the other 2 groups to understand where the groups diverged significantly in terms of stressors and coping mechanisms during the pandemic. We also examined 95% CIs for the t tests of differences to verify that no overlap existed, further indicating that observed differences between groups were significant.
A total of 731 respondents completed the May 2020 survey (wave 1), and 712 respondents completed the May 2021 survey (wave 2).
Results
Audience Representation Across Both Survey Waves
About two-thirds of the respondents who identified as White reported having a preexisting mental or physical health condition (67%, wave 1; 68%, wave 2), as compared with approximately half who identified as Black (46%, wave 1; 47%, wave 2) and 38% (wave 1) and 46% (wave 2) who identified as Hispanic (Table 1). Sixteen percent (wave 1) and 22% (wave 2) of White respondents and 39% (wave 1) and 45% (wave 2) of Black respondents reported financial hardship. In contrast, 60% (wave 1) and 43% (wave 2) of Hispanic respondents reported financial hardship. A greater proportion of respondents who identified as White reported that they were aged ≥65 years (43%, wave 1; 39%, wave 2) when compared with those who identified as Black (16%, wave 1; 25%, wave 2) and Hispanic (12%, wave 1; 4%, wave 2). One-quarter of respondents to the wave 2 survey who identified as Black, as well as 14% of Hispanic respondents and 13% of White respondents, reported experiencing or being at risk of experiencing violence (vs 12%, 18%, and 11%, respectively, in wave 1).
How Right Now campaign priority audience membership and demographic characteristics of AmeriSpeak panel survey respondents, United States, May 2020 and May 2021 a
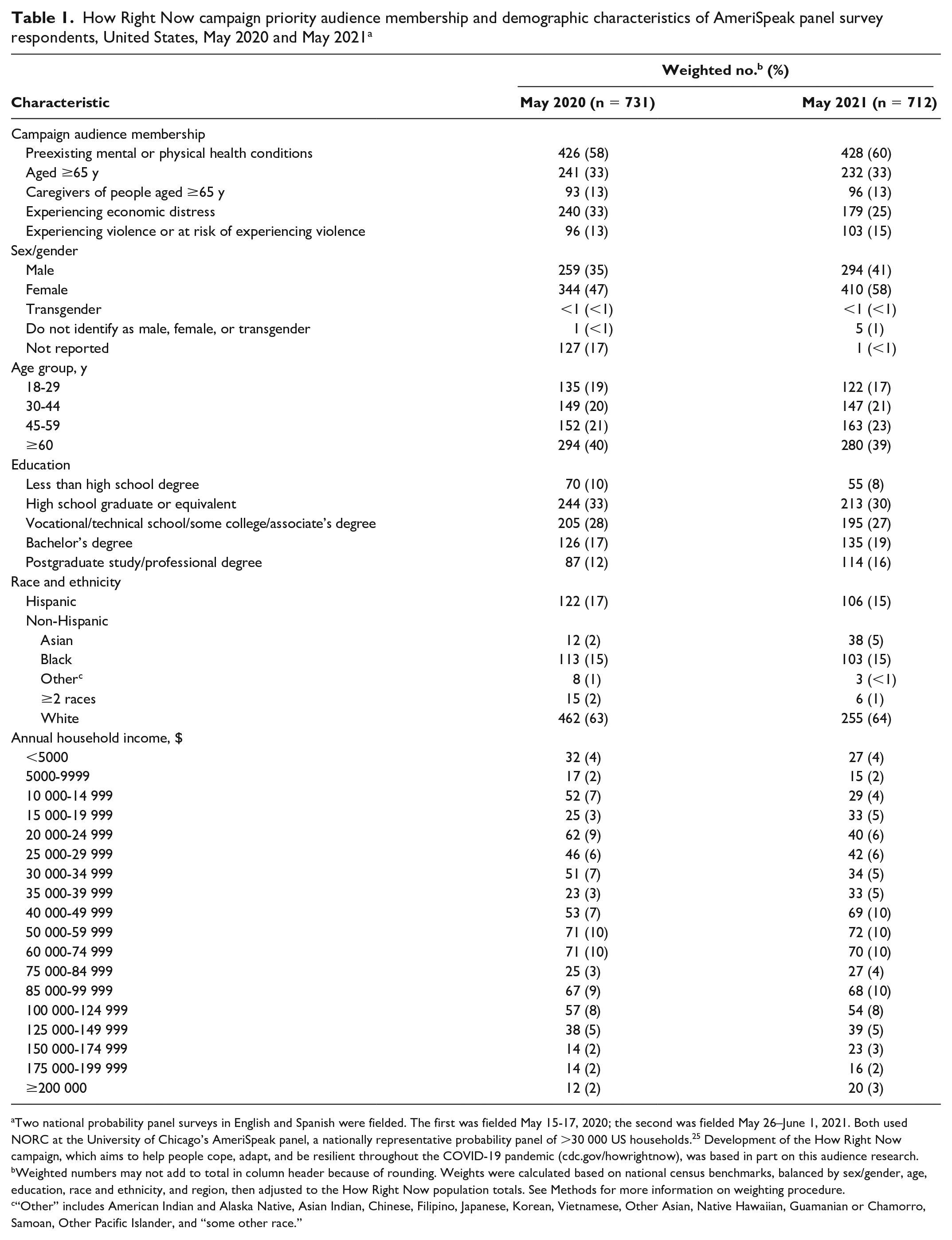
