
Abstract
Both the Occupational Safety and Health Administration and Washington State require safety and health protections for workers exposed to respirable crystalline silica, including tuberculosis (TB) screening as part of occupational medical surveillance. We describe the creation of a TB screening tool for silica-exposed workers receiving regulated medical surveillance examinations in Washington State. The tool provides relevant clinical recommendations to assist health care providers and public health practitioners who choose to use the tool when performing such examinations. A cross-disciplinary team at the Washington State Department of Labor and Industries created the TB screening tool to help health care providers identify silica-exposed workers who should receive a comprehensive evaluation for active TB disease and workers who should or must receive testing for latent TB infection. The Washington State Adult Tuberculosis Screening Tool for Workers Exposed to Respirable Crystalline Silica benefits occupational and respiratory clinicians and public health practitioners by aiding both the individual- and population-level delivery of occupational health and TB screening services to silica-exposed workers receiving required medical surveillance examinations.
Keywords
Silica is a common chemical compound found in many everyday substances, such as beach sand and glass. 1 Humans exposed to silica particles of the crystalline (rather than amorphous) form in sizes small enough to be inhaled (ie, respirable crystalline silica) are at increased risk of developing diseases such as silicosis, lung cancer, chronic obstructive pulmonary disease, and kidney disease. 2 More than 2500 silicosis deaths occurred in the United States from 1999 through 2018. 3 Furthermore, silicosis increases the risk of converting latent tuberculosis infection (LTBI) to active tuberculosis (TB) disease. 4 -6 The risk of developing active TB disease among people who already have LTBI also increases with exposure to respirable crystalline silica before or without the development of silicosis. 7,8
The chronic inhalation of crystalline silica leads to an excess of toxic silica particles, which often leads to apoptosis or necrosis in alveolar macrophages attempting to clear silica particles. 9,10 Silica particles are subsequently released back into the lungs, whereupon the cycle continues via uptake by other macrophages. Over time, this repeated cell death can lead to the development of nodules that are thought to be responsible for the pulmonary problems often seen among patients with silicosis. 9,10 The impairment of cell-mediated immunity is implicated in the increased risk of TB observed in workers exposed to silica. 11
Rulemaking History and the Genesis of the TB Screening Tool
Diseases in silica-exposed miners have been noted for hundreds of years. 12 Exposure to respirable crystalline silica is widespread in occupational settings in the United States and abroad, 2,13 -16 underscoring the ongoing regulatory focus on primary prevention of all silica-related diseases through improved exposure control. 17,18 In 2016, the Occupational Safety and Health Administration (OSHA) adopted a rule for occupational exposure to respirable crystalline silica, which affects an estimated 2.3 million US workers at risk of developing silica-related diseases. 18 Examples of job types and tasks in which silica exposure may occur include, but are not limited to, concrete workers, construction workers conducting demolition, and certain heavy equipment operators. 18 OSHA’s 2016 final rule amended the previously adopted permissible exposure limit and included requirements for exposure assessment, methods for controlling exposure, respiratory protection, medical surveillance, hazard communication, and recordkeeping. 18 Diagnosis and treatment of active TB disease in silica-exposed workers also protects the public, families, and silica-exposed coworkers who are at increased risk of developing active TB from LTBI. 2,12,16,19 This approach is consistent with elements of LTBI identification and treatment outlined in the US domestic TB elimination strategy. 20 -22
OSHA enshrined these principles in the final crystalline silica rule published in March 2016. 18 In addition to strengthening requirements for silica exposure control, the 2016 rule established national minimum medical surveillance standards for certain silica-exposed workers and addressed TB-related health risks, among other conditions linked to silica. In states that operate their own OSHA-approved occupational safety and health plans, such as Washington State, plans must have rules that are at least as effective as those developed by OSHA.
As of 2018, cases of active TB disease occurred in Washington State at a rate of 2.5 reported active cases per 100 000 population. 23 Owing to the recency of public policy that broadened access to TB screening in silica-exposed workers, detailed state-level data on TB burden in this population are not currently available. The state agencies that monitor TB and silicosis disease trends for Washington State are increasing their routine sharing of disease surveillance reports that include these conditions.
