
Abstract
Objective:
Women who have direct exposure to incarceration or indirect exposure through their partner are at high risk for poor health behaviors and outcomes, which may have lasting impacts on their children. The objectives of this study were to estimate the prevalence of recent incarceration exposure among women with a recent live birth and assess the relationship between incarceration exposure and maternal and child health.
Methods:
We used data from the Pregnancy Risk Assessment Monitoring System (36 states and New York City, 2012-2015; N = 146 329) to estimate the prevalence of women reporting that they or their husband/partner spent time in jail during the 12 months before giving birth. We used multivariable logistic regression to assess associations between incarceration exposure and maternal and infant health conditions.
Results:
The prevalence of incarceration exposure shortly before or during pregnancy was 3.7% (95% CI, 3.6%-3.9%). Women with incarceration exposure had increased odds of prepregnancy hypertension (adjusted odds ratio [aOR] = 1.51; 95% CI, 1.26-1.81), prepregnancy and postpartum depressive symptoms (aOR = 1.95 [95% CI, 1.73-2.19] and 1.49 [95% CI, 1.32-1.67], respectively), and having an infant admitted to the neonatal intensive care unit (aOR = 1.18; 95% CI, 1.04-1.33).
Conclusion:
Because a parent’s incarceration exposure is an adverse childhood experience with the potential to disrupt important developmental periods and have negative impacts on the socioemotional and health outcomes of children, it is critical for researchers and health care providers to better understand its impact on maternal and infant health. Prenatal and postnatal care may provide opportunities to address incarceration-related health risks.
Keywords
The United States has the highest incarceration rate (810 per 100 000 population) 1 and number of incarcerated people (nearly 2.1 million) in the world,1,2 although the rate has begun to decline in recent years. 3 The impacts of incarceration are not restricted to people who are directly in contact with the criminal justice system but are shared by those indirectly in contact.4-13 Incarceration is associated with poor health and well-being of intimate partners,4-6 children,7-9 other family members,10,11 and communities of currently or formerly incarcerated people.12,13 More research is needed to understand the implications of incarceration on perinatal health, especially because incarceration primarily impacts adults of childbearing age 14 and is disruptive to employment, housing, and relationships. 15 Disruptions can affect a parent’s capacity to provide safe, stable, nurturing relationships and environments16,17 to newborns and other children and can foster adversities that may affect children during key developmental stages.
Growing up with a household member who has an incarceration history is considered an adverse childhood experience (ACE). 18 ACEs may facilitate chronic, severe, or prolonged exposure to stress, which, in the absence of protective factors, may disrupt brain circuitry and metabolic systems during important developmental periods, resulting in anatomic changes and/or physiologic dysregulations that subsequently influence development of learning and behavior impairments and chronic stress–related physical and mental illnesses. 19 Studies have indicated that ACEs have long-term impacts on both health and well-being.18,20 It can be argued that incarceration-related stress can affect mothers during and after pregnancy in ways that can influence fetal and newborn infant development with potentially life course effects. Furthermore, ACEs are strongly interrelated such that those exposed to parental incarceration history (PIH) often face a higher likelihood of exposure to other adversities, 18 which may impact child health (eg, maternal depression/anxiety, maternal substance misuse) during and after pregnancy. Furthermore, mothers exposed to incarceration or who experience health challenges considered ACEs to children may themselves have been exposed to PIH and other adversities during childhood. 21 High levels of ACEs in mothers under certain conditions have been associated with greater risk of poor birth outcomes. 22 Thus, a better understanding of links between PIH and health may help disrupt transfer of risks to another generation.
