
Abstract
Although human trafficking is recognized as a public health issue, research on the health effects of human trafficking and best intervention practices is limited. We describe 2 citywide collaborative victim services models, the THRIVE (Trafficking, Healthcare, Resources, and Interdisciplinary Victim Services and Education) Clinic at the University of Miami and Jackson Health System in Miami, Florida, and the Greater Houston Area Pathways for Advocacy-based, Trauma-Informed Healthcare (PATH) Collaborative at Baylor College of Medicine, CommonSpirit Health, and San Jose Clinic in Houston, Texas, funded in part by the Office for Victims of Crime, which focus on trauma-informed health care delivery for victims of human trafficking. From June 2015 through September 2021, the THRIVE Clinic served 214 patients with an average age of 28.7 years at the time of their first visit. From October 2017 through September 2021, the PATH Collaborative received 560 suspected trafficking referrals, 400 of which screened positive for labor or sex trafficking. These models serve as a framework for replication of interdisciplinary practices to provide health care for this unique population and preliminary information about the strategies put in place to assist victims during their recovery. Key lessons include the importance of a citywide needs assessment, patient navigators, interdisciplinary care, and building community partnerships to ensure safe housing, transportation, identification, health insurance, vocation services, input from survivors, peer-to-peer mentorship, and medical–legal services. Further research is needed to understand the detrimental health effects of trafficking and the health care needs of victims. In addition, a need exists to develop optimal models of care for recovery and reintegration for this patient population and to address public health, legal, and medical policies to ensure access to and sustainability of comprehensive, trauma-informed, interdisciplinary victim services.
Human trafficking is the recruitment, harboring, transportation, provision, or obtaining of a person for labor and services, through the use of force, fraud, and coercion, for the purpose of subjection to involuntary servitude, peonage, debt, bondage, or slavery.1,2 An estimated 40.3 million human trafficking victims worldwide are part of the more than $150 billion trafficking industry, although estimates of the actual number of victims are hard to obtain because of the hidden and criminal nature of trafficking.3-5 The National Human Trafficking Hotline handled 63 380 cases of human trafficking reported in the United States from 2007 through 2019.6-8
Research indicates that 4 fundamental services for survivors of human trafficking need to be provided: (1) housing; (2) a safe, confidential health care environment with trauma-informed care; (3) a comprehensive needs assessment; and (4) case management to coordinate legal, medical, and social services.2,9-30 Often, medical care lacks the long-term, consistent, trauma-informed approaches necessary for these medically complex patients. The goal of providing trauma-informed care is to realize, recognize, respond to, and resist retraumatization. 31 Health care providers who create a safe, comfortable environment for trafficking victims and practice compassionate, trauma-informed, victim-centered care can improve engagement in and access to services.2,11,12,15,17-33 Women and adolescents interviewed immediately after leaving a trafficking situation in Europe reported a substantial reduction in subjective physical and mental health symptoms after 2 months of continued health care. 34
Two victim services models (1 in Miami, Florida, and 1 in Houston, Texas) are funded in part by the Office for Victims of Crime (OVC), which is 1 of 6 offices of the US Department of Justice established to enhance victim services. In Miami, the THRIVE (Trafficking, Healthcare, Resources, and Interdisciplinary Victim Services and Education) Clinic, based at the University of Miami Miller School of Medicine, provides a model of outpatient trauma-informed interdisciplinary health care for victims of human trafficking, referred primarily by law enforcement. The Greater Houston Area Pathways for Advocacy-based, Trauma-Informed Healthcare (PATH) Collaborative at Baylor College of Medicine, CommonSpirit Health, and San Jose Clinic in Houston is a collaborative citywide victim services model with a focus on health care. These collaborative models provide easy access and high-quality, interdisciplinary, trauma-informed medical care and victim services to restore and rehabilitate survivors of human trafficking.25-33 Previous publications on the 2 models focused on client demographic characteristics, health consequences, and community collaborations,27,35,36 but in-depth descriptions and implementation considerations have not been discussed.
