
Abstract
Objectives
Increasing knowledge about the toxicology of drug overdose and substance misuse (DOSM) is important in improving our understanding of the epidemic. We describe the Minnesota Drug Overdose and Substance Use Pilot Surveillance Activity, which started collecting data on emergency department (ED) visits attributable to DOSM in 2017, with a focus on the toxicology results of a subset of clinical encounters.
Methods
From November 1, 2017, through January 30, 2020, we collected near–real-time data on DOSM-related ED encounters. The Minnesota Department of Health Public Health Laboratory tested leftover clinical specimens (blood and/or urine) for the presence of various substances for patients who died, were hospitalized, had an atypical clinical presentation, or were part of a local drug overdose cluster. Testing looked for >250 drugs or their metabolites, including those commonly misused (eg, methamphetamine, cocaine), prescription medications, synthetic cannabinoids and cathinones, and opioids. We describe characteristics of the overall group and a subgroup of clinical encounters with toxicology results.
Results
Specimens submitted from 6 EDs during the study period represented 239 clinical encounters. Methamphetamine was the most frequently detected substance (67.4%) but was suspected in only 45.6% of encounters. At least 1 opioid was detected in 42.5% of encounters but suspected in only 29.7%. Testing also detected potential adulterants and additives (eg, fentanyl, fentanyl analogues, levamisole) and showed frequent patient exposure to substances not reported by patients or suspected by clinicians. Nearly half (44.4%) of clinical encounters had >1 substance detected.
Conclusions
ED surveillance for DOSM encounters, enhanced by toxicology testing, can provide local situational awareness on overdoses, prevent potential mischaracterization of the true drug overdose epidemic, and inform harm reduction and drug overdose prevention efforts.
The drug overdose epidemic has evolved in recent years. Once attributed to opioids, the epidemic is now one of polysubstance use. Growing numbers of drug overdose deaths have multiple substances detected by toxicology testing. 1,2 In addition, an increasing number of emergency department (ED) visits due to overdose involve multiple drugs or substances. 1,3
Although much research has examined overdose deaths and the contributing substances, literature on the toxicology of nonfatal overdoses is limited. Toxicology data from nonfatal overdose events are lacking for various reasons, including limited toxicology testing in hospital settings and the expense and availability of testing, particularly if results will not change clinical care. 4 -9
Examination of ED visits and hospitalizations due to nonfatal drug overdose or substance misuse (DOSM) and their toxicology results elucidates a broader and more complex picture of the drug overdose epidemic than is apparent when the focus is solely on fatal overdoses. Enhanced toxicology testing can inform public health practitioners, health care providers, and the public about substances circulating in communities, including the presence of novel or highly potent substances. These data allow public health agencies to monitor trends of specific substances and identify substances that are causing clusters of overdoses or severe illness.
To better understand ED visits and hospitalizations attributable to DOSM, the Minnesota Department of Health (MDH) developed the Minnesota Drug Overdose and Substance Use Pilot Surveillance Activity (MNDOSA). This surveillance system uses real-time reporting of ED visits, enhanced toxicology testing of clinical specimens, and medical record data collection to describe trends in ED visits and hospitalizations due to DOSM.
Methods
MNDOSA data collection began at 2 EDs in Northern Minnesota in November 2017. In 2019, four additional EDs in Northern Minnesota began collecting data. We used data collected from November 1, 2017, through January 30, 2020, for this analysis, although data collection is ongoing. All participating EDs were within a 60-mile radius serving similar patient populations. We selected participating sites on the basis of preexisting relationships between ED clinicians and MDH. ED staff members submitted case reports to MDH for all fatal and nonfatal clinical encounters attributable to DOSM treated at the participating ED. This pilot surveillance activity examined trends in drug or substance use without self-injurious intent (referred to by some researchers, health professionals, and others as “recreational use”). The case definition for an encounter was whether the patient’s presenting signs and symptoms were attributable to DOSM, as determined by the clinician. The case definition excluded suicide attempts or self-harm, unintentional ingestion (eg, a child ate a cannabis-laced cookie), unintentional overmedication, assault (eg, a date rape drug was administered to incapacitate the patient), or if alcohol was the only substance suspected. We excluded encounters due to alcohol use alone to limit the reporting burden on participating EDs. We received 651 case reports for MNDOSA encounters, of which 16 encounters were excluded: 13 were ED visits due to suicide attempts, 2 were for unintentional ingestion, and 1 was for assault. We analyzed the remaining 635 encounters to describe ED visits and hospitalizations attributable to DOSM.
