
Abstract
Objectives
Human trafficking is a public health issue that has substantial health consequences. However, research on the preparedness of health facilities to serve people who have experienced or are experiencing human trafficking is limited. We examined health facility preparedness related to human trafficking in Michigan.
Methods
We used a cross-sectional design to explore health facility preparedness related to human trafficking in Michigan. We sampled 10 prosperity regions according to health facility type (Federally Qualified Health Centers, health departments, and hospitals). An email invitation was sent to identified health facility personnel (eg, administrators, physicians, nurses) from May to June 2019 with a link to a 26-item survey with items about current policies, protocols, and areas for improvement related to human trafficking.
Results
Forty-two Federally Qualified Health Centers, health departments, and hospitals responded to the survey. Most health facilities had screening policies and response protocols related to child maltreatment (screening: 32/41 [78.0%]; response: 38/40 [95.0%]) and intimate partner violence (screening: 33/41 [80.5%]; response: 37/40 [92.5%]). However, fewer facilities had a screening policy (16/41 [39.0%]) and response protocol (25/40 [62.5%]) for human trafficking; more of these facilities focused on sex trafficking than on labor trafficking. The top needs related to human trafficking were (1) individual-level health care provider training, (2) health facility–level screening policies and response protocols, (3) community-level resources, and (4) societal-level awareness, funding allocation, and data.
Conclusions
Facility-level resources are needed to ensure that health care providers have adequate training and support to address human trafficking in the health care system.
Human trafficking is a human rights violation with profound health consequences. Human trafficking is compelled service that involves the recruitment of people by force, fraud, or coercion for the purposes of labor trafficking (eg, involuntary servitude, peonage, debt bondage, slavery) or sex trafficking (eg, commercial sex). 1 Although data on the prevalence of human trafficking in the United States are lacking, 2 the International Labour Organization estimates that 40.3 million people worldwide were trafficked in 2016, including 24.9 million in forced labor and 15.4 million in forced marriage. 3
Evidence suggests that victims of human trafficking experience trauma throughout their trafficking experience that is linked to negative physical health (eg, chronic pain, chronic conditions), reproductive and sexual health (eg, pregnancy complications, infections, genitourinary injuries), and mental health outcomes (eg, depression, anxiety, posttraumatic stress disorder, substance abuse). 4 -10 An estimated 28%-88% of human trafficking victims come into contact with a health care provider during their exploitation and often are not recognized as human trafficking victims. 11 -14 However, these studies were limited by small sample sizes (range, 21-173 participants), 11 -14 geography, 11,13 and, in 1 study, a focus on only domestic victims of sex trafficking. 14
Many health care providers in the United States lack the knowledge, training, and confidence to identify and respond to human trafficking. 15-17 Data on health care provider knowledge and response are often limited by small sample sizes and a focus on female sex trafficking victims. In addition to these limitations on identification, human trafficking victims have health care needs that are not being met.
Only a handful of validated screening tools for human trafficking are available, 18 -21 many of which are limited by (1) a lack of evidence, particularly in the health care milieu; (2) a lengthy administration process that is not practical in the fast-paced health care environment; (3) the need for expertise in human trafficking; and (4) being available and validated only in English. Health facilities could consider systemwide policies that provide guidance on universal education, similar to the shift in providing resources to all patients on intimate partner violence (IPV; eg, the Confidentiality, Universal Education and Empowerment, Support intervention [CUES] from Futures Without Violence). 22,23
The lack of a validated screening tool or even trauma-informed and people-centered screening processes that can be used by all health care professionals for potential victims of both labor and sex trafficking is especially problematic for health care facilities attempting to implement guidance on screening and response via policies and protocols. 24-26 Despite the extensive use of institutional screening policies and response protocols to guide health care providers in other areas, these tools are lacking for human trafficking. 27,28
New statewide continuing education requirements on human trafficking went into effect in 2015 for health care professionals in Michigan (Act 368 of the Michigan Public Health Code). 29 However, focus on the systems where health care providers work and provide care is limited. Overall, little research has been conducted on the preparedness of health facilities to serve human trafficking victims. 25 The research that has been conducted at health facilities has focused on hospitals and not considered how other types of health facilities can build on preexisting policies and protocols for IPV and child maltreatment. The objective of this study was to describe the needs of various types of health facilities in Michigan related to education, screening, and response for human trafficking.
