
Abstract
Objective:
Pregnant women are encouraged to engage in physical activity before and during pregnancy. However, few women in the United States engage in sufficient physical activity during pregnancy. We examined physical activity and factors associated with it before and during pregnancy.
Methods:
We analyzed the most recent data from the Pregnancy Risk Assessment Monitoring System (PRAMS; 2016-2019) to describe physical activity among women in Alabama and Rhode Island. We used logistic regression models to assess factors associated with physical activity before and during pregnancy.
Results:
Only 14.6% (n = 1178) of the sample (n = 7734; 3621 in Alabama, 4113 in Rhode Island) met physical activity guidelines before pregnancy and 8.8% (n = 666) during pregnancy. Identifying as White (adjusted odds ratio [AOR] = 1.46) or non-Hispanic ethnicity (AOR = 1.46), being underweight or normal weight (AOR = 1.98), and residing in Rhode Island (AOR = 1.30) were significantly associated with meeting physical activity guidelines before pregnancy. Being underweight or normal weight (AOR = 1.70) remained a significant variable associated with meeting physical activity guidelines during pregnancy.
Conclusions:
Public health professionals and health care providers may consider factors such as race, ethnicity, and body mass index when working to increase physical activity among women before and during pregnancy.
Physical activity maintains and improves overall health, lowers the risk of chronic disease, and extends life expectancy. 1 Physical activity is especially important during the perinatal period to improve the health of the mother and baby; pregnant women are encouraged to engage in physical activity before and during pregnancy and postpartum. 2 Exercising during pregnancy has numerous advantages, including decreased risk for gestational diabetes, excessive weight gain, gestational hypertension, cesarean section, and postpartum depression.3-7 Engagement in physical activity during pregnancy may also help to reduce financial burdens on the US health care system. 8 Preeclampsia costs the US health care system >$2 billion annually; however, the risk for preeclampsia could be reduced with regular engagement in physical activity. 8
The American College of Obstetricians and Gynecologists advises that health care providers encourage women who are having uncomplicated pregnancies to participate in aerobic and muscle-strengthening exercises before, during, and after pregnancy. 2 The college recommends that pregnant women engage in at least 150 minutes of moderate-intensity aerobic physical activity per week.2,9 Most pregnant patients can engage in physical activity to some capacity, and few pregnancy-related medical conditions make it completely contraindicated.2,10 Additionally, women who engage in vigorous-intensity exercise before pregnancy may continue during pregnancy and postpartum. 2
A recent systematic review and meta-analysis found that a low proportion of women in the United States engage in sufficient physical activity during pregnancy. 11 Data from the National Health and Nutrition Examination Survey from 2007 to 2014 indicate that the prevalence of pregnant women meeting physical activity guidelines was only 12.7%. 12 Data from the Centers for Disease Control and Prevention’s (CDC’s) Pregnancy Risk Assessment Monitoring System (PRAMS) in Colorado during 2012-2015 showed that only 10.2% of pregnant women met physical activity guidelines. 13 Epidemiologic data suggest that physical activity levels are consistently low among pregnant women, and few pregnant women meet recommendations for it during pregnancy. Physical inactivity during pregnancy is associated with multiple health problems, including hypertension, obesity, gestational diabetes, cardiovascular disease, and lung disease. 2 Engagement in physical activity may help minimize excessive weight gain and gestational diabetes during pregnancy and reduce symptoms of postpartum depression. 14 Therefore, it is crucial to encourage physical activity during pregnancy and the postpartum period to enhance maternal health.
While existing research underscores the importance of physical activity during pregnancy, less is known about the factors that influence its engagement before and during pregnancy. Literature on the factors associated with physical activity during pregnancy is mixed, suggesting that more research is needed.12,13,15-21 Additionally, limited population-level data are available to describe physical activity and the factors associated with it before and during pregnancy. The objective of this study was to examine factors associated with meeting physical activity guidelines before and during pregnancy using the most recent PRAMS data (phase 8). 22 This study expands the existing literature to better understand physical activity and the factors associated with it among pregnant women. Findings from this study can help inform health education specialists and health care providers in developing interventions, programs, and counseling approaches to encourage women to engage in physical activity before and during pregnancy.
