
Abstract
Objective:
Although many screening tools, resources, and programs for identifying victims of human trafficking exist, consensus is lacking on which tools are most useful, which have been validated, and whether they are effective. The objectives of this study were to determine what tools exist to identify or screen for victims of human trafficking in health care settings and whether these tools have been validated.
Method:
We conducted a scoping review of the literature on human trafficking identification in health care settings following the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) protocol for scoping reviews. We searched the MEDLINE, PsycInfo, Embase, and Scopus databases without language or date limitations. Two independent reviewers screened each citation. We included human research studies in English with populations of all ages, all genders, all geographic locations, and using quantitative and/or qualitative research methods. We excluded studies that were not conducted in a health care setting, review articles, and meta-analyses. We summarized additional screening tools available online and identified through hand-searching.
Results:
Database searches yielded 8730 studies, of which 4806 remained after removing duplicates. We excluded 4720 articles based on title/abstract review, we reviewed 85 full-text studies for eligibility, and we included 8 articles. Hand-searching revealed 9 additional screening tools not found in the literature. Through our search for validated screening tools, only 6 had been studied for validation in health care settings.
Conclusions:
Few studies have evaluated screening tools for identifying victims of human trafficking in health care settings. The absence of a gold standard for human trafficking screening and lack of consensus on the definition of human trafficking make screening tool validation difficult. Further research is required for the development of safe, effective approaches to patient screening.
Human trafficking is a major problem in the United States and globally, with an estimated 40.3 million victims worldwide and 800 000 in the United States annually.1-3 Human trafficking is defined as the involuntary recruitment, transportation, or harboring of a person through force, fraud, or coercion for the purpose of exploitative sexual, physical, or domestic labor, or commercial sex acts or forced labor or services performed by a minor. 4 Human trafficking can have profound health consequences, including physical injuries, sexually transmitted infections, and psychological symptoms.5,6 Consequently, 50% to 88% of victims may have come in contact with a health care provider during their exploitation.6,7 Health care settings are often considered suitable sites for identification of victims, yet it is unclear to what extent identification is practicable, safe, and efficient in these settings. 8
Because of perceived difficulties in identification of human trafficking victims, a need exists for educating health care providers and for systemized methods to improve identification.9-11 Although many screening tools, resources, and programs exist, consensus is lacking on which tools are most useful, which have been validated, and whether they are effective.12-14 In 2012, Macy and Graham 15 performed a review of scientific literature, government reports, and documents from organizations to compile literature relevant to the identification of sex-trafficking victims in the United States. However, many documents and strategies were not validated, and the authors focused on human service settings in general rather than health care settings in particular. A 2016 review examined US health care institution protocols for the identification, treatment, and referral of victims of human trafficking but focused on toolkits and protocols rather than screening tools. 12 A 2017 review examined screening instruments available to identify sexually exploited children for use in health care facilities, limiting its review to the pediatric population. 13 A 2014 review, the closest review to our topic of interest, reviewed screening tools for both sex and labor trafficking for use in US health care settings. 8 However, this review had a limited search strategy, lacked transparency and rigor in its systematic review methods, and did not examine validation studies.
These previous reviews provide a foundation for the literature on screening of trafficking victims; an examination of the validation of screening tools can aid in implementation of evidence-based screening programs. Our scoping review sought to identify and evaluate screening tools that have been validated in peer-reviewed literature for use in health care settings to identify all forms of trafficking, including labor and sex trafficking in the pediatric and adult population, without geographic restrictions.
Methods
Search Strategy
Following the Preferred Reporting Items for Systematic Reviews and Meta-analyses Extension for Scoping Reviews (PRISMA-ScR) guideline, we conducted a review of studies on identification of trafficked people in the health care setting. 16 We developed an internal protocol following the international prospective register of systematic reviews (PROSPERO) model, a database of prospectively registered systematic reviews. 17 All members of the research team received training on the protocol. During March 2020, a trained medical librarian (T.R.) performed searches for studies without language or date restrictions in the MEDLINE, PsycInfo, Embase, and Scopus databases. We developed the searches using a combination of keywords and subject headings centered on the key concepts of “screening” and “human trafficking” (Box). We removed duplicates after the database search.
Ovid MEDLINE search strategy for a scoping review on the validation of screening tools for identifying human trafficking victims in health care settings. This search uses Ovid command language including trunction (*, #) and adjacency (ajd) keywords in the title and abstract (.ti,ab) and medical subject headings (/). The search was conducted on March 10, 2020.
(Interview* or survey* or treatment seeking or screen* or assess* or identif* or charac* or recogn* or report* or detect* or health care or healthcare).ti,ab.