Case reports included information about patient demographic characteristics and suspected drug(s) or substance(s). Information on suspected drug(s) or substance(s) came from patient self-report or clinician judgment based on the patient’s signs and symptoms, particularly in cases in which the patient was unable to or declined to report the substance(s) used. Information about suspected drug(s) may have also been informed by hospital toxicology testing, although the extent to which this information was derived from toxicology testing is unclear. Case reports also included information about whether the following had happened to the patient: died, was hospitalized, had an atypical clinical presentation (ie, unusual signs or symptoms for the suspected substance, as determined by the clinician), or was part of a local cluster of drug overdoses (ie, multiple patients with similar signs and symptoms presenting to the same ED within a short time frame). We reviewed medical records for the subset of patients meeting these criteria (hereinafter, the “subgroup”). Data collected included length of hospitalization, admission to the intensive care unit (ICU), endotracheal intubation, prescription medications, and medications administered in the ED or hospital. If leftover clinical specimens were available for patients in the subgroup, ED staff members sent the specimens to the MDH Public Health Laboratory (PHL) for expanded toxicology testing.
The MDH PHL is 1 of 10 Level 1 laboratories in the national Laboratory Response Network tasked with identifying chemical substances of public health importance. 10 Using Laboratory Response Network resources, the MDH PHL developed the capability to perform expanded toxicology testing on clinical specimens.
MDH PHL staff members analyzed blood and urine specimens using liquid chromatography–tandem mass spectrometry. The targeted testing looked for >250 drugs or their metabolites, including those commonly misused (eg, methamphetamine, cocaine), prescription medications, synthetic cannabinoids and cathinones, and opioids. When the MDH PHL detected a substance indicated by the medical record to be a prescription or medication administered for acute care, we removed the result from statistical analysis of the subgroup. Medications commonly removed were benzodiazepines administered in the ED and prescribed methadone. From the subgroup, we removed 18 opioid-positive results, 4 fentanyl-positive results, and 42 benzodiazepine-positive results (Figure).
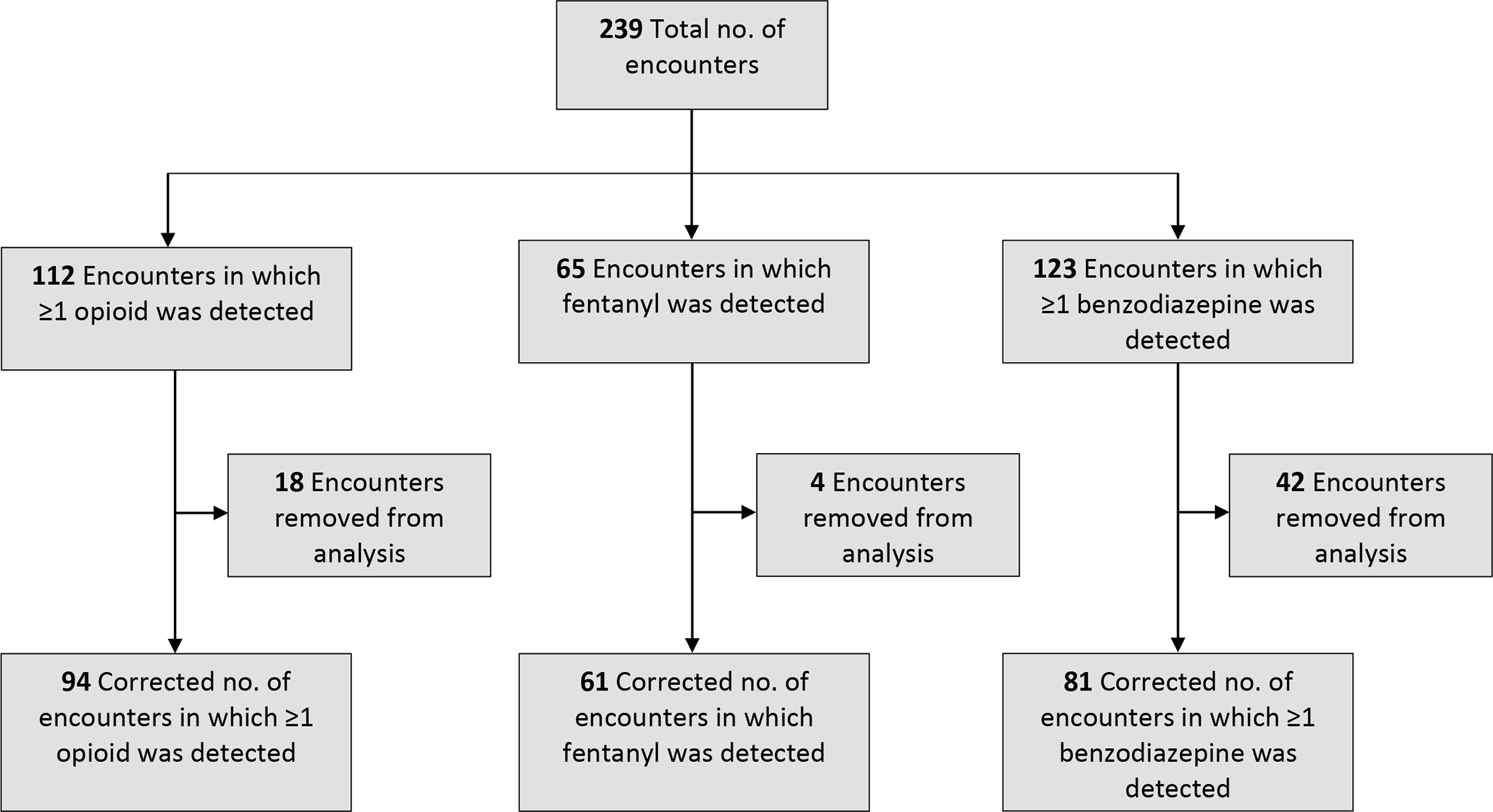
Substances detected by Minnesota Drug Overdose and Substance Use Pilot Surveillance Activity (MNDOSA) toxicology testing, including those indicated in the medical record to be a prescription or medication administered for acute care, Minnesota, 2017-2020. All data are from the MNDOSA. An encounter was removed from analysis if the medical record indicated the substance detected was a prescription or administered for acute care.