Two national probability panel surveys in English and Spanish were fielded. The first was fielded May 15-17, 2020; the second was fielded May 26–June 1, 2021. Both used NORC at the University of Chicago’s AmeriSpeak panel, a nationally representative probability panel of >30 000 US households. 25 Development of the How Right Now campaign, which aims to help people cope, adapt, and be resilient throughout the COVID-19 pandemic (cdc.gov/howrightnow), was based in part on this audience research.
Weighted numbers may not add to total in column header because of rounding. Weights were calculated based on national census benchmarks, balanced by sex/gender, age, education, race and ethnicity, and region, then adjusted to the How Right Now population totals. See Methods for more information on weighting procedure.
“Other” includes American Indian and Alaska Native, Asian Indian, Chinese, Filipino, Japanese, Korean, Vietnamese, Other Asian, Native Hawaiian, Guamanian or Chamorro, Samoan, Other Pacific Islander, and “some other race.”
Differences Among White, Black, and Hispanic Audiences’ Experiences With Mental Health Challenges
In May 2020, Black respondents reported experiencing stress related to the pandemic (61.6%), stress and discord in the family (44.2%), and changes in daily life patterns (59.7%) (Table 2). Fifty-six percent reported changes in sleep patterns (vs 28.6% of White respondents), and 43.2% reported changes in eating habits and/or challenges in maintaining healthy eating habits (vs 27.8% of White respondents). Black respondents reported several economic and family challenges during COVID-19: 46.6% reported personal financial loss (vs 29.2% of White respondents), and 26.4% reported challenges being able to meet basic food or housing needs (vs 9.4% of White respondents).
