
Abstract
Objectives
Although US state laws shape population health and health equity, few studies have examined how state laws affect the health of marginalized racial/ethnic groups (eg, Black, Indigenous, and Latinx populations) and racial/ethnic health inequities. A team of public health researchers and legal scholars with expertise in racial equity used systematic policy surveillance methods to develop a comprehensive database of state laws that are explicitly or implicitly related to structural racism, with the goal of evaluating their effect on health outcomes among marginalized racial/ethnic groups.
Methods
Legal scholars used primary and secondary sources to identify state laws related to structural racism pertaining to 10 legal domains and developed a coding scheme that assigned a numeric code representing a mutually exclusive category for each salient feature of each law using a subset of randomly selected states. Legal scholars systematically applied this coding scheme to laws in all 50 US states and the District of Columbia from 2010 through 2013.
Results
We identified 843 state laws linked to structural racism. Most states had in place laws that disproportionately discriminate against marginalized racial/ethnic groups and had not enacted laws that prevent the unjust treatment of individuals from marginalized racial/ethnic populations from 2010 to 2013.
Conclusions
By providing comprehensive, detailed data on structural racism–related state laws in all 50 states and the District of Columbia over time, our database will provide public health researchers, social scientists, policy makers, and advocates with rigorous evidence to assess states’ racial equity climates and evaluate and address their effect on racial/ethnic health inequities in the United States.
Keywords
Racial/ethnic health inequities are a pervasive problem in the United States. 1 Data show that, on average, Black, Indigenous (including Native American, Native Alaskan, and Native Hawaiian), and Latinx people fare worse than their White counterparts in various health outcomes, including HIV/AIDS, infant mortality, and diabetes. 2 Racism—which operates at the interpersonal, cultural, and structural levels—is a key determinant of racial/ethnic health inequities, and these inequities are not explained by differences in socioeconomic factors. 2 -5 In particular, racism marginalizes, or systematically excludes, Black, Indigenous, and Latinx people from power, status, and other social, economic, and political resources and opportunities, all of which are important social determinants of population health and health inequities. 2,6 In recent years, public health researchers have increasingly examined the role of not only interpersonal but also structural racism in shaping population health outcomes across and within racial/ethnic groups. 1,2,7 Specifically, investigators have found that structural racism—defined as the historically contingent and persistent ways in which social systems and institutions generate and reinforce inequities in access to power, privilege, and other resources among racial/ethnic groups deemed to be superior and those viewed as inferior 1,2,7 —negatively affects health outcomes, including breast cancer, premature mortality, birth outcomes, and cardiovascular disease, among Black people. 1,2,8 -11 In addition, scholars have shown that structural racism, including genocide and immigration policies, undermines the physical and mental health of Native American and Hispanic people, respectively. 1,7,12
According to critical race theory (ie, a collection of intellectual, social, and political practices aimed at studying and transforming the relationship among race, racism, and power), structural racism—which evolves and stems from historical processes such as genocide, slavery, and immigrant exclusion—operates through and is embedded in contemporary federal and state-level laws and policies pertaining to various social systems and institutions, including housing, education, health care, employment, criminal justice, voting rights, and immigration. 13 -17 Past and present laws and policies overtly and covertly, directly and indirectly, and actively and passively (through both inaction and colorblindness) determine the inequitable allocation of social, economic, political, and environmental resources and harms across racial/ethnic groups today. 13 -17 For example, as a result of historical and contemporary housing and banking laws, policies, and practices (eg, redlining, mortgage lending, zoning) that explicitly or implicitly favor White people and disadvantage marginalized racial/ethnic groups, Black, Native American, and Hispanic people are more likely than their White counterparts to live in systematically underresourced neighborhoods that lack access to high-quality infrastructure, social and health services, and educational and employment opportunities. 1,2,7,17
Moreover, as a result of criminal justice laws, policies, and practices that disproportionately affect marginalized racial/ethnic groups (eg, stop-and-identify laws, which allow law enforcement officers to stop a person and demand identification upon “reasonable suspicion” of a crime, and drug sentencing laws), Black, Native American, and Hispanic people—who tend to be the target of over-policing, arrest, and incarceration as a result of conscious and unconscious negative racial stereotypes—are disproportionately represented in US prisons and jails. 1,17 -19 Consequently, voting rights laws that disenfranchise people with previous convictions disproportionately affect Black people and individuals from other marginalized racial/ethnic groups. 18 Furthermore, given pervasive racist stereotypes that erroneously depict Black people as dangerous criminals, stand-your-ground laws systematically threaten the rights and lives of Black people by selectively allowing a person deemed to be superior to harm or kill a Black person by claiming self-defense, even in the absence of an actual threat. 20