The number of women directly exposed to incarceration is substantially smaller than the number of men exposed, but the rate of incarceration is increasing for women while decreasing for men.23,24 From 2008 to 2018, the female jail population grew 15%, while the male population declined nearly 10%. 25 The high rate of incarceration in the United States has largely been linked to drug sentencing laws, which have disproportionately impacted racial and ethnic minority groups, 26 although substance use in many of these groups is similar to or lower than substance use among non-Hispanic White people. 27 As a result, children of racial and ethnic minority groups have an elevated risk of having a parent with an incarceration history. 28
Women who have direct exposure to incarceration, as well as those who have indirect exposure through their partner, are at high risk for poor health behaviors and outcomes,29-31 which in turn may have lasting impacts on their children. Women who are incarcerated are disproportionately low socioeconomic status; have high rates of substance dependence, sexually transmitted infections, and other health problems; and often do not have access to adequate health care.29,30 Women exposed to incarceration are also more likely than women without exposure to incarceration to have experienced ACEs during childhood and other forms of interpersonal violence as adults. 31 Women with incarcerated partners are also at increased risk for HIV, sexually transmitted diseases, 4 mental health 5 and substance use disorders, 6 and poor health behaviors and chronic disease outcomes. 32 These risks, whether accrued directly from incarceration or indirectly via a partner’s life history, may confer short- and long-term health impacts to infants. Lastly, given the disproportionate impact of incarceration on racial and ethnic minority populations, it is particularly important to understand the extent to which racial and ethnic minority groups are disproportionately impacted by PIH and other ACEs. 33
Evidence suggests that PIH increases the risk of anxiety, depression, posttraumatic stress disorder, migraine headaches, asthma, high cholesterol, high body mass index (BMI), marijuana use, and incarceration in adolescents and young adults.7-9,21 Until recently, substantial gaps existed in knowledge concerning PIH impacts during the perinatal period. Several studies in the past decade investigated impacts but were limited because of the small sample size or data from a single state or a specific correctional setting.34,35 Other studies using data from the Pregnancy Risk Assessment Monitoring System (PRAMS) more broadly examine potential impacts of a history of incarceration among a population-based sample. These studies found associations between PIH and increased risk of resource constraints (ie, prenatal care barriers, maternal food insecurity), health risk behaviors (ie, smoking), and poor infant outcomes (ie, infant low birth weight, preterm delivery).36-40 Findings also indicate public assistance and social support may lessen the harmful effects of perinatal PIH.40,41 The current study extends this literature by examining the relationship between PIH and maternal health outcomes, particularly those identified as ACEs (eg, mental health) to children. It also aims to extend what is known about infant birth outcomes.
Methods
PRAMS is a surveillance system that collects information on maternal behaviors and experiences that occur before, during, and shortly after pregnancy among women who deliver live-born infants in selected states, cities, and territories in the United States. PRAMS surveillance currently covers about 83% of all US births. 42 Using a standardized data collection methodology, participating health departments select, from birth certificate records, a monthly stratified random sample of women. From 2 to 6 months after the delivery of a live infant, women are sampled to complete a survey about their experiences before, during, and shortly after pregnancy. Up to 3 self-administered surveys are mailed to sampled mothers, and those who do not respond are contacted for telephone interviews. Survey data are linked to birth certificate data and weighted for sample design, nonresponse, and noncoverage to produce annual site-specific datasets representative of all live births in each site for the year. 42 The PRAMS study protocol was approved by the Institutional Review Board of the Centers for Disease Control and Prevention and each participating site.
Our study included PRAMS data from 36 states (Alabama, Alaska, Arkansas, Colorado, Connecticut, Delaware, Georgia, Hawaii, Illinois, Iowa, Louisiana, Maine, Maryland, Massachusetts, Michigan, Minnesota, Missouri, Nebraska, New Hampshire, New Jersey, New Mexico, New York State, Ohio, Oklahoma, Oregon, Pennsylvania, Rhode Island, Tennessee, Texas, Utah, Vermont, Virginia, Washington, West Virginia, Wisconsin, and Wyoming) and New York City, hereinafter referred to as the 37 sites. The sites collected data from 2012 through 2015 and achieved a targeted weighted response rate threshold (2012-2014: 60%; 2015: 55%) for at least 1 year of data collection during this time. We used data from 2012-2015 because the PRAMS question asking whether during the 12 months before childbirth the respondent or the respondent’s husband or partner spent time in jail was a core question included on surveys for every PRAMS site during that period. Women who responded yes were directly or indirectly exposed to incarceration and comprised the PIH group in the study.
