
Abstract
Objectives
The health profile of Arab American mothers and infants may differ from that of non–Arab American mothers and infants in the United States as a result of social stigma experienced in the historical and current sociopolitical climate. The objective of our study was to compare maternal health behaviors, maternal health outcomes, and infant health outcomes of Arab American mothers and non-Hispanic white mothers in Massachusetts and to assess the role of nativity as an effect modifier.
Methods
Using data from Massachusetts birth certificates (2012-2016), we conducted adjusted logistic and linear regression models for maternal health behaviors, maternal health outcomes, and infant health outcomes. We used Arab ethnicity as the exposure of interest and nativity as an effect modifier.
Results
Arab American mothers had higher odds than non-Hispanic white mothers of initiating breastfeeding (adjusted odds ratio [aOR] = 2.61; 95% CI, 2.39-2.86), giving birth to small-for-gestational-age infants (aOR = 1.28; 95% CI, 1.18-1.39), and having gestational diabetes (aOR = 1.31; 95% CI, 1.20-1.44). Among Arab American mothers, non–US-born mothers had higher odds than US-born mothers of having gestational diabetes (aOR = 1.80; 95% CI, 1.33-2.44) and lower odds of initiating prenatal care in the first trimester (aOR = 0.41; 95% CI, 0.33-0.50). In linear regression models, infants born to non–US-born Arab American mothers weighed 42.1 g (95% CI, −75.8 to −8.4 g) less than infants born to US-born Arab American mothers.
Conclusion
Although Arab American mothers engage in positive health behaviors, non–US-born mothers had poorer maternal health outcomes and access to prenatal care than US-born mothers, suggesting the need for targeted interventions for non–US-born Arab American mothers.
The health profile of Arab American mothers and infants is different from that of non–Arab American mothers and infants. Arab Americans have faced stress and stigma in the United States, both historically and currently. Arab Americans are disproportionately exposed to psychosocial stressors, such as hate crimes 1 and discrimination. 2,3 These stressors can have potent health effects, particularly for mothers and their infants. Studies on the effect of stress and discrimination found evidence in California of increased risk of preterm birth after 9/11 among Arab American mothers, 4 but this result was not replicated in Michigan. 5 Other studies of Arab American mothers found that their infants had lower risks of preterm birth, low birth weight, and infant mortality than non–Arab American mothers in Michigan. 6 -8 Father’s ancestry was also found to affect birth outcomes, with infants born to Arab American mothers and fathers having lower risk of preterm birth and low birth weight than infants born to non–Arab American mothers and fathers. 9 Nevertheless, this area of research is understudied, and little is known about how Arab ethnicity influences a wide range of maternal and infant health outcomes. Furthermore, consensus is limited on how to isolate data on Arab Americans in large administrative databases. Although some research has used surname algorithms, 4,5 other work relies on self-reported ethnicity or place of birth, when available. 6 -8
Nativity, or place of birth, may play an important role in the health of Arab Americans. Maternal health behaviors and infant health outcomes differ between immigrant and nonimmigrant populations in the United States. 10 -16 Moreover, first-generation immigrant mothers and their infants tend to have better health behaviors and outcomes than second- and third-generation mothers and infants in the same racial/ethnic group. 17,18 Immigrant mothers are more likely than their US-born counterparts to start and continue breastfeeding 10,11,19 and are less likely to smoke 10,12,13 or drink alcohol 12,13 during pregnancy. These benefits also extend to their offspring, so that infants born to immigrant mothers have a higher birth weight and lower infant mortality rates than infants of US-born mothers in the same racial/ethnic group. 15,16,18,19
Most research on maternal and child health of Arab Americans has been conducted in Dearborn, Michigan 20 (the city with the largest number of Arab Americans in the United States), 21 and California (the state with the largest number of Arab Americans in the United States). 4 Our understanding of maternal and infant health of Arab Americans is limited outside these 2 areas. The population of Arab immigrants in the United States has grown in recent years, mainly because of unstable conditions in the Middle East and North Africa. Massachusetts was one of the early hubs for Syrian, Lebanese, and other Arab immigrants during the late 1800s and early 1900s. 22 Early Arab immigrants in Massachusetts primarily worked in the garment industry in Boston; after World War II, these groups relocated to suburbs such as West Roxbury, Worcester, and Roslindale. 22 Massachusetts has one of the largest Arab populations in the United States (population size: 195 450, 2.8% of the adult population 21 ); however, little is known about the health of these Arab Americans. Moreover, little research has assessed the role that nativity—US-born versus non–US-born—plays in the relationship between Arab ethnicity and maternal and infant health outcomes.
Using unique birth certificate data collected by Massachusetts, we aimed to (1) compare maternal health behaviors and outcomes and infant health outcomes of Arab American and non-Hispanic white mothers and their infants born in Massachusetts during 2012-2016 and (2) understand the influence of nativity status on the relationship between Arab ethnicity and maternal health behaviors and outcomes and infant health outcomes.