In addition, as a result of laws, policies, and practices that undermine the intergenerational transfer of wealth among Black communities and other marginalized racial/ethnic groups, as well as both structural and interpersonal racism in the education system and employment sector, Black, Native American, and Hispanic people tend to have lower levels of wealth and income than their White counterparts. 1 -4,13,14,17 Consequently, laws pertaining to the minimum wage, income-related housing laws, and predatory lending laws disproportionately affect marginalized racial/ethnic groups. Moreover, as a result of conscious and unconscious biases inaccurately depicting Black people as threatening or violent, Black students are more likely than their White counterparts to be disciplined using force in elementary schools and high schools. 21 -23 Thus, laws that prohibit corporal punishment in public schools will particularly affect Black students and students from other marginalized racial/ethnic groups. Lastly, immigration laws disproportionately target Black and Hispanic immigrants and lead to the social exclusion of marginalized racial/ethnic groups by prohibiting entry, facilitating deportation, and limiting access to social, economic, and political opportunities and resources, as well as legal rights, among immigrants from marginalized racial/ethnic groups deemed to be undesirable. 7,12
In recent years, public health scholars and practitioners have called for greater scientific inquiry into the influence of laws and policies on population health and health inequities. 24 -28 Investigators have found that US state laws, such as state same-sex marriage laws, state Medicaid expansions, and state physical education and daily recess laws, play an important role in shaping the population distribution of various health outcomes, including mental health, cancer screening, and physical activity, within and across social groups. 29 -31 However, excluding the studies conducted by Krieger et al 8 -10 to examine the effect of historical Jim Crow laws on contemporary health inequities between Black and White people, studies assessing the effect of state laws related to structural racism on inequitable distributions of health outcomes across racial/ethnic groups are scarce. 1
Nonetheless, theory and empirical research suggest that historical and contemporary state laws that overtly or covertly privilege White people and disadvantage people from marginalized racial/ethnic groups shape racial/ethnic health inequities through various social, economic, physical, and psychological mechanisms—including economic, residential, educational, and occupational segregation of marginalized racial/ethnic groups into low-quality neighborhoods, schools, and jobs; disproportionate exposure of marginalized racial/ethnic groups to environmental toxins and occupational hazards, as well as chronic and acute psychosocial stressors; forced removal and alienation of marginalized racial/ethnic groups from traditional land resources and practices; discriminatory arrest, detention, and incarceration practices; and fewer health care providers and high-quality facilities in communities of color than in predominantly White neighborhoods. 1 -5,7,32,33 For example, research shows that racial residential segregation, which is linked to housing and banking laws, policies, and practices that disproportionately disadvantage Black people and people from other marginalized racial/ethnic groups, is negatively associated with low birth weight and preterm birth among Black women and higher rates of breast and lung cancer mortality among Black people compared with White people. 2,7,33 Furthermore, investigators found that living in a neighborhood with high levels of police stopping and frisking pedestrians, which occurs disproportionately in Black and Hispanic neighborhoods and disproportionately affects Native American people, 19,34,35 is associated with poor mental and physical health outcomes, including psychological distress, diabetes, and high blood pressure. 36
Policy surveillance, which involves the systematic tracking of laws and policies over time, is a central component of legal epidemiology, an emerging field that investigates law as a determinant of disease etiology, distribution, and prevention in populations. 24,25 Policy surveillance provides data necessary to rigorously evaluate the effect of state laws and policies on population health and health inequities. 24,25 Although databases pertaining to one or some of the issues of interest are available, 37 to our knowledge, no comprehensive database pertaining to US state laws that shape the inequitable allocation of social, economic, and political resources among various marginalized racial/ethnic groups relative to their White counterparts exists.
However, systematically collecting information on state laws related to structural racism over time and place and linking them to individual-level health outcomes is critical for rigorously evaluating their effect on the health of people from marginalized racial/ethnic groups and the magnitude of racial/ethnic health inequities. 24,25 Identifying how state laws that are explicitly or implicitly related to structural racism affect health outcomes among marginalized racial/ethnic groups—including, but not limited to, Black, Indigenous, and Latinx people—may help inform evidence-based policy- and system-level initiatives that repeal unjust and harmful laws, policies, and practices and instead promote social justice and health equity.
We describe the process, undertaken collaboratively by an interdisciplinary team of public health researchers and legal scholars, of developing a comprehensive, longitudinal database of state laws that are explicitly or implicitly related to structural racism and that uniquely or disproportionately undermine the distribution of and access to social, economic, and political resources to various marginalized racial/ethnic groups (eg, Black, Indigenous, and Latinx populations). 13 -17 In addition, we characterize the distribution of state laws related to structural racism in the 50 US states and the District of Columbia from 2010 through 2013 and calculate the absolute and percentage change in the number of laws related to structural racism during that period.