Methods
This study used a cross-sectional survey design. The University of Michigan Institutional Review Board considered this study exempt because of the anonymous nature of the survey.
Sampling and Recruitment
We divided the state into 10 regions according to prosperity regions developed by the governor’s office. 30 We sampled regions according to 3 health facility types: Federally Qualified Health Centers (FQHCs), health departments, and hospitals. We recruited 4 health facilities of each type per region for a total of 120 health facilities that received the survey.
We randomly sampled health departments from 4 counties in each region using the Michigan Department of Health and Human Services map of counties. 31 In some rural regions, a single health department represents more than 1 county.
We classified FQHCs (focused on primary care) into 4 groups based on their health professional shortage area (HPSA) score, which ranges from 0 to 25. 32 We grouped FQHCs based on the following HPSA scores: (1) 0-6, (2) 7-13, (3) 14-19, and (4) 20-25, with higher scores representing higher need. We selected 1 FQHC from each HPSA score group in each region.
Finally, we used the American Health Association Annual Survey Data, which include hospital contact information and number of beds, to develop the hospital list for sampling. We selected 4 hospitals from each region, identified by ZIP codes. We considered the number of beds (range, 15-903) so that each region represented a range of hospital capacity.
Three research assistants telephoned each site using a standardized prompt to explain the study, invite participation, and obtain email addresses to send the survey. If the sites were unable to be reached after 2 attempts by telephone, we used a list of closely matched alternate locations to meet the goal of recruiting 4 health facilities of each type per region.
Measures
We developed a survey with 26 items that addressed (1) characteristics of the health facility (n = 7); (2) yes/no items (n = 11) on the existence of screening policies, response protocols, and educational offerings for IPV, child maltreatment, and human trafficking; (3) a single multiple-choice item on health facility desires; and (4) open-ended response options (n = 7) focused on current screening policies, response protocols, barriers, and desired information, training, and resources.
Procedures
Potential study participants received an email invitation from the study email address with a link to a Qualtrics survey from May to June 2019. We obtained electronic consent from each participant at the beginning of the survey. We reminded participants that the study was voluntary and that they could end participation at any time. Participants could upload written information on any facility policies or protocols related to human trafficking. We kept the Qualtrics survey open for 8 weeks, and we sent an email reminder to nonresponders approximately 2 weeks after the initial survey was sent.
Analysis
The initial sample consisted of 57 respondents. In the quantitative analysis, we excluded 11 respondents who completed <25% of the survey and 4 duplicate respondents (ie, another person in their facility had already submitted a survey), thus yielding 42 respondents (and 43 unique sites) in the final sample. In the qualitative analysis, we did not exclude the 4 duplicate respondents, because we felt they provided an additional perspective, thus yielding 46 respondents in the final sample.
We used concurrent mixed-methods analyses to obtain a basic understanding of health facility practices and needs related to human trafficking in Michigan. We analyzed yes/no and multiple-choice responses using SPSS version 24 (IBM Corp). We first calculated descriptive statistics and frequencies. Because of the small sample size, we used the 2-sided Fisher exact test to compare differences among existence of policies and protocols for the 3 types of health care facilities, with P < .05 considered significant.
We exported all open-ended responses to Microsoft Excel and used content analysis and the constant comparative method of analysis. 33,34 We used content analysis to examine open-ended questions about the content of existing response protocols, continuing education modalities, and barriers to identification and response.
We found a large amount of overlapping content in responses to desires for continuing education and support. We analyzed these 2 open-ended questions together. First, 2 coders (M.M.K., K.M.) read and analyzed each open-ended response independently. Next, the coders met to compare categories for agreement, compiled open codes into a single analytical memo, and combined codes into 4 major themes. Once we achieved data saturation, all authors reviewed themes for validity. 35
We triangulated data from the yes/no questions, the multiple-choice item, and open-ended items to seek convergence and corroborate findings. 36 We compared key themes from the open-ended questions with survey data related to existing policies, protocols, and needs related to human trafficking using convergent validation.