The term “clinical encounter” is the predominant unit of measurement in this analysis because it allows for the inclusion of individual patients more than once in the data. Patients who presented to participating EDs multiple times and whose clinical specimens were analyzed for >1 encounter are represented as separate encounters in our analysis.
We performed descriptive analyses for the overall group and the subgroup of clinical encounters with toxicology results. We used SAS version 9.4 (SAS Institute, Inc) for all analyses. We used Pearson χ2 and Fisher exact tests to detect significant differences among various patient groups, with P < .05 considered significant. Statistical analyses of drug types focused on commonly misused drugs or substances, including methamphetamine, opioids (including fentanyl), marijuana, cocaine, synthetic cannabinoids and cathinones, and suspected adulterants. An adulterant is an ingredient added to a substance either intentionally or unintentionally and may be added for various reasons, including to increase the effects of the drug or to extend the supply by mixing the drug with a less expensive substance. MNDOSA was designated as a public health practice activity under Minnesota statute; because surveillance data were not considered research, institutional review board review was not required.
Results
The median age of all patients was 32 years (range, 12-71 years), and 395 patients (62.2%) were male (Table 1). Most patients were White (57.2%), followed by American Indian/Alaska Native (14.5%). Five patients (0.8%) died and 252 (39.7%) were hospitalized.
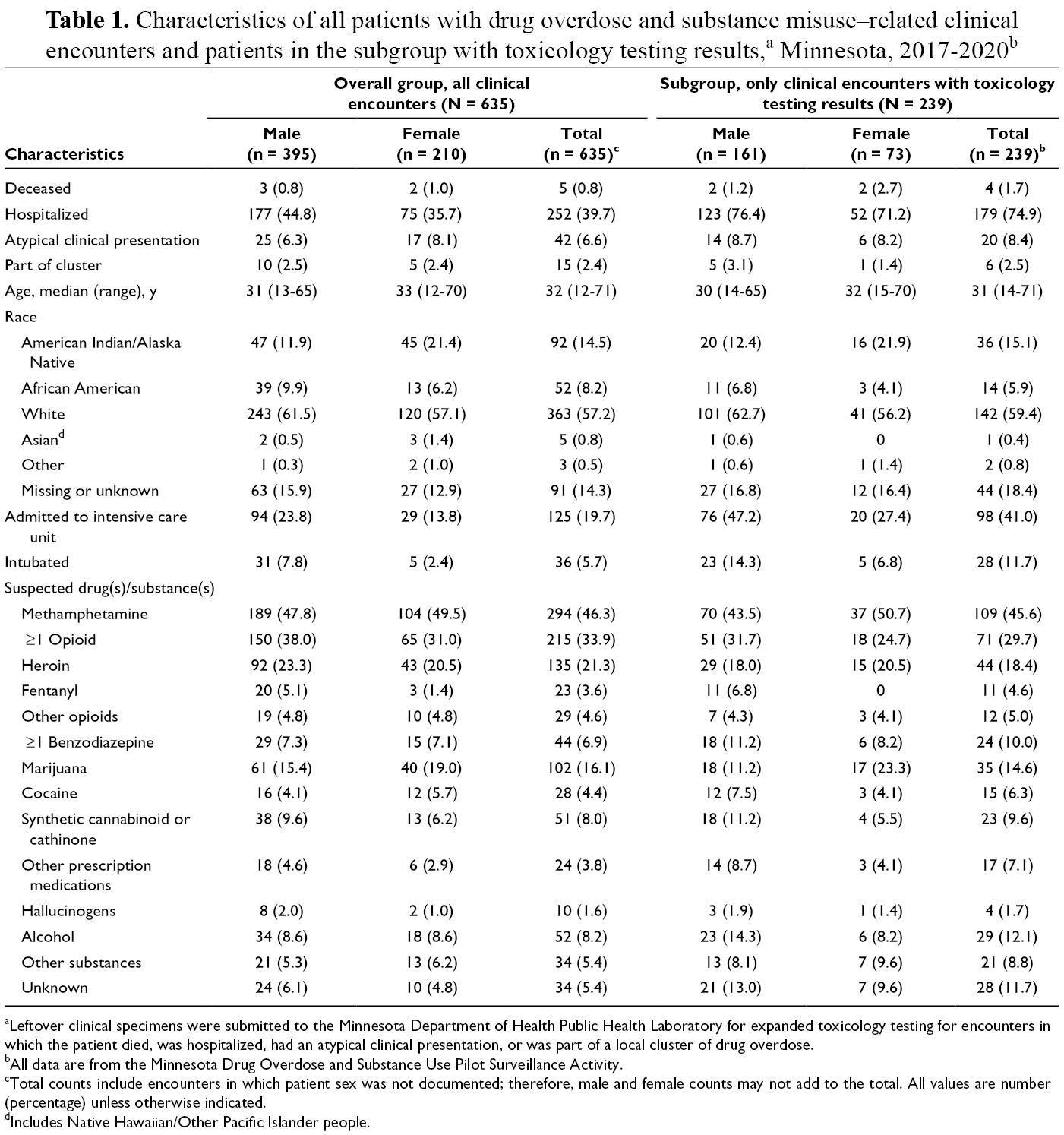
aLeftover clinical specimens were submitted to the Minnesota Department of Health Public Health Laboratory for expanded toxicology testing for encounters in which the patient died, was hospitalized, had an atypical clinical presentation, or was part of a local cluster of drug overdose.
