
Abstract
Objectives:
Diabetes may delay milk letdown, and perceiving milk production as insufficient can lead to breastfeeding cessation. We evaluated whether prepregnancy or gestational diabetes is associated with cessation of breastfeeding by 1 week postpartum.
Methods:
We analyzed 2016-2018 data from 42 sites in the Pregnancy Risk Assessment Monitoring System, a population-based survey of women with a recent live birth. Participants were surveyed 2-6 months after childbirth. We used logistic regression models to evaluate the relationship between prepregnancy or gestational diabetes only and breastfeeding <1 week postpartum among women who had initiated breastfeeding.
Results:
Among 82 050 women who initiated breastfeeding, 4.5% reported breastfeeding <1 week postpartum. Overall, 11.7% of women reported any history of diabetes in the 3 months before becoming pregnant; 3.3% reported prepregnancy diabetes, and 8.4% reported gestational diabetes only. In both unadjusted and adjusted models, the prevalence of breastfeeding <1 week postpartum did not differ significantly among women with prepregnancy diabetes or gestational diabetes only compared with women without any history of diabetes. The prevalence of breastfeeding <1 week postpartum was 4.4% among women without any history of diabetes, 5.6% among women with prepregnancy diabetes (adjusted prevalence ratio [aPR] = 1.15; 95% CI, 0.91-1.46), and 4.5% among women with gestational diabetes only (aPR = 1.01; 95% CI, 0.84-1.20).
Conclusions:
We found no association between a history of diabetes prepregnancy or gestational diabetes only and breastfeeding <1 week postpartum in a large, population-based survey of postpartum women who initiated breastfeeding. Regardless of their diabetes status, women who want to breastfeed might benefit from interventions that support their ability to continue breastfeeding.
Breastfeeding is associated with considerable health benefits for both mother and child. Mothers who breastfeed have a lower risk, compared with mothers who do not breastfeed, of type 2 diabetes, postpartum depression, breast cancer, and ovarian cancer.1,2 Breastfed children have lower rates than nonbreastfed children of infant mortality, respiratory illness, and asthma.1,3-5 Furthermore, formula use incurs health care costs: the direct medical costs of suboptimal breastfeeding was estimated at $3 billion in 2014 in the United States. 6 Consequently, the American Academy of Pediatrics recommends exclusively breastfeeding for about the first 6 months of infant life, followed by breastfeeding in combination with complementary foods until at least 12 months of age. 7 However, only 25% of infants born in 2017 in the United States were exclusively breastfed through 6 months, and only 35% of infants were breastfed for 1 year. 8
Successful long-term breastfeeding for mothers with prepregnancy or gestational diabetes is particularly important because metabolic adaptations during lactation can reverse atherogenic and diabetogenic effects from pregnancy. 9 Diabetes, however, is associated with decreased breastfeeding at 2 months postpartum. 10 It is unknown whether, among the subset of women who initiate breastfeeding, women with diabetes are at higher risk, compared with women without diabetes, of discontinuing breastfeeding before they intend to. Some evidence suggests that diabetes may inhibit lactogenesis stage II, defined as the initial onset of copious production of milk within the first 72 hours postpartum.11-16 Because delays in milk letdown or perceiving milk production as insufficient are key causes of discontinuation in the immediate postpartum period,17,18 diabetes theoretically could lead to breastfeeding cessation in this early period. Thus, our objective was to evaluate the associations between diabetes type (prepregnancy or gestational, assessed separately) and cessation of breastfeeding in the first week postpartum among women who initiated breastfeeding.
Methods
Overview of Survey
We used data from the Centers for Disease Control and Prevention (CDC) Pregnancy Risk Assessment Monitoring System (PRAMS), a surveillance system conducted by CDC in collaboration with state and jurisdiction health departments, which has been described elsewhere. 19 Using both mail and telephone data collection methods, PRAMS collects site-specific, population-based, self-reported data on maternal behaviors and experiences before, during, and shortly after pregnancy among women who had a live birth. Women are randomly sampled from site birth certificates at 2-6 months postpartum and are invited to complete the survey by mail. We used 2016-2018 data from sites that achieved a 55% response rate threshold for data release for at least 1 study year. The institutional review boards (IRBs) of CDC and PRAMS sites provided ethical and approval review for the PRAMS protocol. The Ohio State University IRB determined our analysis to be exempt from review because of its use of only deidentified, publicly available data.