Nurse’s Role/ or Nursing Assessment/ or Mental Health Service/ or Public Health Practice/ or Interviews as Topic/ or Mandatory Reporting/ or Forensic Nursing/ or Social Work/ or Sex workers/ or exp Health Personnel/ed or prevention & control.fs.
1 or 2
((human* or migrant* or sex* or labo#r or adult* or child* or patient* or girl* or boy* or child* or wom#n or m#n) adj3 traffick*).ti,ab.
((Force* or trade or trading or traded or coerc* or slav*) adj3 sex*).ti,ab.
exp Enslavement/ or exp Human Trafficking/
4 or 5 or 6
3 and 7
Five reviewers (M.H., C.J.H., and 3 research assistants) completed a screening by reviewing titles/abstracts, and 4 reviewers (M.H., K.J.T., C.J.H., and H.L.H.) completed an assessment of eligibility by full-text review. We identified studies that examined tools for identification or screening of patients for human trafficking in the health care setting. We included all ages, genders, and geographic locations and excluded studies if they did not include primary data, were review articles or meta-analyses, were not conducted in a health care setting, or were not written in English. We used the same inclusion and exclusion criteria for title/abstract screening and assessment of eligibility; however, if uncertainty existed at the abstract level, we pushed the citation through to full-text review. Two independent reviewers screened and assessed each title/abstract and full-text study. We resolved conflicts through consensus or by the senior author (V.A.) if consensus was not reached.
Four reviewers (M.H., K.J.T., C.J.H., and H.L.H.) hand-searched the 8 included peer-reviewed studies for additional relevant publications, using the same inclusion and exclusion criteria. Hand-searching involved the page-by-page examination of relevant studies within the articles’ text and checking the reference lists of studies retrieved from the database search. Two independent reviewers assessed each additional publication for inclusion. We resolved conflicts through consensus or via the senior author (V.A.) if consensus was not reached.
