
Abstract
Objectives:
Asthma disproportionately affects Black people and people with low incomes, but Medicaid expansion (hereinafter, expansion) data on these populations are limited. We investigated health care use among adults with asthma, before and after expansion, and examined whether asthma-related health care use after expansion varied by demographic characteristics.
Methods:
We analyzed data from the 2011-2013 and 2015-2019 Behavioral Risk Factor Surveillance System Adult Asthma Call-Back Survey on participants aged 18-64 years with current asthma and low incomes in 23 US states. We assessed 5 asthma-related outcomes, including medical visits (routine and emergency) and medication use, for expansion and nonexpansion groups. We used t tests to compare weighted percentages and 95% CIs, then performed adjusted difference-in-differences analyses. Secondary analyses stratified data by race, ethnicity, and sex.
Results:
Primary analyses (N = 10 796) found no significant associations between expansion and any outcome. Analyses stratified by race and ethnicity found no significant changes (eg, asthma controller medication use among non-Hispanic Black participants in the expansion group was 24.1% [95% CI, 14.4%-37.5%] in 2011-2013 and 35.5% [95% CI, 27.0%-45.1%] in 2015-2019; P = .13). Use of asthma controller medication increased significantly among non-Hispanic Other participants in the nonexpansion group (2011-2013: 16.0% [95% CI, 9.5%-25.5%]; 2015-2019: 40.2% [95% CI, 25.5%-56.8%]; P = .01). Asthma-related hospitalizations decreased significantly among women in the expansion group: 2011-2013 (7.8%; 95% CI, 5.3%-11.3%) and 2015-2019 (3.5%; 95% CI, 2.5%-4.9%) (P = .009).
Conclusions:
Investigating factors other than health insurance (eg, social determinants of health) that influence the use of asthma-related health care could advance knowledge of potential strategies to advance health equity for adults with asthma and lower incomes.
Asthma is a common chronic disease that can be worsened by environmental triggers. 1 Asthma affects >25 million people in the United States, resulting in approximately 1.8 million emergency department (ED) visits, 160 000 hospitalizations, 4000 deaths, and $50 billion in medical costs annually.2,3 Asthma cannot be cured but can be controlled. 1 Asthma-related ED visits, hospitalizations, and mortality can be prevented through asthma control efforts, including increasing access to guidelines-based asthma care, such as regularly scheduled medical visits and, when medically indicated, use of asthma controller medication. 4
Asthma disproportionately affects certain US populations, including people with low incomes and/or people who are Black.2,5,6 People with low income are more likely than people with high income to have asthma and require urgent or emergent care for asthma.1,2,7 Rates of asthma-related ED visits and hospitalizations among non-Hispanic Black people in the United States are more than quadruple the rates among non-Hispanic White people in the United States. 8 Non-Hispanic Black people in the United States are more than twice as likely as any other racial and ethnic group to die of asthma.2,9
Modifying health insurance coverage is a potential strategy to advance health equity. 10 Medicaid, a public health insurance program for people with low income, plays a disproportionately large role in covering non-White people in the United States.10,11 Because of the Affordable Care Act, US states and territories have had the option to extend Medicaid eligibility (“Medicaid expansion”) to all adults aged <65 years with incomes <138% of the federal poverty level (FPL).12,13 In 2014, 26 states and the District of Columbia were the first to implement Medicaid expansion (hereinafter, expansion). 13
While the impact of expansion has been investigated in the overall population as well as in people with some health conditions (eg, congestive heart failure, chronic kidney disease), expansion data on people with respiratory conditions, including asthma, are limited.14-17 One study examined hospital data from 7 states and found lower rates of mechanical ventilation among people with asthma or chronic obstructive pulmonary disease in expansion states than in nonexpansion states; however, data on people with asthma were not analyzed separately from data on people with chronic obstructive pulmonary disease. 16 An asthma-focused, population-based study observed an association between expansion and increased prevalence of health insurance coverage among adults with asthma and lower incomes (defined hereinafter as having an annual household income <138% of the FPL), but expansion did not substantially affect the prevalence of asthma-related cost barriers to health care. 15 Another study reported a national increase in asthma medication use after states could implement expansion (2014-2018) compared with before 2014; however, this analysis did not account for whether individual states implemented expansion, and it stratified data by race but not ethnicity. 17
The primary objective of our study was to investigate health care use before and after expansion among adults with asthma and lower incomes from 23 states, while accounting for differences among states in implementing expansion. A secondary objective was to assess whether the impact of expansion on asthma-related health care use varied by race and ethnicity or sex.
