
Abstract
Background:
Youth represent 21% of the Egyptian population; such proportion can create a leading demographic power for economic development and transition. However, with the current COVID-19 pandemic, everyone is exposed to more than usual stressors, adding a burden to their mental health and well-being.
Aim:
This study aims to understand the pandemic’s effect on youth’s mental health in Egypt to strengthen the intervention areas needed to tackle such issues.
Methods:
This observational, analytical, cross-sectional study employed internet platforms of Facebook & WhatsApp groups for a web-based survey that included 412 respondents between 15 and 30 years old. RESULTS The median age of the respondents was 22 years. At least 30% reported increased violence in the street and/or household, and 27.4% of the respondents have considered visiting a psychiatrist during the last period.
Conclusion:
It is evident that the current situation is unprecedented and challenging for everyone; however, some populations are more vulnerable than others. Thus, it’s important to support young people to ensure that the whole community can withstand the pandemic. The governments should support and mitigate some of the stresses that can be directly amended, like the education and job security concerns.
Introduction
In December 2019, Wuhan city in China disclosed cases of severe pneumonia that was later identified as viral infections caused by a novel Coronavirus. Reported cases significantly increased in the city and expanded to other Chinese cities, and by the start of 2020, similar cases have been reported outside of China. On 11 March 2020, the World Health Organization (WHO) announced this disease as a pandemic. 1 Consequently, on the 14th of February 2020, Egypt reported its first Coronavirus COVID-19 case. Since then, the Egyptian Government scaled-up preventive measures, with a partial lockdown starting on the 25th of March 2020 and currently ongoing. 2 By the 15th of November, Egypt had more than 110,547 cases and 6442 deaths and is still rising in a flattening manner. 3 According to Oxford COVID-19 Government Response Tracker (OxCGRT), the highest stringency index was between the 25th of March 2020 and the 6th of June 2020. The stringency index reflects the strictness of the implemented measures, through the collection of publicly available information on 17 indicators of government responses. 4
All these measures are causing unpredicted mental health consequences affecting vulnerable populations. People’s emotional responses vary, including but not limited to fear, anxiety, stress, and uncertainty. Additionally, It may worsen to include a broad range of mental health issues, including distress reactions (insomnia, anger, fear of illness regardless of the exposure), health risk behaviors (increased use of alcohol and tobacco, social isolation), mental health disorders (post-traumatic stress disorder, anxiety disorders, depression), and lowered conscious health. 1 Many people are affected by the direct health impacts of the virus and the consequences of protective measures. Individuals have been substantially distanced from family and friends, living in fear of infection, dying, and/or losing family members. Millions are facing an economic burden with the increased loss or being at risk of losing their jobs. Frequent rumors and false information about the virus and the uncertain future are common causes of stress. All these increase the possibility of a long-term upsurge in the number and severity of mental health problems. 20
Nowadays, in Egypt, young people represent 21% of the total Egyptian population. 5 Young people are one of the most vulnerable groups for mental health consequences following the COVID-19 crisis. Young people are affected by closures of formal and non-formal education opportunities. More than 1.5 billion young people, constituting 91% of the world’s student population, are kept away from schools and universities in more than 190 countries, including Egypt. 6 As a result, they are deprived of social engagement with their peers and educators. Prolonged periods of closures and movement restrictions may lead to further emotional unrest and anxieties increasing their vulnerability for mental health issues.
Methodology
Study design
This study is an observational, analytical, cross-sectional study that employed internet platforms of Facebook & WhatsApp groups for the implementation of the survey.
Study period
This study was conducted over a period of 3 months from May 2020 till August 2020.
Study setting and population
A web-based survey addressing youth response during COVID-19 was broadcasted on the Internet through WhatsApp and Facebook platforms, where users could access the questionnaire by clicking the relevant link. This web-based electronic form was completely voluntary and anonymous.
Sample size and technique
A non-random convenience sample was used for this study. The sample size was calculated using Epi Info software. Based on evidence from the few previous studies and by considering the percentage of youth subjected to mental stress due to COVID-19 as a primary outcome, assuming 80% power, 0.05 level of significance, 30% of null hypothesis value, and the estimated proportion of 30%, the sample size was calculated to be 266 participants. Considering the drop-outs rate, of 41.8%, as in the study by Galesic in 2006, therefore the final sample size was calculated to be 377 participants. The total number of respondents was 412 respondents.