Methods
Guided by critical race theory, 13 -16 using empirical studies pertaining to structural racism and health inequities, 1,2,7,12 and reviewing reports and fact sheets on racism and the law developed by legal organizations such as the American Civil Liberties Union 38 and the National Association for the Advancement of Colored People, 39 the public health researchers on our team developed a preliminary typology of contemporary legal domains pertaining to state-level structural racism in the United States. Our team’s legal scholars then reviewed and revised this initial typology based on their expertise and practical, on-the-ground experience in racial equity. Through this process, we developed a final typology of 10 legal domains related to contemporary state-level structural racism in the United States: voting rights, stand-your-ground laws, racial profiling laws, mandatory minimum prison sentencing laws, immigrant protections, fair-housing laws, minimum-wage laws, predatory lending laws, laws concerning punishment in schools, and stop-and-identify laws.
Using law review articles and legal reports and in consultation with one another and additional racial equity legal experts, our team’s legal scholars determined the laws that should be included in each domain. The scholars then identified the scope and features (eg, population covered or affected, length of related sentence, exceptions, enforcement mechanisms) of each law using primary and secondary (ie, law review articles, legal reports) sources. The 2 legal scholars then characterized each law using a set of mutually exclusive categories (assigned a numeric value) and compiled the categories into a preliminary coding scheme. The legal scholars then collected information on each law using multiple legal databases (ie, Westlaw Next, LexisNexis, Hein Online) for a subset of 6 to 12 randomly selected states (depending on the complexity and variability of a given law across states) in a given year (ie, 2010). The scholars then used the scheme to assign a numerical value to each state for each law in that year. The coding scheme was then revised and finalized based on this process. To ensure that this scheme was applied consistently by the 2 legal scholars, they developed a guide defining each law and its categories and outlining key questions to consider when assigning a numerical value to each state and the District of Columbia for each law using the scheme.
From September 2017 through November 2018, the 2 legal scholars collected information on each law for all 50 states and the District of Columbia in 2010, 2011, 2012, and 2013 using multiple legal databases (ie, Westlaw Next, LexisNexis, Hein Online). Given the time-intensive nature of legal research and funding constraints, we limited the study period to 4 years (ie, 2010-2013). The scholars then assigned a numeric value to each state and the District of Columbia for each law in each year of the study period using the coding scheme. The legal scholars carefully documented any question or issue that arose during the coding process, discussed and resolved them during regular meetings, and iteratively revised and reapplied the coding scheme as needed. In addition, each legal scholar reviewed a subset of the other legal scholar’s coded laws to ensure accuracy. Moreover, the legal scholars documented the specific language that informed the numeric value assigned to each state for a given law and catalogued relevant legal citations and each law’s statutory history during the study period.
In consultation with the legal scholars, the public health researchers on our team reviewed the compiled data and examined patterns in state laws related to structural racism across and within states and years during the study period. The public health researchers then generated descriptive statistics (counts and percentages) to characterize the distribution of all 50 states and the District of Columbia in 2010, 2011, 2012, and 2013 with regard to each law in each legal domain. In addition, we calculated both the absolute and percentage change in the number of explicitly and implicitly racialized state laws from 2010 through 2013. Lastly, we also visualized the data for 4 of the 10 legal domains (namely, voting rights, stand-your-ground laws, mandatory minimum prison sentencing laws, and fair-housing laws) using maps generated in Matlab (Mathworks Inc).
Results
We identified 843 US state laws explicitly or implicitly related to structural racism across the 10 contemporary legal domains (ie, voting rights laws, stand-your-ground laws, racial profiling laws, mandatory minimum prison sentencing laws, immigrant protections, fair-housing laws, minimum-wage laws, predatory lending laws, laws concerning punishment in schools, and stop-and-identify laws) in all 50 states and the District of Columbia from 2010 through 2013. We found that, during the study period, laws that disproportionately discriminated against people from marginalized racial/ethnic groups, including stand-your-ground laws (Figure 1), mandatory minimum sentencing laws (Figure 2), and stop-and-identify laws (Table), were in place in most states. For example, in 2013, twenty-three states had stand-your-ground laws in place (Figure 1), and 41 had passed laws on mandatory minimum sentencing (Figure 2; Table).