Data Extraction
For each study and screening tool included in the review, 4 reviewers (M.H., K.J.T., C.J.H., and H.L.H.) extracted data, and 2 reviewers independently verified data entry. We extracted data on the following: study author(s), year of publication, name of screening tool, year tool was last updated, study design and location, type of trafficking studied, tool creators, tool format and length, health care setting for which tool is intended, eligibility criteria, proportion of patients who screened positive, screening tool validity measurements and gold standard used, and measurements of acceptability, reliability, and feasibility. The senior author (V.A.) resolved any discrepancies in data extraction. This study did not require institutional review board approval because it did not involve human subjects.
Results
We identified 8733 studies through our literature search: 8730 studies through a database search and 3 by a hand-search. After removing duplicates, the search yielded 4806 abstracts (Figure). Title/abstract screening excluded 4720 articles, leaving 85 articles for full-text review. Of these 85 articles, 8 studies met the inclusion criteria (Table 1). Hand-searching those 8 studies led to the identification of 3 additional publications, none of which met the inclusion criteria. The hand-search also revealed 9 screening tools available online that were not found in the literature.
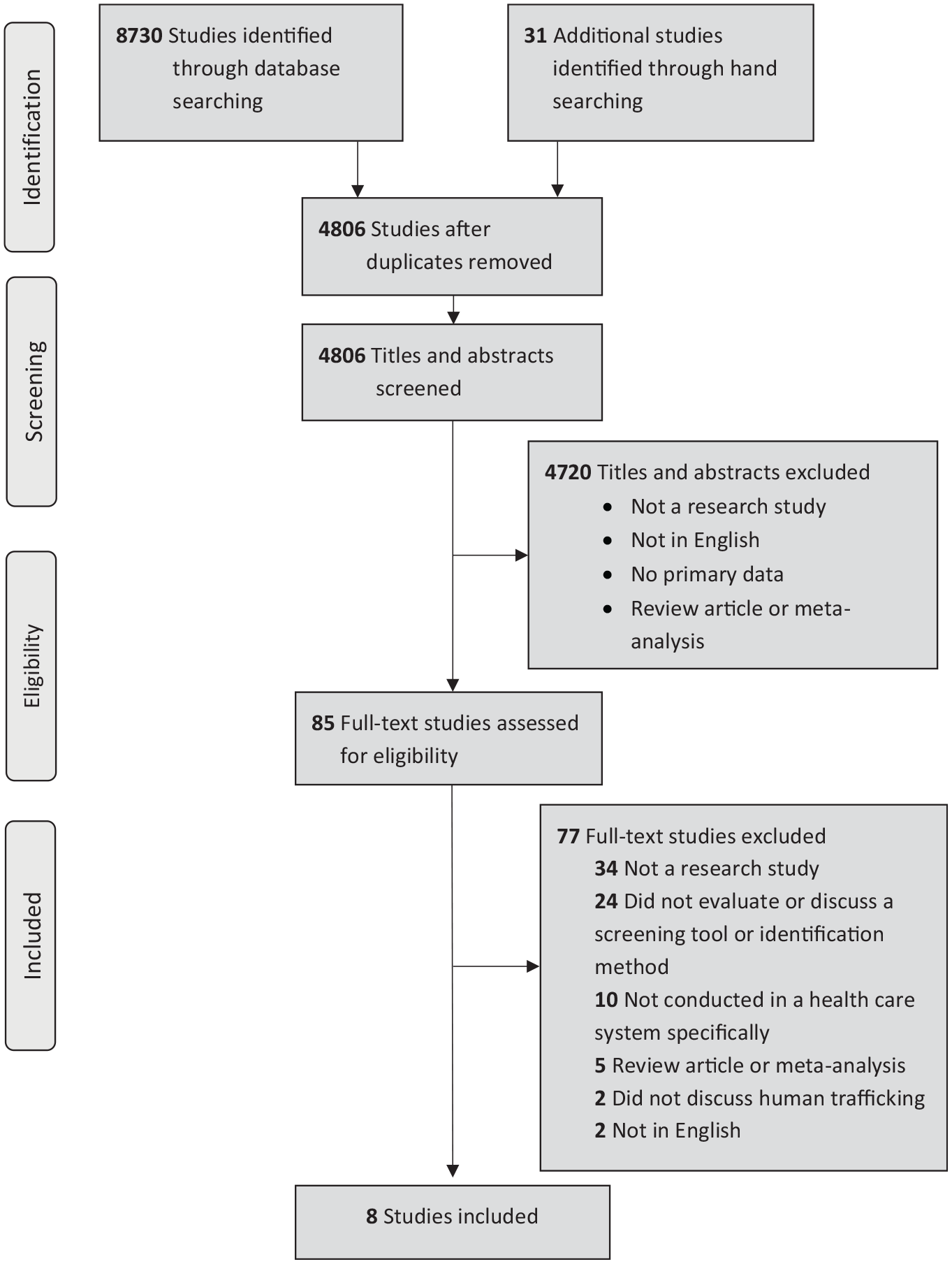
Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) flow chart of a scoping review on the validation of screening tools for identifying human trafficking victims in health care settings, March 2020. Hand-searching involved the page-by-page examination of relevant studies and checking the reference lists of studies retrieved from the database search.