Study tool and data collection technique
An E-form questionnaire (using Microsoft forms) through a link shared on social networks was used. It included the following: socio-demographic background, occupational data, questions to assess their knowledge and attitudes regarding COVID-19, and questions to assess their exposure to mental issues during the era of COVID-19. This questionnaire was adopted and modified from the WHO tool for behavioral insights on COVID-19 (WHO, 2020b) and from two other studies, one by the Scottish youth parliament that involved 2421 responses by young people on their opinion on COVID-19 (The Scottish youth parliament 7 ), and the other by UK health, also addressing the effect of COVID-19 on young people. 8
A pilot testing phase was done to adapt the questionnaire to fit and suit the Egyptian context and verify that items and questions are comprehensible and clear.
Data management
Data were coded and entered on Microsoft forms and transferred to Excel, then exported to SPSS version 21. The data were summarized using descriptive statistics; simple frequencies (numbers and percentages) for qualitative variables, mean & standard deviation for normally distributed quantitative variables, median & quartiles for quantitative skewed variables. Comparisons between groups were analyzed using the appropriate statistical tests of significance. p-value of ≤0.05 was considered significant.
Ethical consideration
Informed consent was obtained from each participant (before participation in the online survey) after proper orientation regarding the objectives of the study and the confidentiality of the collected data. Strict confidentiality about participants’ personal data is maintained throughout data collection, entry, and analysis (according to the Helsinki declaration). The information collected was anonymized.
Informed consent statement
“Your participation in this online survey is completely voluntary. All of the information that you provide for the study will be kept completely confidential. We record your responses, but the questionnaire will not have your name on it, and your responses to our questions are identified only by a number, never by name. We hope that this survey will be considered a baseline assessment that will help assess the mental stress that youth experience in this unprecedented time, which is considered an important step in combating the infection. The survey will take about 10−15 min.”
Results
A total of 412 participants participated in this study, of which (98.5%) agreed to fill the questionnaire. The respondents were between 15 and 30 years of age, with a median age of 22 years. More than half of the respondents were females (58.6%) and the majority of all respondents (94.6%) received University or Postgraduate education. Out of 386 valid responses, (63.7%) (246) were of medical background. The majority of the respondents were single (91.1%). Most of the respondents (82.3%) were from rural settings.
Furthermore, more than half of the respondents were students (57.6%). From a total of 116 respondents who work, 51.7% work in the medical field, while 48.3% had non-medical jobs. Regarding their economic situation, 47.5% responded that their Expenses equal their income, 28.6% responded that Expenses exceed income, and 23.9% Expenses are less than income.
The exact demographic breakdown can be found in the Appendix 1.
The respondents were asked some general questions to assess their state of affairs, specifically with regards to having positive COVID-19 cases in their surrounding friends and relatives and if they believe they have received enough information about the virus. According to the survey, 38.4% of our respondents had at least one case of covid-19 in their immediate social environment. The majority of respondents (92%) were free from any chronic illness. Most of the respondents (70%) had enough access to information about COVID-19.
Moreover, respondents were also asked about the pressures they have experienced and their feelings toward common concerns such as; their financial situation, employment situation, and their ability to take care of their beloved ones. Almost half of them (52%) perceived COVID-19 as a dangerous infection. However, 80% of the respondents did not believe that COVID-19 is associated with stigma. Additionally, more than half of them (59.4%) believed they would get the virus, and the reason was distributed almost equally (29%) and (27%) between being a high-risk population and living in a crowded area respectively. (71.9%) were concerned about their coursework, although only a few percent (36%) were concerned about the closure of schools/colleges. Striking findings were noted in the concern of the respondents to their employment, financial situation, physical wellbeing, mental wellbeing, physical wellbeing of others, and mental wellbeing of other were percentages of the concerned were (63.3%), (67.3%), (68%), (52.7%), (83.5%), and (71.7%) respectively. Furthermore, the majority of the respondents were concerned about the impact of COVID-19 on their social relationships (62.1%) and their ability to look out for others (68%). (83.5%) were concerned about the impact of the coronavirus on their future, and (77.6%) felt concerned about the actions taken by decision-makers to mitigate the transmission of the virus. The full list of questions and analyzed answers can be found in Appendix 2.
