
Abstract
Objective:
Little is known about risk factors associated with COVID-19 infection among Arab American people. We aimed to understand the predictors of receiving a positive COVID-19 test result and being admitted to the hospital for COVID-19 among Arab American adults using data from a hospital near an Arab ethnic enclave.
Methods:
We used electronic medical record data for Arab American adults aged ≥18 years from March 1, 2020, through January 31, 2021, at Sharp Grossmont Hospital in La Mesa, California. The primary outcomes were receiving a positive COVID-19 test result and being admitted to the hospital for COVID-19. We ran logistic regression models with individual- and population-level risk factors to determine the odds of each primary outcome.
Results:
A total of 2744 Arab American adults were tested for COVID-19, of whom 783 (28.5%) had a positive test result. In the fully adjusted model, women had lower odds of receiving a positive test result than men (adjusted odds ratio [aOR] = 0.77; 95% CI, 0.64-0.92), and adults living in high-poverty areas had higher odds of receiving a positive test result than adults in lower-poverty areas (aOR = 1.25; 95% CI, 1.04-1.51). Of the 783 Arab American adults with data on admission, 131 (16.7%) were admitted. For every 1-unit increase in the Charlson Comorbidity Index, the odds of admission increased by 66% (aOR = 1.66; 95% CI, 1.36-2.04).
Conclusion:
The risk of receiving a positive test result for COVID-19 was higher among Arab American adults living in high-poverty areas than in lower-poverty areas. The risk of admission was directly related to overall health status. Future work should aim to understand the barriers to prevention and testing in this population.
Population-level and individual-level social factors confer risk for COVID-19 infection among racially and ethnically minoritized populations.1-3 In particular, forces such as population-level poverty and deprivation have played a prominent role in shaping the disproportionate burden of COVID-19–related infection and mortality among communities of color in the United States.3-5 While risk factors for infection and severity of COVID-19 have been examined for several racial and ethnic minority groups in the United States,6-12 the literature on the risk factors associated with COVID-19 infection among Arab American people is limited.
The estimated >3.5 million Arab American people who live in the United States have ethnic, cultural, or linguistic origins in the Middle East and North Africa 13 and a diversity in health needs.14,15 Several population-level and individual-level factors may put Arab American people at increased risk of COVID-19 infection (and other infectious diseases), including household size, socioeconomic status, health prevention behaviors, and social isolation. 16 Prior work examining disparities in testing, admission, and mortality showed that Arab American people had higher odds of receiving a positive test result for COVID-19 but lower odds of admission or mortality compared with other communities of color. 17 Other racially and ethnically minoritized populations in California have also been found to have an elevated risk of COVID-19 admission and mortality when compared with non-Hispanic White people. 18 Risk factors such as living in high-poverty areas and individual health status influenced COVID-19 admission and mortality in racially and ethnically minoritized populations. 18 We hypothesized that Arab American people have similar population-level and individual-level risk factors that influence their risk of receiving a positive COVID-19 test result and being admitted to a hospital for COVID-19 infection.
Most Arab American people in the United States live in California, where they account for about 2% of the adult population. 19 In California, there are known ethnic enclaves with a high density of Arab American residents. One of the largest such ethnic enclaves is in the East County region of San Diego. The 3 cities that compose East County (El Cajon, La Mesa, and Santee) have large Arab American populations. 20 Ethnic enclaves provide unique opportunities to understand the population-level and individual-level risk factors that put minoritized groups at risk of morbidity or mortality from particular diseases. 21 Understanding the risk factors for receiving a positive COVID-19 test result and being admitted to the hospital for COVID-19 infection among Arab American adults could lead to more targeted interventions that could improve the overall health of this community and other Arab American communities across the United States.
We aimed to understand the predictors of receiving a positive COVID-19 test result and being admitted to the hospital for COVID-19 among Arab American adults in Southern California using data from a hospital near an Arab ethnic enclave. The objective of this study was to elucidate the individual-level and population-level risk factors that put Arab American adults at elevated risk for COVID-19 infection.