Treating people diagnosed with LTBI—which is estimated to range from 4.4% to 4.8% nationally 24 depending on the test used—is vital to successfully eliminating TB in the United States. 25 -28 OSHA’s rule provided the national mandate and authority for medical surveillance for silica-exposed workers. Yet, the diversity of clinical situations that health care providers (hereinafter, providers) are likely to encounter in Washington State suggests that additional guidance for TB screening would assist those conducting regulated medical surveillance examinations. The Washington State Adult Tuberculosis Screening Tool for Workers Exposed to Respirable Crystalline Silica (hereinafter, TB screening tool) benefits occupational and respiratory clinicians and public health practitioners by aiding both the individual- and population-level delivery of occupational health and TB screening services to silica-exposed workers receiving required medical surveillance examinations.
Goals of the TB Screening Tool
In 2018, the Washington State Department of Labor and Industries promulgated a nonmandatory TB screening tool as an adjunct to Washington State’s silica rule (Appendix). Created for use at the point of health care delivery, the document guides providers with 2 key decisions during baseline and periodic surveillance examinations:
Which workers should receive a comprehensive evaluation for active TB disease?
Which workers should have more than the minimum single test for LTBI at baseline examination required by regulation?
Beginning with active TB disease and then focusing on LTBI, this article supplements the TB screening tool by addressing the medical and occupational considerations that are pertinent to the settings of silica surveillance in which it may be used. For LTBI in particular, the TB screening tool includes a discussion of the various approaches to screening and testing in 2 key silica-exposed populations receiving regulated occupational medical surveillance examinations: people at low risk and people at high risk of acquiring LTBI or progressing to active TB disease.
Appendix: Adult tuberculosis screening tool for workers exposed to respirable crystalline silica
This unofficial copy of Washington Administrative Code (WAC) 296-840-175 is based on the official version certified on October 25, 2019, but may not be used instead of a current official version for regulatory purposes. The tool is available at https://app.leg.wa.gov/wac/default.aspx?cite=296-840-175. 29
Target Populations
Washington State Department of Labor and Industries staff members led the creation of the TB screening tool to accompany Washington State’s Respirable Crystalline Silica Standard (chapter 296-840 WAC). 30 The primary population for its use is adult workers with sufficient exposure to respirable crystalline silica to trigger the medical surveillance threshold in the rule (ie, workers who perform construction tasks and are required by the rule to use a respirator for ≥30 days per year and employees who are not performing construction tasks but are occupationally exposed to respirable crystalline silica at or above the action level [currently 25 μg/m3] for ≥30 days per year). For complete administrative language, please refer to chapter 296-840 WAC. 30 The TB screening tool is not copyrighted; as such, it may be widely distributed.
Background and Screening Considerations for Section 1 of the Screening Tool: Symptom Screen for Active TB Disease
TB has been referred to as the great mimicker, 31 because symptoms can be identical to common respiratory conditions such as community-acquired pneumonia or bronchitis, often resulting in delays in diagnosis. Although reducing delays in detecting active TB disease is a crucial target for improving TB control, doing so requires a high index of suspicion among providers, especially when diagnosing TB in patients with silicosis, where active TB disease may be more challenging to identify than in patients without silicosis and radiographic indicators may appear before clinical ones. 32 For this reason, providers should consider the possibility that active TB disease is the cause of (or coincident with other pulmonary diseases contributing to) abnormalities on the chest x-rays that are required at both baseline and periodic medical surveillance examinations under Washington State’s silica rule. Providers are empowered under the rule to order additional tests they “deem appropriate,” 30 which covers additional diagnostic tests for active TB disease. Thus, providers should consider whether to order additional diagnostic tests for active TB disease (eg, sputum smears, cultures, nucleic acid amplification) when investigating abnormalities on chest x-ray. When LTBI test results are positive, LTBI treatment is recommended, but only after active TB disease is ruled out.
Further emphasizing the importance of maintaining a high index of suspicion, a 2009 systematic review of 52 studies on delays in diagnosing pulmonary TB found that in high-income and low- to middle-income countries, diagnosis was delayed by an average of 21.5 and 28.4 days, respectively, after patient contact with the health care system. 33 The strategic plan published by the Centers for Disease Control and Prevention (CDC) Division of Tuberculosis Elimination also highlights the importance of the timely diagnosis of active TB disease, particularly given the lowering of awareness created by the decreasing incidence of TB disease. 34
The TB screening tool includes a checklist of signs and symptoms for active TB disease, a reportable condition in every state. 35,36 Based on CDC literature, 37 section 1 is intended to raise provider index of suspicion for active TB disease under clinical circumstances where patient presentation may warrant additional evaluation.