Methods
The Massachusetts Standard Certificate of Live Birth is composed of a parent worksheet and a hospital worksheet and contains legal and sociodemographic information, as well as information on prenatal care, labor and delivery, neonatal outcomes, and discharge conditions and procedures. We considered eligible for our study all women who delivered a live birth in Massachusetts from January 1, 2012, through December 31, 2016, who provided data on place of birth and/or ethnicity, and whose infants had plausible birth weights. 23 The only exclusion criteria were not having information on place of birth or having infants with an implausible birth weight. The Boston College Institutional Review Board reviewed the study and considered it exempt.
Ethnicity, Nativity, and Race Measures
Massachusetts provides a unique opportunity to understand maternal and infant health among Arab American mothers because the state collects detailed information on ethnicity through birth certificates. 24 Birth certificates offer 39 options for ethnicity, collected independently of race, including an option for Middle Eastern ethnicity. We categorized mothers as Arab if they indicated Middle Eastern as their answer to the following standard question on the birth certificate: “Please mark the one category that best describes your ancestry or ethnic heritage.” We also categorized mothers as Arab if they indicated their place of birth as 1 of 22 Arab League countries 25 in response to the following standard question: “In what state or country were you born?” We categorized mothers who indicated place of birth as the continental United States, Alaska, or Hawaii as US-born and all other mothers as non–US-born. The birth certificate also asks mothers about their ethnicity and race with the following standard 2-step question: “Are you Hispanic/Latino/Spanish?” and “What is your race?” We categorized as non-Hispanic white mothers who indicated white and non-Hispanic.
Maternal Health Behaviors
We considered the following maternal health behaviors in this analysis: initiation of prenatal care in the first trimester, breastfeeding initiation, alcohol consumption in the 3 months before and during pregnancy, and smoking cigarettes in the 3 months before and during pregnancy. To assess prenatal care initiation, mothers were asked: “How many weeks or months pregnant were you when you had your first visit for prenatal care?” The weeks or months within the first 3 months counted as the first trimester. We determined breastfeeding initiation from the discharge portion of the hospital worksheet. The certifier of the worksheet responds to the following yes/no question: “Is mother breastfeeding?” 10 Alcohol consumption was assessed by the following question on the parent worksheet: “Did you drink any alcohol in the three months before this pregnancy and anytime during the pregnancy?” The parents’ worksheet asks mothers to report the number of cigarettes or packs of cigarettes smoked on an average day during the 3 months before pregnancy and during each trimester. 10 If a mother answered yes to the alcohol question or indicated she had smoked at least 1 cigarette, we categorized her as having engaged in that behavior.
Maternal Health Outcomes
The hospital worksheet records risk factors during pregnancy, including gestational diabetes, indicating that glucose intolerance was diagnosed in the pregnancy.
Infant Health Outcomes
Infant health outcomes, determined from birth weight and gestational age recorded on the hospital worksheet, included, on the basis of previous research, 26 the following: birth weight (in grams), preterm birth (<37 weeks), low birth weight (<2500 g), small for gestational age (<10th percentile for gestational age and sex), and large for gestational age (>90th percentile for gestational age and sex). 27
Independent Variables
Mothers self-reported their age (categorized as <29 or ≥30), educational attainment (categorized as ≤high school diploma or ≥some college), marital status (categorized as married or not married), parity (categorized as first live birth or previous live birth), and plurality (categorized as singleton or multiple). Health insurance status was categorized as private, public, or other health insurance (eg, free care, self-pay, health safety net). We used as a socioeconomic indicator self-reported receipt of assistance during pregnancy from the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC).
Statistical Analysis
We used descriptive statistics to compare mothers categorized as Arab with mothers categorized as non-Hispanic white for all years of data. We built unadjusted and adjusted logistic regression models for each dichotomous outcome, using Arab ethnicity as the exposure of interest. We built adjusted linear regression models for the continuous birth weight variable, with Arab ethnicity as the exposure of interest. Adjusted models included all sociodemographic variables, including age, education, marital status, parity, plurality, health insurance status, and WIC status. Models examining an infant health outcome also included infant sex and gestational age.
We then introduced an interaction term to the adjusted regression models (nativity × Arab ethnicity) to examine the interaction of nativity status and Arab ethnicity on each dichotomous outcome (initiation of prenatal care in first trimester, breastfeeding initiation, alcohol consumption in the 3 months before and during pregnancy, smoking cigarettes in the 3 months before and during pregnancy, gestational diabetes, preterm birth, low birth weight, small for gestational age, and large for gestational age). We conducted all analyses using SAS version 9.4 (SAS Institute Inc).
Results
Of 352 467 births during 2012-2016 in Massachusetts, 8901 (2.5%) were among Arab American mothers and 343 566 (97.5%) were among non–Arab American mothers. Of these 352 467 births, we identified and included in our analysis 8204 Arab American mothers and 199 254 non-Hispanic white mothers who had data on all independent variables of interest. Arab American mothers and non-Hispanic white mothers were similar only in plurality (Table 1). Compared with non-Hispanic white mothers, Arab American mothers were younger (60.5% vs 64.5% aged ≥30; P < .001), less educated (25.6% vs 16.9% had ≤high school diploma; P < .001), and more likely to be married at the infant’s birth (94.0% vs 73.9%; P < .001). A smaller percentage of Arab American mothers than non-Hispanic white mothers were born in the United States (15.2% vs 91.1%; P < .001).