Methods
Residents of the Arab American enclave in East County generally seek and receive acute care medical services from Sharp Grossmont Hospital in La Mesa. The data for this analysis came from a larger retrospective study examining differences in testing, admissions, and mortality among racial and ethnic minority groups at Sharp Grossmont Hospital in La Mesa using electronic medical record (EMR) data from March 1, 2020, through January 31, 2021. Identifying Arab American adults from EMR data or public health datasets is hindered because of their classification as White by the federal government.14,22 We identified Arab American adults in 1 of 3 ways commonly used by researchers studying Arab American health.23-25 First, we considered individuals to be Arab American if place of birth recorded in the EMR was determined to be 1 of 22 Arab League countries. Second, individuals who indicated a preferred language of Arabic were denoted as Arab American. Third, we included individuals whose last name was matched to a prevalidated surname list 26 for Arab ethnicity. The Sharp HealthCare Institutional Review Board reviewed this study and considered it exempt.
The primary outcomes of interest for this analysis were receipt of a positive COVID-19 test result and admission to Sharp Grossmont Hospital because of COVID-19. COVID-19 test results were noted in the EMR with details on the date, location, and outcome of each test. Patients were noted to have been admitted to the hospital for COVID-19 if they received inpatient care and if their positive test result occurred before or at the same time as their admission date. Data on characteristics extracted from the EMR included age (18-29, 30-49, 50-69, ≥70 years), sex (male, female), smoking status (ever smoker, never smoker), marital status (married, single/widowed/separated/divorced), health insurance type (private, Medi-Cal, other public/other), and diagnosis with comorbidities included in the Charlson Comorbidity Index (CCI) (obesity, chronic pulmonary disease, diabetes with and without complications, hypertension). We used zip code to assess whether the individual came from a zip code in which >12% of families live in poverty (high-poverty areas), as determined by using 2019 American Community Survey data. 27 We considered individuals who came from a zip code where ≤12% of families live in poverty to live in lower-poverty areas.
We calculated summary statistics for all covariates stratified by each outcome and compared them by using Pearson χ2 tests, with P < .05 considered significant. We ran logistic regression models to determine the odds of receiving a positive test result for COVID-19 and being admitted to the hospital for COVID-19. We ran univariate analyses for each covariate, and we included all covariates in a larger adjusted model for each outcome. We ran all analyses using SAS version 9.4 (SAS Institute Inc).
Results
Testing
A total of 2744 Arab American adults aged ≥18 years were tested for COVID-19 during the study period at Sharp Grossmont Hospital, 783 (28.5%) of whom received a positive test result (Table 1). When compared with people who received a negative test result, a higher percentage of those who received a positive test result were younger (12.4% vs 20.9% were aged ≥70 years; P < .001), living in a high-poverty area (62.2% vs 57.1%; P = .015), and married (64.4% vs 59.7%; P = .02). Compared with adults who received a negative test result for COVID-19, adults who received a positive test result for COVID-19 had a lower prevalence of ever smoking (18.1% vs 24.7%; P < .001) or having chronic pulmonary disease (5.6% vs 8.9%; P = .004) and a lower CCI (1.9 vs 2.9; P < .001). In the fully adjusted model, women had lower odds of receiving a positive test result for COVID-19 than men (adjusted odds ratio [aOR] = 0.77; 95% CI, 0.64-0.92) (Table 2). Adults living in high-poverty areas had higher odds of receiving a positive test result than adults living in lower-poverty areas (aOR = 1.25; 95% CI, 1.04-1.51). With every 1-unit increase in CCI, the odds of receiving a positive test result decreased by 17% (aOR = 0.83; 95% CI, 0.77-0.89).