Characteristics of peer-reviewed validation studies of human trafficking screening tools for use in health care settings, published up to March 2020
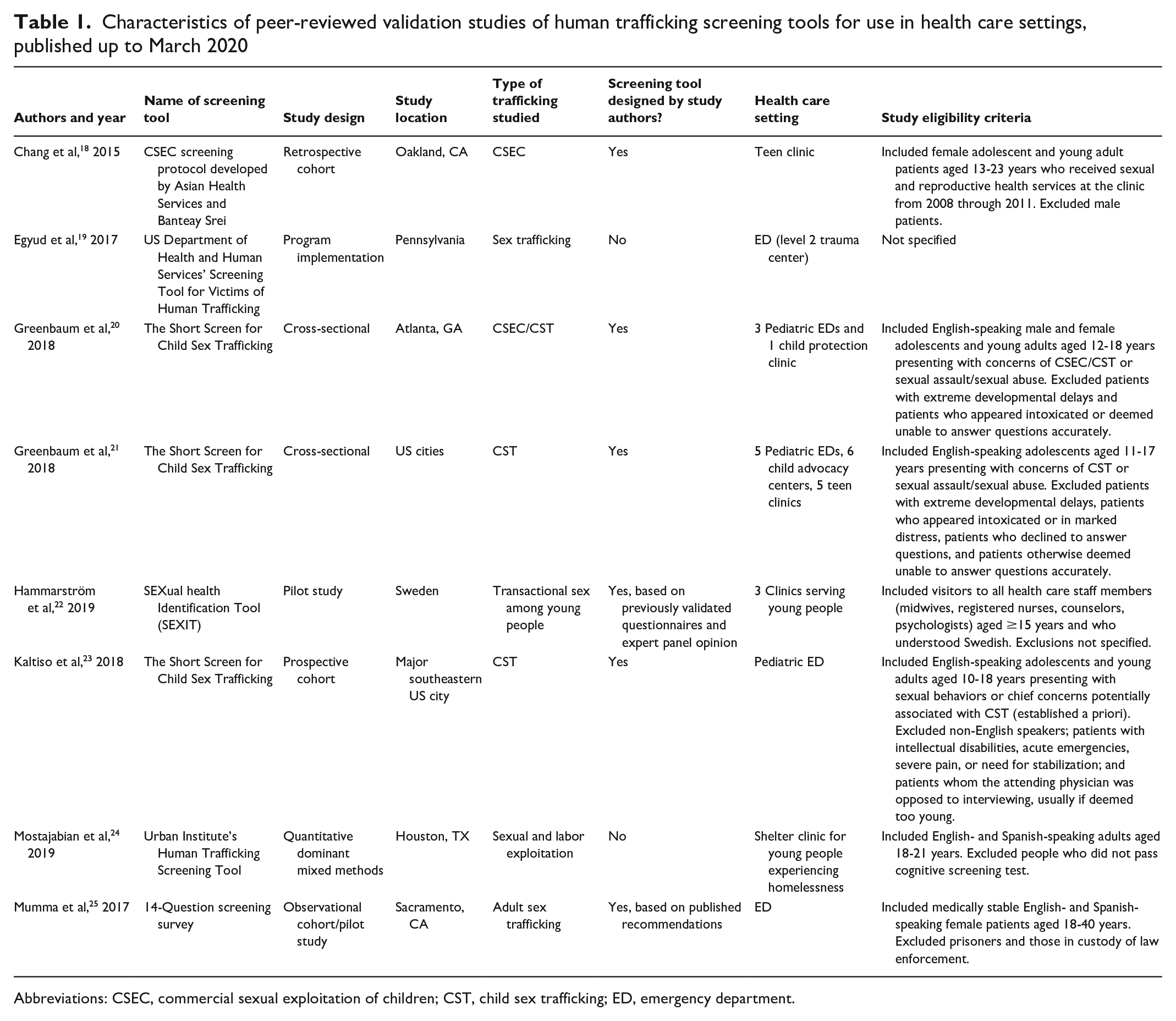
Abbreviations: CSEC, commercial sexual exploitation of children; CST, child sex trafficking; ED, emergency department.
Study Characteristics
The 8 peer-reviewed studies evaluated 6 unique screening tools for human trafficking screening in health care settings (Table 1). The Short Screen for Child Sex Trafficking was assessed in 3 validation studies.20,21,23 Of the 8 included studies, 7 were conducted in the United States, and 1 was conducted in Sweden. 22 Five studies aimed to identify victims of child sex trafficking or transactional sex among young people,18,20-23 1 aimed to identify both child and adult victims of sex trafficking, 21 1 focused on both sexual and labor exploitation among young people, 22 and 1 focused solely on screening for adult sex trafficking. 25
Most of the health care settings in which screening tools had been evaluated were pediatric and adult emergency departments. Other health care settings were teen clinics, clinics serving young people, 1 child protection clinic, and advocacy clinics. Five studies included male and female participants, and 2 studies excluded male participants. One study did not provide inclusion and exclusion criteria, and 1 study provided only inclusion criteria. Of the 7 studies conducted in the United States, 3 required patients to speak English and 2 required patients to speak either English or Spanish. The study conducted in Sweden required patients to speak Swedish for inclusion. Of the 6 studies that provided exclusion criteria, 4 excluded patients with intellectual disabilities or developmental delays.