Measure of Diabetes
We created an independent variable for having prepregnancy diabetes, gestational diabetes only (ie, no prepregnancy diabetes), or neither based on the following 2 yes/no questions: (1) “During the 3 months before you got pregnant with your new baby, did you have type 1 or type 2 diabetes (NOT gestational diabetes or diabetes that starts during pregnancy)?” and (2) “During your most recent pregnancy, did you have gestational diabetes (diabetes that started during this pregnancy)?” We classified women who responded that they had both prepregnancy diabetes and gestational diabetes as having prepregnancy diabetes. We defined “without diabetes” as not having any history of diabetes.
Measure of Breastfeeding Cessation at <1 Week Postpartum
Participants were asked, “Did you ever breastfeed or pump breast milk to feed your new baby, even for a short period of time?” Those who responded yes were asked whether they currently were breastfeeding or feeding their baby pumped milk (yes or no). Those who were no longer breastfeeding when they completed the PRAMS survey were asked to report the duration, in weeks or months, that they breastfed. For our primary outcome, breastfeeding <1 week postpartum, we created a dichotomous variable (yes or no) for breastfeeding for <1 week among those who initiated any breastfeeding (ie, including feeding at the breast or pumping milk). At the time of survey completion, women who reported their infants were deceased or not living with them were instructed to skip questions on breastfeeding.
Confounders
We considered the following characteristics as confounders given their association in the literature with diabetes and breastfeeding <1 week postpartum20-29: marital status (married or unmarried), maternal education (<high school diploma, high school diploma or GED [General Educational Development], or ≥some college), race and ethnicity (non-Hispanic Black, non-Hispanic White, Hispanic, non-Hispanic American Indian/Alaska Native, non-Hispanic Other [reported ≥1 race or other non-White], or non-Hispanic Asian or Pacific Islander), age (<20, 20-24, 25-34, and ≥35 y), chronic hypertension (yes or no), enrollment in the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) during pregnancy (yes or no), any cigarette use during pregnancy (yes or no), delivery method (cesarean section or vaginal delivery), infant birth weight (<2500 g [low birth weight], 2500-4000 g [normal birth weight], >4000 g [macrosomia]), and body mass index (BMI; in kg/m2; underweight [<18.5], overweight [25.0-29.9], obese [≥30.0], and normal [18.5-24.9]). Most confounders included in the PRAMS dataset were derived from birth certificate data; however, BMI was a composite variable in the PRAMS dataset that was computed from self-reported weight and height in the PRAMS survey.
Statistical Analysis
Among women who initiated breastfeeding, we examined the weighted prevalence of breastfeeding <1 week postpartum and confounders of interest by diabetes status. We excluded from analysis women who did not initiate breastfeeding, because the objective of this analysis was to assess breastfeeding cessation among those who had initiated breastfeeding. While other factors independent of physiologic factors (eg, breastfeeding intention) may influence breastfeeding initiation, we were unable to control for these other factors with the data available in the PRAMS dataset.
We used 95% CIs to assess differences in the distribution of characteristics by diabetes status; that is, we used nonoverlapping CIs to indicate significant differences. We computed unadjusted prevalence ratios (PRs) using unadjusted logistic regression models to evaluate the relationship between each confounder, prepregnancy diabetes, and gestational diabetes only and breastfeeding <1 week postpartum. We constructed a separate model for each confounder. We then constructed the final adjusted logistic regression model to compute adjusted PRs (aPRs) that accounted for the confounders. We also conducted sensitivity analyses to assess (1) differences between women included in the analysis and women excluded because of missing data on covariates, (2) whether the inclusion of women with missing data on covariates affected the regression results, and (3) differences in breastfeeding duration at ≤2 (vs >2) and ≤4 (vs >4) weeks postpartum. To make the data representative of each site’s population of live births, we used sample weights to account for the sampling design, nonresponse, and noncoverage. We conducted the analyses using SAS-callable SUDAAN version 11.0.3 (RTI International).