Methods
Database and Sample
This cross-sectional analysis examined data collected from 2016 to 2019 in the most recent PRAMS 22 survey (phase 8). Data from 2020 were not included because of the potential variation in physical activity and limited access to opportunities and facilities during the COVID-19 pandemic.23,24 A detailed overview of the PRAMS survey and procedures can be found elsewhere. 22 PRAMS was initiated in 1987 and is a joint surveillance project between state health departments and CDC that collects data on pregnancy. Women with a recent live birth in participating states are chosen at random from birth certificate records and mailed a survey 2 to 6 months after delivery. Participants are deemed nonresponders if they do not complete the survey after they are contacted by telephone because of nonresponse to the mailed survey. 22
We analyzed PRAMS data for Alabama and Rhode Island because only these 2 states collected information about the outcome variables of interest related to physical activity. PRAMS data collection methods and survey methodology for Alabama and Rhode Island were comparable, 22 enabling us to combine data from the 2 states into a pooled dataset. A total of 8173 pregnant respondents were assessed for inclusion in this study. Pregnant women who were told by a health care provider that they could not engage in physical activity for any reason before or during pregnancy were excluded (n = 439), resulting in a final analytic sample of 7734: 3621 in Alabama and 4113 in Rhode Island. Because of the public availability and deidentified nature of PRAMS data, The University of Alabama Institutional Review Board deemed this study exempt from board review.
Measures
The outcome variables for the study were binary indicators of whether the pregnant women met physical activity guidelines before and during pregnancy. Physical activity was assessed by 2 self-reported items: one for before pregnancy and another for during pregnancy. The items asked, “During the 3 months before you got pregnant with your new baby/during the last 3 months of your pregnancy, how often did you participate in any physical activities or exercise for 30 minutes or more?” Both items included the following response options: “less than 1 day per week,” “1 to 2 days per week,” “3 to 4 days per week,” “5 or more days per week,” and “I was told by a doctor, nurse, or other health care worker not to exercise.” For the analysis, participants who reported exercising for ≥30 minutes for ≥5 days per week were coded as meeting physical activity guidelines (1 = yes), while participants who reported any other responses were coded as not meeting guidelines (0 = no).
Independent variables included sociodemographic, intrapersonal, and interpersonal factors. Sociodemographic and intrapersonal characteristics were as follows: maternal age (<24, 25-34, ≥35 y), race (White, Black/African American, other [American Indian, Chinese, Japanese, Filipino, Hawaiian, other non-White, Alaska Native, mixed race, and other Asian racial categories]), ethnicity (Hispanic, non-Hispanic), education level (high school diploma or less, some college, college or advanced degree), prepregnancy body mass index (BMI; underweight/normal weight, overweight, obese), health insurance (private, other [Medicaid, self-pay, Indian Health Services, CHAMPUS/TRICARE, and other government sources]), annual household income (<$16 000, $16 000-$39 999, $40 000-$85 000, >$85 000), gestational age at first prenatal visit (number of weeks, number of months, did not go), number of previous live births (0, 1, ≥2), and pregnancy intention (intended at that time, intended later, intended sooner, not intended at that time/unsure). Interpersonal variables included marital status (married, not married), Special Supplemental Assistance Program for Women, Infants, and Children (WIC; yes, no), prepregnancy health care visit (yes, no), access to a health care provider (yes, no), number of prenatal visits (<8, 9-11, ≥12), and health care provider advice about weight gain during pregnancy (yes, no). We cleaned all data and recoded variables before analysis. We used original categories for PRAMS items and coding schemes (eTable 1 in the Supplement).
Data Analysis
We conducted descriptive analyses to calculate rates of meeting physical activity guidelines before and during pregnancy and to summarize sample characteristics with unweighted frequencies and weighted percentages. We conducted bivariate analyses to examine associations between sociodemographic, intrapersonal, and interpersonal factors and meeting physical activity guidelines before and during pregnancy. We assessed associations between categorical variables and physical activity by using the Pearson χ2 test, and we used point biserial correlation to determine relationships between continuous variables and physical activity. We included variables that demonstrated statistical significance (hereinafter, significance) in the bivariate analyses (P < .05) in the multivariable models.