Human Trafficking Screening Tools
Five validation studies provided some measure of screening tool effectiveness, such as the proportion of patients who screened positive for human trafficking (Table 2). Values ranged from 7.3% 18 to 49.3%. 23 Four studies reported measures of screening tool validity, such as sensitivity and specificity. Sensitivity ranged from 84.4% 21 to 100.0%, 25 and specificity ranged from 53.1% 23 to 78.0%. 25 One study examined the content validity and face validity of the SEXual health identification tool (SEXIT). 22 Five studies specified the gold standard used for validation measurements, such as patient self-report, health care providers’ decision, or social work documentation. Only 2 assessed screening tool acceptability,19,22 no studies examined screening tool reliability, and 2 studies measured screening tool feasibility (Table 2).22,25
Characteristics of validated human trafficking screening tools for use in health care settings identified in peer-reviewed literature, March 2020
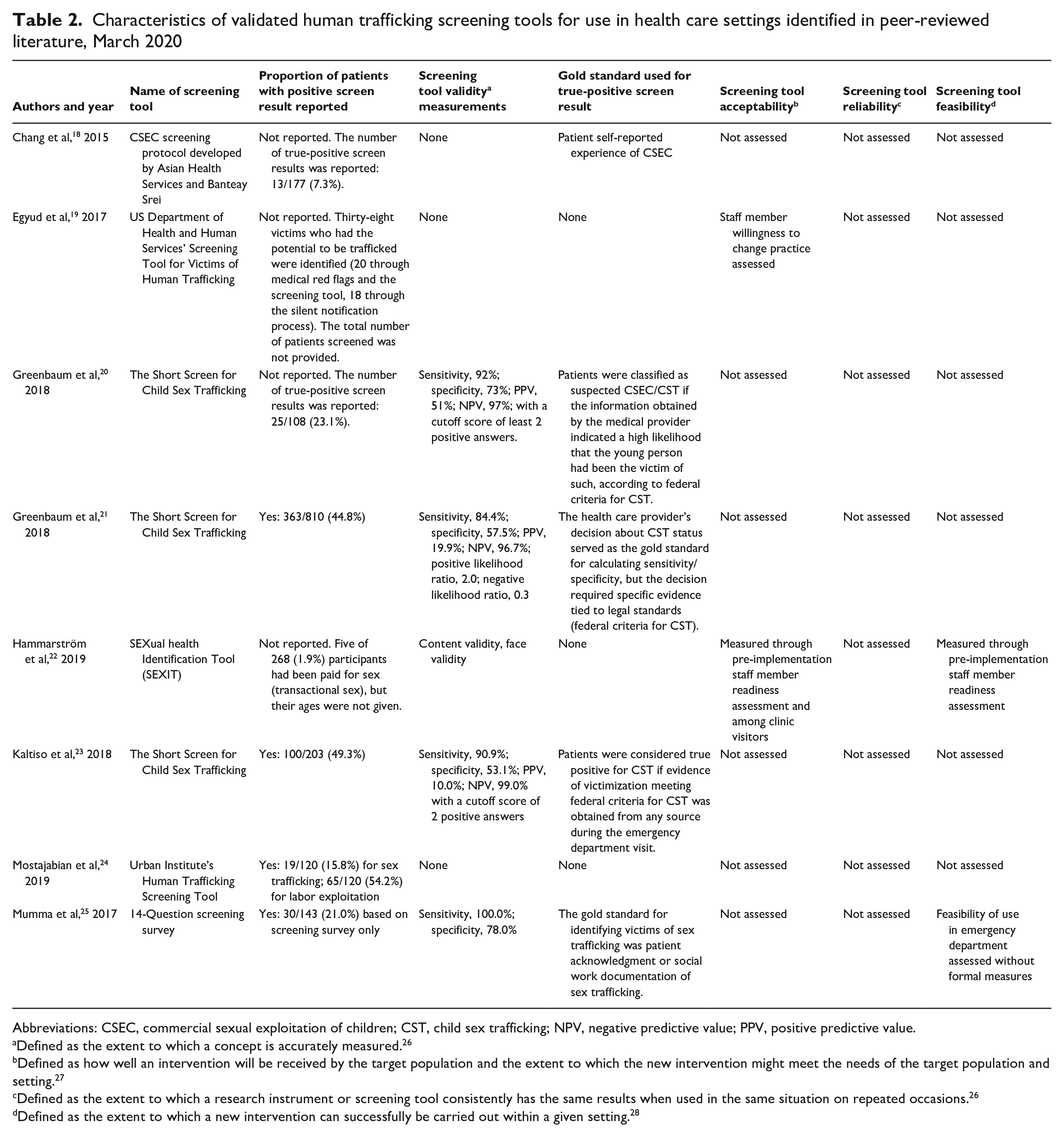
Abbreviations: CSEC, commercial sexual exploitation of children; CST, child sex trafficking; NPV, negative predictive value; PPV, positive predictive value.
Defined as the extent to which a concept is accurately measured. 26
Defined as how well an intervention will be received by the target population and the extent to which the new intervention might meet the needs of the target population and setting. 27
Defined as the extent to which a research instrument or screening tool consistently has the same results when used in the same situation on repeated occasions. 26
Defined as the extent to which a new intervention can successfully be carried out within a given setting. 28
Screening questions covered a range of themes, such as housing situation, substance use, law enforcement involvement, intimate partner violence, sexual or labor exploitation, immigration status, and physical health. Of the screening tools found in the 8 validation studies, 4 were administered exclusively as questionnaires, 1 as an interview, and 1 as a self-administered survey. One screening tool (Urban Institute Human Trafficking Screening Tool [HTST]) was administered as either a questionnaire or a survey. Finally, only 1 screening tool included an opportunity for victims to self-identify via a silent notification method after an interview. 19 Tool length ranged from 6 questions (Short Screen for Child Sex Trafficking) to 19 questions (Urban Institute HTST).