We also reviewed policies for inclusion of the definition of human trafficking, discussion of both labor and sex trafficking, and the location (stand-alone vs part of preexisting policy/protocol).
Results
Sample Characteristics
Facilities in the quantitative analysis included 13 health departments, 7 FQHCs, and 22 hospitals (Table 1). We received responses from all prosperity regions; however, the highest response rate was from the Detroit metropolitan region. The HPSA scores of FQHCs that responded to the survey ranged from 14 to 23 (Table 2). Regional health facility response rates varied from 8.3% to 66.7% in the final sample; a higher percentage of hospitals (55.0%) than FQHCs (17.5%) and health departments (32.5%) responded.
Responses to a survey on health facility preparedness related to human trafficking, by health facility and region, Michigan, May–June 2019 a
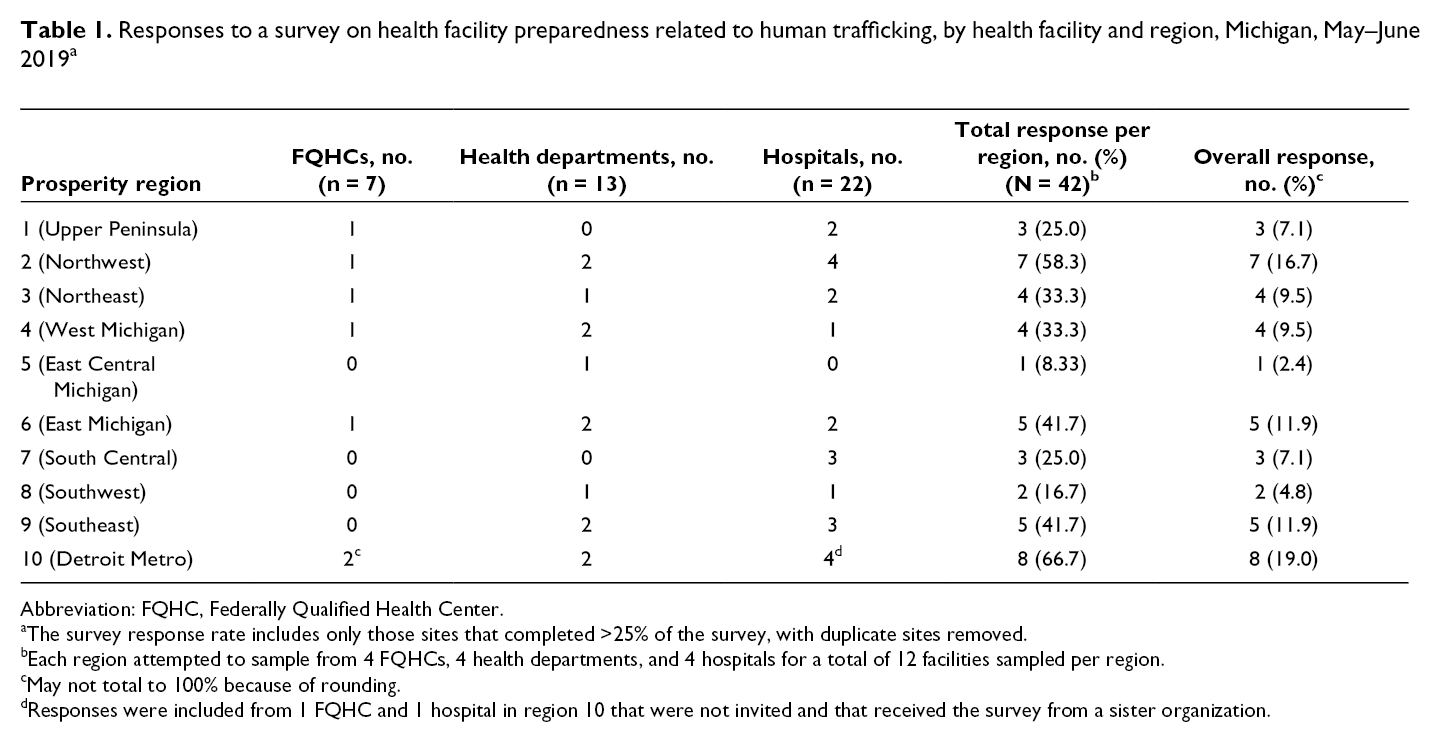
Abbreviation: FQHC, Federally Qualified Health Center.
aThe survey response rate includes only those sites that completed >25% of the survey, with duplicate sites removed.
bEach region attempted to sample from 4 FQHCs, 4 health departments, and 4 hospitals for a total of 12 facilities sampled per region.
cMay not total to 100% because of rounding.
dResponses were included from 1 FQHC and 1 hospital in region 10 that were not invited and that received the survey from a sister organization.