Purpose
The purpose of this case study is to provide a detailed description of 2 unique models of health care for victims of human trafficking, outcomes, lessons learned, and practice implications. A need exists to develop standard-of-care practices for serving victims of all forms of human trafficking. Ideally, established collaborative victim services models can serve as a framework nationwide to create practices for interdisciplinary, comprehensive, and trauma-informed health care services.
Methods and Outcomes
THRIVE Clinic, Miami
Key partners, including medical, legal, and social services professionals, recognized the need for health care resources in recovery for adult trafficking victims and, in 2015, established the THRIVE Clinic. The OVC awarded funding for expansion of this initiative in 2016. 37 The THRIVE Clinic provides medical and mental health care services for trafficking victims in an outpatient clinic setting located in a public tertiary care hospital, Jackson Memorial Hospital, which is a teaching hospital for the University of Miami Miller School of Medicine (Figure 1). Policies and protocols ensure services are trauma-informed and coordinated with other service providers, including the US Department of Homeland Security, the State Attorney’s Office, homeless shelters, substance abuse treatment centers, and community agencies serving this population. The THRIVE Clinic serves victims of all forms of suspected or confirmed human trafficking, regardless of their sex, gender, age, or immigration status. From June 2015 through September 2021, the THRIVE Clinic received an average of 6 patient referrals per week and served 214 patients. Seventy-five percent of trafficking victims were US citizens, 95% were female, and 78% were aged <30 years at their initial visit. Eighty-three percent of patients reported sex trafficking, 9% reported labor trafficking, and 8% reported both; 40% identified as Black, 35% as Hispanic, and 18% as White. 36
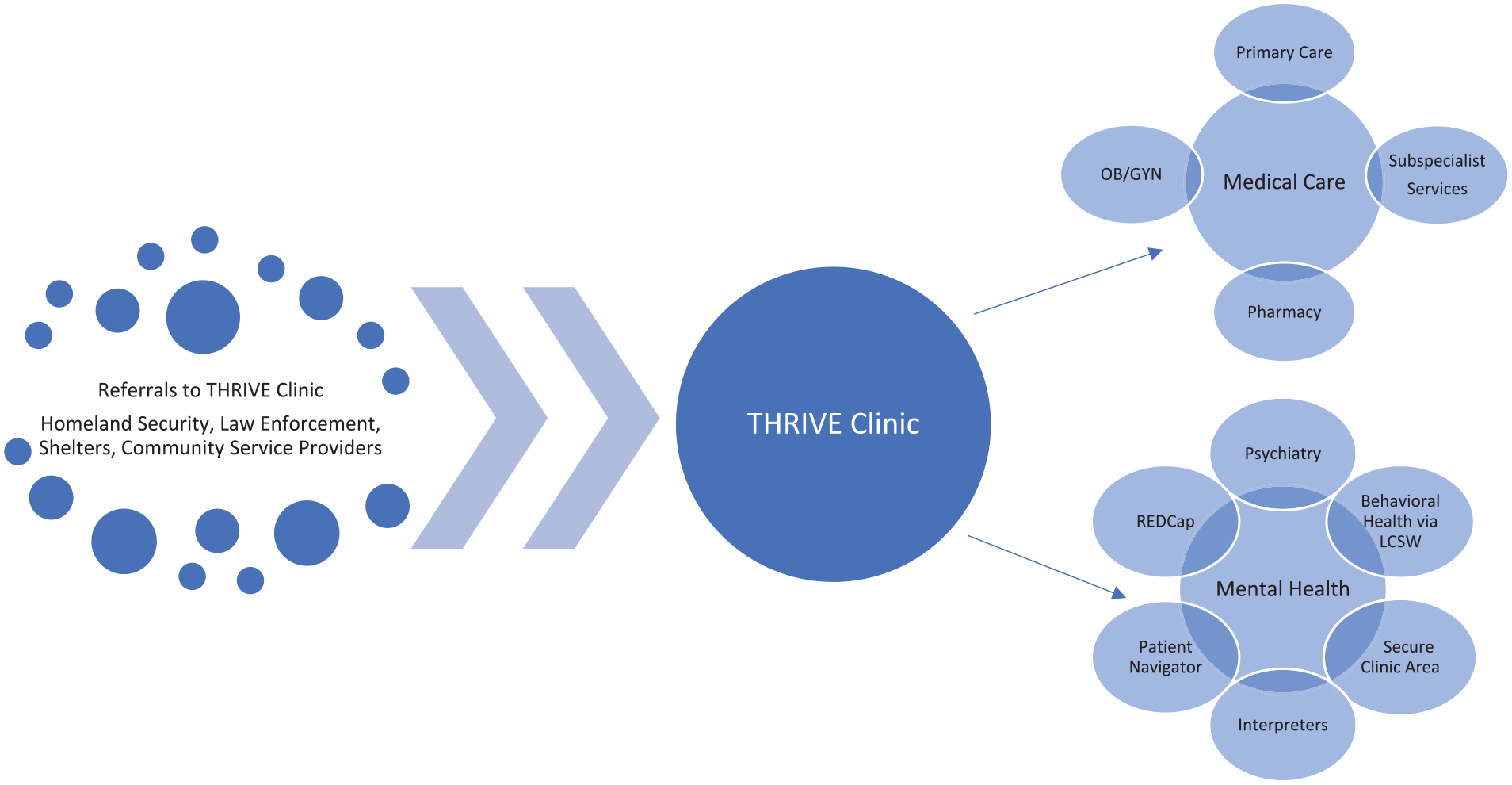
THRIVE (Trafficking, Healthcare, Resources, and Interdisciplinary Victim Services and Education) Clinic health care model for victims of human trafficking. Survivors enter the THRIVE Clinic through referrals from multiple sources for physical and mental health care services. Several measures are included to ensure a patient’s mental health is taken into consideration and services are trauma informed, including having a patient navigator, access to interpreters, and special intake