We obtained maternal demographic information from birth certificate data, including data on age (<20, 20-24, 25-34, ≥35), race and ethnicity (non-Hispanic White, non-Hispanic Black, non-Hispanic American Indian/Alaska Native [AI/AN], non-Hispanic Other, and Hispanic [of any race]), and marital status (married, not married). We examined birth outcome measures. Data on preterm birth (PTB; <37 weeks of gestation) and low birth weight (LBW; <2500 g) came from the birth certificate, and data on neonatal intensive care unit (NICU) admission came from the questionnaire. Information on maternal health conditions, health care–related characteristics, and behavioral and environmental risk factors came from the questionnaire. These measures included prepregnancy diabetes, hypertension, and overweight/obesity (BMI ≥25.0 kg/m2), self-reported prepregnancy depression (ie, did a health care worker tell you that you had this condition?) and postpartum depressive symptoms (ie, answering “always or often” to either of the 2 questions adapted from the Patient Health Questionnaire–2 [PHQ-2] 43 screener about feeling down or depressed and having less interest in activities formerly enjoyed since the baby was born), health insurance coverage in the prenatal period, physical abuse (ie, “During the 12 months before you got pregnant with your new baby” and “during your most recent pregnancy” “did your husband or partner push, hit, slap, kick, choke, or physically hurt you in any way?”), and smoking and alcohol use in the 3 months before pregnancy and during the last 3 months of pregnancy. We combined the 2 physical abuse variables to construct a categorical variable with the 3 possible abuse statuses (ie, no abuse before or during pregnancy, abuse before pregnancy only, abuse during pregnancy only combined with abuse during both periods). The prevalence of experiencing abuse during pregnancy only was small; as such, we combined this category with the category of experiencing abuse both before and during pregnancy.
We pooled weighted data from the 37 sites during the 4 years to calculate the prevalence estimates. We examined the bivariate associations between incarceration history and maternal and infant characteristics using Wald F χ2 tests. We ran crude odds ratios (ORs) and adjusted odds ratios (aORs) to examine the relationships between incarceration exposure and maternal and infant health outcomes. We included demographic variables found to be significant in the bivariate tests, as well as health insurance for prenatal care and experience of physical abuse (before and/or during pregnancy), which have been associated with maternal and child outcomes,44-47 in all adjusted multivariable logistic regression analyses. In addition, because previous studies found associations between smoking during pregnancy and birth outcomes, 48 smoking during pregnancy was also included in adjusted models for birth outcomes. We used SAS-callable SUDAAN version 11.0.3 (RTI International) to account for the complex sampling design.
Results
Based on data from the 37 sites (N = 146 329), the overall prevalence of women reporting that they or their husband or partner were in jail in the 12 months before the birth of their recent baby was 3.7% (n = 6389; Table 1). The distribution of PIH by race and ethnicity—non-Hispanic White (51.3%), non-Hispanic Black (25.5%), non-Hispanic AI/AN (2.5%), non-Hispanic Other (5.3%), and Hispanic (15.5%)—differed significantly from the distribution among women without PIH (P < .001). Differences between women with and without PIH on most demographic and health-related measures were significant. Higher proportions of women with PIH versus without PIH were younger (aged 20-24 years: 36.4% vs 20.1%) and not married (78.8% vs 37.0%; P < .001). A significantly higher proportion of women with PIH versus without PIH had prenatal care covered by Medicaid (70.5% vs 35.9%; P < .001). More than twice as many women with PIH versus without PIH reported smoking during the 3 months before pregnancy (52.2% vs 19.7%), and this difference was 3-fold when examining smoking during pregnancy (33.6% vs 8.8%; P < .001). The 2 groups did not differ significantly on drinking before or during pregnancy; >50% of women in both groups reported drinking alcohol before pregnancy but <10% reported drinking alcohol during pregnancy. Compared with women without PIH, a significantly higher proportion of women with PIH reported abuse by a husband, partner, or ex-husband/ex-partner before pregnancy only (6.9% vs 0.8%) and reported abuse during pregnancy or both before and during pregnancy (16.1% vs 1.7%; P < .001).