Number of patients seen annually at health facilities (n = 42), by health facility type, Michigan, May–June 2019 a
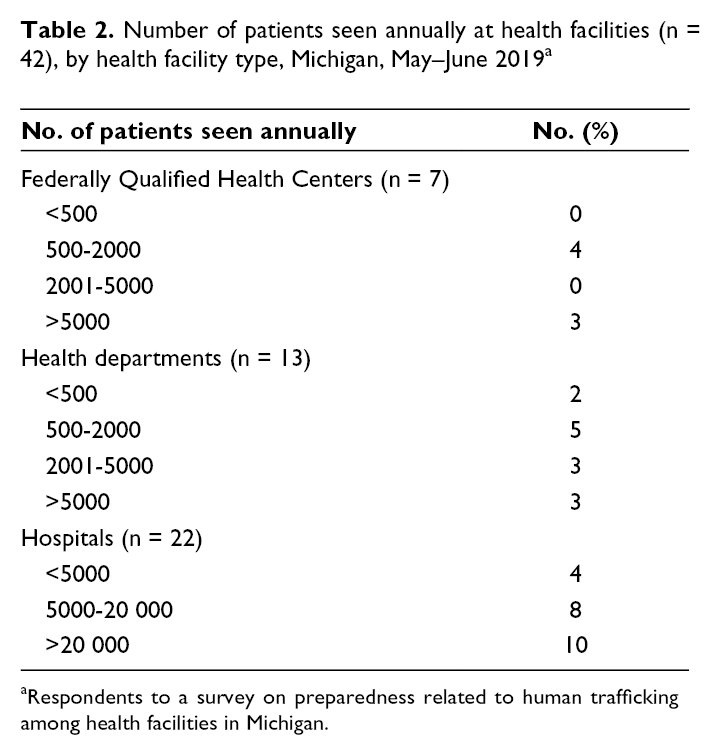
aRespondents to a survey on preparedness related to human trafficking among health facilities in Michigan.
Screening Policies and Response Protocols
Most health facilities had screening policies related to child maltreatment (32 [78.0%]) and IPV (33 [80.5%]) (Table 3). Of 16 (39.0%) facilities with a screening policy for human trafficking, 13 included a screening policy for sex trafficking and 10 included a screening policy for labor trafficking. We found no significant differences between the type of health facility and the presence of a screening policy related to child maltreatment (P = .52), IPV (P = .57), or human trafficking (P > .99).
Health facilities with screening and response policies related to child maltreatment, intimate partner violence, and human trafficking, Michigan, May–June 2019 a
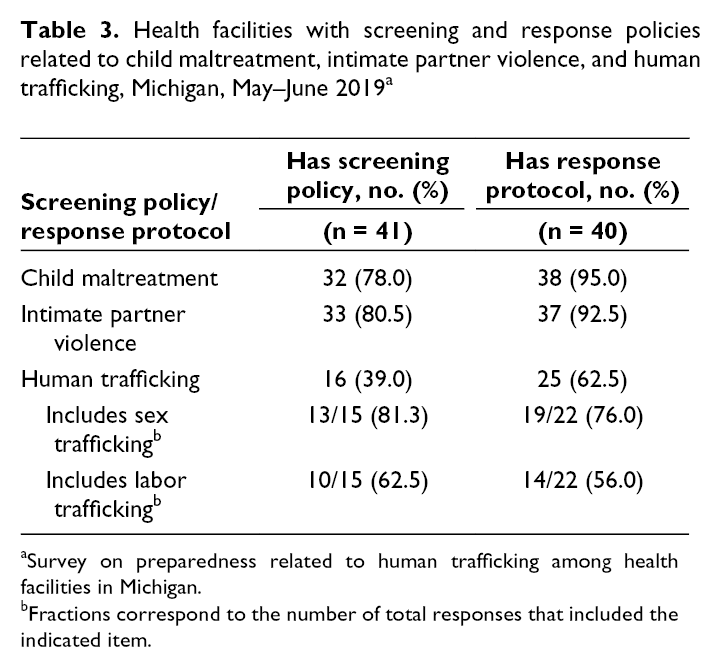
aSurvey on preparedness related to human trafficking among health facilities in Michigan.