procedures to reduce the retraumatization of patients having to retell their trafficking history. This model includes using REDCap—a dedicated, patient-centered, trauma-informed, secure, interactive clinical database shared across specialty providers and a clinic location in a secure area with special accommodations to increase survivor privacy, minimize wait times, and expedite patient registration. Abbreviations: LCSW, licensed clinical social worker; OB/GYN, obstetrics/gynecology.
The THRIVE Clinic has a comprehensive interdisciplinary model of care with core specialties of primary care, obstetrics, gynecology, and psychiatry. Specialty care consultations are provided on site at the clinic to minimize navigation in unfamiliar places. An on-site pharmacy provides medication for free or on a sliding fee scale. The clinic is located in a secured area with special accommodations to increase victim privacy, minimize wait times, and expedite patient registration. Special intake procedures, including use of a shared clinical database for all providers, including medical, legal, and social services providers, reduces the retraumatization that can occur when victims retell their trafficking history. Telephone interpreter services are accessible 24 hours per day, 7 days per week, in more than 150 languages. Victims with hearing and visual impairment have access to an audiovisual conferencing interpreting system. The patient navigator accompanies victims during their outpatient visits, coordinates their care, provides supportive services, and maintains regular communication to ensure access to care. In January 2020, a faculty psychiatrist initiated a formal residency rotation for senior psychiatry residents and fellows. Patients with psychiatric and psychological challenges engage with the psychiatry team to create a treatment plan focused on behavioral/emotional issues and medication management. A social worker works with the health care team and patient to address emotional/behavioral issues with a treatment plan designed to create better coping and problem-solving skills. Collaboration with public health, legal, and social services is important for victims as they navigate reintegration into society. Developing these community partnerships involves discussions of the best way to collaborate to provide victim services that ideally serve the patients. Memorandums of understanding between organizations are established to share information and avoid duplication of services.