Prevalence of a woman or her partner/husband being in jail during the 12 months before the delivery of a live-born infant, by selected maternal and infant characteristics, Pregnancy Risk Assessment Monitoring System, 2012-2015 a
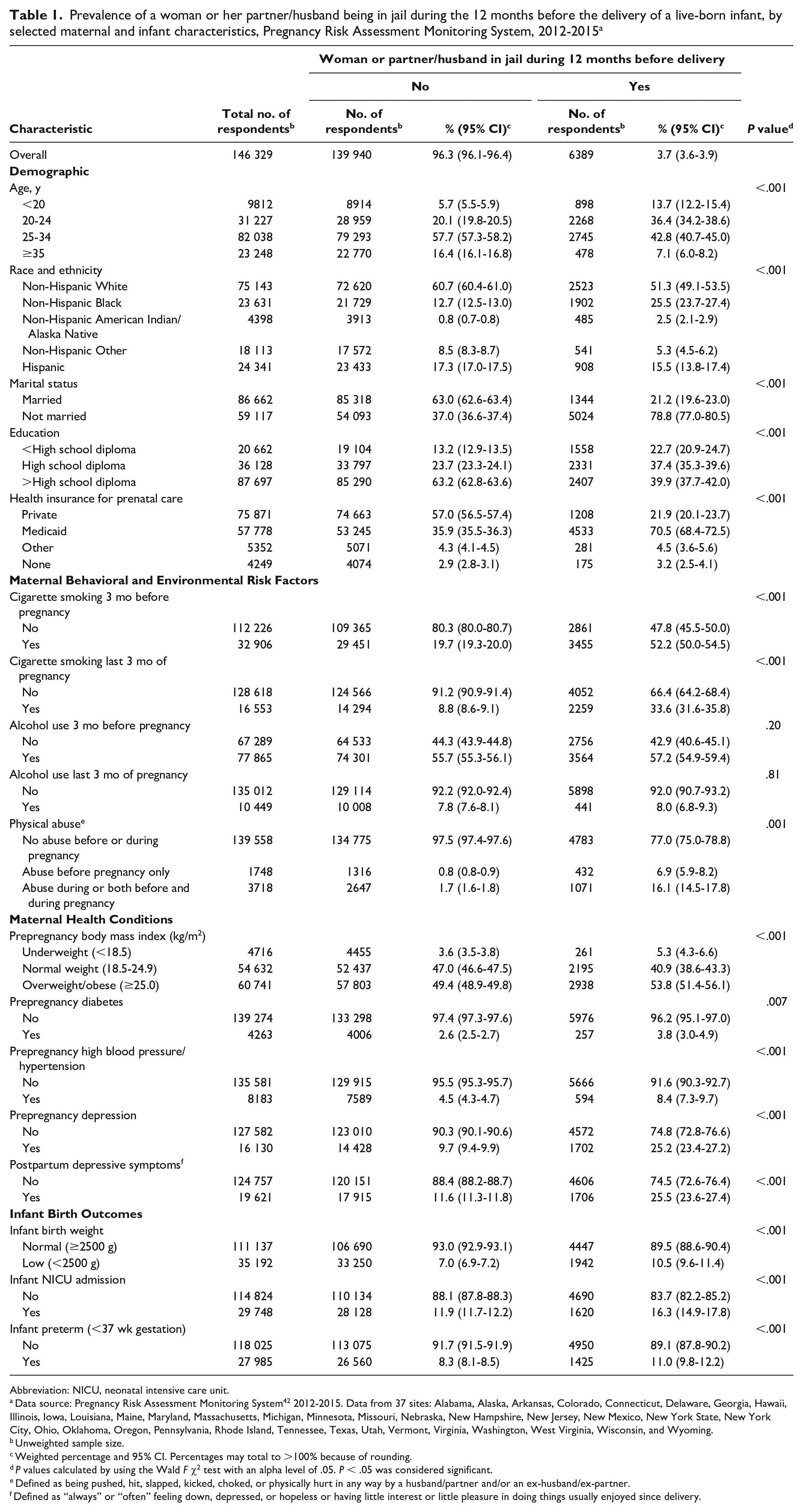
Abbreviation: NICU, neonatal intensive care unit.