bFractions correspond to the number of total responses that included the indicated item.
Most health facilities had response protocols for child maltreatment (38 [95.0%]) and IPV (37 [92.5%]; Table 3). Twenty-five (62.5%) health facilities reported having response protocols for human trafficking, of which 19 facilities had response protocols related to sex trafficking and 14 facilities had response protocols related to labor trafficking. We found no significant differences between the type of health facility and the presence of a response protocol related to child maltreatment (P = .24), IPV (P = .57), or human trafficking (P = .75).
Eleven of 21 respondents noted that prioritizing safety and referrals was a necessary component of protocols to respond to human trafficking (Table 4). Of 33 respondents, 17 noted limited resources and 14 noted a lack of training as barriers to serving human trafficking victims. Eight of 23 respondents wrote that outside speakers were most likely to provide opportunities for learning about human trafficking, and 25 of 28 respondents saw continuing education offerings as the highest health facility need related to human trafficking.
Analysis of open-ended and multiple-choice responses to a survey on health facility preparedness related to human trafficking, Michigan, May–June 2019 (N = 46) a
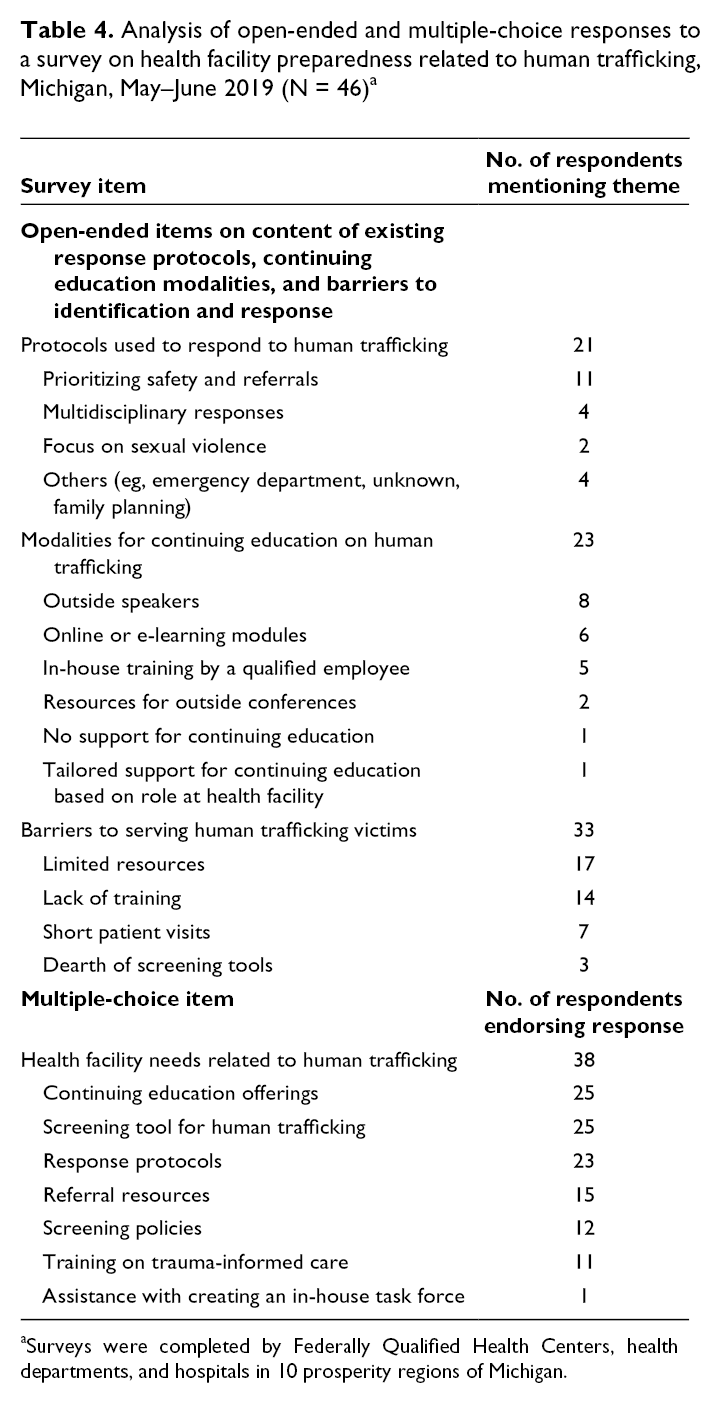
aSurveys were completed by Federally Qualified Health Centers, health departments, and hospitals in 10 prosperity regions of Michigan.