Results
Overall, data from surveys conducted in 2016 (31 sites), 2017 (36 sites), and 2018 (31 sites) were eligible for inclusion (Figure). The weighted mean response rate for these 42 sites was 61% during the study period. Our analytic sample excluded women who reported their infants were deceased or not living with them at the time of survey completion (n = 1942) and women who did not initiate breastfeeding (n = 12 707). After excluding women with missing data on breastfeeding duration (n = 2612), diabetes status (n = 1422), and confounders (n = 7377), our final analytic sample included 82 050 women. A higher proportion of women with missing data than women in the analytic sample were unmarried; had ≤high school education; were non-Hispanic Black, non-Hispanic Asian or Pacific Islander, or Hispanic; were aged ≤24 years; were enrolled in WIC during pregnancy; and had an infant with a low birth weight. The distribution of other characteristics was similar between women included in the analytic sample and women excluded because of missing data (online-only Supplemental Table S1).
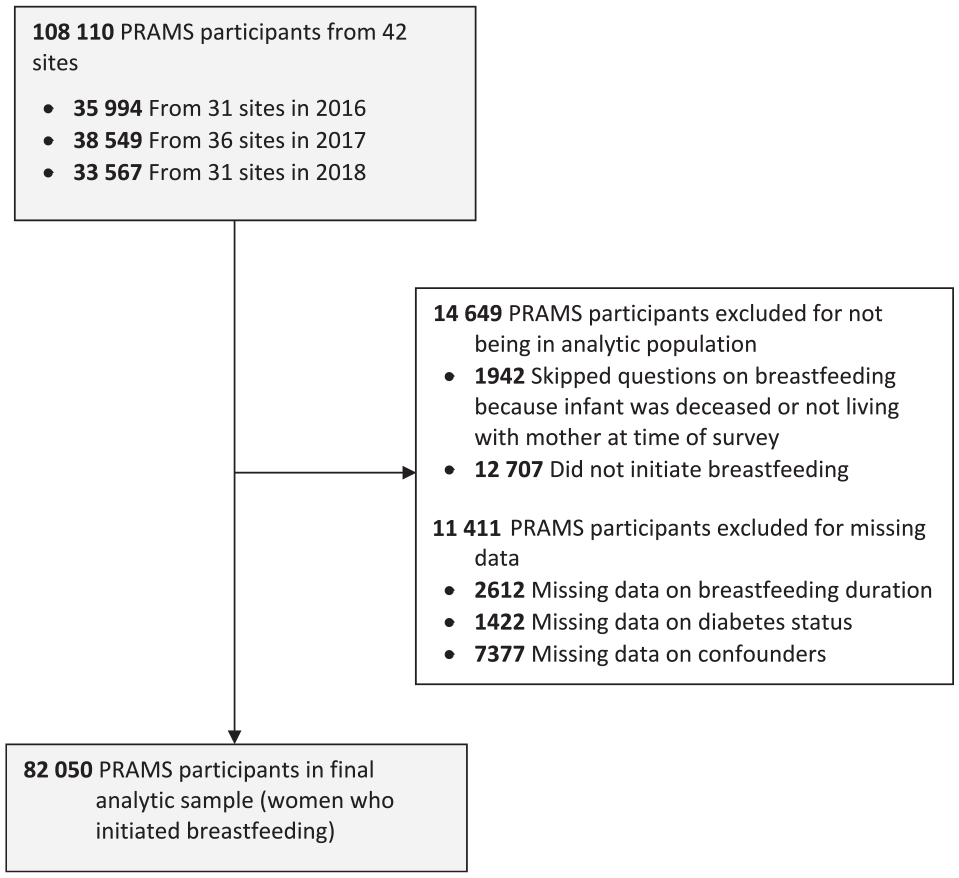
Selection and exclusion of respondents for analyses of data from the Pregnancy Risk Assessment Monitoring System (PRAMS), 2016-2018, to compare breastfeeding <1 week postpartum among women with and without diabetes. Data source: Shulman et al. 19
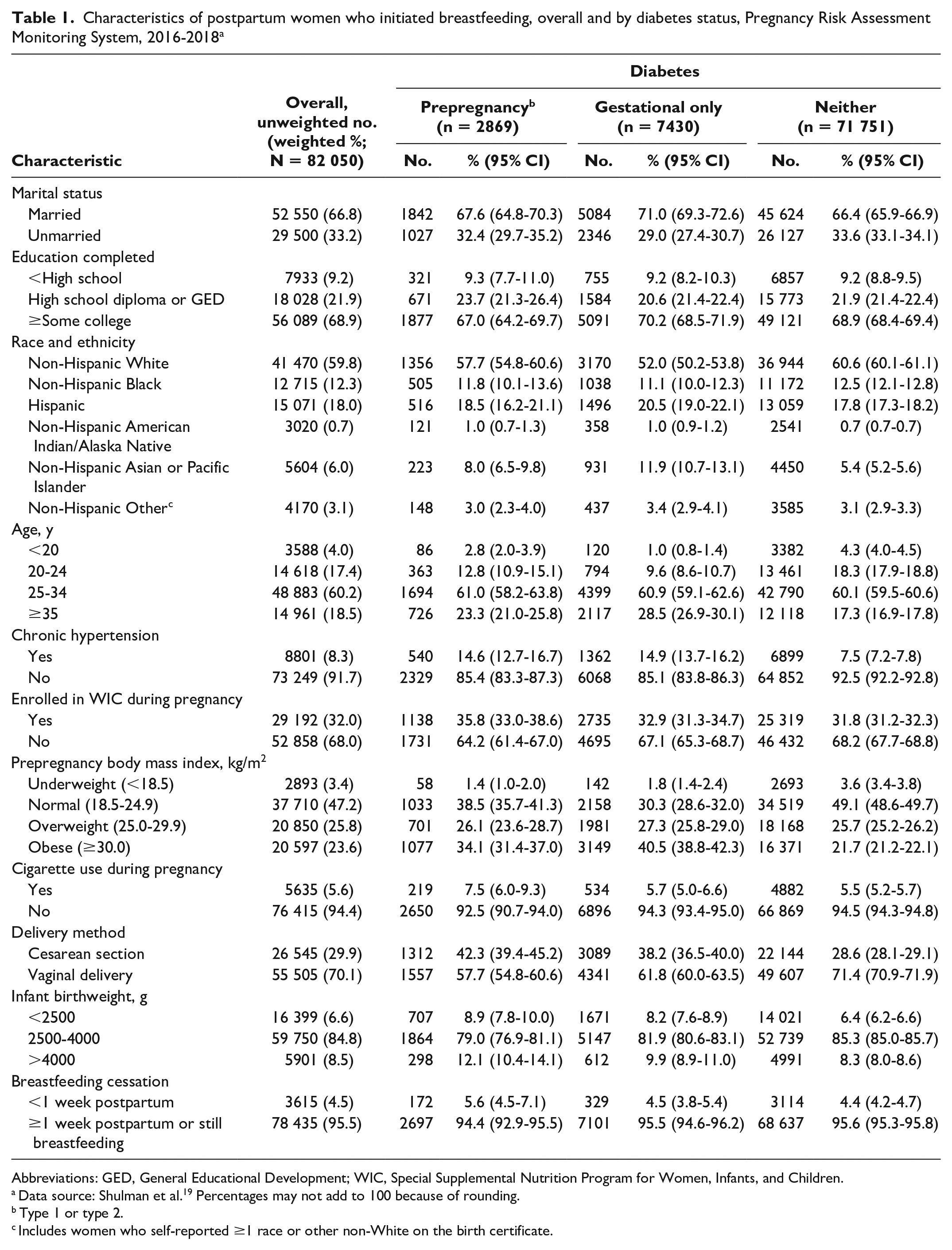