Distribution of sociodemographic and outcome variables by Arab ethnicity for mothers represented in state birth certificate data, Massachusetts, 2012-2016 a
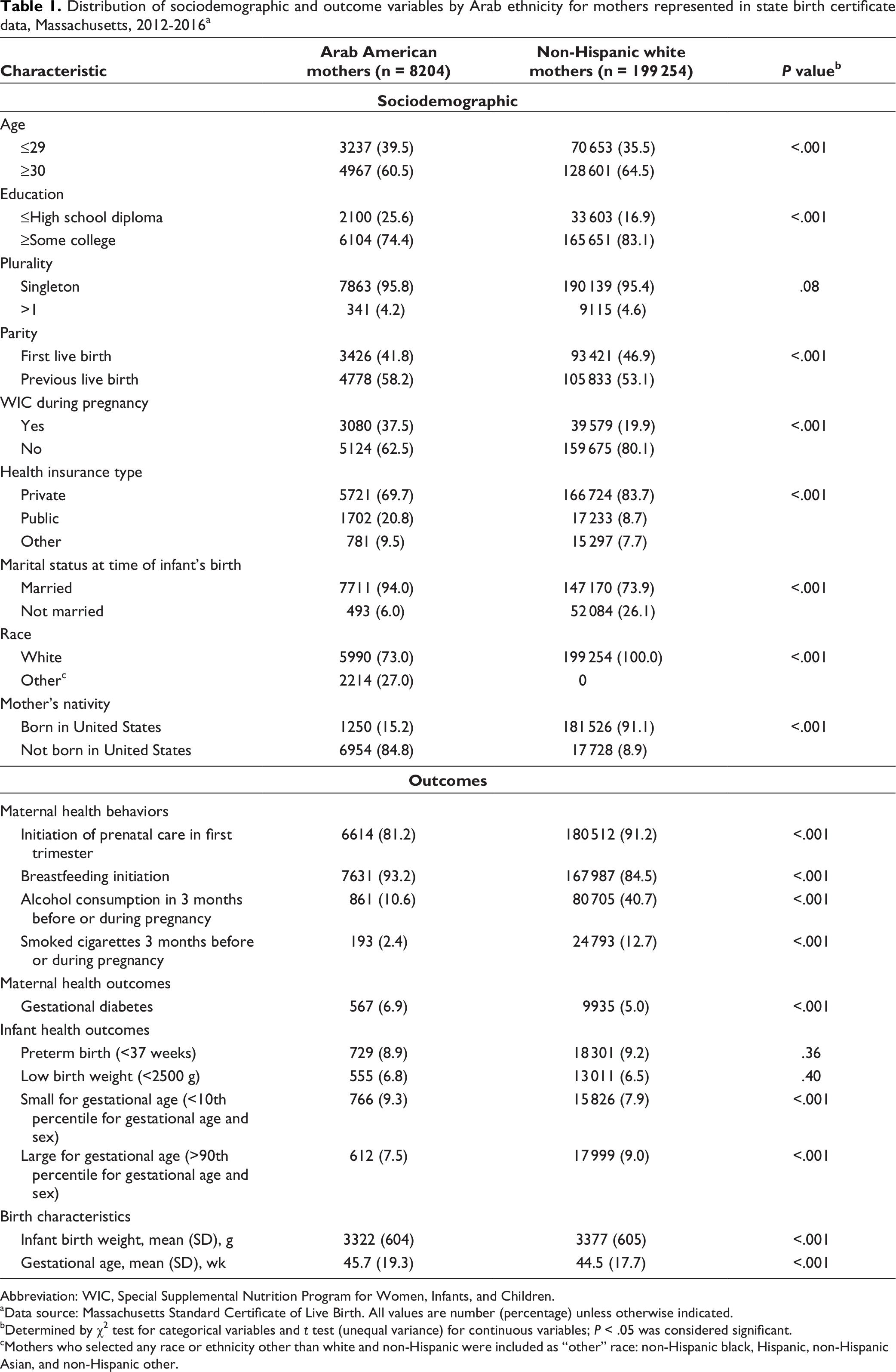
Abbreviation: WIC, Special Supplemental Nutrition Program for Women, Infants, and Children.
aData source: Massachusetts Standard Certificate of Live Birth. All values are number (percentage) unless otherwise indicated.
bDetermined by χ2 test for categorical variables and t test (unequal variance) for continuous variables; P < .05 was considered significant.
cMothers who selected any race or ethnicity other than white and non-Hispanic were included as “other” race: non-Hispanic black, Hispanic, non-Hispanic Asian, and non-Hispanic other.