Hand-searching these 8 studies led to the discovery of 9 additional human trafficking screening tools designed for use in health care settings (Table 3). One of these 9 screening tools was validated by the tool authors in a published technical report that was not peer-reviewed but is available on their website (the WestCoast Children’s Clinic Commercial Sexual Exploitation–Identification Tool). 29 We found no validation or evaluation studies for the other 8 screening tools.
Summary of validated and nonvalidated screening tools available online to identify trafficked people in health care settings, published until March 2020
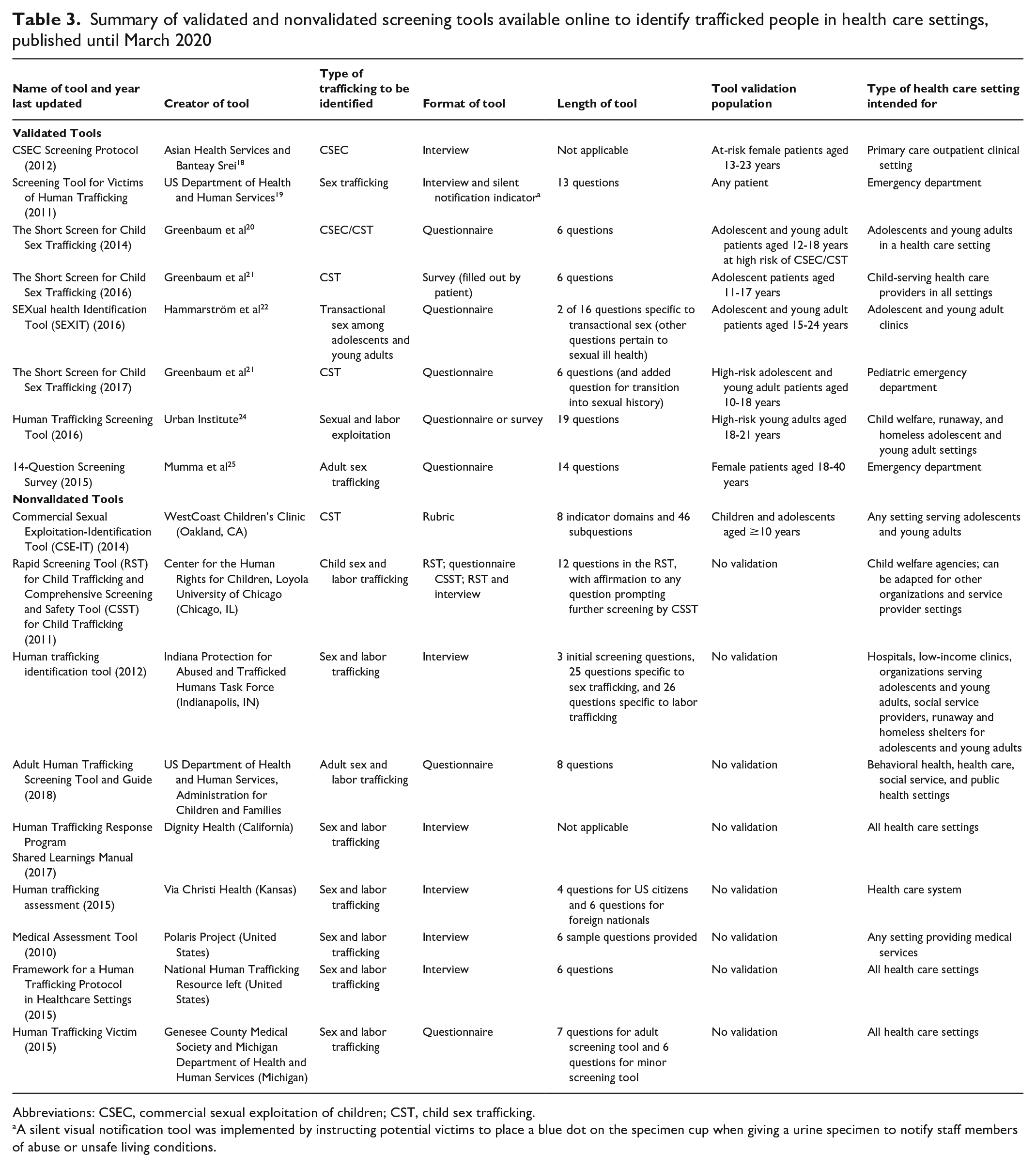
Abbreviations: CSEC, commercial sexual exploitation of children; CST, child sex trafficking.