Most women in the analytic sample were married, had completed at least some college, were non-Hispanic White, and were aged ≥25 years (Table 1). Most women did not have chronic hypertension, were not enrolled in WIC during pregnancy, and did not report cigarette use during pregnancy. Nearly half had a normal prepregnancy BMI. Most women had a vaginal delivery (70.1%) and gave birth to an infant with a normal birth weight (84.8%). While 88.3% of women (n = 71 751) did not have diabetes during their pregnancy, 3.3% had prepregnancy diabetes and 8.4% had gestational diabetes only. Overall, 4.5% of women had ceased breastfeeding by 1 week postpartum.
Characteristics of postpartum women who initiated breastfeeding, overall and by diabetes status, Pregnancy Risk Assessment Monitoring System, 2016-2018 a
Abbreviations: GED, General Educational Development; WIC, Special Supplemental Nutrition Program for Women, Infants, and Children.
Data source: Shulman et al. 19 Percentages may not add to 100 because of rounding.
Type 1 or type 2.
Includes women who self-reported ≥1 race or other non-White on the birth certificate.
The distribution of selected characteristics differed between women with and without diabetes in the 3 months before becoming pregnant. Compared with women without diabetes, a higher proportion of women with either prepregnancy or gestational diabetes were non-Hispanic Asian or Pacific Islander, were aged ≥35 years, had hypertension, had obesity prepregnancy, had a cesarean section, and had an infant with a low birth weight.