bAll data are from the Minnesota Drug Overdose and Substance Use Pilot Surveillance Activity.
cTotal counts include encounters in which patient sex was not documented; therefore, male and female counts may not add to the total. All values are number (percentage) unless otherwise indicated.
dIncludes Native Hawaiian/Other Pacific Islander people.
The subgroup consisted of data from 239 encounters and was demographically similar to the overall group (Table 1). The median age of subgroup patients was 31 years (range, 14-71 years), and 161 patients (67.4%) were male. Most patients in the subgroup were White (59.4%), followed by American Indian/Alaska Native (15.1%). Four patients (1.7%) in the subgroup died and 179 (74.9%) were hospitalized.
The most frequently detected substances in clinical encounters in the subgroup were caffeine (94.6%), cotinine (a metabolite of nicotine; 94.6%), amphetamine (70.6%), and methamphetamine (67.4%). After methamphetamine, the most frequently detected misused substances were opioids (42.5%), benzodiazepines (41.1%), marijuana (39.3%), fentanyl (26.0%), cocaine (13.4%), and synthetic cannabinoids or cathinones (4.6%) (Table 2). We found no significant differences by gender when stratified by substance. A higher percentage of African American patients than patients in other racial groups had a positive result for cocaine. A higher percentage of patients aged 32-42 years than patients in other age groups were positive for methamphetamine. Compared with patients not admitted to the ICU, patients admitted to the ICU were significantly more likely to test positive for ≥1 opioid (P = .003), fentanyl (P = .03), ≥1 benzodiazepine (P = .047), cocaine (P = .014), or a synthetic cannabinoid or cathinone (P = .02). Intubated patients were significantly more likely than patients who were not intubated to test positive for ≥1 opioid (P = .004) or ≥1 benzodiazepine (P = .048).
Characteristics of clinical encounters with enhanced toxicology results, by detected substance, Minnesota, 2017-2020 a
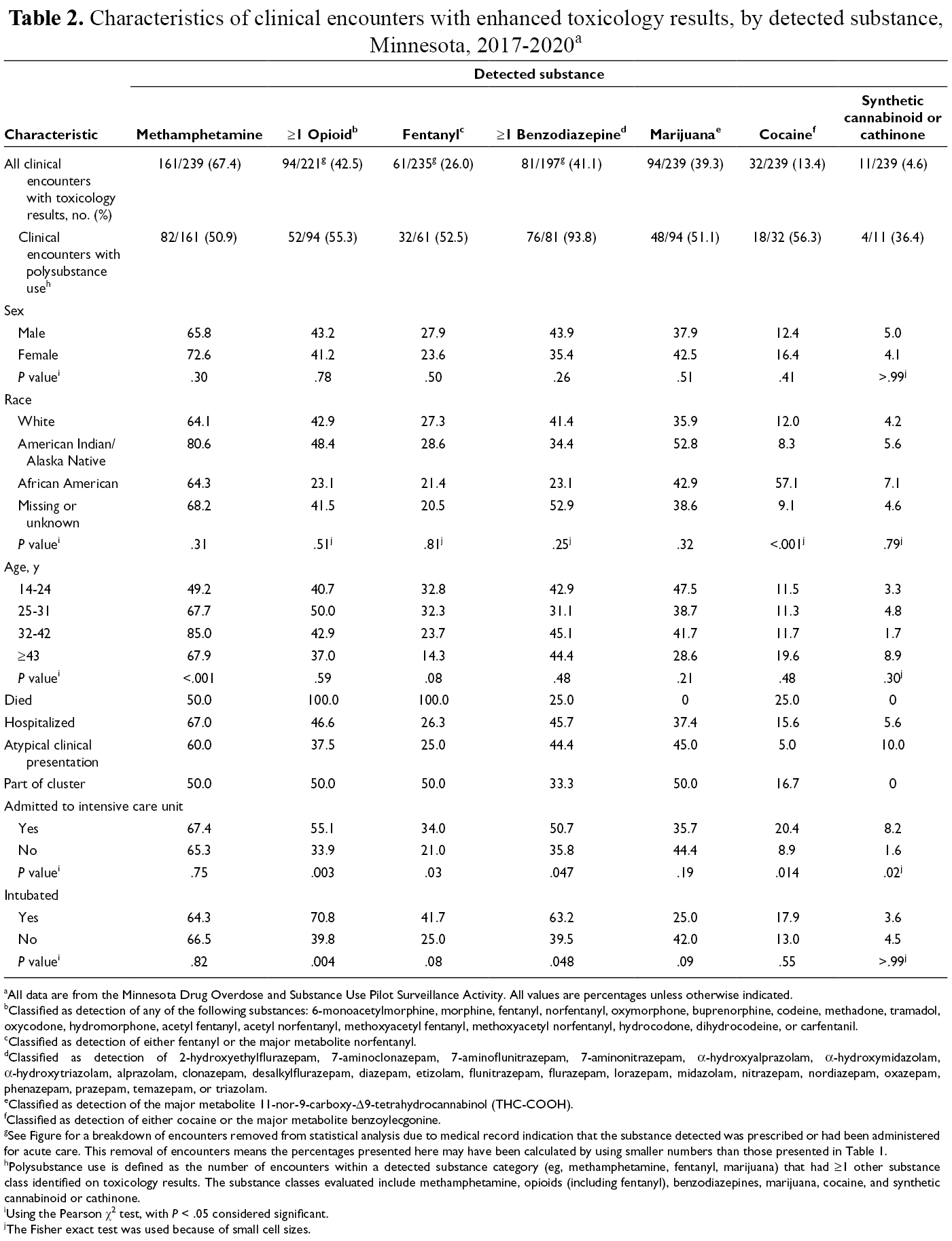
aAll data are from the Minnesota Drug Overdose and Substance Use Pilot Surveillance Activity. All values are percentages unless otherwise indicated.
bClassified as detection of any of the following substances: 6-monoacetylmorphine, morphine, fentanyl, norfentanyl, oxymorphone, buprenorphine, codeine, methadone, tramadol, oxycodone, hydromorphone, acetyl fentanyl, acetyl norfentanyl, methoxyacetyl fentanyl, methoxyacetyl norfentanyl, hydrocodone, dihydrocodeine, or carfentanil.
cClassified as detection of either fentanyl or the major metabolite norfentanyl.