Background and Screening Considerations for Section 2 of the TB Screening Tool: Risk Assessment for LTBI
Anecdotal feedback from Washington State’s occupational health community as part of the rulemaking process strongly suggested that TB screening was not being broadly and systematically performed in silica-exposed workers. Furthermore, no regulatory mandate to conduct this screening existed before the release of OSHA’s 2016 crystalline silica rule. Rulemaking by regulatory bodies, including OSHA and the Washington State Division of Occupational Safety and Health, was expected to increase surveillance examinations in silica-exposed workers. The inclusion of LTBI screening in silica-exposed workers acknowledges broader findings, such as those of the CDC Division of Tuberculosis Elimination’s strategic plan, which states that “almost 90% of US TB cases result from reactivation of LTBI rather than recent transmission.” 34 That same document called for the publication of guidance to identify people for TB testing. Section 2 of the TB screening tool supports these efforts and rests upon several key principles:
Screening for TB is not the same as testing. Latent TB testing must be made available to all covered workers receiving baseline silica surveillance examinations, in populations with a low and high incidence of LTBI. Such baseline testing is a Washington State occupational standard that adheres to federal requirements. People receiving LTBI screening during periodic examinations (ie, after baseline examinations) do not always require testing for LTBI.
The TB screening tool uses confirmatory testing to address false-positive test results in low-risk people in populations with a low incidence of LTBI.
For testing requirements among people who have previously received a positive test result for TB, inquire with the regulator (eg, with the Washington State Division of Occupational Safety and Health). CDC does not recommend repeating the tuberculin skin test (TST) in patients who have a written record of a positive test result or who have already been treated for TB disease. 38
The TB screening tool helps providers prioritize testing for people at higher (vs lower) risk of LTBI acquisition or higher (vs lower) risk of progression to active TB disease.
Screening and Testing for LTBI in People at Low and High Risk of LTBI Acquisition or Progression to Active TB Disease
Testing for LTBI in the United States is commonly performed using the TST or interferon gamma release assay (IGRA). Test results, however, are not always accurate. Consideration must be given to the rates of both false-negative and false-positive test results, taking into account the expected prevalence of LTBI and the risk profile of the tested person. 24,39 -42
Although people who use the TB screening tool may choose to use either the TST or IGRA to test for LTBI, we recommend IGRA over TST in workers who have previously received the bacillus Calmette-Guérin (BCG) vaccine, because the IGRA is less likely to return false-positive test results from previous BCG vaccination. 43 Although determining the history of BCG vaccination varies by country, changing policies over time, and the unreliability of BCG history, 44,45 most people born outside the United States have received the BCG vaccine. Clinicians may find resources such as the BCG World Atlas to be helpful sources of information on past and present BCG vaccination practices. 45
Recommendations and Public Health Practice Implications: Screening and Testing for LTBI Among Low-Risk People
The positive predictive value of either the TST or IGRA decreases substantially when the prevalence of LTBI is sufficiently low in the tested population. 46 As such, the Washington State Department of Labor and Industries and the Washington State Department of Health determined that the TB screening tool should anticipate the need to control false-positive test results in people at low risk of either having acquired TB infection or having excess risk of disease progression who are screened in Washington State, particularly because testing for LTBI is required as a component of baseline regulatory medical examinations that certain silica-exposed workers receive. Under Washington State’s rule, the determination of whether to test for LTBI when conducting the periodic screening that follows baseline testing is at the discretion of the provider. Screening does not always result in testing. According to the TB screening tool, “low risk” refers to silica-exposed patients who have no identified risk factors for either (1) having acquired TB infection or (2) having excess risk of disease progression. 29 Factors relevant to these 2 streams of risk assessment are further described (Box).