In addition, the participants were asked about some of the causes of distress that affects their daily life and if they are concerned about the effect of the preventive measures on these situations. Most of the respondents reported decreased physical activity (81.2%). Although overall sleep was increased (58.6%), a high portion of the respondents reported increased intermittent sleep (58.9%) and decreased deep sleep (41.2%). Additionally, findings showed an increase in household violence (32.2%) as well as violence in the streets (31.8%). Food quantities increased (56.9%) whereas an equal percentage was reported in increased (34.5%) and decreased (35.7%) healthy dietary habits by the respondents. More than three-quarters of the respondents reported a decrease in overall mood (75.1%) and a decrease in mental health (73.4%). The exact breakdown is shown in annex 3.
Furthermore, to measure if young people were able to withstand all these stressors, we asked them if they considered consulting a psychiatrist and if so, what was the preferred mode of consultation during the implemented measures. The majority of the respondents did not think about consulting a psychiatrist (72.4). Out of those who thought about it, (82.1%) visited the psychiatrist’s office, and only (17.9%) made their appointment virtual. Further information can be found in Table 1.
How young people were able to withstand stressors during the pandemic.

Given the effect of the virus on the respiratory system, it was necessary to include a question about smoking patterns and whether it was helpful or not. 92.1% of our respondents were non-smokers, so the below division is based on the 32 respondents. 29.4% of the smoking respondents considered stress a main factor in the change in cigarette consumption. Whereas 27.8% of the shisha smokers considered the closure of the coffeeshops the main reason for the change in shisha smoking. 6.9% considered quitting, and the main reasons were caring about their own health (38.9%), and closure of coffeeshops (27.8%). The full breakdown of questions and frequencies can be found in Appendix 4.
The respondents were also asked if they believe they have enough access to information around COVID19, 70.2% responded with Yes. The percentage of males who believed having enough access to info about COVID-19 was significantly higher than that of females (75.65% in males and 66.4% in females, with a p-value of 0.046). When analyzing the economic status, there was a significant difference between the three categories with a p-value of 0.046. The exact comprehensive breakdown, according to different demographics, can be found in Table 2.
Youth belief if they have enough access to information around COVID19.

Living in an urban or rural area showed no statistical difference (p-value = 0.497) when comparing if anyone in the respondents’ immediate social environment got infected with COVID-19. However, a statistical difference (p-value = 0.014) was reported between Medical and Non-medical occupations where respondents who work in a medical setting reported 60% confirmed COVID-19 cases within their immediate social environment compared to only 33.9% confirmed cases within the immediate social environment of respondents who work in a non-medical setting. The stratification on the place of residence and job results can be found in Table 3
Sociodemographic characteristics relation with COVID-19 infection of immediate social environment.

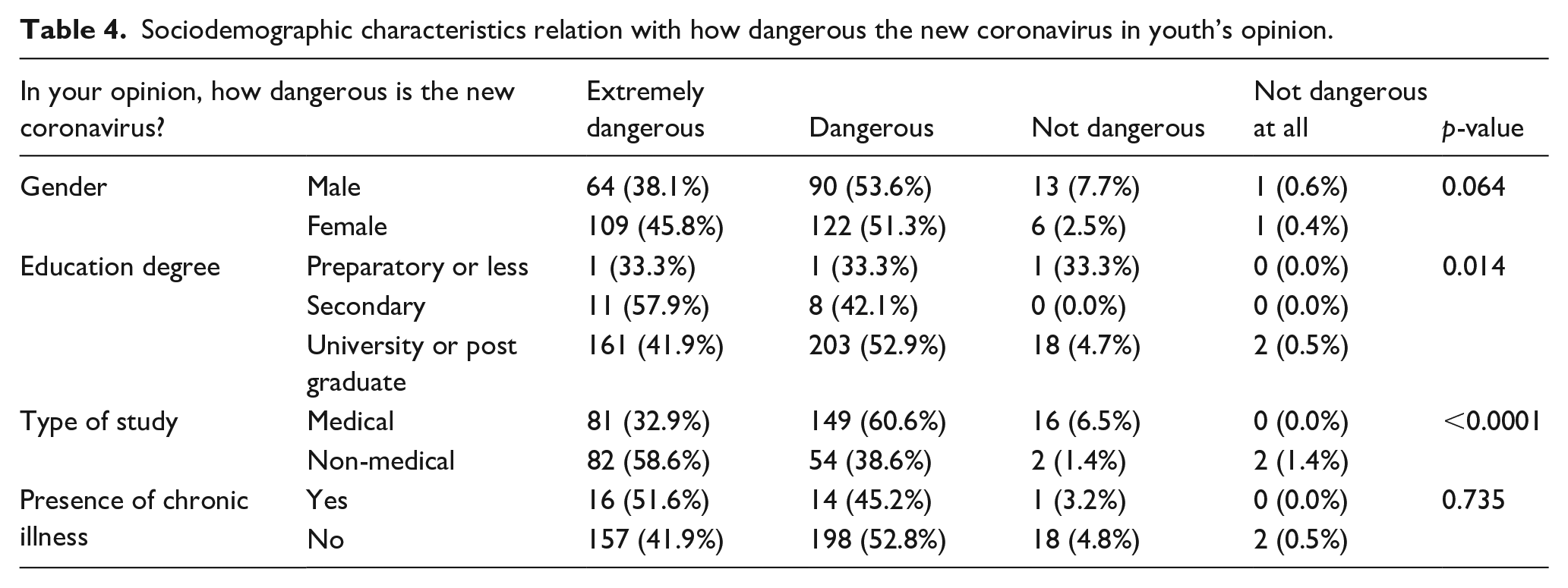