Characteristics of Arab American adults who were tested for COVID-19 or had admission data for COVID-19, Sharp Grossmont Hospital, La Mesa, California, March 1, 2020, through January 31, 2021 a
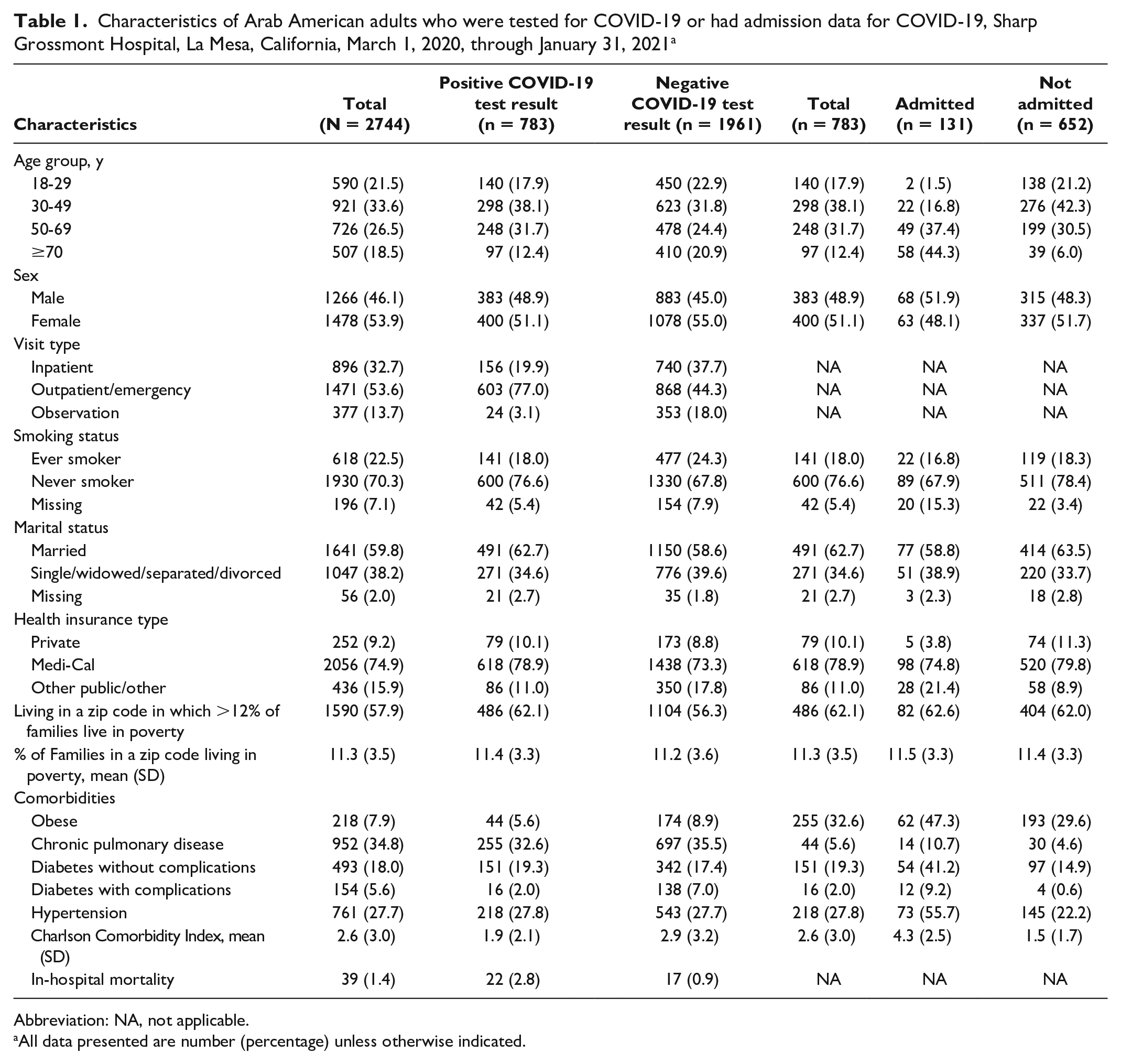
Abbreviation: NA, not applicable.
All data presented are number (percentage) unless otherwise indicated.