dClassified as detection of 2-hydroxyethylflurazepam, 7-aminoclonazepam, 7-aminoflunitrazepam, 7-aminonitrazepam, α-hydroxyalprazolam, α-hydroxymidazolam, α-hydroxytriazolam, alprazolam, clonazepam, desalkylflurazepam, diazepam, etizolam, flunitrazepam, flurazepam, lorazepam, midazolam, nitrazepam, nordiazepam, oxazepam, phenazepam, prazepam, temazepam, or triazolam.
eClassified as detection of the major metabolite 11-nor-9-carboxy-Δ9-tetrahydrocannabinol (THC-COOH).
fClassified as detection of either cocaine or the major metabolite benzoylecgonine.
gSee Figure for a breakdown of encounters removed from statistical analysis due to medical record indication that the substance detected was prescribed or had been administered for acute care. This removal of encounters means the percentages presented here may have been calculated by using smaller numbers than those presented in Table 1.
hPolysubstance use is defined as the number of encounters within a detected substance category (eg, methamphetamine, fentanyl, marijuana) that had ≥1 other substance class identified on toxicology results. The substance classes evaluated include methamphetamine, opioids (including fentanyl), benzodiazepines, marijuana, cocaine, and synthetic cannabinoid or cathinone.
iUsing the Pearson χ2 test, with P < .05 considered significant.
jThe Fisher exact test was used because of small cell sizes.
Most substances were detected by toxicology testing more frequently than were suspected by the clinician or reported by the patient (Tables 1 and 2). Methamphetamine was suspected in 45.6% of encounters but detected in 67.4% of encounters, and ≥1 opioid was suspected in 29.7% of encounters but detected in 42.5% of encounters. Toxicology testing results also found evidence of polysubstance use more frequently than was suspected or indicated on case reports. When looking only at the drug types methamphetamine, opioids (including fentanyl), marijuana, cocaine, and synthetic cannabinoids and cathinones, >1 drug was suspected in 27.2% of subgroup encounters but was detected in 44.4% of subgroup encounters (data not shown). Among clinical encounters in which methamphetamine was suspected to have been at least 1 of the drugs of exposure, methamphetamine was detected in 90.8%, ≥1 opioid was detected in 38.6% (including fentanyl in 23.9%), and ≥1 benzodiazepine was detected in 47.1% of encounters (Table 3). Among encounters in which opioids were suspected, ≥1 opioid was detected in 86.4%, methamphetamine was detected in 73.2%, fentanyl was detected in 69.1%, and ≥1 benzodiazepine was detected in 40.0% of encounters.