Methods
We used Behavioral Risk Factor Surveillance System (BRFSS) Adult Asthma Call-Back Survey (ACBS) data from 2011-2013 and 2015-2019, excluding 2014 data as a phase-in period.15,18,19 BRFSS is an ongoing, state-based, random-digit-dialed, cross-sectional telephone survey of noninstitutionalized US adults aged ≥18 years. 20 BRFSS is conducted in 50 states, the District of Columbia, and 3 US territories. 21 Details about BRFSS, including its disproportionate stratified sample design for landline telephone samples, random sample design for the cellular telephone survey, and iterative proportional fitting (also known as raking for weighting), are available elsewhere.20-22 ACBS is a follow-up telephone survey that participating states administer approximately 2 weeks after BRFSS to BRFSS participants who responded that they ever had asthma.20,23 Informed consent was obtained; state-specific institutional review board requirements apply to each participating state. The Human Research Protection Office at the Centers for Disease Control and Prevention determined that BRFSS and ACBS data analyses were exempt from review (exempt category 2). 24 ACBS details, including survey design, are available elsewhere.23,24
We pooled years of ACBS data to obtain a sufficiently large sample to generate stable estimates. For this analysis, we included states with ACBS data from both periods (2011-2013 and 2015-2019) but excluded data from Indiana and Pennsylvania because these states implemented expansion in 2015 (the first year of this study’s postexpansion period). The final dataset included 23 states.
We included ACBS participants aged 18-64 years with current asthma and annual household income <138% of the 2016 FPL. We excluded adults aged ≥65 years because they were not included in the expansion provision of the Affordable Care Act. 12 We categorized ACBS participants with current asthma if they answered yes to 2 questions: “Has a doctor, nurse, or other health professional ever told you that you had asthma?” and “Do you still have asthma?” We calculated annual household income as a percentage of FPL, accounting for family size and using midpoints of reported income categories, as in prior analyses.15,25
We defined the expansion group as ACBS participants from states in the dataset that implemented expansion in 2014: Connecticut, Hawaii, Iowa, Massachusetts, Michigan, Nevada, New Hampshire, New Mexico, New York, Ohio, Oregon, Rhode Island, and Vermont. 26 The nonexpansion group comprised participants from states that did not implement expansion in 2014: Florida, Georgia, Kansas, Maine, Missouri, Montana, Nebraska, Texas, Utah, and Wisconsin. 26
We assessed 5 dichotomous outcomes using ACBS questionnaire items 23 : ≥1 routine asthma checkup during the past 12 months, ≥1 visit to an ED or urgent care center for asthma during the past 12 months, ≥1 hospitalization for asthma during the past 12 months, use of rescue inhaler medication (short-acting β-agonist or short-acting anticholinergic medication) during the past 3 months, and use of asthma controller medication (inhaled corticosteroid, long-acting β-agonist, leukotriene modifier, methylxanthine, cromolyn, immunomodulator, or oral corticosteroid medication) during the past 3 months. We selected these 5 outcomes because they often involve the use of health insurance. 14
We used SAS version 9.4-callable SUDAAN version 11.1 (Research Triangle Institute) to address ACBS’s complex survey design. 24 We used ACBS final weights to adjust for loss of sample between BRFSS interviews and ACBS interviews, along with compensating for nonresponse during BRFSS and ACBS interviews.15,22-24 Thus, results were representative of states in the dataset. We calculated weighted percentages and 95% CIs for each outcome, by period (2011-2013, 2015-2019) and group (expansion, nonexpansion). Then, within each group, we conducted descriptive analyses, comparing 2011-2013 estimates with 2015-2019 estimates by using t tests. We then performed quasi-experimental difference-in-differences regression analyses to assess the effect of expansion on each outcome, similar to prior expansion studies.15,25,27-29 This linear regression model compared changes from before to after expansion in states that implemented expansion in 2014 with changes during the same period in states that did not implement expansion that year.15,25 Regression analyses adjusted for race and ethnicity, sex, age, and participating states15,30; these results were calculated as percentage-point changes and SEs. More information about this regression model, which includes an interaction term for each state’s Medicaid expansion status, is available elsewhere. 15 We conducted a sensitivity analysis that excluded data from Maine and Montana, because these states were included in the nonexpansion group per our group definitions (ie, states not implementing expansion in 2014 were considered the nonexpansion group), but these 2 states implemented expansion later during the study period (Maine in 2016, Montana in 2019 26 ). In addition, we aggregated data from expansion and nonexpansion groups to test every outcome for common trend (2011-2019, including 2014), assessing trends using logistic regression analyses and determining inflection points by using JoinPoint Regression version 5.1 (National Cancer Institute).