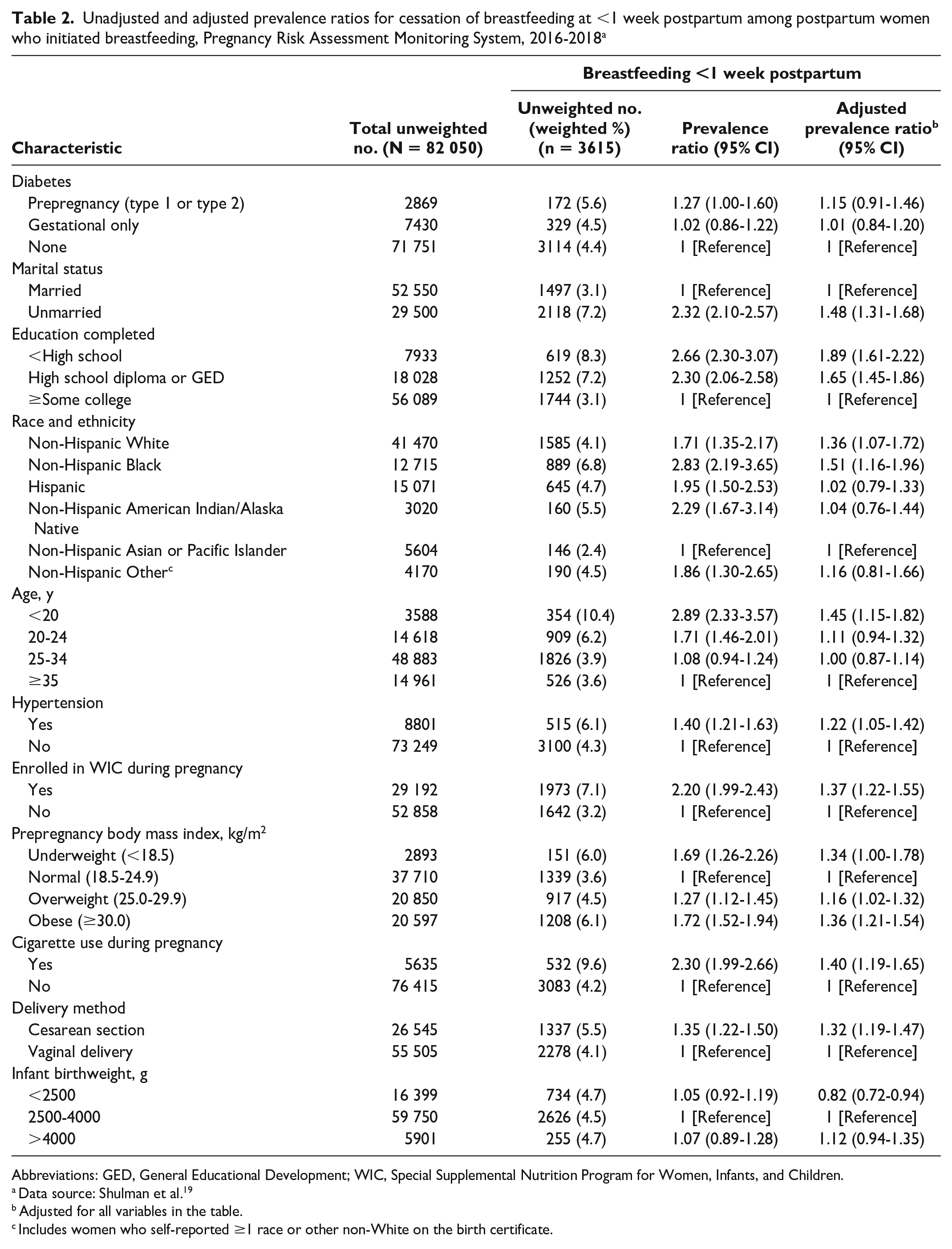
In adjusted analyses, the prevalence of breastfeeding <1 week postpartum was significantly higher among women who had the following demographic characteristics: were unmarried (vs married), had ≤high school diploma or GED (vs ≥some college), were non-Hispanic Black or non-Hispanic White (vs non-Hispanic Asian or Pacific Islander), and were aged <20 years (vs aged ≥35 y). The prevalence of breastfeeding <1 week postpartum was also significantly higher among women reporting the following conditions or behaviors: having chronic hypertension (vs not), enrollment in WIC during pregnancy (vs not), an overweight or obese prepregnancy BMI (vs normal prepregnancy BMI), smoked cigarettes during pregnancy (vs not), and delivered via cesarean section (vs vaginal delivery; Table 2). The prevalence of breastfeeding <1 week postpartum was lower among women with infants who had a low birth weight (vs normal birthweight; aPR = 0.82; 95% CI, 0.72-0.94).