Suspected and detected substances among clinical encounters with enhanced toxicology results, Minnesota, 2017-2020a
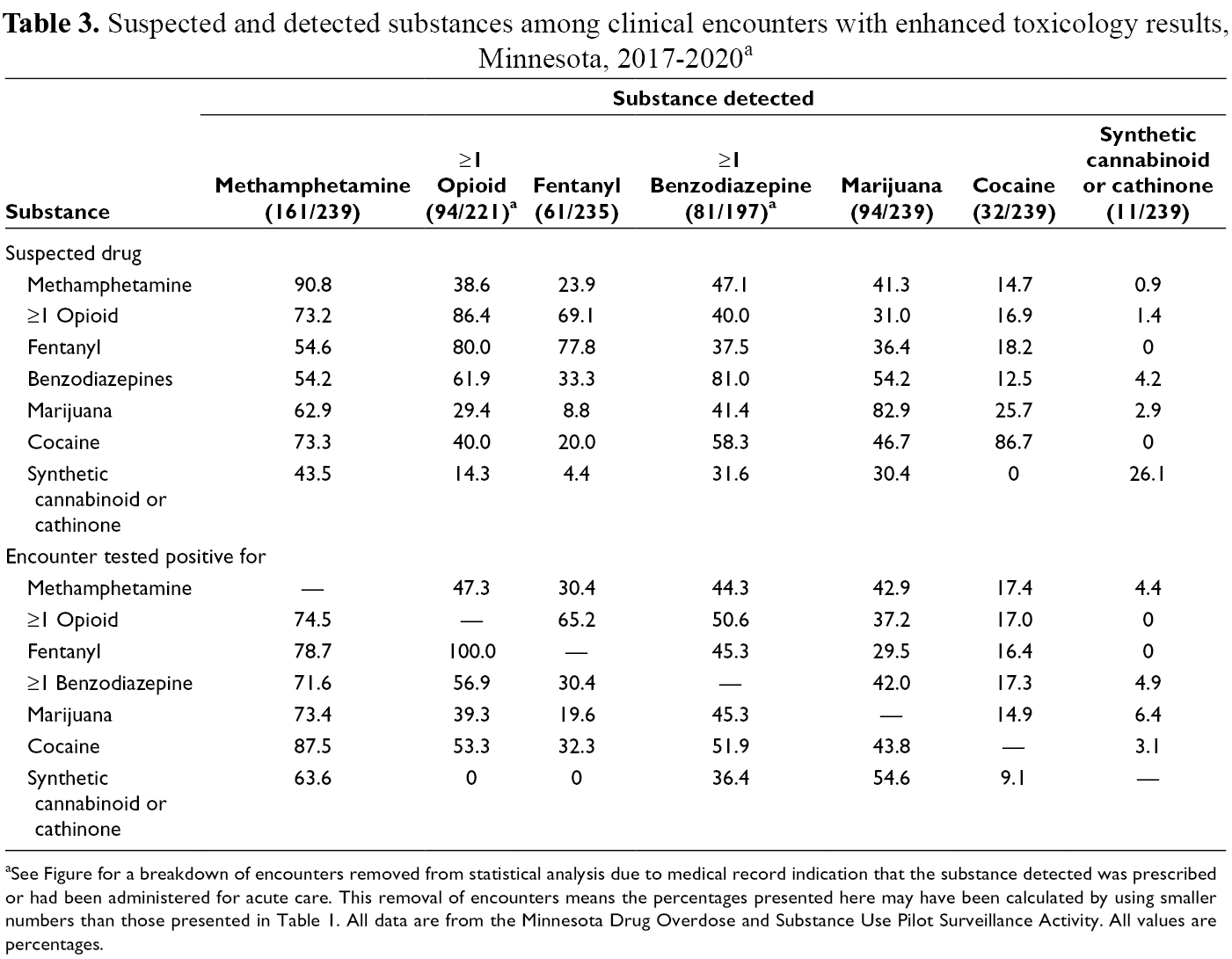
aSee Figure for a breakdown of encounters removed from statistical analysis due to medical record indication that the substance detected was prescribed or had been administered for acute care. This removal of encounters means the percentages presented here may have been calculated by using smaller numbers than those presented in Table 1. All data are from the Minnesota Drug Overdose and Substance Use Pilot Surveillance Activity. All values are percentages.