We developed separate multivariable logistic regression models for meeting physical activity guidelines before and during pregnancy. Each model included the sociodemographic, intrapersonal, and interpersonal factors identified as significant in the corresponding bivariate analyses. We estimated the proportion of variance explained by the logistic regression models using Nagelkerke R2. We also examined potential 2-way interaction effects (eg, WIC × race, WIC × ethnicity, married × education, health care provider advice about weight × race, health care provider advice about weight × BMI). For both regression models, we added covariates that did not demonstrate a significant univariate association with the outcomes to determine whether differences were observed. We observed no differences in the relationship between the independent variables and physical activity, so we retained the original models containing the variables with a significant univariate relationship with physical activity. All analyses accounted for the complex sampling design of PRAMS by using survey weights. We considered α = .05 to be significant. We treated missing values using listwise deletion. We conducted statistical analyses in SPSS Complex Samples Module version 28.0 (IBM Corp).
Results
Most participants were White (64.1%), non-Hispanic (88.0%), married (54.1%), and aged 25 to 34 years (56.9%) and had a nonprivate source of health insurance (53.4%; Table 1). More than half reported that they had a prepregnancy health care visit with their health care provider (58.9%) and received advice from a health care provider about weight gain during pregnancy (53.1%).
Characteristics of pregnant women, overall and by state, Pregnancy Risk Assessment Monitoring System, 2016-2019, Alabama and Rhode Island a
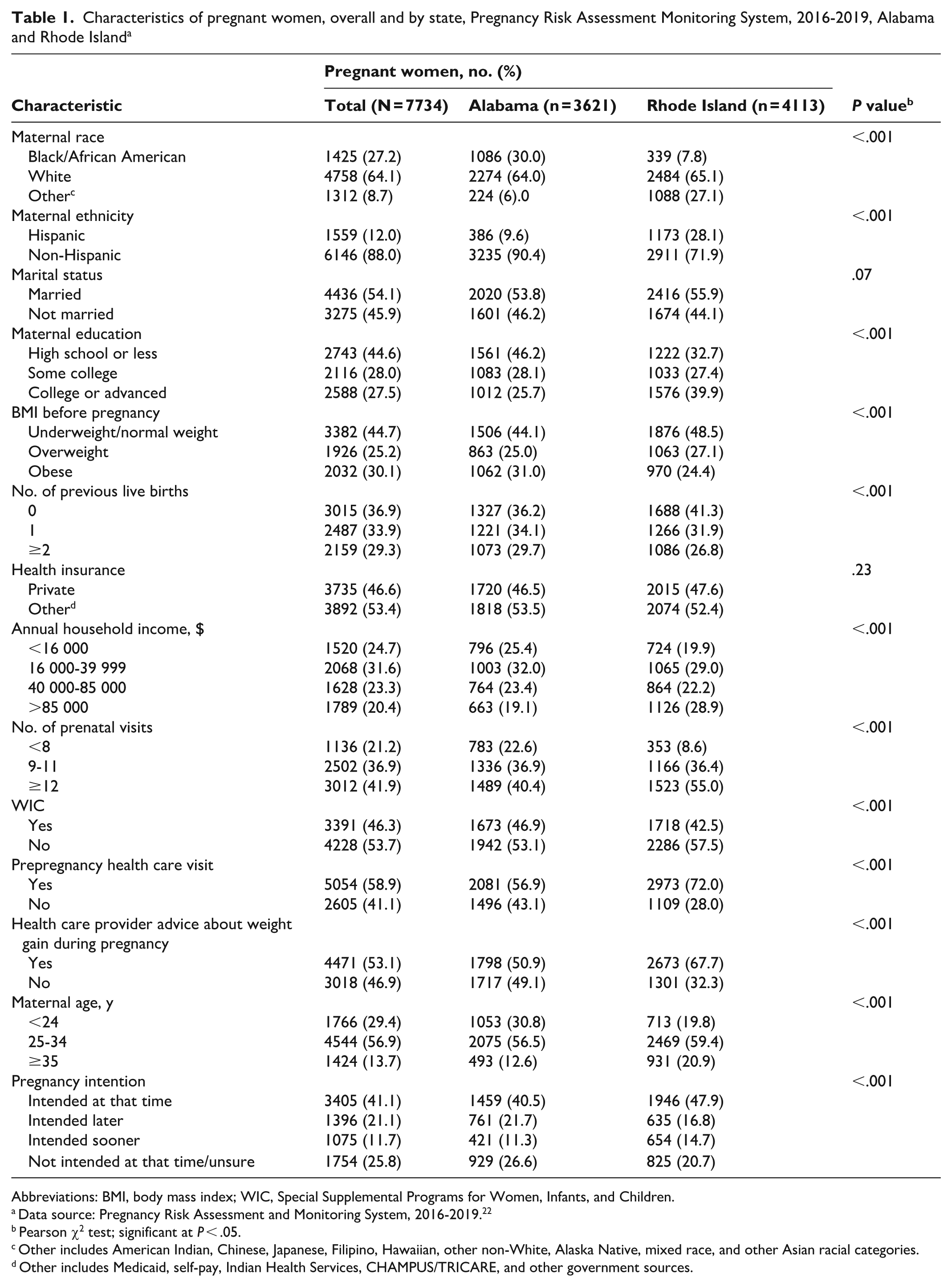
Abbreviations: BMI, body mass index; WIC, Special Supplemental Programs for Women, Infants, and Children.