We stratified the findings of how dangerous the new coronavirus is according to gender, education degree, type of study and person with chronic illness. There was not a statistical difference in any strata except in the type of study (p-value = < 0.0001) where most medical students reported that the new coronavirus is dangerous (60.6%) compared to non-medical students (38.6%). Being male or female has not yielded a difference in the findings where both reported that the new coronavirus is dangerous with a 53.6% and 51.3% respectively (p-value = 0.064). In addition to that, respondents who were at their preparatory, secondary and university/postgraduate degrees reported that the new coronavirus is dangerous nearly equally (33.3%, 42.1%, and 52.9% respectively) showing no statistical difference (p-value = 0.014). No significant difference was found between having a chronic illness or not (p-value = 0.735). The full analysis can be found in Table 4.
Sociodemographic characteristics relation with how dangerous the new coronavirus in youth’s opinion.
There was not any statistical difference between groups of strata on their thoughts of the new coronavirus association with stigma. Both males and females reported that they think it is not associated with stigma (77.4% and 81.9% respectively) with a p-value of 0.258. Additionally, more than half of the respondents who are at their preparatory education thought it is not a stigma toward people infected by it (66.6%). Nearly equal proportions of respondents who are at their secondary (68.4%) and university/postgraduate degrees (80.7%) reported the same (p-value = 0.226). Equal distribution was also noted among respondents who live in Urban and Rural areas where most of them did not think the new coronavirus is a stigma (81.9% and 80% respectively) showing no significant difference between the strata (p-value = 0.657). The exact details can be found in Appendix 5.
Discussion
70.2% of all respondents stated that they have enough access to information around COVID19, with similar percentages in both rural and urban settings of 69.8% and 72.2% respectively, reflecting the equitable access to information in both settings. This is also the result of the rigorous awareness campaigns and the efforts tackling infodemics and fake news conducted by the Government of Egypt, in collaboration with UN entities and civil societies and the private sector.9–13
When it comes to the fear of the virus, 42.6% of the respondents considered the virus to be very dangerous, and 52.2% considered it more or less dangerous. This high level can lead to increased public fear which in turn can result in the increase of stigma and discrimination. 14
At the time of the survey, based on the responses 30.7% thought that the virus was a cause of stigma toward people infected. Despite the relatively low percentage, this can be alarming especially with the risk of a larger, more vigorous second wave. 15
The measures implemented to control the pandemic included isolation of positive and suspected cases, the lockdown of the country and closure of airports. 16 Quoting from the World Health Organization’s (WHO’s) Director of Global Infectious Hazard Preparedness Sylvie Briand said, “Fear and stigma go together, and when people fear, they tend to stigmatize some groups and what we try to do is to reduce this fear” 17
On asking whether they think they are at risk of getting infected with Coronavirus, 59.4% responded with Yes, 10.1% responded with No, and 30.5% did not know. From a total of 241 who responded with Yes on the previous question, in response to why they think they are likely to get infected, 29% chose I am a high-risk population, 27% chose to Live in a crowded area, 23.2% chose many relatives or neighbors got infected, 19.5% chose to Live in an ill infrastructure area, 0.8% chose I already got infected and 0.4% chose other.
Such percentages provide us with a window of opportunity to ensure that all environmental factors can be targeted. This takes us back to the importance of ensuring that fear does not increase and becoming a bigger issue that the pathogen itself.