Exploratory analyses stratified data by race, ethnicity, and sex. In addition, to provide context for these secondary analyses, we conducted analyses of health insurance coverage stratified by race and ethnicity and by sex. Finally, we performed sensitivity analyses that excluded people aged 18-25 years, considering another Affordable Care Act provision extending parents’ private health insurance plan dependent coverage to adults aged <26 years.
For all analyses (including linear time effects for trend analyses), we set the significance level at .05, excluded observations with missing outcome data, and suppressed results when the relative SE was >0.3. 24
Results
This analysis included data from 10 796 unique adults with current asthma and lower incomes, representative of 23 states. Respondents in both the expansion and nonexpansion groups were mostly female and non-Hispanic White (Table 1). Point estimates for the percentage of non-Hispanic Black respondents in both expansion and nonexpansion groups ranged from 14.3% to 19.4% across the entire study period; for Hispanic participants, point estimates ranged from 12.6% to 16.0%. During 2011-2013, 81.2% (95% CI, 76.9%-84.8%) of expansion group participants reported having health insurance, compared with 93.3% (95% CI, 91.2%-94.9%) in 2015-2019. In the nonexpansion group, 70.1% (95% CI, 64.2%-75.3%) of respondents had health insurance in 2011-2013 and 73.5% (95% CI, 69.0%-77.5%) in 2015-2019.
Characteristics of adults aged 18-64 years with current asthma and lower incomes, a by Medicaid expansion status in 2014, Behavioral Risk Factor Surveillance System Asthma Call-Back Survey, 2011-2013 and 2015-2019
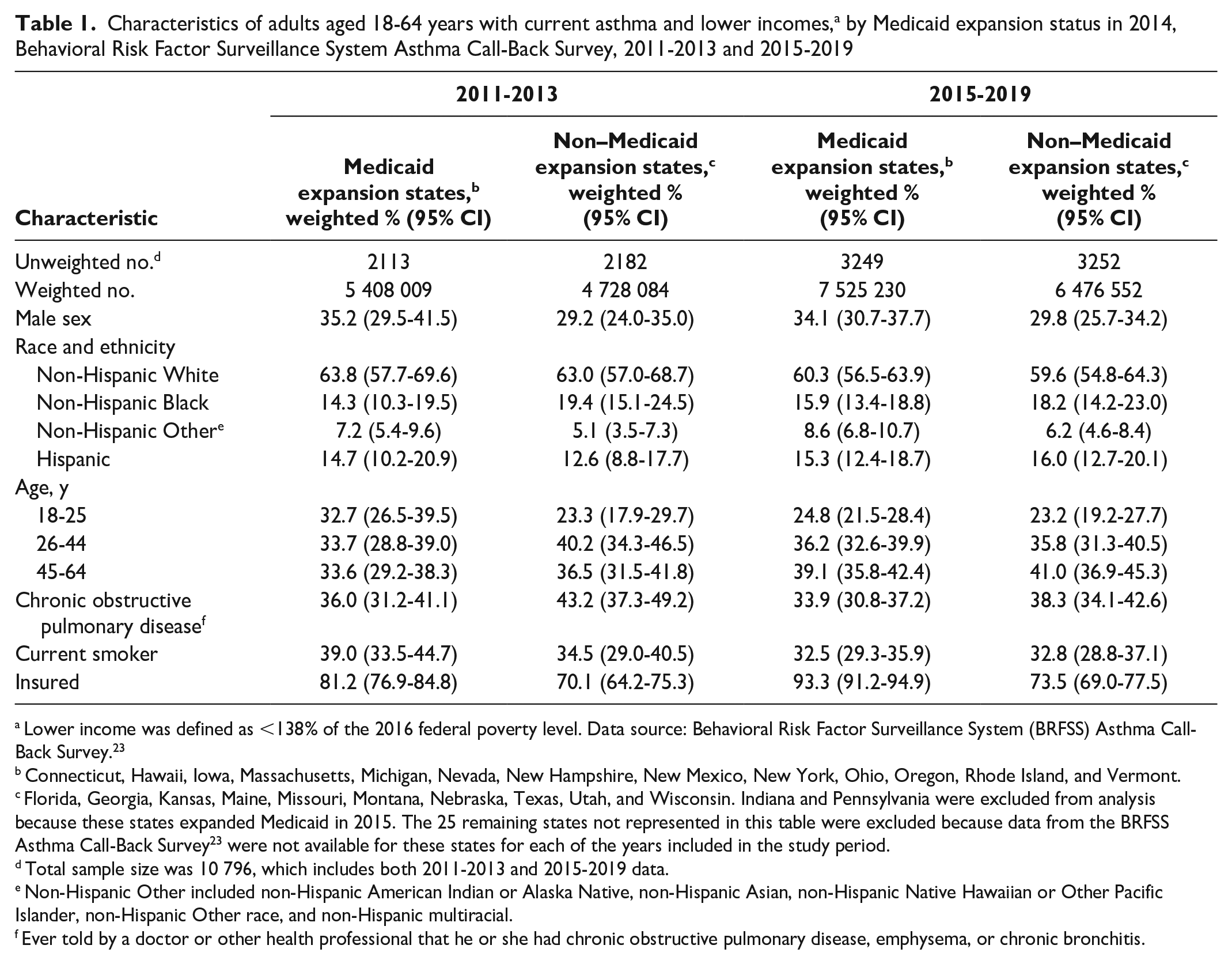
Lower income was defined as <138% of the 2016 federal poverty level. Data source: Behavioral Risk Factor Surveillance System (BRFSS) Asthma Call-Back Survey. 23