Maternal Health Behaviors
A larger percentage of Arab American mothers than non-Hispanic white mothers initiated breastfeeding (93.2% vs 84.5%; P < .001), and a smaller percentage of Arab American mothers than non-Hispanic white mothers smoked cigarettes (2.4% vs 12.7%; P < .001) or drank alcohol before or during pregnancy (10.6% vs 40.7%; P < .001) (Table 1). After we adjusted for sociodemographic characteristics, Arab American mothers had lower odds than non-Hispanic white mothers of initiating prenatal care in the first trimester (adjusted odds ratio [aOR] = 0.42; 95% CI, 0.39-0.44) and higher odds of initiating breastfeeding (aOR = 2.61; 95% CI, 2.39-2.86) (Table 2). Arab American mothers had lower odds than non-Hispanic white mothers of reporting alcohol consumption (aOR = 0.20; 95% CI, 0.18-0.21) or smoking cigarettes (aOR = 0.22; 95% CI, 0.19-0.25) before or during pregnancy.
Odds ratios for maternal health behaviors and health outcomes and infant health outcomes for Arab American mothers compared with non-Hispanic white mothers giving birth and represented in state birth certificate data, Massachusetts, 2012-2016 a
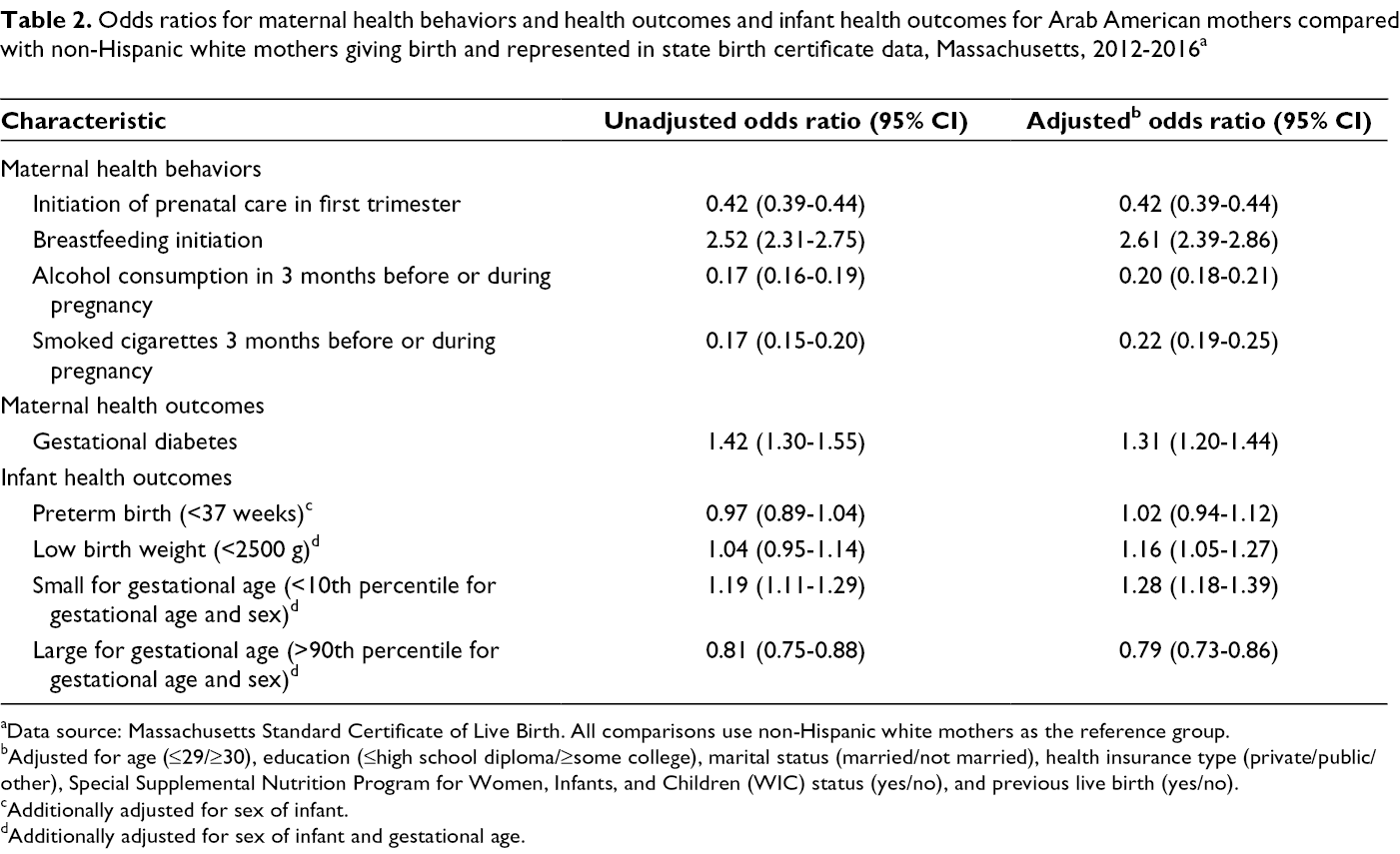
aData source: Massachusetts Standard Certificate of Live Birth. All comparisons use non-Hispanic white mothers as the reference group.
bAdjusted for age (≤29/≥30), education (≤high school diploma/≥some college), marital status (married/not married), health insurance type (private/public/other), Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) status (yes/no), and previous live birth (yes/no).
cAdditionally adjusted for sex of infant.
dAdditionally adjusted for sex of infant and gestational age.