Data source: Pregnancy Risk Assessment Monitoring System 42 2012-2015. Data from 37 sites: Alabama, Alaska, Arkansas, Colorado, Connecticut, Delaware, Georgia, Hawaii, Illinois, Iowa, Louisiana, Maine, Maryland, Massachusetts, Michigan, Minnesota, Missouri, Nebraska, New Hampshire, New Jersey, New Mexico, New York State, New York City, Ohio, Oklahoma, Oregon, Pennsylvania, Rhode Island, Tennessee, Texas, Utah, Vermont, Virginia, Washington, West Virginia, Wisconsin, and Wyoming.
Unweighted sample size.
Weighted percentage and 95% CI. Percentages may total to >100% because of rounding.
P values calculated by using the Wald F χ2 test with an alpha level of .05. P < .05 was considered significant.
Defined as being pushed, hit, slapped, kicked, choked, or physically hurt in any way by a husband/partner and/or an ex-husband/ex-partner.
Defined as “always” or “often” feeling down, depressed, or hopeless or having little interest or little pleasure in doing things usually enjoyed since delivery.
A significantly higher proportion of women with PIH than without PIH reported prepregnancy overweight or obese status (53.8% vs 49.4%; P < .001; Table 1). Significantly higher proportions of women with PIH also self-reported that before pregnancy they had been told by a doctor, nurse, or other health care worker that they had diabetes (3.8% vs 2.6%; P = .007), hypertension (8.4% vs 4.5%; P < .001), or depression (25.2% vs 9.7%; P < .001). After pregnancy, a significantly higher proportion of women with PIH than without PIH reported postpartum depressive symptoms (25.5% vs 11.6%; P < .001). Similarly, infants born to women with PIH had poorer outcomes than infants born to women without PIH: the prevalence of LBW (10.5% vs 7.0%), NICU admissions (16.3% vs 11.9%), and PTB (11.0% vs 8.3%) was significantly higher among infants of women with PIH than among infants of women without PIH (all P < .001).
Findings from the crude logistic regression models indicated that women with PIH had higher odds of each adverse maternal and infant outcome examined than did women without PIH. However, these differences did not hold for prepregnancy overweight/obesity status and prepregnancy diabetes when adjusted for confounders. In other adjusted models, women with PIH compared with women without PIH had 2.37 (95% CI, 2.13-2.64) and 2.62 (95% CI, 2.32-2.95) times the odds of smoking before and during pregnancy (Table 2). Women with PIH had significantly higher odds of prepregnancy hypertension (aOR = 1.51; 95% CI, 1.26-1.81), prepregnancy depression (aOR = 1.95; 95% CI, 1.73-2.19), and postpartum depressive symptoms (aOR = 1.49; 95% CI, 1.32-1.67) than women without PIH. Furthermore, they had increased odds of having an infant admitted to a NICU (aOR = 1.18; 95% CI, 1.04-1.33).