Connecticut, Hawaii, Iowa, Massachusetts, Michigan, Nevada, New Hampshire, New Mexico, New York, Ohio, Oregon, Rhode Island, and Vermont.
Florida, Georgia, Kansas, Maine, Missouri, Montana, Nebraska, Texas, Utah, and Wisconsin. Indiana and Pennsylvania were excluded from analysis because these states expanded Medicaid in 2015. The 25 remaining states not represented in this table were excluded because data from the BRFSS Asthma Call-Back Survey 23 were not available for these states for each of the years included in the study period.
Total sample size was 10 796, which includes both 2011-2013 and 2015-2019 data.
Non-Hispanic Other included non-Hispanic American Indian or Alaska Native, non-Hispanic Asian, non-Hispanic Native Hawaiian or Other Pacific Islander, non-Hispanic Other race, and non-Hispanic multiracial.
Ever told by a doctor or other health professional that he or she had chronic obstructive pulmonary disease, emphysema, or chronic bronchitis.
We found no significant differences between 2011-2013 and 2015-2019 for all outcomes that assessed asthma-related medical encounters (routine checkup, ED or urgent care center visit, hospitalization) or medication use (rescue inhaler, asthma controller medication) (Table 2). Adjusted difference-in-differences analyses showed no significant differences between 2011-2013 and 2015-2019 for all outcomes (Table 3); 95% CIs for difference-in-differences analyses included the null. Results were similar in sensitivity analyses excluding Maine and Montana. Results of other sensitivity analyses that excluded people aged 18-25 years did not differ significantly (eTables 1-3 in the Supplemental Material). Common trend testing for all outcomes did not identify any significant linear trends, nor was the year 2014 identified as an inflection point for any outcome.