Maternal Health Outcomes
We found a higher prevalence of gestational diabetes among Arab American mothers than among non-Hispanic white mothers (6.9% vs 5.0%; P < .001) (Table 1). Arab American mothers had higher odds of having gestational diabetes (aOR = 1.31; 95% CI, 1.20-1.44) than non-Hispanic white mothers after adjustment (Table 2).
Infant Health Outcomes
Infants born to Arab American and non-Hispanic white mothers had similar gestational age and birth weight (Table 1). Infants born to Arab American mothers and non-Hispanic white mothers had a similar prevalence of preterm birth (8.9% vs 9.2%) and low birth weight (6.8% vs 6.5%). Arab American mothers had infants who weighed 69.8 g (P < .001) less than infants of non-Hispanic white mothers, after we controlled for age, education, marital status, health insurance status, WIC enrollment, infant sex, infant gestational age, plurality, and parity in linear regression models (Table 3). We found no differences in risk for preterm birth in adjusted models. Infants born to Arab American mothers had higher odds than infants born to non-Hispanic white mothers of being born with low birth weight (aOR = 1.16; 95% CI, 1.05-1.27) or being small for gestational age (aOR = 1.28; 95% CI, 1.18-1.39) and lower odds of being large for gestational age (aOR = 0.79; 95% CI, 0.73-0.86) after adjustment (Table 2).
Linear regression results for birth weight (in grams) comparing infants born to Arab American mothers and non-Hispanic white mothers among mothers reporting a birth on state birth certificates, Massachusetts, 2012-2016 a
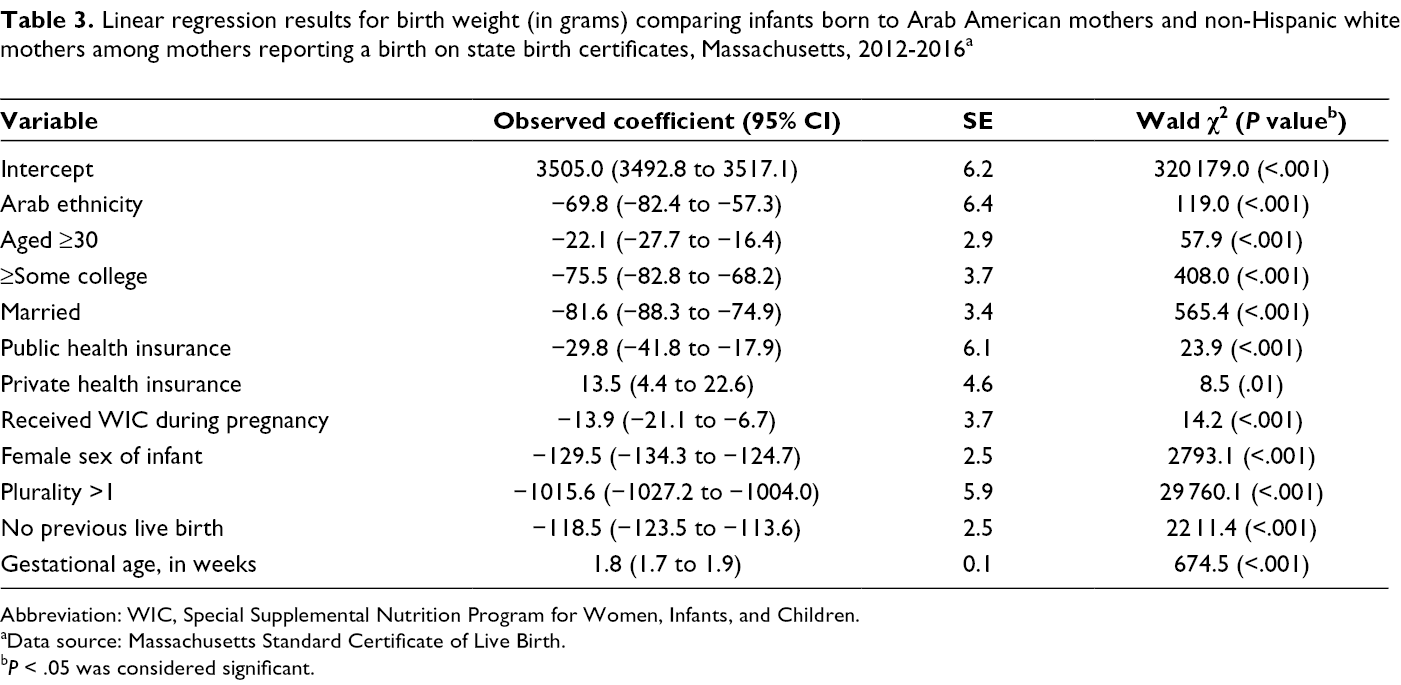
Abbreviation: WIC, Special Supplemental Nutrition Program for Women, Infants, and Children.
aData source: Massachusetts Standard Certificate of Live Birth.
b P < .05 was considered significant.