Association between a woman or her partner/husband being in jail during 12 months before delivery of live-born infant and selected health-related characteristics, Pregnancy Risk Assessment Monitoring System, 2012-2015 a
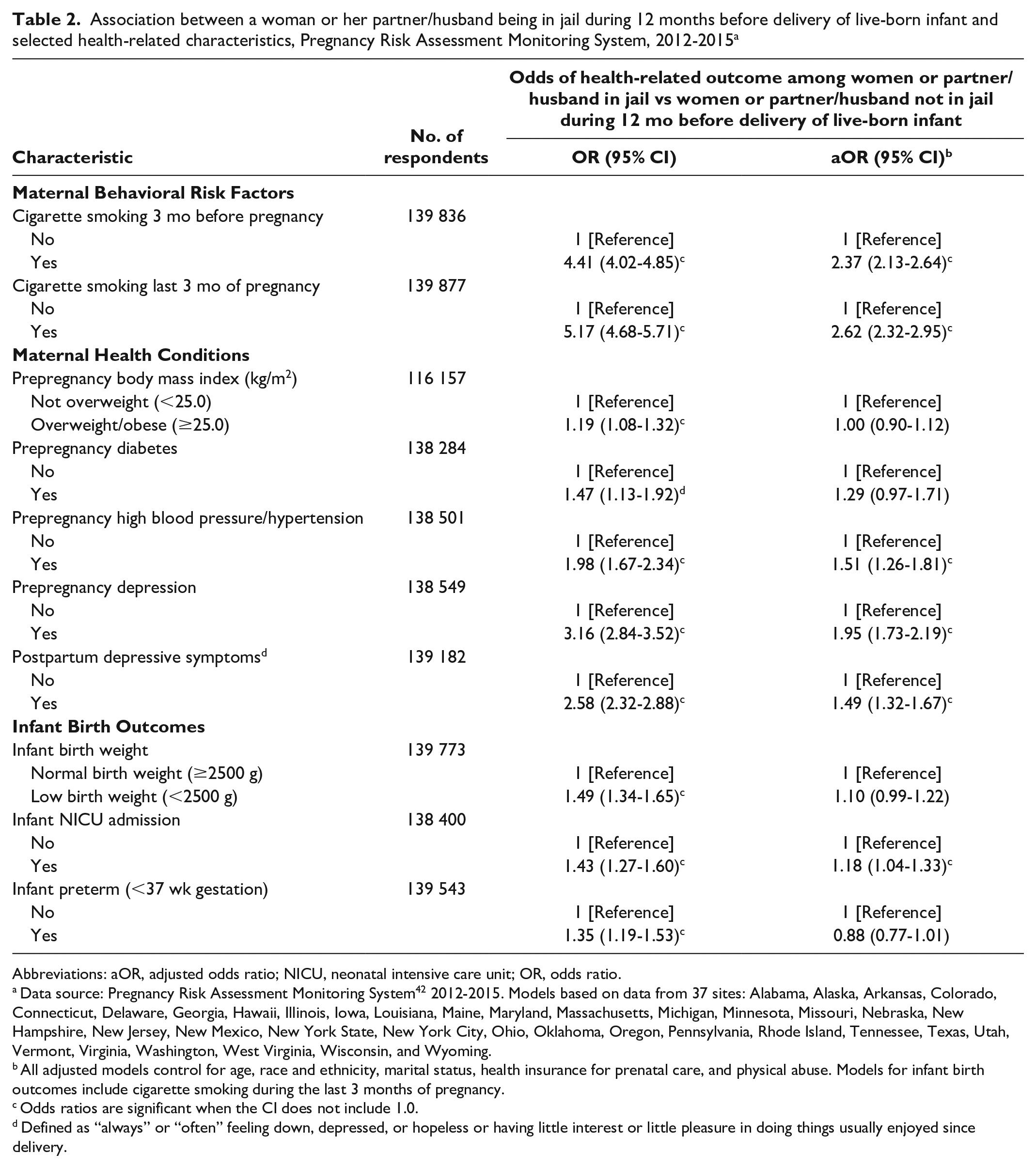
Abbreviations: aOR, adjusted odds ratio; NICU, neonatal intensive care unit; OR, odds ratio.
Data source: Pregnancy Risk Assessment Monitoring System 42 2012-2015. Models based on data from 37 sites: Alabama, Alaska, Arkansas, Colorado, Connecticut, Delaware, Georgia, Hawaii, Illinois, Iowa, Louisiana, Maine, Maryland, Massachusetts, Michigan, Minnesota, Missouri, Nebraska, New Hampshire, New Jersey, New Mexico, New York State, New York City, Ohio, Oklahoma, Oregon, Pennsylvania, Rhode Island, Tennessee, Texas, Utah, Vermont, Virginia, Washington, West Virginia, Wisconsin, and Wyoming.