Weighted percentages of health care use outcomes among adults aged 18-64 years with current asthma and lower incomes, a by Medicaid expansion status in 2014, Behavioral Risk Factor Surveillance System Asthma Call-Back Survey, 2011-2013 and 2015-2019
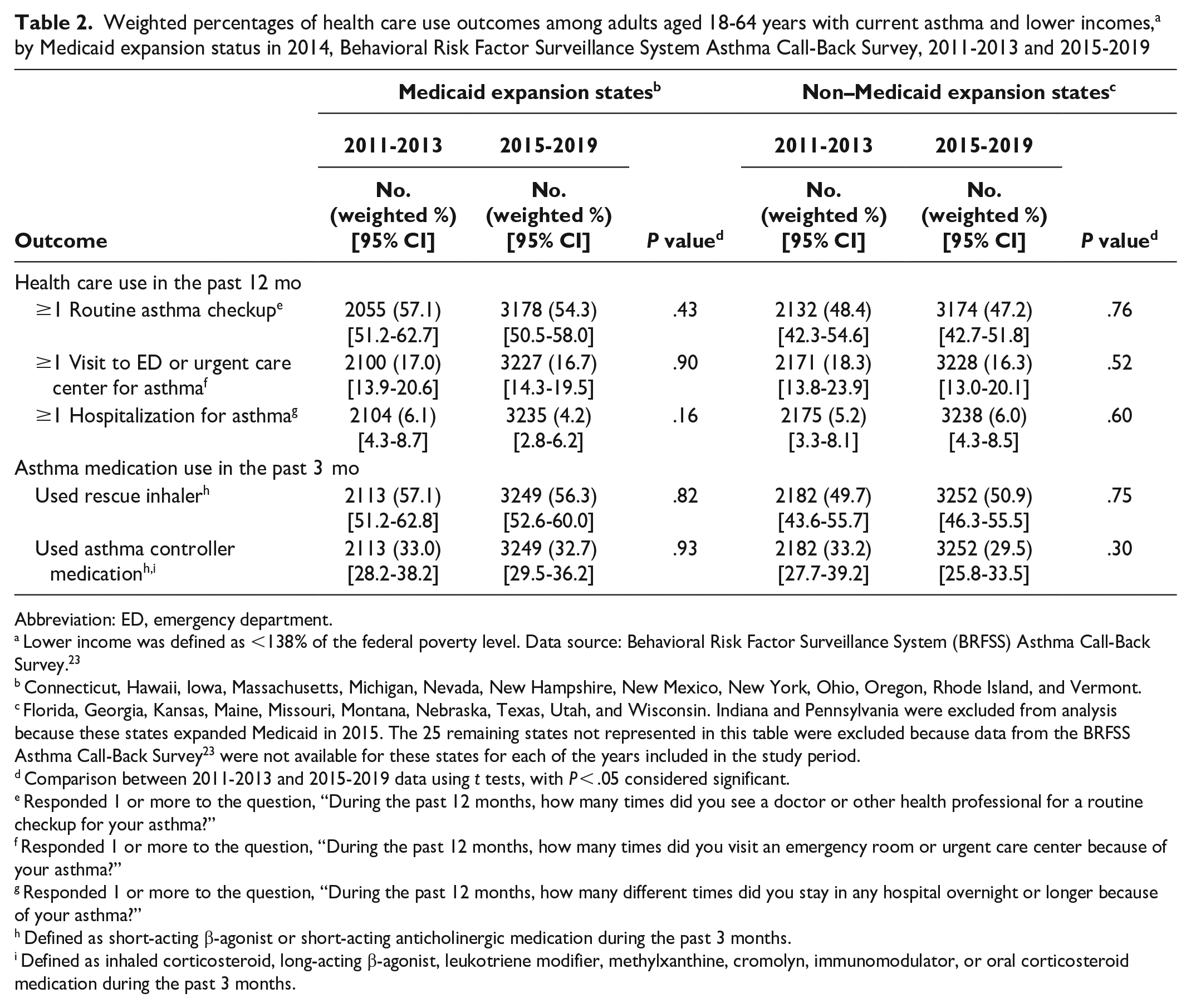
Abbreviation: ED, emergency department.