In addition to analyzing specimens for commonly misused drugs or substances, toxicology testing looked for known or suspected adulterants, including fentanyl and fentanyl analogues. Fentanyl may have been used intentionally by patients, in which case it would not be considered an adulterant; however, it was considered an adulterant if it was not listed as a suspected drug on the case report form. Of the 61 encounters in which fentanyl was detected, it was not indicated on the case report form for 54 (89%) encounters. In addition to fentanyl, 3 fentanyl analogues were detected: acetylfentanyl, methoxyacetylfentanyl, and acrylfentanyl. Other potential adulterants were also identified. For example, levamisole was detected in a small percentage of specimens, most of which were also positive for cocaine.
Discussion
MNDOSA toxicology testing indicates patient exposure to multiple drugs and substances not reported by patients or suspected by clinicians. To our knowledge, this is the first analysis to compare suspected substances with detected substances. Although previous studies have examined polysubstance use as detected by toxicology testing, these data have not been compared with substances to which patients were suspected to have been exposed. 1,11,12
Except for synthetic cannabinoids and cathinones, commonly misused drugs were detected by toxicology testing more frequently than they were suspected. Methamphetamine was the most frequently detected substance, which is consistent with reports of common methamphetamine use in this region of the state.
MNDOSA data paint a different picture than hospital discharge data for nonfatal drug overdose ED visits. This traditional surveillance method, based on discharge diagnosis codes rather than extensive toxicology testing, 13 showed that from 2018 to 2019, opioids (n = 268) were the most frequently implicated substances in ED visits in the area served by the pilot EDs, followed by benzodiazepines (n = 58), stimulants (n = 52), cannabis (n = 26), synthetic drugs (n = 12), and cocaine (n = 3). The ED visits described in hospital discharge data were not mutually exclusive; multiple substances implicated in the same ED visit would be included in the count for each substance, thus failing to summarize information on polysubstance use. The comparison of overdose trends captured by MNDOSA with overdose trends captured by traditional surveillance methods emphasizes the discrepancies in data collected by various surveillance methods, likely due to challenges inherent in diagnosis coding. This finding highlights the need to supplement traditional surveillance methods with toxicology testing of health care encounters for DOSM to capture the larger context of DOSM trends.
The demographic characteristics of MNDOSA patients differ from characteristics of the general population in this region of Minnesota. The population in this area is predominantly White (92.2%) followed by American Indian/Alaska Native (2.7%). 14 The higher percentage of American Indian/Alaska Native patients in the MNDOSA sample compared with the general population is consistent with findings that people of color are more likely to experience drug overdose than the White population in Minnesota. 15 In 2019, American Indian/Alaska Native people in Minnesota were 7 times more likely than White people to die of a drug overdose. Although these disparities in drug overdoses are seen in many states, Minnesota has one of the worst race rate disparities in fatal overdoses in the United States. 15
Polysubstance use was common, with >1 type of drug detected in 44.4% of subgroup clinical encounters. MNDOSA’s finding of widespread polysubstance use could be attributed to 1 of 2 possibilities: (1) patients intentionally used multiple substances either concomitantly or within a short period or (2) patients unknowingly used a mischaracterized or adulterated substance. Patients may have used multiple substances for the synergistic effect created by combining substances and/or because of addiction to multiple substances. 1,2,11,16,17 Patients also may have used a substance they believed was something different than what it actually was, for example, counterfeit pills. 16 -19
It is well known that illicit drugs may be adulterated with various substances, including various types of sugars, metals, caffeine, over-the-counter products such as acetaminophen, prescription medications, or illicitly manufactured substances such as fentanyl, fentanyl analogues, or methamphetamine. 8,11,16,17,20 -23 Our analysis revealed the presence of adulterants in clinical specimens of patients presenting to the ED for DOSM. Specifically, our analysis showed that fentanyl was not suspected in most (89%) encounters in which fentanyl was detected. In addition, levamisole, a prescription medication used to treat parasitic infections, is also a known cocaine adulterant and was detected in a small percentage of specimens.
Whether patients intended to use multiple substances is unknown. Regardless, health care providers should be aware of the frequency with which multiple drug classes are involved in ED visits and hospitalizations attributed to DOSM. Clinician awareness is important given the potential for unknown interactions between substances or complications due to specific substances. 3,8,20,21
Improving the knowledge of people who use drugs about the presence of highly potent adulterants in the local drug supply is one important way surveillance data can be used to inform harm reduction strategies and reduce morbidity and mortality from DOSM. 17,20 One study showed that although a high percentage of people who use drugs had knowledge of the risk of fentanyl overdose, 72% of people perceived their personal risk to be low or nonexistent. 24 Reasons for low or no perceived risk included not intending to use opioids and trusting the person who supplied the drugs. Surveillance data incorporating toxicology testing illustrate the polysubstance nature of drugs and demonstrate the importance of carrying naloxone even among people who believe they use non-opioid substances, in case of adulteration. 1,11
To our knowledge, this pilot surveillance activity is the only one in the nation conducting expanded toxicology testing on DOSM encounters reported in near-real time. Beyond the novel analytical findings, lessons learned from the logistical implementation of MNDOSA should be considered by other jurisdictions considering implementing similar programs. Identifying site champions to advocate for and educate peers about the project was essential to MNDOSA’s success. In addition, sites had concerns about sharing private data with MDH, which staff members worked to alleviate by explaining the reasons for the data collection, the secure storage and handling of the data, and the authority of MDH to collect the data. The main challenges encountered were the logistics of case report and clinical specimen submission to MDH and clinician reminders to submit case reports for eligible patients. Site champions set up case reporting and specimen submission processes that fit within ED-specific workflows. To remind ED clinicians to submit case reports, MDH staff members analyzed site-specific data and presented the data to sites regularly; sharing data with sites incentivized reporting and informed ED staff members of patient trends.