Health Facility Desires
We elucidated 4 themes from the open-ended questions on desires for support and continuing education (n = 33 respondents). The themes can be depicted within an ecological framework (Figure): (1) individual-level health care provider training, (2) health facility–level screening policies and response protocols, (3) community-level multidisciplinary resources and response teams, and (4) societal-level awareness, funding allocation, and data on human trafficking.
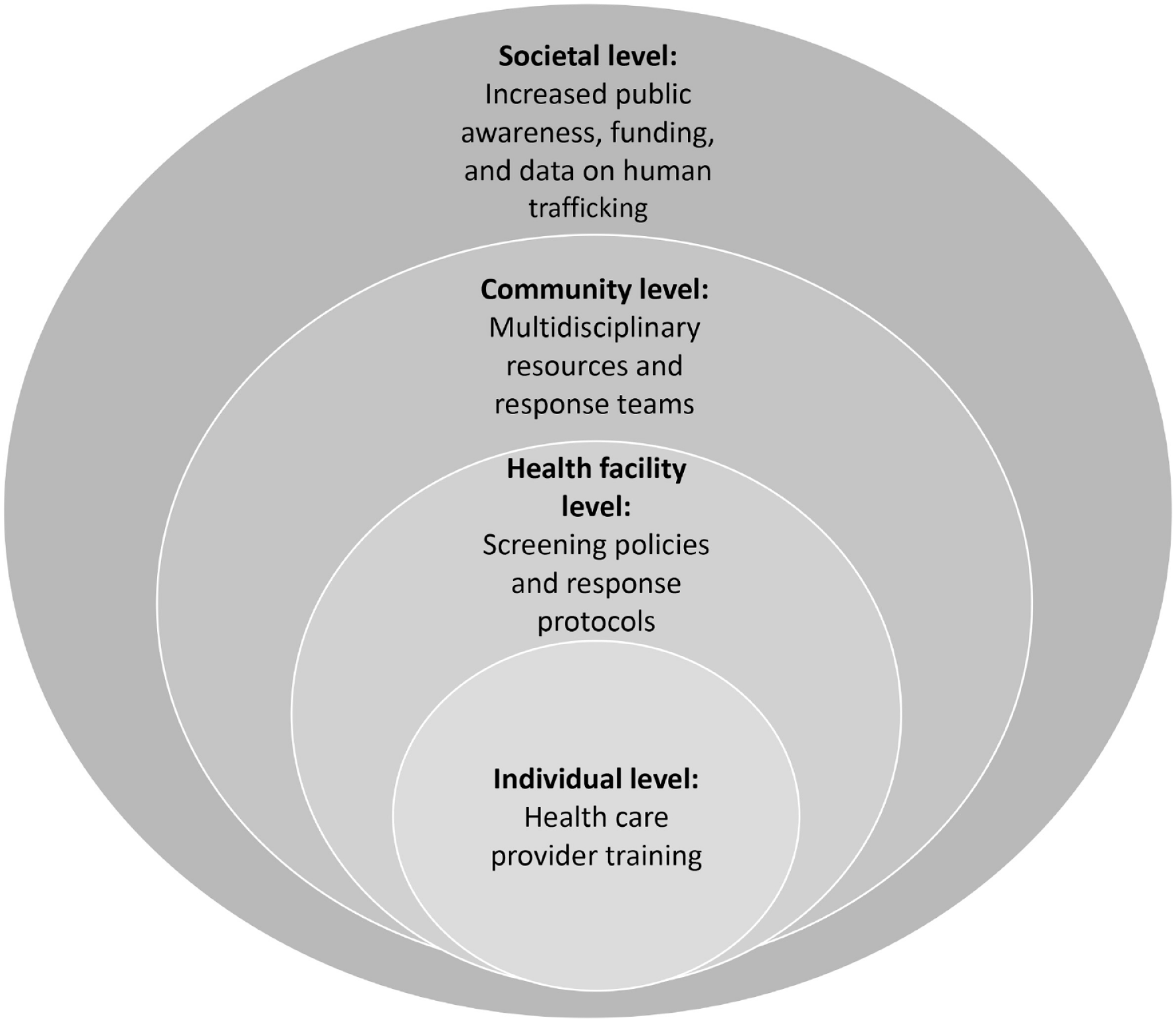
Socioecological framework to guide improvements in human trafficking identification and response in the health care setting and themes identified from open-ended questions on the desires for support and continuing education received, as part of a survey on health facility preparedness related to human trafficking, Michigan, May–June 2019.
At the individual level, participants described training related to human trafficking, trauma-informed care, and realistic case studies to help educate all staff members (eg, medical assistants, nurses, physicians, counselors, front office staff members). This theme was reflected in statements such as, “We need training. This is not even a topic discussed at our facility” and “Trauma training for nurses would be [a] beneficial resource for victims of human trafficking.”
At the health facility level, participants described screening policies and response protocols that are implemented in all units, not just the emergency department and obstetric triage. In addition, participants noted that having these facility-level resources in the electronic medical record would make them the most accessible to clinicians. This theme was reflected in the following response, “Examples of screening tools and policies. Getting staff comfortable with what to do if they believe there is a possible victim present.”
At the community level, participants wanted a 24-hour hotline and “multidisciplinary teams in order to coordinate care across the service continuum through established trusted/vetted relationships for soft handoffs of victims for care beyond the hospital.” One participant stressed the need for internal resources related to mental health, noting:
“If there was funding and demand for mental health services specifically for victims of human trafficking or sexual assault, we could keep this population connected within our facility, thus limiting the chance of losing contact with victims because they don’t follow through on a referral to another agency.”
Finally, at the societal level, participants noted a need for more awareness, funding, and data to provide a “profile of human trafficking.” Participants said that increasing required training for health care providers would require additional funds. One participant said, “Nurses/physicians have so many mandatory education modules they have to complete each year, adding human trafficking is a cost that the health system cannot afford to pay for at this time.”