The PATH Collaborative, Houston
The PATH Collaborative is a community-based system designed to provide victims of human trafficking with immediate avenues to integrated health services addressing their unique biopsychosocial needs while also promoting awareness and competency among health care providers in caring for these victims. The PATH Collaborative brings together the elements of local advocacy with Doctors for Change, an organization focused on community health through research, education, collaboration, and advocacy; a specialized program for trafficking victims in one of the nation’s largest patient-centered medical homes, Baylor College of Medicine’s Anti-Human Trafficking Program (BCM-AHTP); one of the widest faith-based health networks, CommonSpirit Health; and a community indigent care clinic for uninsured people, San Jose Clinic, to bridge issues of awareness and access in the health care setting.27,38
The dual mission of the PATH Collaborative—health care intervention and advocacy—is accomplished by codifying a network in which all participant health systems are trafficking informed by trainings headed by Doctors for Change and an integrated referral pathway for identified trafficking victims. The BCM-AHTP, based in Ben Taub Hospital, specializes in stabilization and case management and receives referrals from San Jose Clinic, CommonSpirit Health hospitals in the region, and the Harris Health System. Beyond the acute care setting, for people experiencing homelessness or residents of Harris County, the Harris Health System, the county hospital, provides access to 23 primary care centers, 5 same-day clinics, 7 specialty clinics, and 2 major hospitals. For people who are otherwise uninsurable, San Jose Clinic offers primary care, specialty care, and dental, diagnostic, and pharmacy services in a single facility. Funding includes awards from the OVC and Catholic Health Initiatives National Foundation. Coverage options for both medical and psychiatric care require a network of partners who communicate effectively and prioritize the needs of patients first. From October 2017 through September 2021, the PATH Collaborative received 560 suspected trafficking referrals, 400 of which screened positive for labor or sex trafficking.
Beyond the health care setting, the PATH Collaborative provides community leadership and coalition building through the endeavors of CommonSpirit Health and Doctors for Change. Part of CommonSpirit Health, St. Luke’s Hospital’s Houston Area Health Care Consortium brings together health care professionals across disciplines and clinical settings to collaborate with municipal leaders, nongovernmental organizations, survivor leaders (incorporating survivor experience and leadership), and prosecution and law enforcement allies. The PATH Collaborative partners with consortium members including Physicians for Human Rights to provide evaluations for asylum and expert work on civil and criminal cases for trafficking survivors. Furthermore, with guidance from its Anti-Human Trafficking Committee, Doctors for Change has taken the lead in educating partners in the Houston community with the mission of ending human trafficking in Houston and beyond.
Lessons Learned
THRIVE Clinic
The THRIVE Clinic was established to operate daily to ensure access to care and treatment; outpatient appointments are available within 24-48 hours. A patient navigator was hired to accompany patients on the medical campus to alleviate 2 major obstacles patients encountered: navigating the health care system and registering in the clinic for an appointment. Without safe housing and transportation, patients struggle with adherence to health care plans. The THRIVE Clinic team provides safe transportation to and from the clinic and establishes community partnerships with local shelters to identify safe and appropriate housing; however, finding housing is difficult because homelessness is a major problem in south Florida. Because of the complex health care needs of trafficking victims, a navigator or case manager is essential to assist patients with follow-up. The patient navigator, social worker, or nurse is on call every day to assist victims during off hours.
Many victims have issues with identification because they have crossed state or country borders. As such, working with law enforcement and legal services helps patients establish a safety plan, identification, and access to health care services. Obtaining medical services requires patient identification, and, with documentation from law enforcement that the patient is a victim of human trafficking, patients meet with a financial counselor to fast track their ability to obtain services. Patients work with the social worker to identify resources for health insurance coverage. Creating long-term psychiatric and mental health services has been difficult but was recently expanded to include a robust team of mental health providers.
Having a consistent team of medical, legal, and social service providers who provide trauma-informed care is essential. Creating a network of health care providers, including subspecialists to consistently serve THRIVE Clinic patients, is necessary for victims to build trust. Gastroenterology and neurology are 2 specialty care services that victims need the most because of health consequences from injuries and trauma, including head injuries, seizures, chronic headaches, and eating disorders. Health care providers, including subspecialists, come to the same THRIVE Clinic to provide care, and this approach provides stability and a sense of safety for the victim. THRIVE Clinic patients are typically afraid to use emergency department services because traffickers take their victims there for acute care. As a result, the THRIVE Clinic partnered with the emergency department to decrease retraumatization. Upon arrival at the emergency department, victims are escorted to a private and secure area for examination.