Data source: Pregnancy Risk Assessment and Monitoring System, 2016-2019. 22
Pearson χ2 test; significant at P < .05.
Other includes American Indian, Chinese, Japanese, Filipino, Hawaiian, other non-White, Alaska Native, mixed race, and other Asian racial categories.
Other includes Medicaid, self-pay, Indian Health Services, CHAMPUS/TRICARE, and other government sources.
Before pregnancy, only 14.6% of the total sample met physical activity guidelines (Figure). Before pregnancy, a greater percentage of women in Rhode Island (17.7%) than in Alabama (14.1%) met physical activity guidelines (χ2 = 11.92; df = 2.99; P < .001). In the last trimester, only 8.8% of the total sample met physical activity guidelines. We found no significant association between state of residence and meeting physical activity guidelines during pregnancy (χ2 = 2.43; df = 3.00; P = .21).
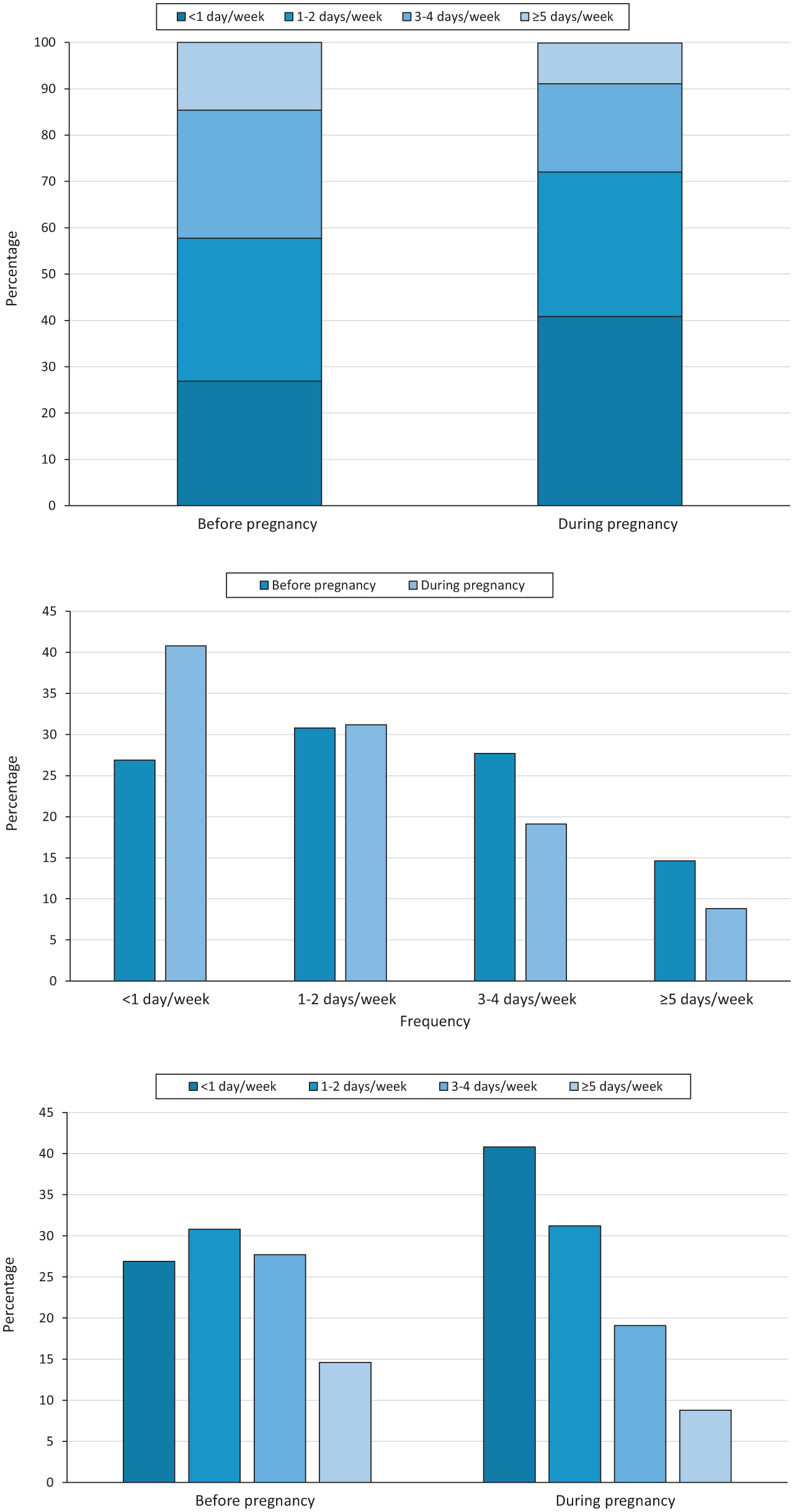
Rates of physical activity frequency among pregnant women before and during pregnancy, Pregnancy Risk Assessment Monitoring System, 2016-2019, Alabama and Rhode Island. Percentages were calculated according to sample probability weights. Data represent participant responses to the item “During the 3 months before you got pregnant with your new baby/during the last 3 months of your pregnancy, how often did you participate in any physical activities or exercise for 30 minutes or more?” Data source: Pregnancy Risk Assessment Monitoring System, 2016-2019. 22