Proportion of respondents in an AmeriSpeak panel survey who reported experiencing each of the following items and using each of the following coping strategies during the COVID-19 pandemic, by racial and ethnic group, United States, May 2020 and May 2021 a
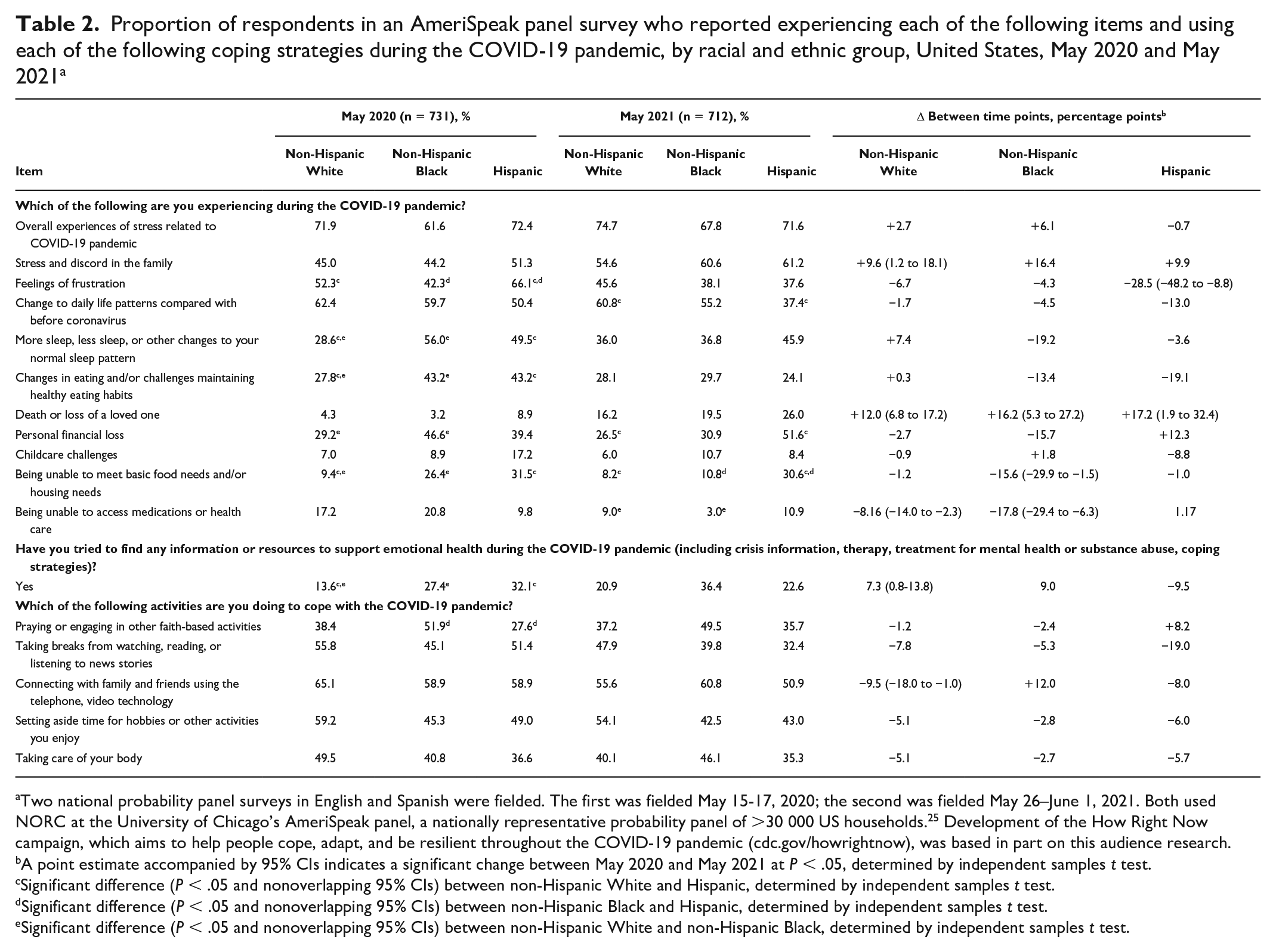
Two national probability panel surveys in English and Spanish were fielded. The first was fielded May 15-17, 2020; the second was fielded May 26–June 1, 2021. Both used NORC at the University of Chicago’s AmeriSpeak panel, a nationally representative probability panel of >30 000 US households. 25 Development of the How Right Now campaign, which aims to help people cope, adapt, and be resilient throughout the COVID-19 pandemic (cdc.gov/howrightnow), was based in part on this audience research.
A point estimate accompanied by 95% CIs indicates a significant change between May 2020 and May 2021 at P < .05, determined by independent samples t test.
Significant difference (P < .05 and nonoverlapping 95% CIs) between non-Hispanic White and Hispanic, determined by independent samples t test.
Significant difference (P < .05 and nonoverlapping 95% CIs) between non-Hispanic Black and Hispanic, determined by independent samples t test.
Significant difference (P < .05 and nonoverlapping 95% CIs) between non-Hispanic White and non-Hispanic Black, determined by independent samples t test.