A silent visual notification tool was implemented by instructing potential victims to place a blue dot on the specimen cup when giving a urine specimen to notify staff members of abuse or unsafe living conditions.
Of the 17 screening tools, 6 targeted victims of child trafficking (with 2 tools originating from the Short Screen for Child Sex Trafficking), 2 targeted a broader category of adolescent and young adult victims of trafficking, 2 targeted adult victims, and 7 targeted victims of all ages. Eight tools sought to identify victims of sex trafficking, and 9 tools aimed to identify victims of sex and/or labor trafficking. No screening tool was designed to identify solely victims of labor trafficking. Most available screening tools included requirements such as the presence of red flags that would then prompt the screening tool. These tools often consisted of physical, emotional, and behavioral indicators including chief concerns about sexual assault or physical abuse, or social characteristics such as homelessness or undocumented status. Only 3 screening tools had no requirement for screening and instead recommended screening all presenting patients.
Discussion
Through our comprehensive search for validated screening tools in peer-reviewed literature, only 6 tools had been studied for validation in health care settings. We identified an additional 9 screening tools intended for use in health care settings online without associated peer-reviewed validation studies. Our findings suggest that tools intended to detect trafficking victims might not always be validated, designed for use in health care settings, or general enough to be used for different types of trafficking.8,12,13,15 One obstacle in human trafficking research, and specifically in the validation of screening tools, is that no gold standard has been established for identifying victims in health care settings, leading several of the included studies to use self-identification, social work documentation, or physician concern as a reference to determine screening tool sensitivity and specificity. 30 However, many victims do not disclose their trafficking status because of a lack of trust in health care workers, fear of trafficker retaliation, guilt and shame, or lack of awareness that they are being trafficked.13,30,31 Because disclosure or physician concern is not a reliable reference standard for identification, these validation studies may not be especially strong.
Future studies should be conducted with true validation in mind, instead of administering screening tools in real-world health care settings where the prevalence of human trafficking is unknown. Studies could be conducted in social service organizations that care for survivors of human trafficking, where the tools would be administered to people whose trafficking status is known, allowing for a more accurate assessment of the screening tool’s sensitivity and specificity before being tested in health care settings. Among the currently available screening tools, the Short Screen for Child Sex Trafficking is the only tool that has been evaluated in several studies.20,21,23 Although it is short and has consistently demonstrated relatively high sensitivity (923%, 84.4%, 90.9%), its specificity is low (73.0%, 57.5%, 53.1%), and it aims to identify victims of child sex trafficking only. Future studies could further evaluate this screening tool for both pediatric and adult populations. It is also notable that assessments of reliability and feasibility were nearly absent. Ensuring that the screening tools produce consistent measures across various tool administrators is critical to ensure inter-rater reliability.
All but 1 of the 8 peer-reviewed studies focused solely on the identification of sex trafficking victims, which highlights a greater focus of anti-trafficking efforts on sex trafficking rather than labor trafficking, despite both being human rights violations with consequences for individual and community health. 32 The focus of law enforcement on prosecuting sex trafficking to a greater extent than labor trafficking reinforces the perception that labor trafficking occurs to a lesser degree and perpetuates a cycle of decreased identification and rescue of labor trafficking victims. 32
The terminology used to describe human trafficking varied, particularly for minors. Terms included commercial sexual exploitation of children, child sex trafficking, or more general terms such as sex trafficking or sexual and labor exploitation. SEXIT was included as a screening tool for sex trafficking because it asks respondents whether they have ever been “reimbursed/paid for sex” and targets adolescents and young adults aged 15-24 years. However, the authors refer to this as “transactional sex” rather than sex trafficking. One step in establishing formal identification protocols in health care institutions is to reduce the variability of terms to streamline data collection and reporting. Consistent terminology is key to conducting relevant research and developing laws, policies, and programs to prevent human trafficking, and definitions should be empirically established. 33
One limitation in the articles evaluating screening tools was their inclusion criteria. Three studies included only English-speaking participants, and 4 studies excluded patients with developmental delays or intellectual disabilities. These restrictions lead to the exclusion of populations highly vulnerable to human trafficking and limit the generalizability of these validation studies. The English-language requirement for screening may impede identification of victims of labor trafficking. An analysis of cases investigated from 2008 to 2010 in the United States showed that 95% of confirmed victims of labor trafficking were undocumented or legal immigrants who may not speak English, whereas most confirmed sex trafficking cases were US citizens. 34 In addition, young people with intellectual disabilities have high rates of various types of sexual victimization and are at greater risk for sex trafficking exploitation than young people without intellectual disabilities. 35 Lastly, only 1 study 22 noted that being lesbian, gay, bisexual, transgender, or queer/questioning (LGBTQ+) was a risk factor for human trafficking victimization, despite LGBTQ+ young people experiencing a higher vulnerability to sex trafficking than their non–LGBTQ+ peers. 36 These risk factors need to be addressed in the context of trafficking identification and survivor advocacy programs.