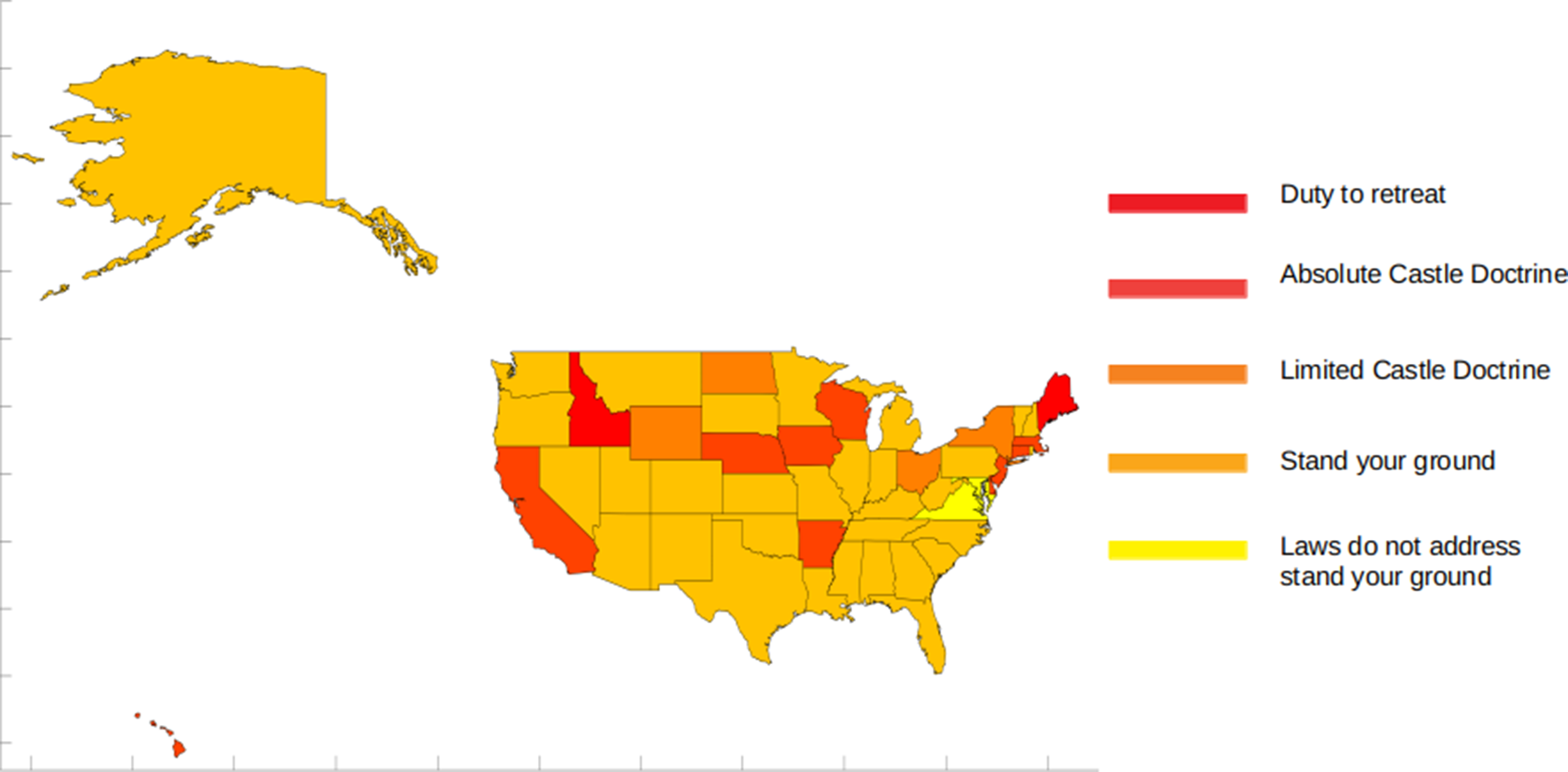
Geographic distribution of stand-your-ground laws in 50 US states and the District of Columbia, 2013.