Policy Analysis
Participants shared 8 policies and protocols: 5 included a definition of human trafficking, of which 4 were based on federal legal definitions, and 1 did not mention labor or sex trafficking. Four policies were preexisting policies on various forms of interpersonal abuse (eg, child maltreatment, IPV, sexual assault) that either did not mention human trafficking at all (n = 1) or listed it as a form of abuse but did not specify guidance related to human trafficking (n = 3). The other 4 policies included a number of links to outside resources. However, many of these links were broken, leading to potential difficulties accessing the resources and information needed during a health care encounter.
Discussion
This study found that most health facilities surveyed in Michigan had screening policies and response protocols for child maltreatment and IPV, but fewer health facilities had screening policies and response protocols related to human trafficking, particularly policies and protocols that addressed both labor and sex trafficking. The legal protections in place for reporting and responding to child maltreatment have likely driven the need for institutional policies and protocols. For IPV, national policies and funding to support universal screening (eg, Affordable Care Act) and guidance from national groups such as the US Preventive Services Task Force and American College of Obstetricians and Gynecologists have contributed to the creation of facility-wide policies and protocols. 37,38 To date, most research and media attention have focused explicitly on sex trafficking, leaving health care providers with little guidance on screening and responding to labor trafficking and the needs (eg, visas, other legal relief) of human trafficking victims who are foreign nationals or undocumented immigrants. 39
Screening policies and response protocols are designed to help health care facilities and health care providers deliver standardized care to all patients. Human trafficking screening policies and response protocols can build on existing policies and protocols related to child maltreatment, elder abuse, IPV, and sexual violence. 40 Health facilities that have developed policies and protocols could share them with other facilities. It is important to ensure that human trafficking policies and protocols are comprehensive, clearly define human trafficking, and note unique differences from other forms of abuse. In Michigan, no legal guidance addresses human trafficking of foreign nationals or undocumented immigrants. Many health care providers lack knowledge on the legal needs of human trafficking victims, underscoring the need for multidisciplinary teams and continuing education.