As the MNDOSA pilot continues, efforts are underway to expand surveillance to other EDs in Minnesota to increase the representativeness of the data collected. In February 2020, an ED in the Twin Cities Metropolitan Area joined the pilot. In addition, expanding the case definition to include alcohol use may be considered as the understanding of alcohol’s role in drug overdoses increases. As MNDOSA expands to other EDs, toxicology testing may help identify clusters of DOSM by linking patients between EDs or identifying drug supplies contaminated with a particularly dangerous substance. The next steps of this project are to link the encounters with toxicology results to the encounter record in hospital discharge data to examine whether the diagnosis codes assigned were consistent with toxicology results. This linkage will provide further clarification of the extent of drug use beyond traditional surveillance methods, which will provide a more accurate representation of the epidemic in the participating region of the state.
Building a better understanding of ED visits and hospitalizations through surveillance activities such as MNDOSA can improve overdose prevention efforts. Surveillance provides timely awareness of substances involved in nonfatal overdoses and emerging trends in drug use before deaths occur. 1,12,19,25 These findings also illustrate the need for substance use treatment programs to recognize and address clients’ polysubstance use and co-occurring addictions. 2
Limitations
This analysis had several limitations. First, toxicology testing may not have identified novel substances, such as newer synthetic cannabinoids, cathinones, or fentanyl analogues. As new chemical compositions are synthesized and circulated, laboratories are challenged to keep pace, making comprehensive detection of these substances difficult. 5,6,19 Given this limitation, the percentage of positive results for synthetic cannabinoids and cathinones described here is likely an underrepresentation of the true exposure to these substances. Toxicology testing also may not have detected all substances to which patients were exposed, depending on the time between exposure and clinical specimen collection. Substances are metabolized and eliminated from the body at different rates; thus, if the substance were eliminated from the body before specimen collection, it would have been undetected in toxicology testing. Conversely, the psychoactive constituent of marijuana, tetrahydrocannabinol, may stay in the body for a longer period than other drugs, meaning marijuana can be detected for a longer time after exposure than other drugs. 26 Thus, the percentage of positive marijuana results is likely an overestimate of recent use.
Second, the reported suspected drug or substance may not have included all substances suspected in the clinical encounter. Clinicians may have suspected multiple substances but only reported one, or patients may have reported fewer drugs than they actually used. Third, toxicology testing may have detected medications that were administered for clinical care before ED arrival or were prescribed to the patient but not indicated in the medical record. Although these positive results may not indicate illicit use, they were not removed from statistical analysis if they were not listed in the patient medical record. On the other hand, a medication administered for acute care may also have been used illicitly before the overdose but was removed from the statistical analysis because it was indicated in the medical record. This situation is most likely with the combination of opioids and benzodiazepines, because both substances are used illicitly and for acute care.
Fourth, participating EDs may have underreported MNDOSA cases because of competing priorities in the ED. It is possible that not all patients who met the case definition were reported or had clinical specimens submitted; thus, these results may not be generalizable to all ED visits and hospitalizations attributable to DOSM. Fifth, the population described in this analysis is not representative of the general US population. As such, the findings are not generalizable to other communities or states.
Conclusions
MNDOSA results to date can inform harm reduction, drug overdose prevention efforts, and screening and intervention services to ensure that people with substance use disorder receive the care needed. Toxicology data provide valuable information about the drug overdose epidemic that other current methods of nonfatal overdose surveillance lack, primarily the identification of specific drugs or substances involved in clinical encounters. ED surveillance of DOSM, enhanced by laboratory characterization, can provide local situational awareness about overdoses and prevent potential mischaracterization of the true epidemic.
Footnotes
Acknowledgments
The authors thank the following people for their contributions: Deborah Anderson, PharmD, Minnesota Poison Control System; Jon Cole, MD, and Travis Olives, MD, Hennepin Healthcare and Minnesota Poison Control System; and Nicholas Van Deelen, MD, St. Luke’s Hospital.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support for this project was provided by a number of partners, including the Council of State and Territorial Epidemiologists through the Applied Epidemiology Fellowship Program and funding through the Substance Abuse/Mental Health pilot grants. In addition, the Centers for Disease Control and Prevention Enhanced State Opioid Overdose Surveillance and Overdose Prevention in States Surge Support provided funding support for this project.