Unadjusted and adjusted prevalence ratios for cessation of breastfeeding at <1 week postpartum among postpartum women who initiated breastfeeding, Pregnancy Risk Assessment Monitoring System, 2016-2018 a
Abbreviations: GED, General Educational Development; WIC, Special Supplemental Nutrition Program for Women, Infants, and Children.
Data source: Shulman et al. 19
Adjusted for all variables in the table.
Includes women who self-reported ≥1 race or other non-White on the birth certificate.
In both the unadjusted and adjusted models, the prevalence of breastfeeding <1 week postpartum did not differ significantly among women with prepregnancy diabetes and gestational diabetes only compared with those without diabetes. The prevalence of breastfeeding <1 week postpartum among women with prepregnancy diabetes was 5.6%, compared with 4.4% among those without diabetes (aPR = 1.15; 95% CI, 0.91-1.46). The prevalence of breastfeeding <1 week postpartum among women with gestational diabetes was 4.5%, similar to the prevalence among women without diabetes (aPR = 1.01; 95% CI, 0.84-1.20). In sensitivity analyses that included women with missing data on covariates, the results of the adjusted models were consistent with the results reported for the analytic sample (online-only Supplemental Table S2). In additional sensitivity analyses, when comparing breastfeeding cessation at ≤2 weeks and ≤4 weeks, breastfeeding cessation did not differ between women with prepregnancy diabetes and women without diabetes at ≤2 weeks or ≤4 weeks. However, a higher proportion of women with gestational diabetes reported breastfeeding cessation at ≤2 weeks (21.0% vs 19.4%; aPR = 1.09; 95% CI, 1.01-1.18) and ≤4 weeks (33.8% vs 30.3%; aPR = 1.10; 95% CI, 1.04-1.15) compared with women without diabetes.
Discussion
Our study findings from a representative survey of recently postpartum women in 42 sites in the United States during 2016-2018 showed that, among women who initiated breastfeeding, prepregnancy diabetes and gestational diabetes only were not significantly associated with breastfeeding cessation by 1 week postpartum. We adjusted for maternal characteristics, behaviors, and conditions that are thought to act as confounders of diabetes and cessation of breastfeeding.20-29 Consistent with the literature, these factors were independently associated with breastfeeding <1 week postpartum in our analysis, except for low birth weight, which had an inverse relationship. Specifically, the prevalence of breastfeeding <1 week postpartum was higher among women who were unmarried (vs married), had ≤high school diploma or GED (vs ≥some college), were non-Hispanic Black or non-Hispanic White (vs non-Hispanic Asian or Pacific Islander), were aged <20 years (vs aged ≥35 y), had chronic hypertension (vs not), were enrolled in WIC during pregnancy (vs not), did not have a normal prepregnancy BMI (vs normal prepregnancy BMI), used cigarettes during pregnancy (vs not), and delivered via cesarean section (vs vaginal delivery). These factors could be used to identify women who might need additional support to successfully continue breastfeeding.
Although women might not initiate breastfeeding for a range of reasons (eg, lack of clinician support, household responsibilities, lack of breastfeeding education), the cessation of breastfeeding before women intended to cease breastfeeding could indicate a problem with milk letdown or production.17,18 Lower levels of serum insulin secretion relative to serum glucose after a glucose challenge and lower serum adiponectin predict delayed lactogenesis. 11 These factors, related to metabolic glucose control, suggest that poor glucose control can delay lactogenesis. Studies have demonstrated an association between diabetes and delayed lactogenesis overall or during stage II12-16 or delayed milk prolactin concentration (a marker for successful lactogenesis stage II). 29 However, these studies had small sample sizes, ranging from 39 to 77 women, and, thus, could not control adequately for important factors. A larger analysis (n = 3404) was conducted among a subset of participants in the Black Women’s Health Study, a convenience study of Black women in the United States who were primiparous with a singleton birth during 1995-2009. 30 In the Black Women’s Health Study, which controlled for factors including age and BMI, women with any history of prepregnancy diabetes ceased breastfeeding earlier than women without any history of prepregnancy diabetes.