Our results reinforce findings from a qualitative study conducted in 2018 in South Carolina hospitals while also extending the findings to various types of health systems (eg, FQHCs, health departments, hospitals), a different region, and illustrating the prevalence of other types of policies and protocols that can be used as a framework to address needs specific to human trafficking. 25 It is essential that all types of health care facilities are included in research on human trafficking. 41 Health care facilities serve a vital role in human trafficking identification and response that has been overlooked in state and federal policies. 42 Health facilities have the ability to recommend and/or provide rigorous training to their entire workforce (eg, front office, environmental services, health care providers) to ensure that all employees are working together to meet the needs of human trafficking victims. They also can work to ensure that screening policies and response protocols are easily integrated into electronic medical records to ensure consistent use. Ongoing efforts are needed to provide continuing education and training to the health care workforce and support staff members. 27,43-45
Victims of human trafficking have complex and diverse health care, social service, and legal needs. 45 Without institutional policies and protocols to bridge the gap between health care providers and resources at the community and national levels, it is difficult to mount the coordinated multidisciplinary response that victims of human trafficking need. 46 This lack of coordination was evident in our data when respondents indicated that they were unaware of resources that already exist, including the 24-hour National Human Trafficking Hotline. Evidence-based resources and tools that are translated into multiple languages are needed for health care providers and health facilities, such as websites with continuing education training, sample policies and protocols, and guidelines on best practices (https://humantrafficking.umich.edu). 47
Limitations
This study had several limitations. First, it was limited by its geographic focus on Michigan; however, the insights gathered may inform our understanding of health facility needs throughout the United States. Second, the response rate was higher among hospitals than among FQHCs and health departments and higher for the Detroit metropolitan region than for the other 9 prosperity regions. As such, some of the rural regions that depend on FQHCs and health departments may not have been well represented in our study. These facilities may have had fewer resources for human trafficking than facilities that participated in the survey because of limited health facility and community resources. Third, of the 120 health facilities contacted, only 42 unique sites completed the survey, and we received written information on policies and protocols from only 8 of the 25 facilities that reported having one. The limited number of policies and protocols shared could be because respondents were not willing to share their internal documents or because, upon further review, they realized that their health care facilities and associated policies and protocols did not explicitly cover human trafficking, despite indicating on the survey that they had a human trafficking policy or protocol. Finally, because of the small number of policies and protocols received, we were unable to examine other important components, such as racial and ethnic disparities and attention to particularly vulnerable populations (eg, foreign nationals, undocumented immigrants, people experiencing homelessness, runaway young people).
Conclusions
Globally, the 2030 Sustainable Development Goals developed by the United Nations General Assembly to achieve a more sustainable future for all have set the target to eliminate human trafficking 48 ; however, our study showed that substantial work is required at all ecological levels to achieve this goal. 49 As awareness of human trafficking has grown, many states have begun to pass legislation requiring that health care providers complete continuing education on the topic before license renewal. 42 However, these state-level policies are only one piece of a larger framework needed to address human trafficking at the individual, health facility, community, and societal levels. Policies that strictly focus on individual-level knowledge and training will not be successful in eradicating human trafficking without larger systemic changes. Many of these changes can begin at the health facility, with standardized guidance on screening and response, including multidisciplinary response and referral networks established in the community.
Footnotes
Acknowledgments
The authors thank Emily Sheridan-Fulton, MPH, MSW, and Tamar Alexanian, JD, for their assistance with this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors acknowledge funding and support from Katheryn F. Soller. The University of Michigan Human Trafficking Collaborative would not have been possible without her contributions and foresight.