Selected risk factors for acquiring tuberculosis (TB) or for progressing to active TB disease a
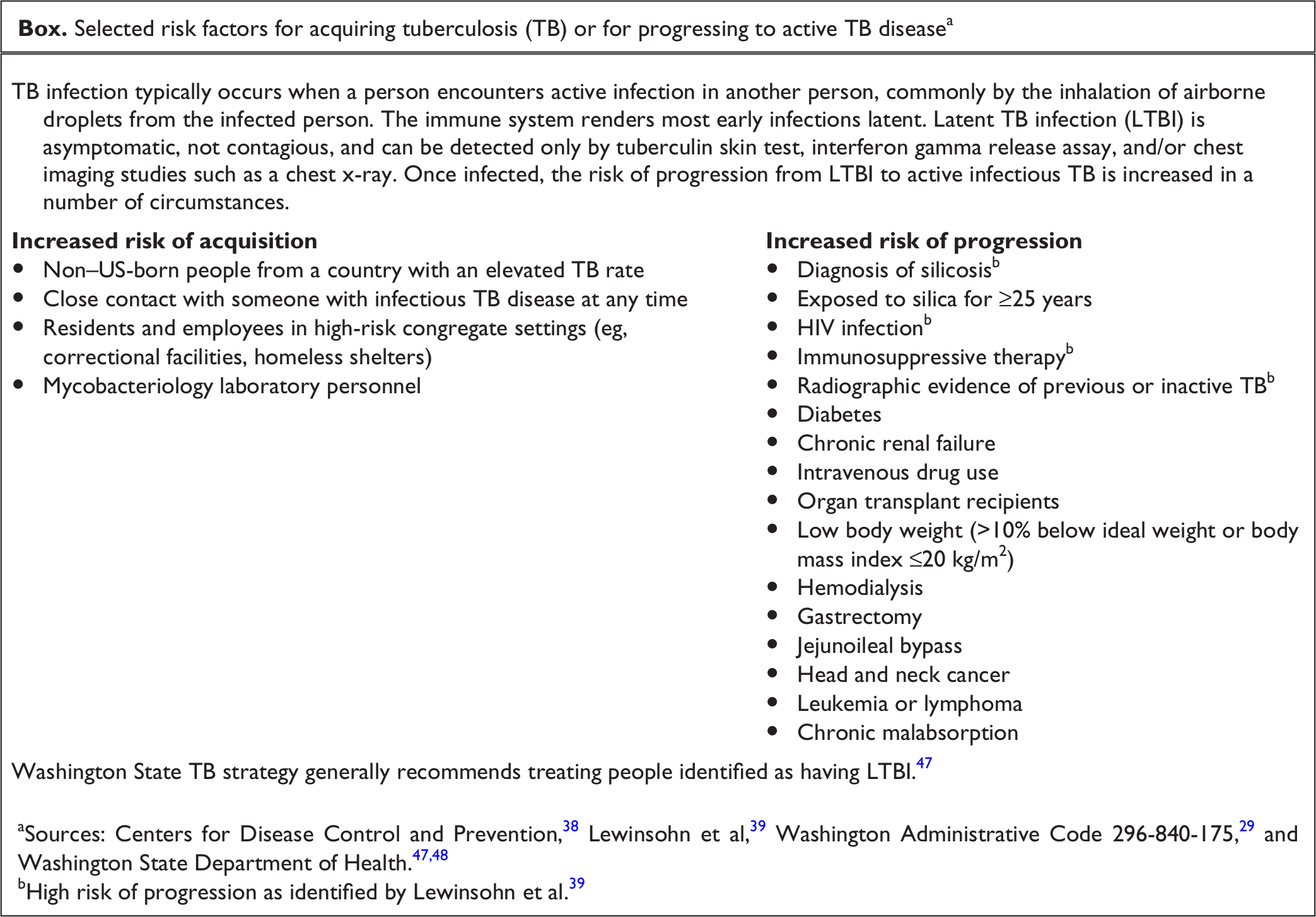
aSources: Centers for Disease Control and Prevention, 38 Lewinsohn et al, 39 Washington Administrative Code 296-840-175, 29 and Washington State Department of Health.47,48
bHigh risk of progression as identified by Lewinsohn et al. 39
Because the TB screening tool uses 2 positive test results to confirm LTBI among people at low risk for TB infection and disease progression, the TB screening tool advocates for a second round of testing after an initial positive test result in this group. Low-risk patients with discordant test results are considered LTBI negative. Requiring a second test to confirm an initial abnormal test result is a screening strategy that reduces false-positive test results. 29,39 The TB screening tool does not recommend performing a second test for LTBI in this low-risk group when the initial test result is negative. Users of the TB screening tool should be aware that false-positive and false-negative test results for both TST and IGRA are possible, the details of which are well-described in the medical literature. 29,38,39,43,47 Because adverse effects such as ulceration or necrosis may occur when repeating the TST in people who have already received a positive test result, we recommend not repeating the TST when performing confirmatory testing after an initial abnormal TST. 49,50 The standard permits the use of the IGRA or other “alternative TB tests . . . if sensitivity and specificity are comparable to TST.” 51
Recommendations and Public Health Practice Implications: Screening and Testing for LTBI Among Higher-Risk People
The TB screening tool recommends testing patients with a higher (vs lower) risk of TB acquisition or progression in agreement with several recommendations of the 2017 American Thoracic Society/Infectious Diseases Society of America/CDC Clinical Practice Guidelines: Diagnosis of Tuberculosis in Adults and Children. The guideline explicitly organizes the approach to diagnostic testing on the likelihood of being infected with TB (LTBI acquisition) and the likelihood of developing active TB disease if infected (TB progression). 39 To facilitate the identification of silica-exposed people at higher (vs lower) risk of TB acquisition or progression, the TB screening tool includes a selected list of risk factors. Additional information is available from the Washington State Department of Health Tuberculosis Services Manual. 47
For people likely to be infected with TB, the authors of the 2017 American Thoracic Society/Infectious Diseases Society of America/CDC Clinical Practice Guidelines: Diagnosis of Tuberculosis in Adults and Children made separate recommendations for whether 1 or 2 tests are indicated depending on the risk of TB progression. For people who are likely to be infected with TB and at high risk of TB progression, the authors recommend a second test if the initial test result is negative. Test results are positive, overall, if either test result is positive. 39 This approach effectively requires that an initial negative test result be confirmed, which reduces false-negative test results overall. 39 Providers have discretion when using the TB screening tool to determine whether to order 1 or 2 LTBI tests after identifying risk factors for TB disease progression, with the exception that at least 1 test for LTBI is required as part of baseline examinations performed under the Washington State standard.