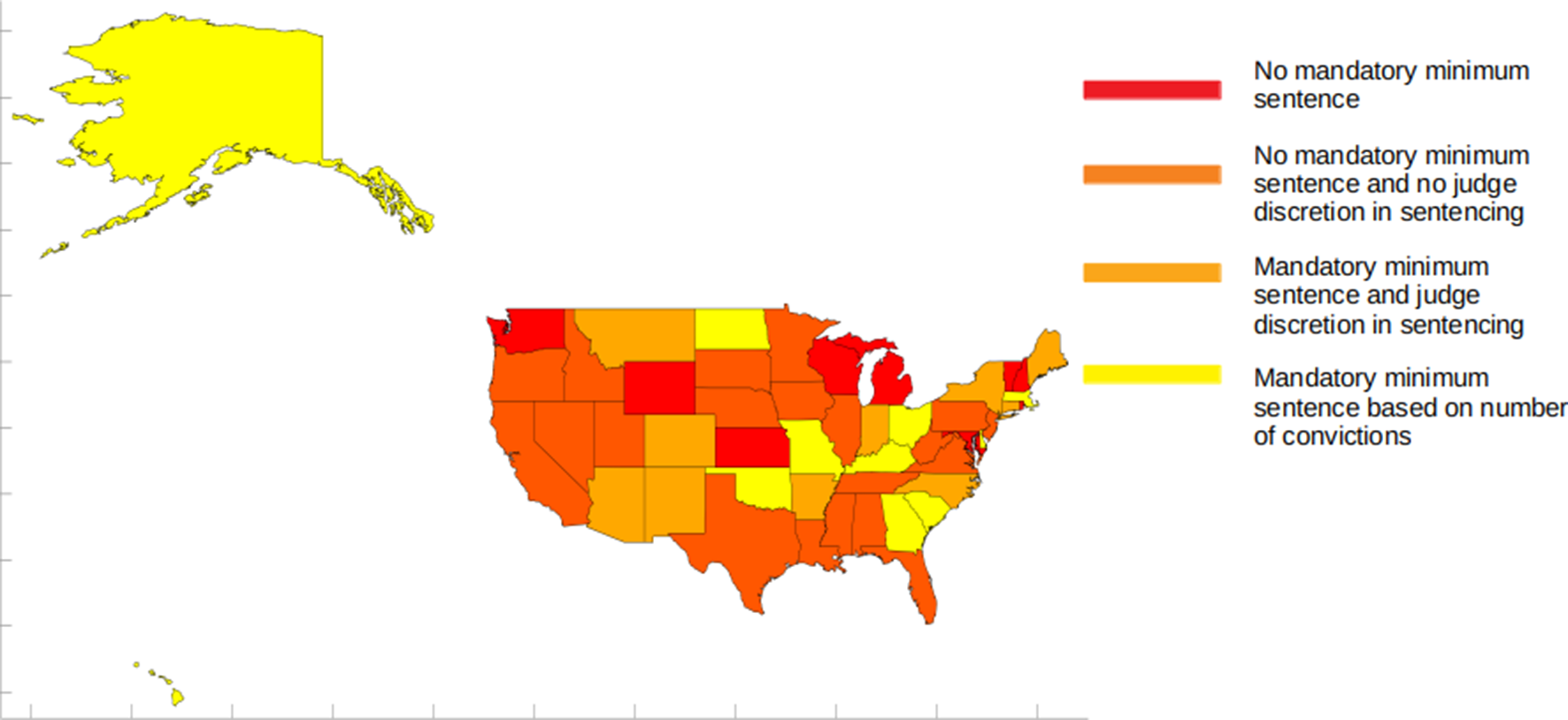
Geographic distribution of mandatory minimum sentencing laws in 50 US states and the District of Columbia, 2013.
Distribution of and change in contemporary structural racism–related laws in the 50 states and the District of Columbia (N = 51), by legal domain and year, 2010-2013
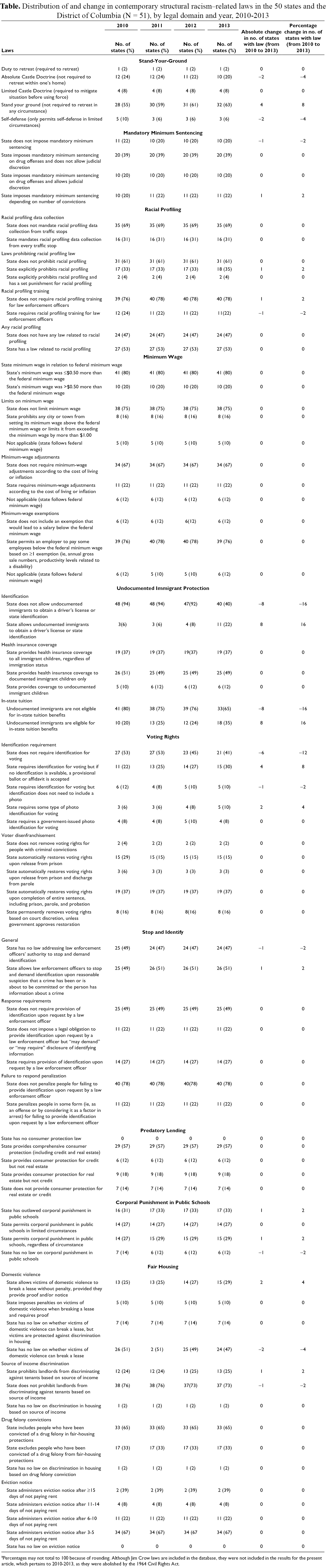
aPercentages may not total to 100 because of rounding. Although Jim Crow laws are included in the database, they were not included in the results for the present article, which pertains to 2010-2013, as they were abolished by the 1964 Civil Rights Act.