Nativity Interaction
When compared with US-born Arab American mothers, non–US-born Arab American mothers had lower odds of initiating prenatal care in the first trimester (aOR = 0.41; 95% CI, 0.33-0.50), smoking cigarettes (aOR = 0.15; 95% CI, 0.11-0.21), or drinking alcohol (aOR = 0.11; 95% CI, 0.09-0.12) (Table 4). Non–US-born Arab American mothers had higher odds than US-born Arab American mothers of initiating breastfeeding in the first trimester (aOR = 2.06; 95% CI, 1.65-2.57). Non–US-born Arab American mothers had higher odds than US-born Arab American mothers of having gestational diabetes (aOR = 1.80; 95% CI, 1.33-2.44).
Effect modification results by nativity status for Arab American mothers and non-Hispanic white mothers born in and outside the United States for maternal health behaviors and outcomes and infant health outcomes for mothers reporting a birth on state birth certificates, Massachusetts, 2012-2016 a
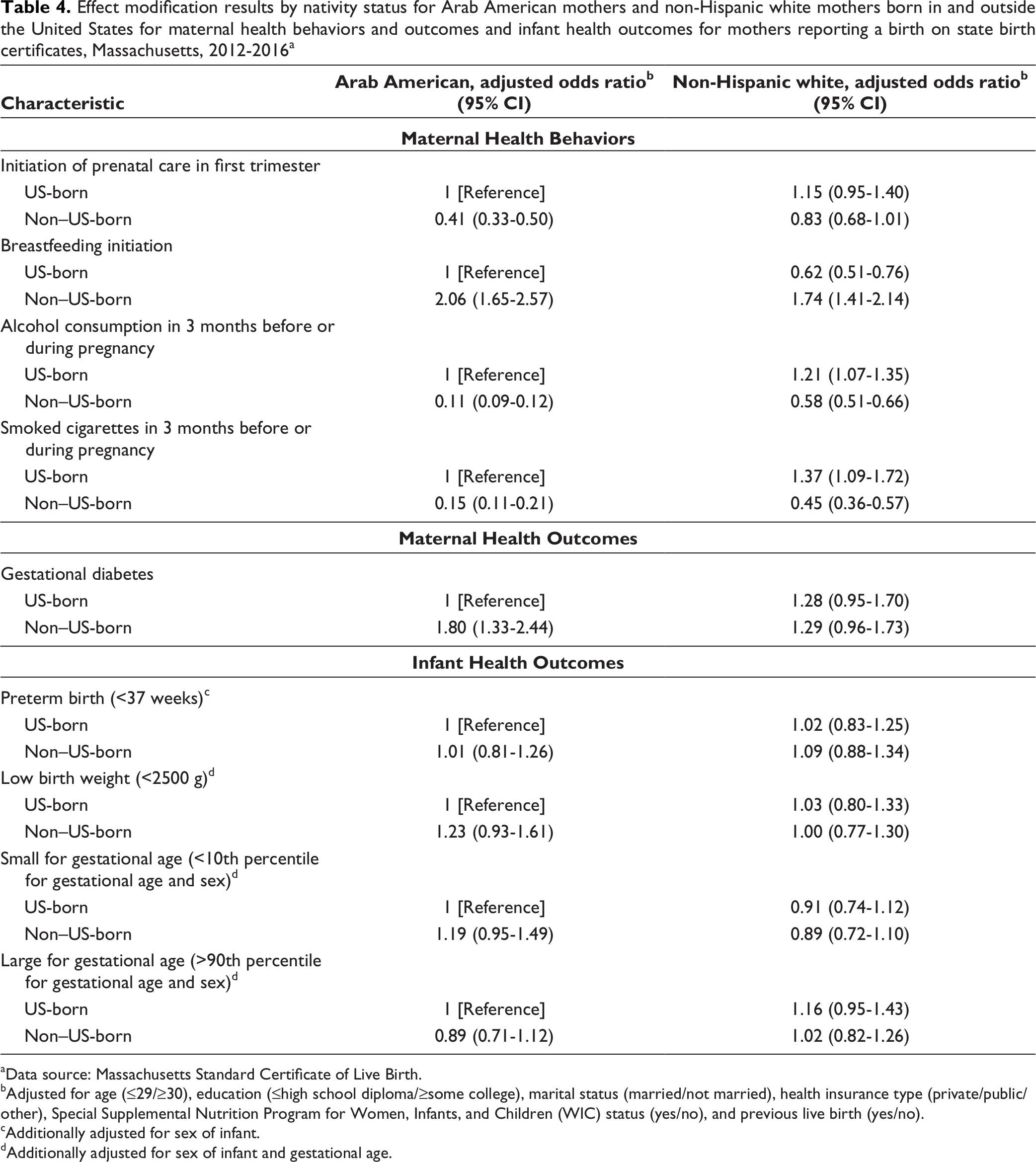
aData source: Massachusetts Standard Certificate of Live Birth.
bAdjusted for age (≤29/≥30), education (≤high school diploma/≥some college), marital status (married/not married), health insurance type (private/public/other), Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) status (yes/no), and previous live birth (yes/no).
cAdditionally adjusted for sex of infant.
dAdditionally adjusted for sex of infant and gestational age.