We found significant relationships between meeting physical activity guidelines before pregnancy and race (χ2 = 39.76; df = 1.86; P < .001), ethnicity (χ2 = 11.10; df = 1.00; P < .001), prepregnancy BMI (χ2 = 79.94; df = 2.00; P < .001), and state of residence (χ2 = 8.89; df = 1.00; P < .001). During pregnancy, we found significant relationships between meeting physical activity guidelines and maternal age (χ2 [1.956; n = 7459] = 14.146; P = .02), education level (χ2 [1.975; n = 7187] = 23.624; P < .001), prepregnancy BMI (χ2 = 24.48; df = 2.00; P < .001), health insurance (χ2 = 27.70; df = 1.00; P < .001), annual household income (χ2 = 16.74; df = 2.97; P = .02), marital status (χ2 = 18.80; df = 1.00; P < .001), and WIC participation (χ2 = 11.47; df = 1.00; P = .01).
In the first logistic regression model, which explored physical activity before pregnancy (Nagelkerke R2 = .030; P < .001), the following variables were significantly associated with meeting physical activity guidelines: identifying as White (AOR = 1.46; P = .003) or non-Hispanic ethnicity (AOR = 1.46; P = .01), being underweight or normal weight (AOR = 1.98; P < .001), and residing in Rhode Island (AOR = 1.30; P < .001) (Table 2). Women with a prepregnancy BMI classified as underweight/normal weight (AOR = 1.98; 95% CI, 1.58-2.49) and overweight (AOR = 1.43; 95% CI, 1.10-1.85) had a greater likelihood of meeting physical activity guidelines than women with a BMI classified as obese. When compared with Black/African American women, White women had an increased likelihood of meeting physical activity guidelines (AOR = 1.46; 95% CI, 1.15-1.86). Additionally, non-Hispanic women (vs Hispanic women; AOR = 1.46; 95% CI, 1.07-1.99) and women who lived in Rhode Island (vs Alabama; AOR = 1.30; 95% CI, 1.11-1.51) had a greater likelihood of meeting the physical activity guidelines.