Similarly, most states had not enacted laws that prevent unjust treatment or undue burden among people from marginalized racial/ethnic groups from 2010 through 2013, including laws that prohibit racial profiling (Table), prevent voter disenfranchisement upon a criminal conviction (Figure 3), completely outlaw corporal punishment in public schools (Table), or prevent discrimination in housing based on source of income (Figure 4; Table). For example, in 2013, only 2 states had laws in place that did not remove voting rights for people with criminal convictions (Figure 3), and only 13 states had passed laws that prohibit landlords from discriminating against tenants based on source of income (Figure 4; Table).
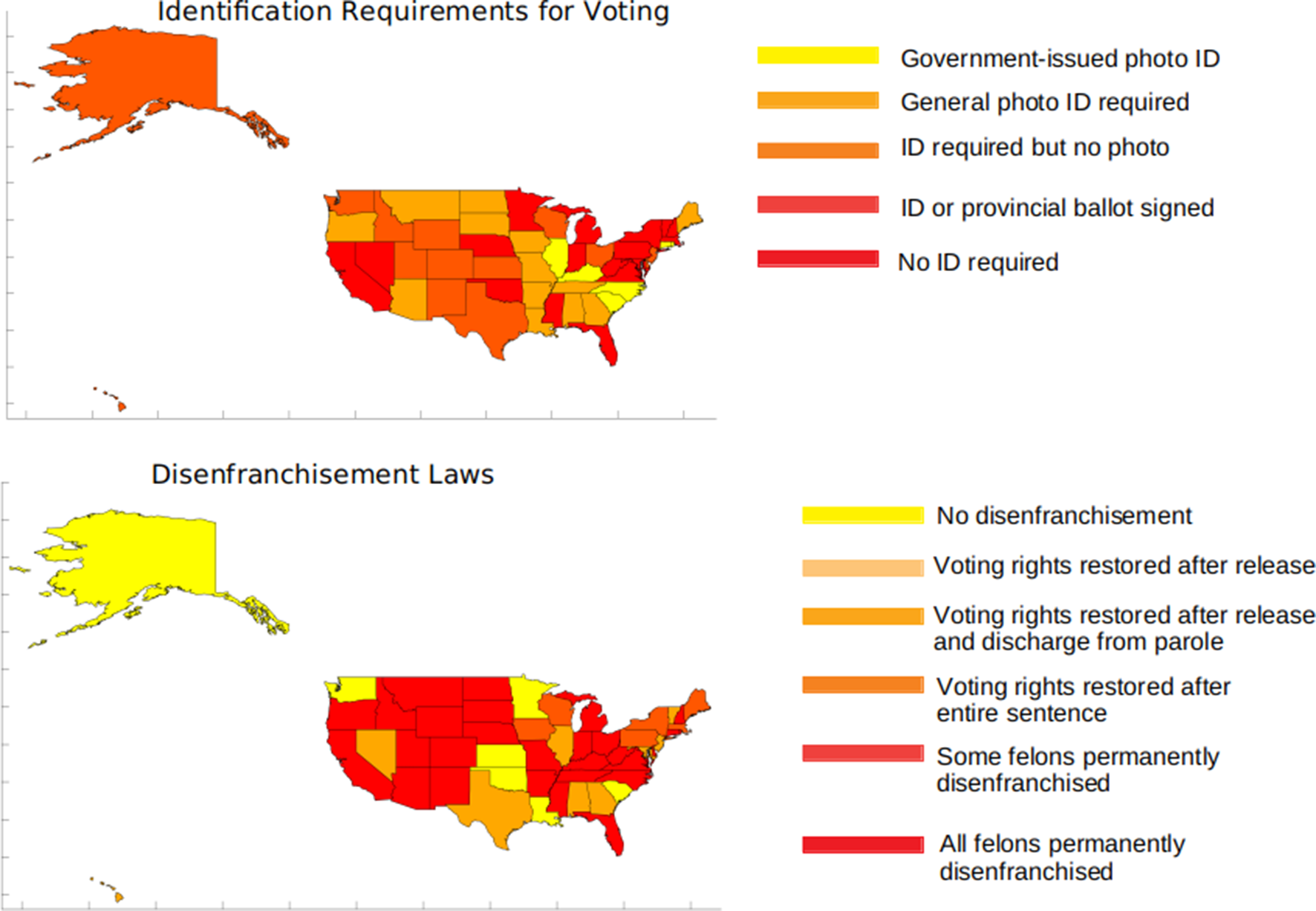
Geographic distribution of voting rights laws in 50 US states and the District of Columbia, 2013. Abbreviation: ID, identification.