All adjusted models control for age, race and ethnicity, marital status, health insurance for prenatal care, and physical abuse. Models for infant birth outcomes include cigarette smoking during the last 3 months of pregnancy.
Odds ratios are significant when the CI does not include 1.0.
Defined as “always” or “often” feeling down, depressed, or hopeless or having little interest or little pleasure in doing things usually enjoyed since delivery.
Discussion
This study used a large population-based sample of women from across the United States to (1) determine the prevalence of recent direct or indirect incarceration exposure among women with a recent live birth and (2) examine the relationship between incarceration exposure and maternal and infant health. From 2012 through 2015, the overall prevalence of women who reported that they or their husband or partner were exposed to incarceration during the 12 months before the birth of the baby was 3.7%. This prevalence was similar to the prevalence reported in other studies that used PRAMS data with different years and composition of participating states.40,49
The Dumont study found that compared with women not exposed to incarceration in the year before delivery, women with PIH more frequently experienced social and economic hardship, less frequently reported using birth control, and less frequently received prenatal care. 49 Their research further indicated that compared with women not exposed to incarceration in the year before delivery, women with PIH less often engaged in practices that can promote infant health and well-being, such as breastfeeding, 49 and more frequently reported smoking before and during pregnancy. 38 The current study confirms findings on maternal smoking and prenatal care initiation behaviors and strengthens what is known about maternal and infant health status.
Our study revealed an association between incarceration exposure and mother’s prepregnancy hypertension and prepregnancy and postpartum depressive symptoms. Because maternal mental health conditions are also considered an ACE, strategies are needed to address disparities before, during, and after pregnancy. Support for early health interventions may influence women’s engagement in health promotion practices that may benefit themselves and their infants and prevent children’s downstream ACE exposure. Prenatal care providers have the opportunity to identify women who may have depression during pregnancy. The American College of Obstetricians and Gynecologists recommends that clinicians screen patients at least once for depression during the perinatal period and provide appropriate referrals or follow-up treatment as necessary. 50 Similarly, the US Preventive Services Task Force recommends that clinicians provide or refer pregnant and postpartum patients who are at increased risk of perinatal depression to counseling interventions. 51 Research in prenatal care settings also indicates patients are comfortable with being screened for ACEs 52 (ie, potential sources of depression). Furthermore, enhanced primary care for adults may be used to identify and address psychosocial problems that can affect family functioning, including parenting quality. 53
Findings related to birth outcomes were mixed. Women who reported PIH during 2012-2015 had rates of LBW and PTB (10.5% and 11.0%, respectively) that exceeded the national average (8.1% and 9.6%, respectively, in 2015), 54 which is concerning given that LBW and PTB are major causes of infant mortality and leading contributors to health complications among infants in the United States. In adjusted regression analyses, however, incarceration exposure remained significantly related only to NICU admission, and associations with LBW and PTB were not significant (P = .09 and P = .06, respectively). Our findings are not consistent with those of a recent study by Testa and Jackson. 40 The 2 studies used PRAMS data from different years. As such, the states represented in the data and the analytical sample sizes of the studies differ. In addition, our analysis controlled for smoking and physical abuse, which have been shown to be associated with poor birth outcomes.45-48,55 Research also suggests that links between incarceration exposure and birth outcomes may be explained by other confounding factors, such as relational and financial stressors. 56
The significant association between incarceration exposure and NICU admission may be related to neonatal abstinence syndrome (NAS), a postnatal drug withdrawal syndrome primarily caused by maternal opiate use. Although the most recent data on drug use in correctional populations come from 2007-2009, before steep increases in rates of opioid use disorder in the general population, these data indicated that female jail detainees more frequently reported regular use of heroin/opiates than male jail detainees did (25% vs 17%). 57 In addition, from 2008 to 2018, the female jail detention rate increased 15.4%, whereas the male detention rate decreased 9.1%. 24 This finding is important because research indicates that the opioid epidemic has influenced increases in the incidence of infants with NAS in NICUs. 58 Maternal opioid use measures were not included in the data, so it was not possible to examine whether the association between incarceration exposure and NICU admission was related to maternal drug use. It is worth noting, however, that from 2012 to 2014, the rate of opioid use disorder documented at delivery hospitalization increased from 4.9 per 1000 delivery hospitalizations in 2012 to 6.5 per 1000 delivery hospitalizations in 2014, 59 whereas the rate of NAS per 1000 hospital births increased from 6.0 to 8.0. 60 Alternatively, research indicates that the association between incarceration exposure and NICU admission may be related to health care provider and hospital-based practices.61,62 Future research focused on identifying mechanisms underlying links between incarceration exposure and NICU admission could help determine how best to prevent NICU admissions and promote healthy outcomes.