Bivariate and adjusted logistic regression models for receiving a positive test result (vs negative test result) for COVID-19 and being admitted to the hospital for COVID-19 among Arab American adults, Sharp Grossmont Hospital, La Mesa, California, March 1, 2020, to January 31, 2021
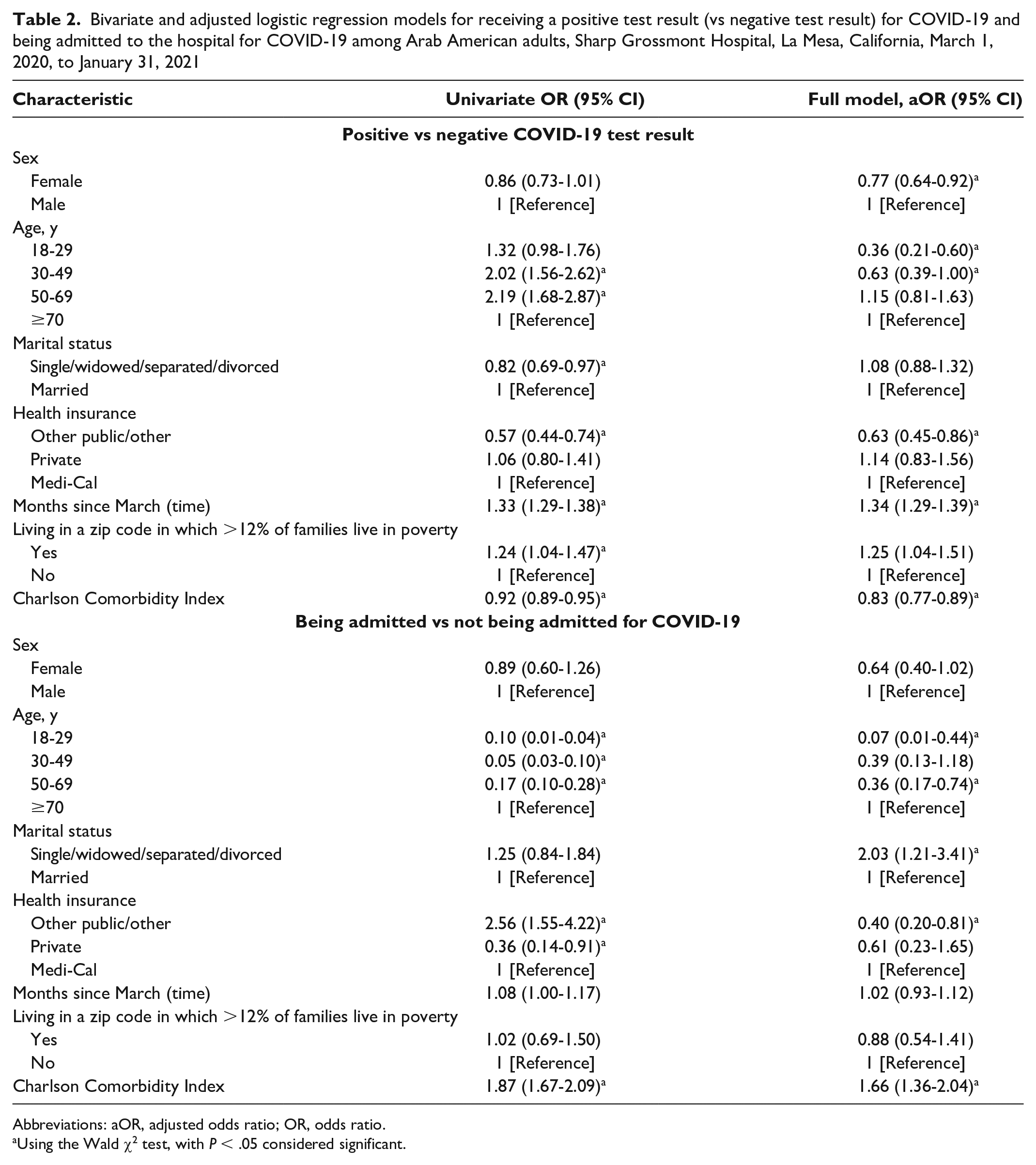
Abbreviations: aOR, adjusted odds ratio; OR, odds ratio.