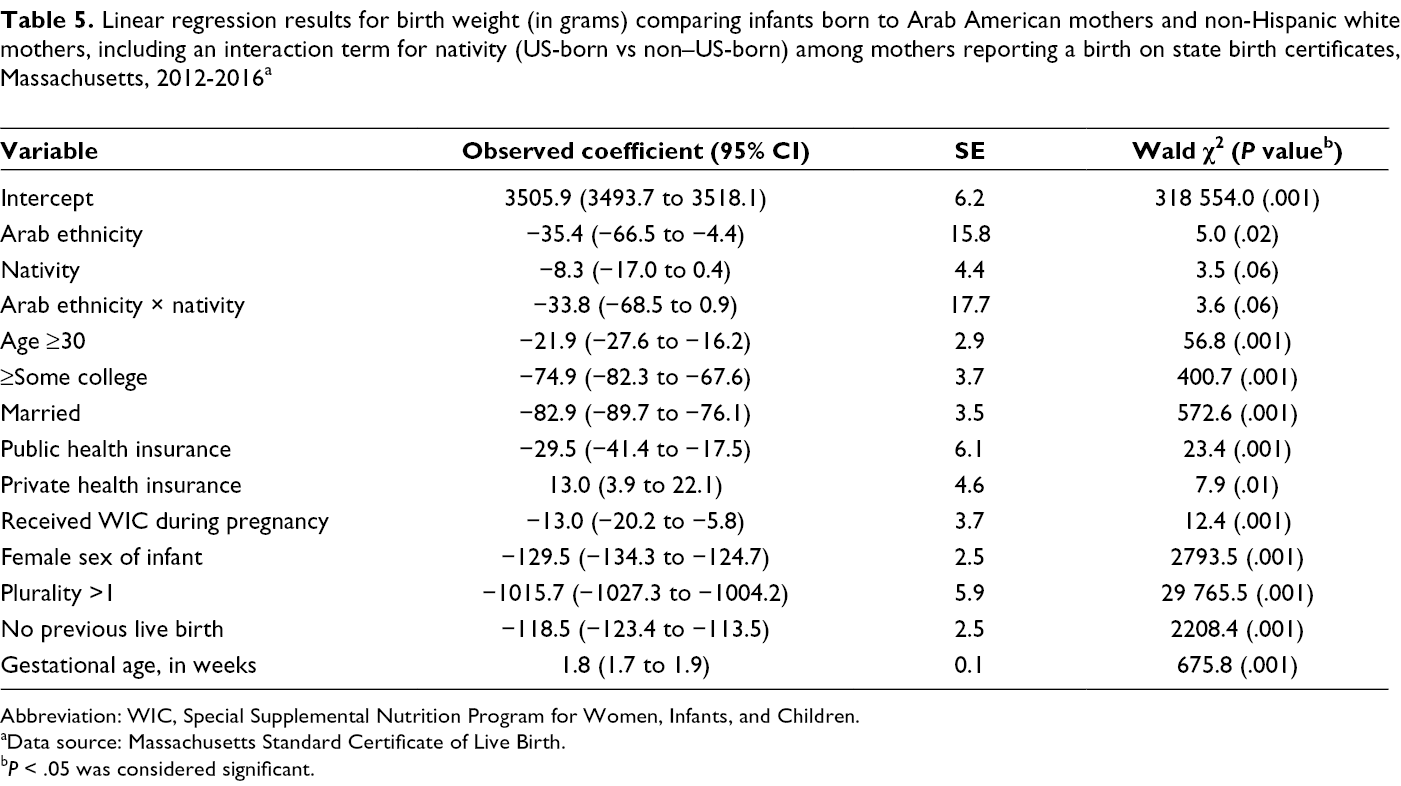
When considering place of birth as an effect modifier, non–US-born and US-born Arab American mothers gave birth to infants with similar health outcomes (Table 4). Infants born to non–US-born Arab American mothers weighed 42.1 g less than infants born to US-born Arab American mothers, 75.9 g less than infants born to non–US-born non-Hispanic white mothers, and 77.5 g less than infants born to US-born non-Hispanic white mothers (Table 5).
Linear regression results for birth weight (in grams) comparing infants born to Arab American mothers and non-Hispanic white mothers, including an interaction term for nativity (US-born vs non–US-born) among mothers reporting a birth on state birth certificates, Massachusetts, 2012-2016 a
Abbreviation: WIC, Special Supplemental Nutrition Program for Women, Infants, and Children.
aData source: Massachusetts Standard Certificate of Live Birth.
b P < .05 was considered significant.
Discussion
Our findings suggest that Arab American mothers in Massachusetts engage in healthy maternal behaviors before and during their pregnancies. Few studies have examined maternal health behaviors among Arab American mothers in the United States. 28 Although we found that Arab American mothers had a slightly lower prevalence of preterm birth than non-Hispanic white mothers in unadjusted analyses, these differences were no longer apparent after adjustment. Arab American mothers in our study had higher odds than non-Hispanic white mothers of giving birth to an infant with low birth weight and an infant who was small for gestational age. These results differ from the results in a study conducted in Michigan, which suggested that infants born to Arab American mothers had a reduced risk of adverse birth outcomes compared with their non–Arab American counterparts. 7,29 Differences in preterm birth and risk of having a small-for-gestational-age infant between Arab American mothers and non–Arab American mothers in Michigan and Massachusetts may be due to differences in education level, marital patterns, and maternal risk behaviors during pregnancy. 30 These differences may have also been caused by differences in methods for identifying Arab Americans in databases. The data in Massachusetts are based on self-report, whereas the data in Michigan rely on surname algorithms. This difference may lead to differences in study populations.