Our study also identified disparities in the prevalence of incarceration exposure among non-Hispanic Black and non-Hispanic AI/AN women compared with non-Hispanic White women. Given the disparities in incarceration exposure for women of color, the high rates of PTB and LBW among women with recent exposure, and the general disparities by race and ethnicity that exist in PTB and LBW, effective prevention and intervention strategies are needed for racial and ethnic minority women.
Limitations
This study had several limitations. First, PRAMS covers about 83% of all US births, but findings are representative only of the states included in this study. 42 Second, PRAMS data from the questionnaire are self-reported and may be subject to underreporting of sensitive topics. Third, the PRAMS incarceration exposure measure focuses on time spent in jail and does not indicate which parent was exposed to incarceration; both factors have implications for identifying effective clinical and social interventions. Fourth, with respect to health measures, it was not possible to verify clinical diagnosis for conditions such as depression, and while smoking and alcohol use were included in the analysis, controlling for all substance misuse behaviors associated with poor birth outcomes was not possible. Fifth, although it is possible for currently incarcerated women to be selected for participation in the survey, their ability to participate depends on state and local laws. Thus, some of the women most at risk for poor maternal and infant outcomes may not have been able to participate in the study. Finally, the analysis relied on cross-sectional data; thus, it is not possible to determine the direction of association and whether incarceration causes poor outcomes or is merely associated with these outcomes.
Conclusion
Differences exist in maternal characteristics and infant health outcomes when comparing mothers with recent direct or indirect incarceration exposure with women without such history. For significant findings, aORs were generally <2.0. As such additional research is needed to determine the extent to which these mothers and infants are at increased risk of poor health conditions and appropriate clinical responses. However, because a parent’s incarceration exposure is an ACE with the potential to disrupt important developmental periods, impair learning and behavior, and contribute to chronic stress-related physical and mental illnesses,7,19 it is critical for researchers and health care providers to understand the mechanisms underlying the relationship between incarceration and health. It is important for incarceration-exposed women, who largely depend on Medicaid for prenatal care, to have access to prenatal care and enhanced primary care. 53 All mothers benefit from being screened for ACEs, depression, and other risk behaviors and having access to appropriate services (eg, mental health and substance abuse treatment, counseling for survivors of interpersonal violence) to address health needs before, during, and after childbirth. Screening may be particularly important for mothers with recent incarceration exposure. Also, home visitation programs may help foster stronger parent–child bonds and the consistent practice of health promotive behaviors. 63 Finally, strategies that directly influence reductions in population-level incarceration may also help improve maternal and infant health and prevent transfer of adversities across generations.
Footnotes
Acknowledgements
The authors thank the PRAMS Working Group for coordinating collection of the data used in the analysis and Katie Ports, PhD, for providing feedback during the development of this article when she worked for the Division of Violence Prevention, Centers for Disease Control and Prevention.
Author Note
Denise V. D’Angelo is now affiliated to Division of Violence Prevention, National Center for Injury Prevention and Control, Centers for Disease Control and Prevention, Atlanta, GA, USA.
Disclaimer
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.