Using the Wald χ2 test, with P < .05 considered significant.
Admission
A total of 783 Arab American adults had data on admission for COVID-19, of whom 131 (16.7%) were admitted (Table 1). Compared with adults who were not admitted, a higher percentage of adults who were admitted were aged ≥70 years (44.3% vs 6.0%; P < .001) and had a poorer health profile with a higher prevalence of obesity (47.7% vs 36.1%; P = .015), chronic pulmonary disease (10.7% vs 4.6%; P = .006), diabetes without complications (41.2% vs 14.9%; P < .001), and hypertension (55.7% vs 22.2%; P < .001). In the fully adjusted model, adults who were not married had higher odds of admission than those who were married (aOR = 2.03; 95% CI, 1.21-3.41) (Table 2). In addition, for every 1-unit increase in CCI, the odds of admission increased by 66% (aOR = 1.66; 95% CI, 1.36-2.04).
Discussion
By using data from EMRs from a hospital near an Arab ethnic enclave, we showed that the risk of receiving a positive test result for COVID-19 was higher among Arab American adults living in high-poverty areas and lower among Arab American adults with better overall health. Risk of hospital admission in this group was directly related to overall health status, with adults who had more comorbidities experiencing elevated risk of hospital admission. Population-level poverty prevalence was not associated with hospital admission, suggesting that the acute impact of living conditions may be associated with the risks of disease transmission but not with morbidity, the latter being driven principally by underlying overall health.
The patterns observed for admission because of COVID-19 among Arab American adults are similar to patterns found among Hispanic/Latinx and non-Hispanic Black populations in previous studies.7,8,12 Individuals who were healthier (ie, had lower CCI) had higher odds of receiving a positive test result for COVID-19, suggesting that they might be at higher risk for exposure because of continued employment or a lack of perceived susceptibility. In addition to overall health status, marriage was protective against admission for COVID-19 in our sample. A study among non-Hispanic Black people had similar findings. 10 Marriage has been found to have positive influences on health and wellness.28,29 The proportion of Arab American people who are married is higher than the proportion in the general US population 19 ; marriage may be a form of social support that protects against a range of health conditions in Arab American populations.
Limitations
The implications of this analysis are constrained by the limitations in the methodology. First, we used a validated Arab surname algorithm to identify Arab American patients from the EMR but cannot be sure that we captured all Arab American patients in our sample. Because of the ways in which Arab American people are categorized by race and ethnicity on forms, there is no standardized way to ensure all Arab American people are captured from EMRs or other health datasets. Second, only Arab American people who received a COVID-19 test at Sharp Grossmont Hospital were considered, and results may not be generalizable to people without health insurance or people who were not tested at a hospital. Because most Arab American people included in the analysis had Medi-Cal, California’s version of Medicaid, we feel comfortable generalizing our results to those at all socioeconomic levels. Third, patterns for infection and severity could be influenced by immigration and acculturation variables, both of which were not available from the EMR. For example, work with other immigrant groups suggests that time since immigration, English language proficiency, and other acculturation variables all influence morbidity and mortality among immigration populations.30,31
Conclusions
To our knowledge, this is the first analysis to examine predictors for receiving a positive test result for COVID-19 and being admitted to the hospital for COVID-19 infection among Arab American people in Southern California. Future work should aim to understand the barriers to prevention and testing in this population and the protective factors present in Arab American ethnic enclaves that may reduce the need for admission. In particular, more attention should be paid to the positive community characteristics that may influence disease incidence in this minoritized group.
Footnotes
Acknowledgements
The authors thank Jennifer Sheppard, MBA, and James Curtis, Sharp HealthCare clinical analysts, for their contributions in extracting and validating the datasets used for analysis.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: K.L.G. is an employee at Sharp HealthCare Center for Research. R.A. is a member of the medical staff at Sharp Grossmont Hospital.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.