Incorporating survivor experience and leadership is part of building the model at THRIVE Clinic, and peer-to-peer mentorship, which may decrease recidivism rates, is available for patients. A need exists for vocational training and academic scholarships to assist victims with job training and education. The key to building community partnerships is learning the landscape of victim services in the city, identifying available services, creating collaborations, and identifying gaps in care and ways to address them to create a streamlined network for patients to access victim services including health care.
PATH Collaborative
Establishing a collaborative citywide model in Houston required learning the victim services landscape of the city, services offered, and gaps in services as well as working with community partners to ensure victims can access all services needed for long-term healing and recovery. The BCM-AHTP was established to provide trafficking-tailored stabilization and case management and, from this experience, program literature on the best mental health practices for victims of human trafficking have been published.27,35,39 Medical referrals for patients living in Harris County were made to the Harris Health System for primary care and other health care services. Part of building this collaborative model was finding a medical home for uninsured patients and patients not living in Harris County. We met with several medical homes in Houston that provided care for vulnerable populations (eg, economically disadvantaged and uninsured populations, victims of abuse) before finding San Jose Clinic. In addition, the Healthcare Consortium worked to build community partnerships to ensure safe housing, transportation, identification, health insurance, vocation services, peer-to-peer mentorship, and medical–legal services.