In several articles, trained researchers administered the tool.23-25 However, if health care providers are to ultimately administer these tools, evidence of their use by health care providers is needed. Few studies examined the acceptability or appropriate workflow for incorporating the screening tools into regular practice. Of the tools for which a validation study was found, only 2 studies also assessed staff member readiness for implementation of the screening tool.19,22 Although insufficient data are available to determine the optimal length of questionnaires, succinctness and ease of administration are important elements to consider when designing tools for use by health care providers. 13 Lastly, it is necessary to clarify whether the goal of screening for human trafficking is to consistently and universally screen all patients in health care settings such as emergency departments or to target patients who present with red flags (eg, pelvic or abdominal pain, no photographic identification, avoiding eye contact). 19 An emphasis on the initial recognition of red flags by clinicians to prompt administration of screening tools showcases the importance of clinical training and education. 31
Intimate partner violence (IPV) screening in health care settings has barriers similar to human trafficking screening, including time constraints, lack of consistent protocols, and lack of evidence of effectiveness. 37 Both types of screening have the potential for adverse outcomes, such as increased retaliation from the abuser and safety concerns for health care staff members, but also offer unique opportunities for education and discussion with the patient. In 2004, the US Preventive Services Task Force recommended against universal screening for IPV because of insufficient data on the effectiveness and benefits of screening tools. 38 In 2013, the task force updated its recommendation to recommend routine IPV screening for all women of reproductive age, based on data showing that IPV screening was associated with improved health outcomes.39,40 Similarly, although the literature on screening for trafficking is insufficient, further research focusing on effectiveness and outcomes may demonstrate the utility of screening for trafficking in health care settings.
Finally, screening tools must exist within larger protocols outlining events that should take place after victim identification, including referrals to local resource organizations, child protective services, and trained law enforcement. 12 HEAL Trafficking and Hope for Justice recently published a Protocol Toolkit for Developing a Response to Victims of Human Trafficking in Health Care Settings that may be useful for health care institutions looking for guidance on the identification and care of trafficking victims. 41 As anti-trafficking educational programs and initiatives grow within the field of medicine, recommendations for screening should be built on rigorous validation studies that assess accuracy, safety, reliability, feasibility, and acceptability in various health care settings and usefulness for victim detection. 8
Limitations and Strengths
Our review had 2 limitations. First, the underrepresentation of health-related research on human trafficking and lack of standardized search terminology led to the identification of a limited number of studies on its recognition in health care settings, despite relatively broad inclusion and exclusion criteria. This underrepresentation may be tied to the hidden and criminal nature of trafficking, as well as methodological challenges related to validating screening tools among a difficult-to-access population. Second, because we included only studies available in English, we may have missed pertinent non–English-language research studies on human trafficking identification.
Our review also had several strengths. First, our search included literature on screening for both sex and labor trafficking for adults and children and was not limited to the United States. Second, we used systematic methods with the support of a research librarian to search for a broad body of literature, and we included relevant resources and tools published online, which were not found in peer-reviewed journals. Third, each abstract, full-text article, and non–peer-reviewed resource was screened by 2 independent researchers. Our summary of human trafficking screening tools designed for health care providers may support interested health care institutions in promoting further research on screening for trafficked people, as well as enhancing training of medical students, residents, and physicians.
Conclusions
Despite the high prevalence of human trafficking globally and nationally, and its profound consequences on health, our scoping review highlights a gap between available screening tools for human trafficking identification in health care settings and validation in the peer-reviewed literature. Labor trafficking is even more underrepresented than sex trafficking in academic research, with most identification efforts geared toward sex trafficking. The absence of a reliable gold standard for identification and lack of academic and legal consensus on the definition of human trafficking make the validation of new screening tools difficult. Although health care settings could be ideal windows of opportunity for recognizing and assisting trafficked people, barriers persist. Currently, insufficient data are available to conclude that widespread use of screening tools and indicator checklists in health care settings leads to improved victim recognition. Further research is required for the development of safe and effective approaches to patient screening, identification, and provision of trauma-informed care for this vulnerable population.
Footnotes
Author Note
Veronica Ades is now affiliated to Department of Obstetrics, Gynecology, and Women’s Health, Albert Einstein College of Medicine, Bronx, New York, USA.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.