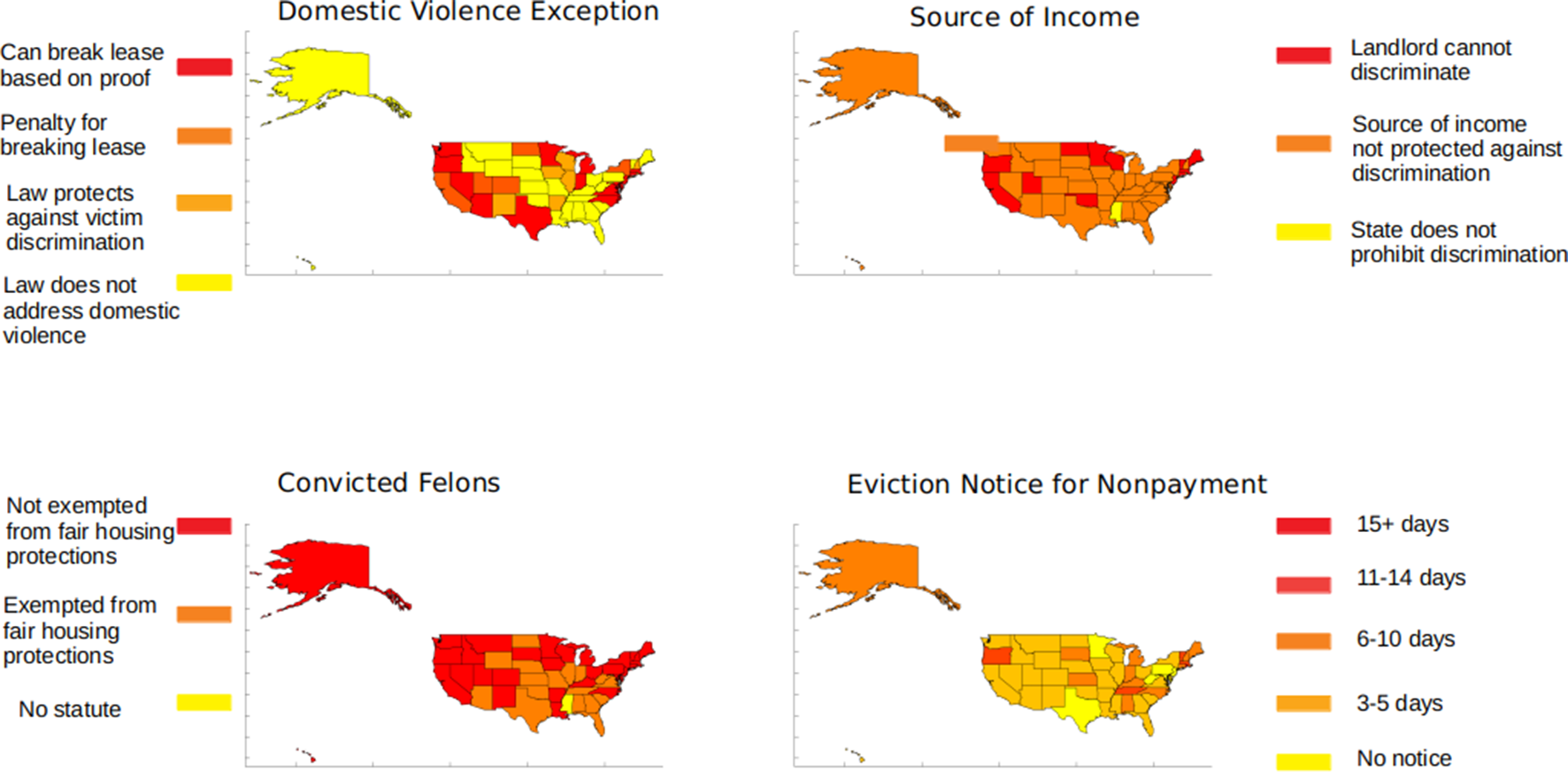
Geographic distribution of fair-housing laws in 50 US states and the District of Columbia, 2013.
State laws linked to structural racism changed little from 2010 to 2013 across all 10 legal domains. Although some states amended their laws from year to year, in most instances, amendments did not substantially change the language or effect of the law. Of the 843 state-level laws we examined, only 82 (10%) were amended during the study period; of these amendments, fewer than half altered the law in a substantive way (Table). From 2010 through 2013, most substantive changes pertained to increases in the number of stand-your-ground laws, some undocumented immigrant protection laws, voter identification requirement laws, and some fair-housing laws.