Multivariable logistic regression analysis of meeting physical activity guidelines before and during pregnancy, Pregnancy Risk Assessment Monitoring System, 2016-2019, Alabama and Rhode Island a
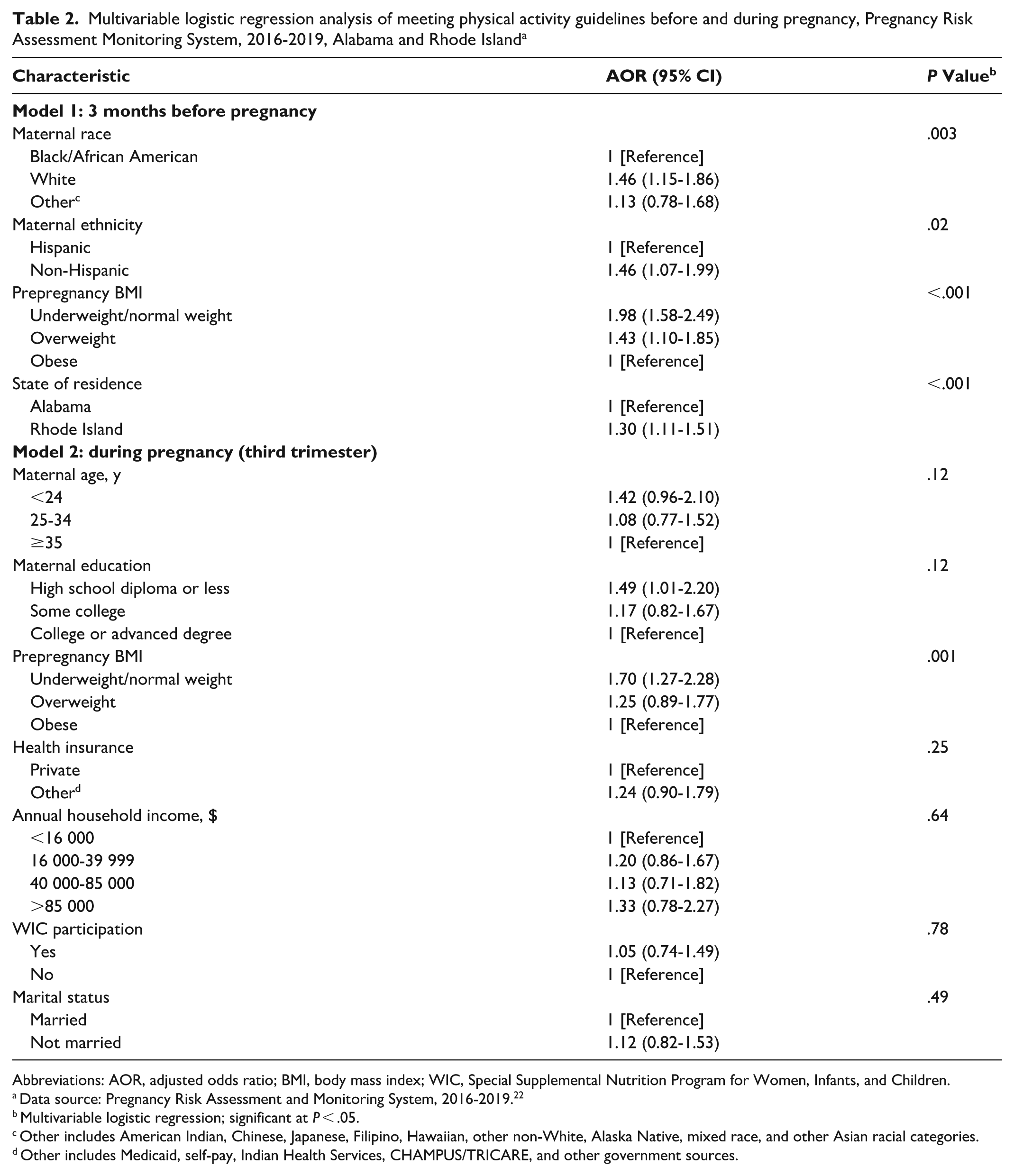
Abbreviations: AOR, adjusted odds ratio; BMI, body mass index; WIC, Special Supplemental Nutrition Program for Women, Infants, and Children.