Similarly, gestational diabetes has been linked to delayed lactogenesis. A prospective cohort study of 883 women with gestational diabetes treated with insulin found that 33% of women reported delayed lactogenesis; however, the study did not include a comparison arm of women without gestational diabetes. 31 Other studies suggesting an association between gestational diabetes and poor lactation were limited by small sample sizes of 16-40 women.11,32
Our analysis, however, measured breastfeeding cessation by 1 week postpartum for any reason rather than delayed lactogenesis specifically. Furthermore, participants with recognized diabetes who intended to breastfeed might have received targeted interventions to promote their successful breastfeeding, which might have mitigated the effects of their diabetes condition on lactation. Most evidence on the effects of diabetes on lactogenesis, to date, has come from studies with small sample sizes,11-14,23-29 which may also explain differences. Our analysis was strengthened by the use of data from a large, population-based sample of women from 42 sites. Also, we were able to adjust for many potential confounders of the relationship between diabetes and cessation of breastfeeding at <1 week postpartum, and, in contrast to previous research on this topic,11-16,30-32 we evaluated prepregnancy diabetes and gestational diabetes separately. This separation is important because the 2 conditions could differ in their effect on lactogenesis. In addition, in sensitivity analyses, gestational diabetes was associated with breastfeeding cessation by 2 weeks and 4 weeks postpartum, which is important given that breastfeeding could reduce diabetes risk; however, whether this finding is related to delayed lactogenesis is unknown.
Limitations
This study had several potential limitations. First, we relied on self-reported data, which are subject to misclassification from social desirability bias and recall bias. Second, data were cross-sectional and can be used only to assess associations. Third, PRAMS did not differentiate between type 1 and type 2 diabetes or the degree to which women were successfully managing their prepregnancy or gestational diabetes. Without an indicator of glycemic control (eg, glycated hemoglobin A1c) or use of insulin or medications (eg, metformin) for glycemic control, our measure of a true association between diabetes and breastfeeding <1 week postpartum could have been masked. Fourth, we were not able to assess other diabetes-related factors (eg, breastfeeding intention) that might influence a woman’s decision or ability to continue breastfeeding, because such data were not available in PRAMS. Fifth, the wording in the PRAMS survey questions asked women to self-report if they had prepregnancy or gestational diabetes in contrast to asking if they were told by a health care provider that they had these conditions. The broad wording may have led women to overreport diabetes, thus weakening the association between diabetes and breastfeeding <1 week postpartum. Sixth, women excluded from the analysis because of missing data differed from the analytic sample for some characteristics, including marital status, education, race and ethnicity, age, WIC participation, and infant birth weight. While the exclusion of these respondents might have influenced the results, findings for breastfeeding cessation <1 week postpartum in the sensitivity analysis were consistent with findings in the analytic sample. Lastly, the analysis might not have been powered to detect differences by diabetes status given the small proportion of the sample who reported having diabetes.
Conclusion
Regardless of their diabetes status, women who want to breastfeed might benefit from interventions that support their ability to carry out the practice and address differences in breastfeeding <1 week postpartum by demographic factors. 33 Hospital interventions shown to improve breastfeeding outcomes include avoiding use of supplemental feedings and pacifiers, breastfeeding on demand, breastfeeding instruction, having the infant remain with the mother rather than in the hospital nursery, initiating breastfeeding immediately (ideally within 1 hour) after birth, and integrating lactation support and specialists in primary and pediatric care.33-35 Furthermore, because improving glycemic control among women with insulin-dependent diabetes leads to increased prolactin secretion, 16 future research could assess the role of glycemic control among women with diabetes and breastfeeding cessation.
Supplemental Material
sj-docx-1-phr-10.1177_00333549221099082 – Supplemental material for Prepregnancy and Gestational Diabetes and Cessation of Breastfeeding <1 Week Postpartum, United States, 2016-2018
Supplemental material, sj-docx-1-phr-10.1177_00333549221099082 for Prepregnancy and Gestational Diabetes and Cessation of Breastfeeding <1 Week Postpartum, United States, 2016-2018 by Katherine Kortsmit, Kirsten I. Boone, Lee Warner, Jessica Horan, Julie K. Bower and Maria F. Gallo in Public Health Reports
Footnotes
Disclaimer
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.