Discussion
Historical and contemporary state laws play an important role in shaping population health and health equity in the United States, 8 -10,27 -31 including the health of people from marginalized racial/ethnic groups and the magnitude of racial/ethnic health inequities. 1,7 -10,12 Our database is the first of which we are aware to provide comprehensive, detailed, and analyzable information on salient contemporary state laws pertaining to 10 legal domains in all 50 states and the District of Columbia from 2010 through 2013. This information will allow researchers to use the tools of legal epidemiology to rigorously evaluate the effect of state laws that are explicitly or implicitly linked to structural racism on the health of people from marginalized racial/ethnic groups and the magnitude of racial/ethnic health inequities in the United States. 24,25 Specifically, our team plans to evaluate the effect of these laws on health outcomes within and across racial/ethnic groups to help inform the development and implementation of evidence-based state laws, policies, and practices that help promote racial and health equity in the United States. Upon completion of these analyses, we will make our database freely available to other researchers to use in their own public health and social science research examining the effect of structural racism–related state laws (individually or in aggregate) on health and health care, economic, and social outcomes and inequities over time. Moreover, we will disseminate our database to policy makers, policy advocates, and community stakeholders at no cost to support state policy initiatives and advocacy efforts that promote racial and health equity. Our database will allow states to compare their structural racism–related state laws with the laws of other states and provide advocates and community stakeholders with the detailed information they need to advocate for laws and policies that help advance racial equity in their state.
We learned several important lessons while developing our comprehensive database of structural racism–related state laws. First, we learned that it is of the utmost importance to develop a detailed protocol to systematically collect accurate information on each legal domain and law. The protocol must then be strictly followed by each legal scholar for each domain and each law across all 50 states and the District of Columbia and in every year to maintain consistent coding. Second, we had some challenges in identifying the most relevant laws in each domain and the most salient aspects of each law, including its effect, enforcement, and remedies. We found that having an interdisciplinary team of both public health researchers with a background in the structural and social determinants of racial/ethnic health inequities and legal scholars with expertise in racial equity was essential to ensuring the relevance and accuracy of our database. In addition, in deciding which laws to include in each legal domain and what aspects of each law to consider, we found that carefully and systematically documenting our rationale, engaging in regular group discussions, and collecting the legal language that supported our decisions (which will be made publicly available along with our database to guide analytic decisions and the interpretation of research findings) were critical in not only identifying the laws that were strongly related to structural racism and capturing the most salient aspects of these laws, but also promoting interrater reliability among the legal scholars coding the laws.
Third, we found that posing and answering a set of theoretically grounded research questions for not only the process of compiling the database as a whole but also for each domain and each law across all states and years was essential for developing a comprehensive database of state laws pertaining to structural racism. Our research questions, which were informed by critical race theory, 13 -16 guided our reading of the laws’ language and provided a consistent foundation to turn to when a law went beyond the scope of interest. Fourth, through the process of compiling the database, we found that a 4-year period did not adequately capture meaningful changes in laws over time. Most states did not amend existing laws during the study period, and among the few states that did, most did not do so in a substantive way. Thus, given the slow pace of legal and policy change, we plan to extend our database to span a longer time frame (eg, 1990 to the present day) in coming years. Lastly, new legal domains relevant to racial equity have emerged since we began developing our database (eg, marijuana legalization and decriminalization laws, which disproportionately affect people from marginalized racial/ethnic groups). 40 Therefore, we will update our database so that it includes information on these more recent legal developments for each state in every year during the extended study period.
Despite modest changes in some protective laws (namely, some undocumented immigrant rights laws and fair-housing laws) from 2010 through 2013, our findings suggest that most states continued to have in place laws that are explicitly or implicitly related to structural racism—including stand-your-ground laws and voter identification requirement laws, which more states instituted during the study period. Legal epidemiology and policy surveillance provide an important framework and tools for identifying the effect of state laws on population health and health equity. 24 -26 By using policy surveillance strategies to collect data on structural racism–related state laws across all 50 states and the District of Columbia over time, our database will provide public health researchers, social scientists, policy makers, and advocates with rigorous evidence to assess states’ legal climates toward marginalized racial/ethnic groups. 25 Using legal epidemiology methods, analysts can then determine their effect on health, economic, and social outcomes within and across racial/ethnic groups. 24,26 In the future, we will link this state-level database to individual-level health outcomes, with the goal of rigorously evaluating the effect of these structural racism–related state laws on health outcomes among marginalized racial/ethnic groups. Together, these efforts will facilitate the development and implementation of evidence-based state laws, policies, and practices that promote racial and health equity and positively contribute to the lives and health of Black, Indigenous, and Latinx people, among others, in the United States.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Harvard Catalyst grant and a Boston Children’s Hospital faculty grant awarded to S.B. Austin and M. Samnaliev. S.B. Austin was supported by the Leadership Education in Adolescent Health project, Maternal and Child Health Bureau, Health Resources and Services Administration grants T71-MC00009 and T76-MC00001.