Data source: Pregnancy Risk Assessment and Monitoring System, 2016-2019. 22
Multivariable logistic regression; significant at P < .05.
Other includes American Indian, Chinese, Japanese, Filipino, Hawaiian, other non-White, Alaska Native, mixed race, and other Asian racial categories.
Other includes Medicaid, self-pay, Indian Health Services, CHAMPUS/TRICARE, and other government sources.
In the second logistic regression model, which explored physical activity during the third trimester of pregnancy (Nagelkerke R2 = .027; P < .001), prepregnancy BMI (P = .001) was the only variable significantly associated with meeting the guidelines (Table 2). Women with a prepregnancy BMI classified as underweight/normal weight (AOR = 1.70; 95% CI, 1.27-2.28) had a greater likelihood of meeting physical activity guidelines than women with a prepregnancy BMI classified as obese. We observed no significant interactions between the intra- and interpersonal variables in the first or second regression model.
Discussion
Only 14.6% of women with a recent live birth in Alabama and Rhode Island met physical activity guidelines before pregnancy, and the proportion dropped to 8.8% during the last trimester of pregnancy. Multivariable regression analyses revealed that race, ethnicity, prepregnancy BMI, and state of residence were all significantly associated with meeting physical activity guidelines before pregnancy. However, prepregnancy BMI was the only variable associated with meeting the guidelines during pregnancy. Findings from this study may help health care providers, public health professionals, and health education specialists develop strategies to encourage and increase physical activity engagement among pregnant women before and during pregnancy.
Our findings are similar to previous epidemiologic studies, which found that although most pregnant women are informed about the benefits of physical activity, only a small proportion meet the guidelines.12,13,21 The prevalence of physical activity also dramatically decreases in the last 3 months of pregnancy, similar to the findings in our study.13,15,21,25,26 Analyses of previous waves of PRAMS data have consistently shown low compliance with physical activity guidelines during pregnancy. In a study using 2008 PRAMS data from North Carolina and Colorado, only 9% of pregnant women met physical activity guidelines, and 2012-2015 PRAMS data from Colorado showed that only 10.2% of pregnant women met the guidelines. 13 Findings in this stream of research emphasize the need to encourage women to engage in physical activity before and during pregnancy, which may be achieved through education and awareness programs that reach women early in pregnancy and those in the preconception stage. Education from professionals such as health care providers and health education specialists, as well as support for physical activity, should be incorporated into programming for women of childbearing age. The American College of Obstetricians and Gynecologists recommends the use of motivational counseling strategies, such as the 5 A’s (ask, advise, assess, assist, and arrange), for physical activity counseling with pregnant women. 1 Future research should explore the extent to which health care providers use motivational counseling strategies to encourage physical activity in their perinatal patients.
Before pregnancy, race and ethnicity were both associated with meeting physical activity guidelines. Previous research also showed that non-Hispanic White women were more likely than Hispanic women and non-Hispanic Black/African American women to meet physical activity guidelines before pregnancy.16,18,19 Findings from the current study and previous studies support the need for community-based programs that are culturally tailored to encourage physical activity among Black/African American and Hispanic women, especially before becoming pregnant. 16 In our study, we could not differentiate between occupational and nonoccupational physical activity because of the PRAMS physical activity item. Previous research using other national data sources (eg, the Behavioral Risk Factor Surveillance System) showed that Hispanic women were significantly less likely than non-Hispanic White women to meet aerobic physical activity guidelines for nonoccupational physical activity. 27 Additional research is needed to explore barriers to physical activity in these groups, which can help inform the development of future public health initiatives to increase physical activity among these women. From a preconception perspective, public health professionals and health care providers should promote and track clients’ physical activity before pregnancy and share and discuss these records with their patients, because research has shown that physical activity levels decrease during pregnancy for all women.21,26
Prepregnancy BMI was associated with meeting physical activity guidelines before and during pregnancy. In our study, women with a prepregnancy BMI classified as underweight or normal weight were more likely than women with a BMI classified as obese to meet physical activity guidelines before and during pregnancy. Prior research also showed associations between BMI and physical activity among pregnant women.13,20,21 The most recent PRAMS analysis conducted prior to this study showed the same associations with BMI and physical activity before and during pregnancy and demonstrated a continuation of this trend over time. 13 Health education specialists, public health professionals, and health care providers working with women of childbearing age who are overweight or obese should focus on providing counseling and education sessions before and during pregnancy to encourage physical activity.17,28 Efforts to address physical activity in these groups should focus on developing counseling and education-based programs to guide women toward resources and appropriate types of physical activity, especially during pregnancy. 17 Additionally, identifying and offering access to physical activity programs and helping women enroll in such programs before and during pregnancy may help address the low rates of physical activity.