The TB screening tool recommends dual testing to reduce the risk of false-positive test results in workers at low risk of having TB for whom baseline testing is required. In contrast, the TB screening tool does not provide a recommendation for dual testing among workers who are at higher (vs lower) risk. Except for the single test for LTBI required at baseline examinations, the TB screening tool leaves the assessment of various screening and testing strategies up to the ordering provider once risk factors for TB infection acquisition or TB disease progression have been identified.
Various clinical circumstances could occur among silica-exposed workers with TB risk factors and with abnormal LTBI test results. Examples include responding to indeterminate IGRA results and screening people who previously received a positive test result, were treated for LTBI, or have previous TB test results believed to be falsely positive. Users of the TB screening tool may consider contacting their local public health authorities for additional assistance in such circumstances.
Screening for and treating LTBI in silica-exposed workers complements primary prevention via reductions in silica exposure. Evidence shows that nontrivial risk of future active TB disease remains after treatment of LTBI in silica-exposed workers. 52 LTBI treatment should not be used as a substitute for interventions that reduce silica exposure at the individual and population levels.
Conclusion
Recently updated regulations have increased worker protections against the health hazards of exposure to respirable crystalline silica. The updated regulations include addressing the risk of progression to active TB disease from previous LTBI in silica-exposed workers. The TB screening tool is an adjunct to recent Washington State regulations and CDC’s call for the publication of guidance to identify people for testing. The current version of the TB screening tool is available from the Washington State Code Reviser at WAC 296-840-175. An unofficial copy of the TB screening tool is included herein (Appendix). The TB screening tool is intended to assist providers in identifying workers who should receive a comprehensive evaluation for active TB disease and whom to test for LTBI during occupational medical surveillance examinations for employees exposed to silica. The identification and treatment of workers with active or latent TB is essential to eliminating TB. 25 -28
Footnotes
Appendix
Adult tuberculosis screening tool for workers exposed to respirable crystalline silica.
Acknowledgments
The authors thank the following people for their contributions: Jiho H. Bryson, MD, MPH; Kathleen M. Fagan, MD, MPH; Jacquie Goodwill; Carolyn Reeb-Whitaker, MS; the Washington State Department of Health Tuberculosis Program; and the Washington State Department of Labor and Industries Division of Occupational Safety and Health.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: N.K.R. discloses unpaid academic affiliations with the University of Washington, Seattle, Washington.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors were paid employees of the Washington State Department of Labor and Industries.