Building a Sustainable Model
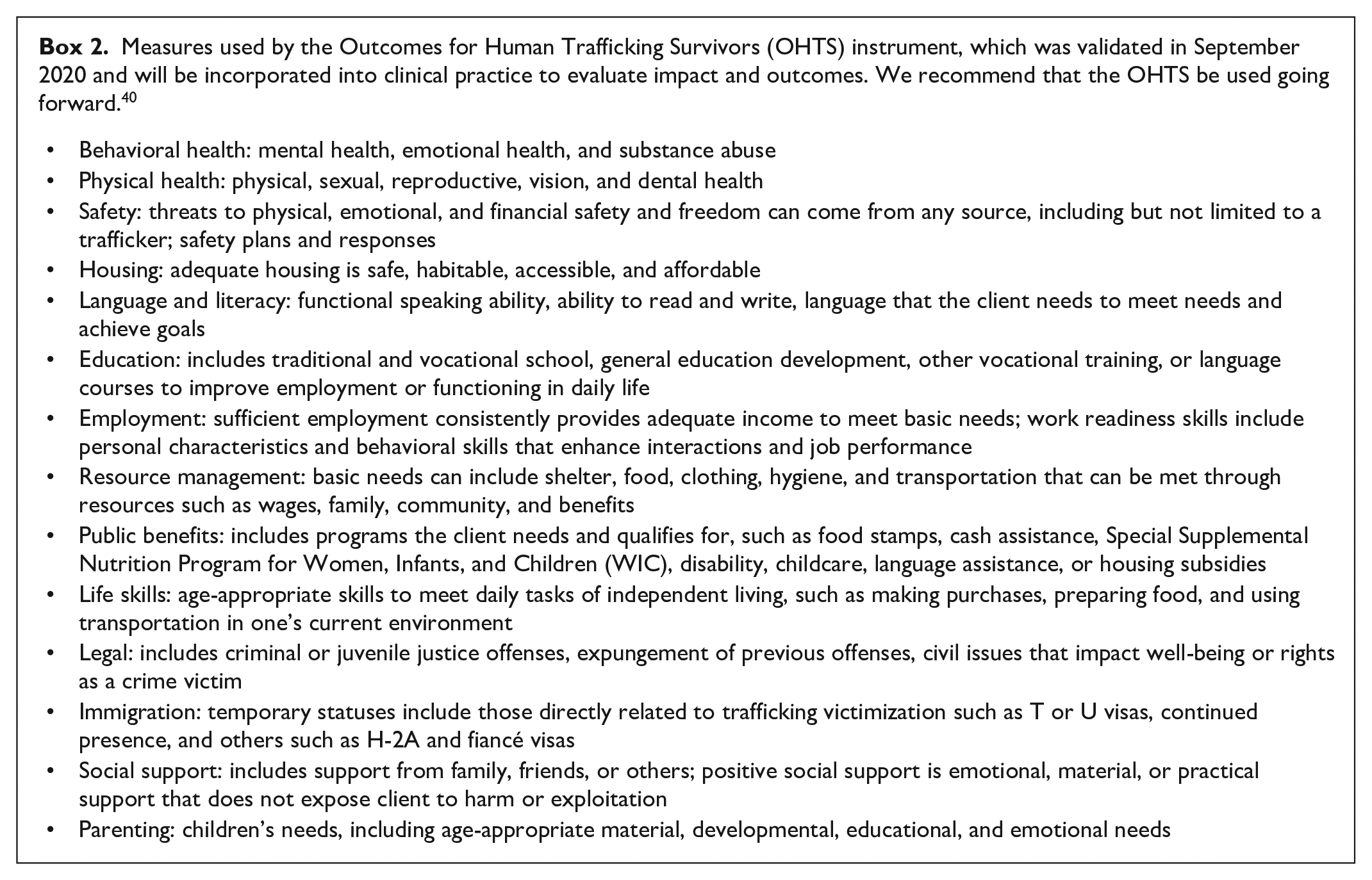
The goal for each community in which citywide preventive and rehabilitative human trafficking health care models are implemented is to create a system that streamlines victim services that are trauma-informed, interdisciplinary, and survivor-informed. By combining physical, mental, and social health care into a reliable medical home for victims, healing from trauma can be maximized to ensure victims of trafficking can effectively rehabilitate and successfully reintegrate into society. Critical to meeting that goal for as many victims as possible is to create a model that is both sustainable and replicable (Figure 2). The models discussed in this article are purely descriptive; outcome data are forthcoming. Data were collected on various aspects of the program and patients (Box 1) because no validated tools were available when these programs were initiated. Recently, the Outcomes for Human Trafficking Survivors instrument was validated and will be incorporated into clinical practice to formally evaluate impact and outcomes (Box 2). 40 Currently, a similar model is being established in Atlanta, Georgia. Two medical homes have been identified in Atlanta: a federally qualified health center for adults and children and a medical home for the lesbian, gay, bisexual, transgender, queer and/or questioning, intersex, and asexual and/or ally+ community. Collaborations with the Georgia Statewide Human Trafficking Task Force, family planning clinics, and local