Non–US-born Arab American mothers in our study gave birth to infants who weighed less than the infants of US-born Arab American mothers and non–US-born non-Hispanic white mothers. Our results contrast with the results of other studies of immigrant groups that suggest that first-generation immigrants have the best maternal and infant health outcomes. 31 Two studies conducted among Arab American mothers in Michigan found that non–US-born Arab American mothers had lower odds than US-born Arab American mothers of delivering their infant preterm. 8,30 Some evidence on physical and mental health outcomes suggests that the immigrant health paradox may not hold for Arab immigrants 32 in California. Non–US-born Arab American mothers in Massachusetts may experience stigma and discrimination that non–US-born Arab American mothers in Michigan may not experience because of differences in community ethnic composition and density of Arab immigrant communities (known to be high in parts of Michigan). 21 In addition, recent waves of immigration to the United States from the Middle East have been motivated by an increase in violence and war, potentially leading to immigrants who are unhealthy when arriving in the United States. Finally, the social experiences of Arab American mothers in Massachusetts may be different from the social experiences of Arab American mothers in Michigan. Further study is needed to understand community context and the influence of local environment on infant health outcomes in both Michigan and Massachusetts. Arab American immigrant mothers are a unique immigrant group in the United States, potentially needing targeted interventions.
Arab American mothers in our study had higher odds than non-Hispanic white mothers of having gestational diabetes. Although no studies, to our knowledge, have examined the risk of gestational diabetes among Arab American mothers, studies of Arab mothers in the Middle East suggest a high prevalence of gestational diabetes in this population. 33,34 Mothers in other racial/ethnic minority and immigrant groups in the United States (black, Hispanic, and Asian) have higher odds than non-Hispanic white mothers of developing gestational diabetes. 35 Our results indicate that Arab American mothers should be included with these groups when interventions designed to reduce the risk of developing gestational diabetes are being developed. Consistent with previous studies among other immigrant groups, 36 our study found that nativity status modified the relationship between Arab ethnicity and the odds of gestational diabetes. Non–US-born Arab American mothers had higher odds than US-born Arab American mothers of having gestational diabetes.
Limitations
Our study had several limitations. First, we could not account for time lived in the United States, despite knowing that this factor may influence the risk of preterm birth and health behaviors among non–US-born mothers. 31 Second, we cannot be certain that we captured data on all mothers with Arab ethnicity from the Massachusetts birth certificate data. We relied on self-reporting of Middle Eastern ethnicity or a birthplace in a Middle Eastern country on the birth certificate. Middle Eastern women who did not self-report their ethnicity as Middle Eastern would have been included in the group of non-Hispanic white women in our analysis; this misclassification could have biased our results toward the null. Furthermore, expatriates or non-Arabs born in the Middle East may have been included in the group of Arab American women, which could also have biased our results toward the null. Third, because birth certificates do not ask mothers about their level of acculturation, we could not account for this factor, which is known to influence some health behaviors and outcomes. Furthermore, the birth certificate captures data on a small number of health behaviors and outcomes, limiting the information captured on Arab American mothers. Finally, the birth certificate does not capture data on other potential confounders, such as household income, so we used WIC status during pregnancy and health insurance type as indicators of socioeconomic circumstances.
Conclusion
Despite these limitations, our analysis provides evidence, outside California and Michigan, that Arab American mothers participate in healthy behaviors and that they and their infants experience adverse health outcomes at different rates than do their non-Hispanic white counterparts. Compared with non-Hispanic white mothers, Arab American mothers had lower odds of initiating prenatal care, consuming alcohol, and smoking before and during their pregnancy, but higher odds of initiating breastfeeding. Infants born to Arab American mothers had higher odds than infants born to non-Hispanic white mothers of being born with low birth weight and being small for gestational age but no difference in odds for preterm birth. The higher odds of having gestational diabetes among Arab American mothers than among non-Hispanic white mothers in Massachusetts suggest a need for specialized education and outreach. We also observed that nativity status modified the relationship between Arab ethnicity and prenatal care initiation, breastfeeding initiation, alcohol consumption, smoking, and gestational diabetes, emphasizing the need for targeted education and outreach to Arab immigrants in Massachusetts. Linking data across multiple administrative databases is needed to improve our understanding of the social and structural determinants of health for this population. Future research should also aim to examine differences in determinants of health across settings to better understand the special health needs of Arab Americans in different parts of the country. Because of the complexities of Arab immigration to the United States, more research should be undertaken to understand the relationships between acculturation and maternal health outcomes, especially in nutrition, physical activity, and stress.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no direct funding with respect to the research, authorship, and/or publication of this article.