Lower income was defined as <138% of the federal poverty level. Data source: Behavioral Risk Factor Surveillance System (BRFSS) Asthma Call-Back Survey. 23
Connecticut, Hawaii, Iowa, Massachusetts, Michigan, Nevada, New Hampshire, New Mexico, New York, Ohio, Oregon, Rhode Island, and Vermont.
Florida, Georgia, Kansas, Maine, Missouri, Montana, Nebraska, Texas, Utah, and Wisconsin. Indiana and Pennsylvania were excluded from analysis because these states expanded Medicaid in 2015. The 25 remaining states not represented in this table were excluded because data from the BRFSS Asthma Call-Back Survey 23 were not available for these states for each of the years included in the study period.
Comparison between 2011-2013 and 2015-2019 data using t tests, with P < .05 considered significant.
Responded 1 or more to the question, “During the past 12 months, how many times did you see a doctor or other health professional for a routine checkup for your asthma?”
Responded 1 or more to the question, “During the past 12 months, how many times did you visit an emergency room or urgent care center because of your asthma?”
Responded 1 or more to the question, “During the past 12 months, how many different times did you stay in any hospital overnight or longer because of your asthma?”
Defined as short-acting β-agonist or short-acting anticholinergic medication during the past 3 months.
Defined as inhaled corticosteroid, long-acting β-agonist, leukotriene modifier, methylxanthine, cromolyn, immunomodulator, or oral corticosteroid medication during the past 3 months.
Percentage-point changes in health care use outcomes after Medicaid expansion in 2014, among adults aged 18-64 years with current asthma and lower incomes a (difference-in-differences analyses), Behavioral Risk Factor Surveillance System Asthma Call-Back Survey, 2011-2013 and 2015-2019
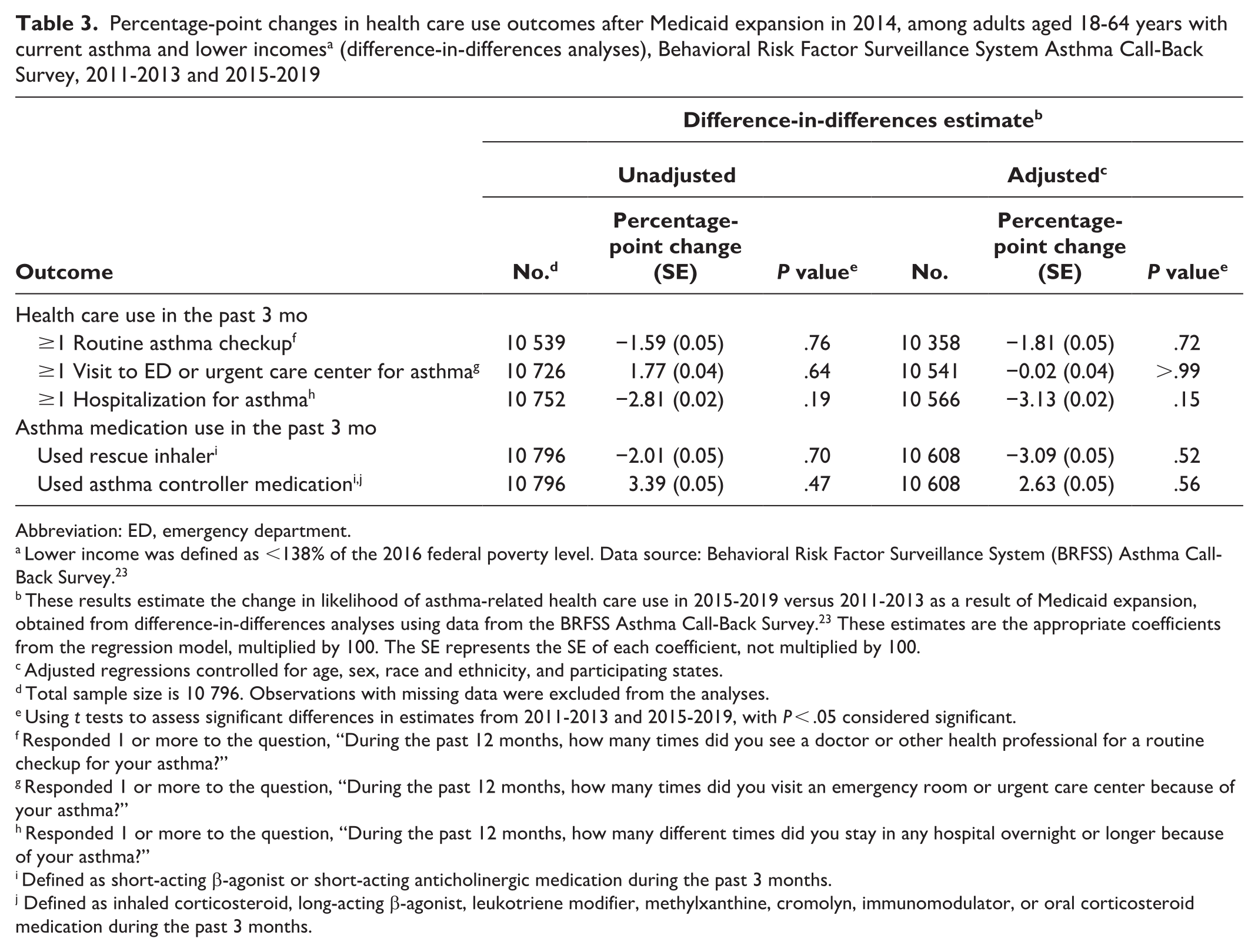
Abbreviation: ED, emergency department.
Lower income was defined as <138% of the 2016 federal poverty level. Data source: Behavioral Risk Factor Surveillance System (BRFSS) Asthma Call-Back Survey. 23
These results estimate the change in likelihood of asthma-related health care use in 2015-2019 versus 2011-2013 as a result of Medicaid expansion, obtained from difference-in-differences analyses using data from the BRFSS Asthma Call-Back Survey. 23 These estimates are the appropriate coefficients from the regression model, multiplied by 100. The SE represents the SE of each coefficient, not multiplied by 100.