A smaller percentage of Black respondents in May 2021 than in May 2020 reported challenges in being able to meet basic food or housing needs (from 26.4% to 10.8%, a decrease of 15.6 percentage points) and accessing medications or health care (from 20.8% to 3.0%, a decrease of 17.8 percentage points). In May 2021, 67.8% of Black respondents said that they had experienced stress related to the pandemic, and 60.6% reported discord in the family. Although a smaller percentage of Black respondents (3.0%) than White respondents (9.0%) reported being unable to access medications or health care, a larger percentage of Black respondents than White respondents had lost a loved one (19.5% vs 16.2%).
In May 2020, 71.6% of Hispanic respondents reported experiencing stress related to the pandemic, and 51.3% reported stress and discord in the family. Feelings of frustration were also common among Hispanic respondents, with 66.1% reporting these feelings as compared with 52.3% of White and 42.3% of Black respondents. Hispanic respondents noted substantial changes in daily life patterns, such as changes in sleep patterns (49.5% vs 28.6% of White respondents) and eating habits (43.2% vs 27.8% of White respondents). Many Hispanic respondents reported economic challenges: 39.4% reported personal financial loss, 31.5% reported challenges being able to meet basic food or housing needs (vs 9.4% of White respondents), and 17.2% reported challenges with child care.
One year later, feelings of frustration among Hispanic respondents decreased from 66.1% to 37.6%. However, many challenges remained, including 30.6% of Hispanic respondents being unable to meet basic food or housing needs (vs 8.2% of White respondents). Personal financial loss also remained common, with 51.6% of Hispanic respondents (vs 26.5% of White respondents) reporting personal financial loss. Approximately 1 in 4 (26.0%) Hispanic respondents had lost a loved one, a 17.1 percentage-point increase from May 2020. Overall experiences of stress (71.6%) and discord in the family (61.2%) remained common among Hispanic respondents, as did disrupted sleep patterns (45.9%).
Differences Among White, Black, and Hispanic Audiences’ Coping With COVID-19–Related Mental Health Challenges
In May 2020, respondents reported using various coping strategies to manage the stress, social isolation, and life challenges and worries introduced during the COVID-19 pandemic. Many Black respondents reported that they had connected with friends and family using remote technologies (58.9%), prayed (51.9%), took breaks from the news (45.1%), engaged in hobbies (45.3%), and took care of their body (40.8%) to cope with the pandemic. They were more likely to engage in prayer and other faith-based activities than White respondents (38.4%). More than one-quarter (27.4%) of Black respondents reported that they tried to find information or resources to support their emotional health during the pandemic (eg, crisis information, therapy, treatment for mental health or substance abuse, coping strategies), which was significantly greater than the 13.6% of White respondents who reported trying to do so.
One year later, we detected no significant changes in the coping strategies used by Black respondents. Because of a 7.3 percentage-point increase in information seeking among White respondents, the difference between Black and White respondents was no longer significant.
Hispanic respondents also reported using various coping strategies. In May 2020, many Hispanic respondents reported that they had connected with friends and family using remote technologies (58.9%), took breaks from the news (51.4%), engaged in hobbies (49.0%), and took care of their body (36.6%) to cope with the pandemic. Approximately one-third (32.1%) had looked for information or resources to support their emotional health, which was greater than among White respondents (13.6%). One year later, we found no significant changes in coping strategies used by Hispanic respondents (Tables 2 and 3).