Health care providers may choose to use evidence-based approaches such as motivational interviewing or the 5 A’s to encourage pregnant women to incorporate physical activity into their routine during pregnancy.1,13 Health care providers should focus on improving the weight status and physical activity of pregnant patients before pregnancy because previous studies show that improving weight status before pregnancy may help improve physical activity during pregnancy. 13 Additionally, previous research showed that about one-third of pregnant women report not receiving advice about the importance of physical activity from their health care providers, which suggests that efforts to increase physical activity should emphasize the importance of counseling patients about it.2,21
Strengths and Limitations
This study had several strengths and limitations. One strength was the use of PRAMS data, which increased the internal and external validity of the study findings. A second strength was the ability to explore relationships before and during pregnancy. Limitations were primarily due to the use of cross-sectional secondary data. First, the self-report nature of the PRAMS survey imposed limitations, including the threat of response biases, such as social desirability, that may have influenced our findings. Second, engagement in physical activity could have been incorrectly reported by women in the study. Women were asked to recall their physical activity before becoming pregnant and during the last trimester of pregnancy when they received the PRAMS questionnaire 2 to 6 months after birth. Third, the PRAMS physical activity items did not specify exercise intensity (ie, moderate or vigorous), which limited how meeting physical activity guidelines was defined in this study. Fourth, women were asked to indicate their engagement with physical activity only during the third trimester, so the analysis could not account for any changes in physical activity that may have occurred throughout the pregnancy. Fifth, for some variables, groups were combined to meet statistical assumptions for analysis, resulting in the inability to differentiate among some of the demographic subgroups, such as underweight and normal weight and various sources of health insurance. Sixth, the R2 values for both regression models were low, indicating that additional research is warranted to further explore factors associated with physical activity before and during pregnancy that were not accounted for in the present study. Lastly, this study could not account for other potential confounding factors, such as state-level influences (eg, physical activity promotion programs), which may affect physical activity patterns across the PRAMS waves analyzed in this study.
Conclusion
This study adds to the current literature about physical activity and factors associated with meeting the physical activity guidelines before and during pregnancy using population-level data from PRAMS. The study findings indicate that some groups of women may be less likely than other groups to engage in physical activity before and during pregnancy. Pregnancy has been suggested as an ideal time to encourage behavior changes in physical activity, because women are under more frequent medical care than they are before pregnancy and may have increased motivation to make lifestyle changes that may affect their health and the baby’s health. 1 Our findings can be used by health care providers, health education specialists, and public health professionals to identify groups of women on which to focus public health efforts to meet physical activity recommendations before and during pregnancy.
Supplemental Material
sj-docx-1-phr-10.1177_00333549261438079 – Supplemental material for Factors Associated With Physical Activity Before and During Pregnancy: Analysis of 2016-2019 PRAMS Data
Supplemental material, sj-docx-1-phr-10.1177_00333549261438079 for Factors Associated With Physical Activity Before and During Pregnancy: Analysis of 2016-2019 PRAMS Data by Nuha H. Abutalib, Amanda H. Wilkerson, Nayoung Kim, Beth H. Chaney, Taylor Zingg and Maria Hernandez-Reif in Public Health Reports®
Footnotes
Acknowledgements
The authors thank the PRAMS Working Group, which includes the PRAMS Team, Division of Reproductive Health, CDC, and the following PRAMS sites for their role in conducting surveillance and allowing the use of their data: PRAMS Alabama, PRAMS Rhode Island.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online. The authors have provided these supplemental materials to give readers additional information about their work. These materials have not been edited or formatted by Public Health Reports’s scientific editors and, thus, may not conform to the guidelines of the AMA Manual of Style, 11th Edition.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.