The WHO Director-General said; “The mental health needs of young people need to be cared for and responded to by mainstream mental health services. There is no health without mental health.” 18
The 63.9% of all respondents are either concerned or very concerned about their employment situation. According to CAPMAS, in the second quarter of 2020, the unemployment rate rose to 9.6%. 19 Financial and economic challenges in emergencies are just some of the possible challenges imposed by crises. 20
The current stress and worry that young people are facing are very overwhelming. They have to deal with all the challenges during this unprecedented time. At the same time, many people have lost or are at risk of losing their jobs, have been socially isolated and separated from their loved ones, and experienced different levels of lockdown. Widespread misinformation, also known as infodemics, about the virus, protective measures and deep uncertainty about the future impose an additional source of distress. 20
Our participants have expressed an unfortunate and supporting statistics, where 67.3% of all respondents are either concerned or very concerned about their financial situation. 68% felt concerned or very concerned about their physical wellbeing while 83.5% regarding the physical wellbeing of others. Moreover, 52.7% were concerned or very concerned regarding their mental health and 57.7 regarding the mental health of others.
73.4% of all respondents have stated the worsening of their mental health status and 75.1% that their overall mood has decreased or worsened due to the coronavirus and the implemented measures.
At Least 30% of the respondents have observed increased violence in their households or the streets. Violence toward women and children has been discussed and addressed by many entities requesting governments to make sure that vulnerable populations are not left behind. 21
One hundred twelve participants considered consulting a psychiatrist regarding their decreased mental health issues. However, only 23.2% of them actually did, and 17.9% of them did so through virtual consultations.
More than 80% of all respondents are worried about the impact of coronavirus (COVID-19) on the future.
Conclusion
COVID-19 is a very unfortunate event that has many people stressed, jobless and isolated. Respondents’ fear of infection and increased mental stressors suggest how vulnerable they are. In addition to that, the study findings suggest that the socioeconomic context of the COVID-19 crisis has impacted their employment status sustainability. Furthermore, the increasing percentage noted in the study for household violence, as well as, social stigma associated with the coronavirus suggests devastating extra stressors to such a vulnerable group. Although the increasing burden is obvious with the study findings, the findings show that less than their quarter sought assistance through virtual consultations with a psychiatrist.
Recommendations
Actions must be taken to ensure the vulnerable populations are not left behind and in order to maintain the wellbeing of youth. The uncertainty of their future and the vague and changing nature of the virus is an extra stressor that the world needs to withstand. Boldness is required to acknowledge the stress the whole world is facing.
Young people need to be provided with safe access to online medical consultations, with highest degrees of professionalism, confidentiality, and optional anonymity, if needed.
More health awareness campaigns need to be implemented, that have an adaptable nature and readiness to respond to any arising rumors and misinformation in a timely manner. These Campaigns should also tackle the concerns and advocate for assurances to be provided to young people regarding the unpredictability of their education system and employment situations. Governments need to ensure that young people are an essential component of the response and provide them with working and learning opportunities adaptable to the current circumstances. Moreover, further support needs to be extended to enable them to transition back to their normal lifestyle, whenever possible.
Limitations of the study
Understanding of the virus and actions to mitigate its spread has evolved since this study, and we could not expand on those developments. Items included in planned follow-up waves of the survey will adapt accordingly and expand data capture on behaviors, among other just-in-time topics.
This study was conducted online among a random group of young people in Egypt, which was very difficult in the early phases of the COVID-19 pandemic quarantine measures. Thus, these findings may have limited generalizability, especially for the whole population adults. And finally, as was clarified in the results, a small percentage of people refused to participate in the study.
Footnotes
Appendix
Statistical analysis of stigma amongst different groups.

| Do you think the new Coronavirus is a stigma towards people infected by it? | Yes | No | p-value | |
|---|---|---|---|---|
| Gender | Male | 38 (22.6%) | 130 (77.4%) | 0.258 |
| Female | 43 (18.1%) | 195 (81.9%) | ||
| Education degree | Preparatory education or less | 1 (33.3%) | 2 (66.6%) | 0.226 |
| Secondary | 6 (31.6%) | 13 (68.4%) | ||
| University or postgraduate | 74 (19.3%) | 310 (80.7%) | ||
| Place of residence | Urban | 13 (18.1%) | 59 (81.9%) | 0.657 |
| Rural | 68 (20.0%) | 325 (80.0%) | ||
Acknowledgements
We would like to extend our gratitude to all the study participants and the organizations that help to disseminate the survey amongst the population group, namely the International Federation of Medical Students’ Associations in Egypt and Y-Peer Egypt
Author contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the executive board of the participating organizations to enable rollout of the survey.