Proportion of respondents in an AmeriSpeak panel survey who reported that they agree that they have been able to cope with the COVID-19 pandemic by engaging in each of the following, by racial and ethnic group, United States, May 2020 and May 2021 a
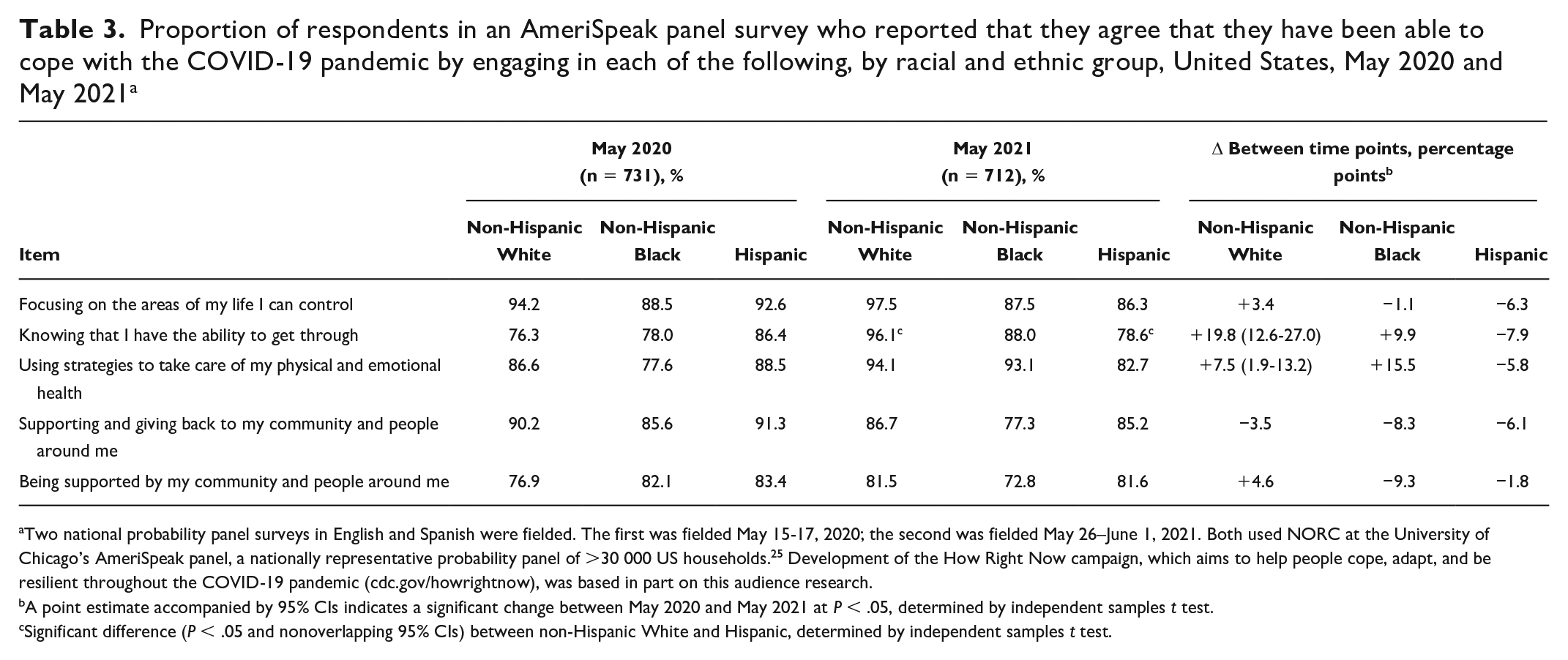
Two national probability panel surveys in English and Spanish were fielded. The first was fielded May 15-17, 2020; the second was fielded May 26–June 1, 2021. Both used NORC at the University of Chicago’s AmeriSpeak panel, a nationally representative probability panel of >30 000 US households. 25 Development of the How Right Now campaign, which aims to help people cope, adapt, and be resilient throughout the COVID-19 pandemic (cdc.gov/howrightnow), was based in part on this audience research.
A point estimate accompanied by 95% CIs indicates a significant change between May 2020 and May 2021 at P < .05, determined by independent samples t test.
Significant difference (P < .05 and nonoverlapping 95% CIs) between non-Hispanic White and Hispanic, determined by independent samples t test.
Many participants reported a belief in their ability to cope and remain resilient during difficult times. In May 2020, 88.5% of Black respondents agreed that they had been able to cope by “focusing on the areas of my life that I can control” (Table 3). Three-quarters (77.6%) of Black respondents said that they used strategies to take care of their physical and emotional health. Reliance on the community was also common: the majority of Black respondents said that they had coped by “supporting and giving back to my community and people around me” (85.6%) and by “being supported by my community and people around me” (82.1%). One year later, we found no significant shifts in these patterns.