organizations for mental health care services, transitional housing and vocational services, medical–legal with pro bono legal services, and organizations serving non–US-born victims have been established. Establishing these collaborations required meeting with partners, understanding the victim services available and gaps in care, and addressing ways to streamline services for victims.
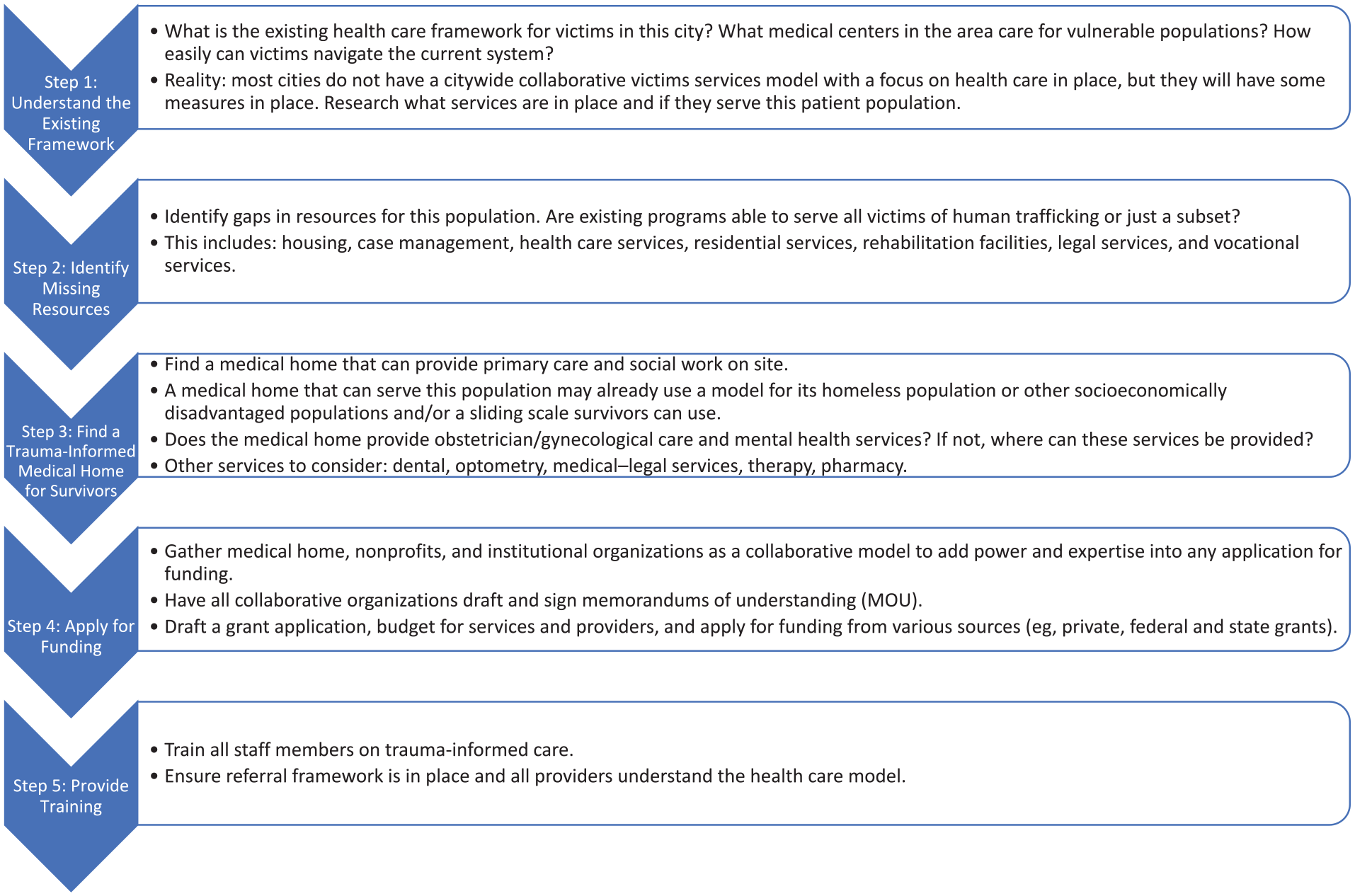
Steps to creating a sustainable, collaborative, trauma-informed, citywide victim services model with a focus on health care for victims of human trafficking.
Data to be reported for THRIVE Clinic and the PATH Collaborative to evaluate demographic characteristics of the patient population, health consequences of human trafficking, number of patients served and resources used, and the effectiveness of interventions for the patients and in the community.
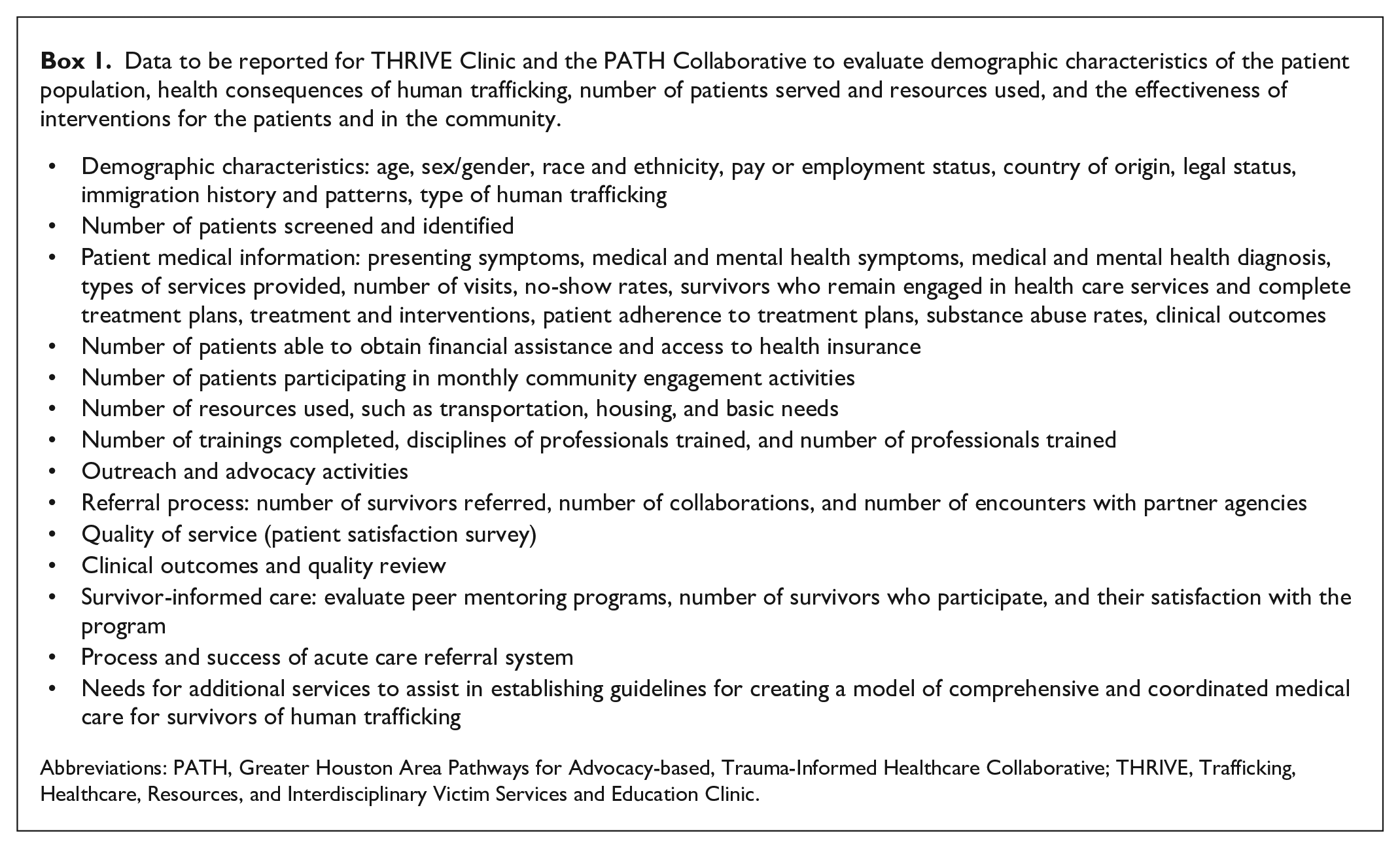
Abbreviations: PATH, Greater Houston Area Pathways for Advocacy-based, Trauma-Informed Healthcare Collaborative; THRIVE, Trafficking, Healthcare, Resources, and Interdisciplinary Victim Services and Education Clinic.
Measures used by the Outcomes for Human Trafficking Survivors (OHTS) instrument, which was validated in September 2020 and will be incorporated into clinical practice to evaluate impact and outcomes. We recommend that the OHTS be used going forward. 40
Sustainability of this model depends on funding opportunities through local, state, and federal grants such as the OVC. Private and institutional donors can also serve as sources of revenue. To build a sustainable, trauma-informed model, salaried positions for service providers need to be factored in the budget, which will ensure continuity of care, an important component of trauma-informed care. In addition to securing funding, sustainability is also achieved through finding programs, medical centers, and nonprofit organizations in the city or community that have existing resources and experience serving vulnerable populations. These programs are best able to incorporate victims of human trafficking into their existing medical framework, have a referral network in place, and have the infrastructure needed to apply for large grants. Replicability of the model ensures not only that a sustainable model can be built in a given city but that a similar, streamlined model can be built in any new city or community where human trafficking is an endemic problem. Although the model will differ slightly in each city based on the city’s programs and resources, this framework can guide efforts through important steps and considerations that have led to successful models in other large cities.
Athough the interdisciplinary models presented here are descriptive, and we did not evaluate the impact and outcomes of the programs, this article contributes to the literature on the health care needs and consequences of trafficking and provides an overview of program development and implementation. Further research is needed to understand the detrimental health effects of trafficking, develop optimal models and standard of care for recovery and reintegration for this patient population, and address public health, legal, and medical policy to ensure patient access to comprehensive, trauma-informed, interdisciplinary victim services.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.