In May 2020, 92.6% of Hispanic respondents agreed that they had been able to cope by “focusing on the areas of my life that I can control.” Most Hispanic respondents (88.5%) also said that they used strategies to take care of their physical and emotional health. Reliance on the community was also common: the majority said that they had coped by “supporting and giving to my community and people around me” (91.3%) and by “being supported by my community and people around me” (83.4%). We detected no significant shifts in these patterns 1 year later.
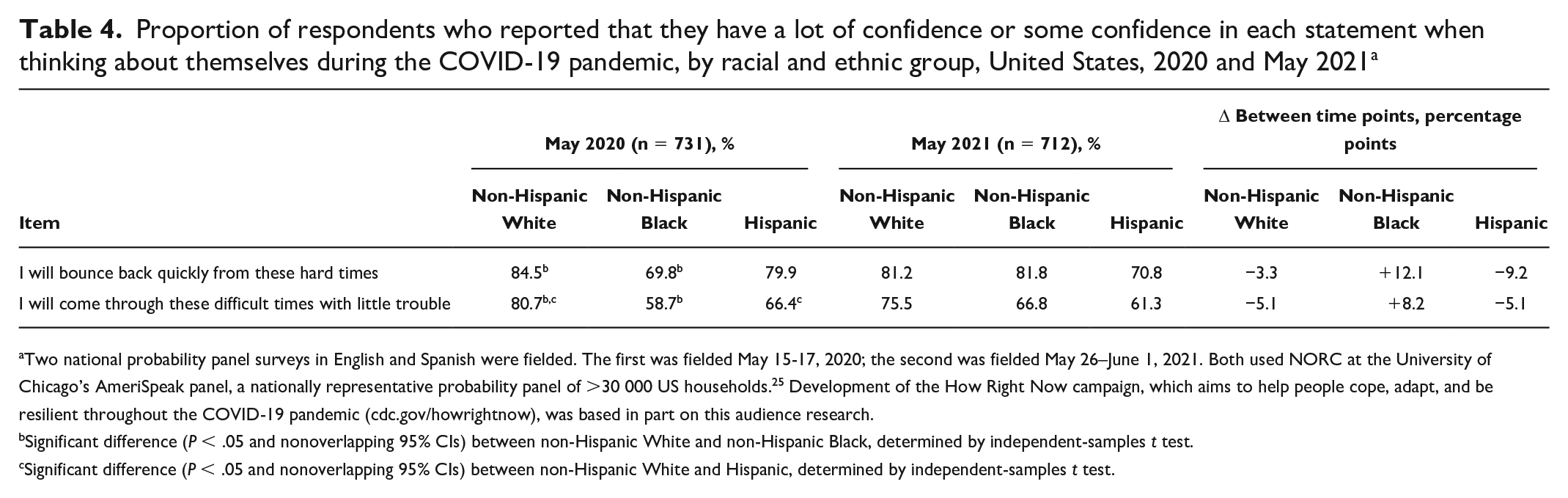
Disparities among racial and ethnic groups became more pronounced when the measures of perceived resilience were examined (Table 4). In May 2020, White respondents (80.7%) were much more likely to report that they “will come through these difficult times with little trouble” than Black (58.7%) and Hispanic (66.4%) respondents. A greater percentage of White respondents (84.5%) than Black respondents (69.8%) reported an ability to “bounce back.” We detected no differences between the groups 1 year later. We found an increase in White respondents from 2020 (76.3%) to 2021 (96.1%) who said that they were able to cope by knowing that they “have the ability to get through” (Table 3). However, we found no such changes among Black respondents, and agreement with this statement among Hispanic respondents decreased significantly from 86.4% in May 2020 to 78.6% in May 2021. In contrast, the percentage of White respondents agreeing with this statement in 2021 was significantly different from the percentage of Hispanic respondents.
Proportion of respondents who reported that they have a lot of confidence or some confidence in each statement when thinking about themselves during the COVID-19 pandemic, by racial and ethnic group, United States, 2020 and May 2021 a
Two national probability panel surveys in English and Spanish were fielded. The first was fielded May 15-17, 2020; the second was fielded May 26–June 1, 2021. Both used NORC at the University of Chicago’s AmeriSpeak panel, a nationally representative probability panel of >30 000 US households. 25 Development of the How Right Now campaign, which aims to help people cope, adapt, and be resilient throughout the COVID-19 pandemic (cdc.gov/howrightnow), was based in part on this audience research.
Significant difference (P < .05 and nonoverlapping 95% CIs) between non-Hispanic White and non-Hispanic Black, determined by independent-samples t test.
Significant difference (P < .05 and nonoverlapping 95% CIs) between non-Hispanic White and Hispanic, determined by independent-samples t test.
Discussion
Our study contributes to broadening our understanding of how the COVID-19 pandemic has shaped behavioral health outcomes and exacerbated the need for supportive services, especially among communities of color. Key findings demonstrate how race and ethnicity correlate with negative socioeconomic impacts 20 and care-seeking behaviors, 24 both of which affect overall well-being. Our findings provide a nuanced view of how substantially mental health experiences and coping strategies differed among White, Black, and Hispanic audience groups during the COVID-19 pandemic, with Black and Hispanic people experiencing substantially greater negative impacts and feeling less confident than White people in their ability to be resilient throughout the pandemic.
Our study also provides insights into what exactly has differed and how needs and coping strategies have shifted during the pandemic. Black and Hispanic people have experienced economic challenges and increased stress and discord in the family. Yet, reliance on family, friends, and community for support was common among Black and Hispanic survey respondents, as was their attempt to lessen negative mental health impacts by taking breaks from the news, engaging in hobbies, and taking care of their physical health. They also reported seeking information to support their mental health and emotional well-being.
Finally, HRN’s Emotional Health Resiliency and Thriving Conceptual Model provides a framework for other mental health researchers and practitioners to be able to examine the factors that can result in positive and negative mental health outcomes.
Translational Insights
These findings highlight how the pandemic has disproportionately affected the mental health, coping, and resilience of people of color, adding to previous work that has elucidated this connection between demographic characteristics and mental health. The findings that Black and Hispanic people have been disproportionately affected by the COVID-19 pandemic and sought emotional health–related information and resources at higher rates than White people during this time underscore the need for resources and services that are tailored to the experiences of populations with limited support mechanisms (eg, those with limited or no access to health care, those without legal status).
A communication campaign such as HRN offers a possible approach to addressing some of these challenges. The campaign’s resources exemplify this approach (eg, webpages tailored to address feelings such as loneliness and grief, conversation guides, linkages to mental health service organizations serving Black or Hispanic communities and additional information).
Limitations
Our study had several limitations. First, the research focused on HRN’s audiences, so although the research has general applicability to the US population, the study’s findings reflect the experiences and perceptions of HRN’s audiences. Second, the use of self-reported data may have resulted in selection bias. Third, within-group variances may have occurred because of the study’s cross-sectional design.
Fourth, the Black and Hispanic samples were small, as was the sample of respondents completing the Spanish-language survey (2%), which limited the study team’s ability to analyze the Spanish-language responses. Fifth, we did not assess disparities according to geographic and immigration status; these disparities warrant further research. Finally, the social justice movements during summer 2020 may have contributed to the emotional health of the communities of focus in our study; the effect of the social justice movement on emotional health should be considered in future work. 27
Conclusion
Aligning with previous research,5,27 our study findings suggest how vulnerability to adverse mental health outcomes among racial and ethnic minority groups, caused by the social and structural barriers that they face, has been amplified during the COVID-19 pandemic, creating challenges in coping and resilience. Continued monitoring of mental health and coping strategies among racial and ethnic minority groups is essential to the development of culturally sensitive resources that acknowledge the strength that these communities are already demonstrating and help them better cope with the challenges that they face in emergency situations such as the COVID-19 pandemic.
Footnotes
Acknowledgements
The authors acknowledge Ashani Johnson-Turbes, PhD, of NORC at the University of Chicago for her expertise and assistance in developing the conceptual model featured in this article. The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received the following financial support for the research, authorship, and/or publication of this article: This work was supported by a subcontract from the CDC Foundation (project 1085).