Adjusted regressions controlled for age, sex, race and ethnicity, and participating states.
Total sample size is 10 796. Observations with missing data were excluded from the analyses.
Using t tests to assess significant differences in estimates from 2011-2013 and 2015-2019, with P < .05 considered significant.
Responded 1 or more to the question, “During the past 12 months, how many times did you see a doctor or other health professional for a routine checkup for your asthma?”
Responded 1 or more to the question, “During the past 12 months, how many times did you visit an emergency room or urgent care center because of your asthma?”
Responded 1 or more to the question, “During the past 12 months, how many different times did you stay in any hospital overnight or longer because of your asthma?”
Defined as short-acting β-agonist or short-acting anticholinergic medication during the past 3 months.
Defined as inhaled corticosteroid, long-acting β-agonist, leukotriene modifier, methylxanthine, cromolyn, immunomodulator, or oral corticosteroid medication during the past 3 months.
In exploratory, descriptive analyses stratified by race and ethnicity, most differences were not significant (Table 4). For example, use of asthma controller medication among non-Hispanic Black participants in the expansion group increased from 24.1% (95% CI, 14.4%-37.5%) in 2011-2013 to 35.5% (95% CI, 27.0%-45.1%) in 2015-2019 (P = .13). Use of asthma controller medication among non-Hispanic Black participants in the nonexpansion group decreased from 25.7% (95% CI, 17.0%-36.9%) in 2011-2013 to 20.8% (95% CI, 12.9%-31.8%) in 2015-2019 (P = .49). Use of asthma controller medication increased significantly among non-Hispanic Other participants in the nonexpansion group from 16.0% (95% CI, 9.5%-25.5) in 2011-2013 to 40.2% (95% CI, 25.5%-56.8%) in 2015-2019 (P = .01) but not in the expansion group.
Weighted percentages of health care use outcomes among adults aged 18-64 years with current asthma and lower incomes, a by Medicaid expansion status in 2014 and race and ethnicity, Behavioral Risk Factor Surveillance System Asthma Call-Back Survey, 2011-2013 and 2015-2019
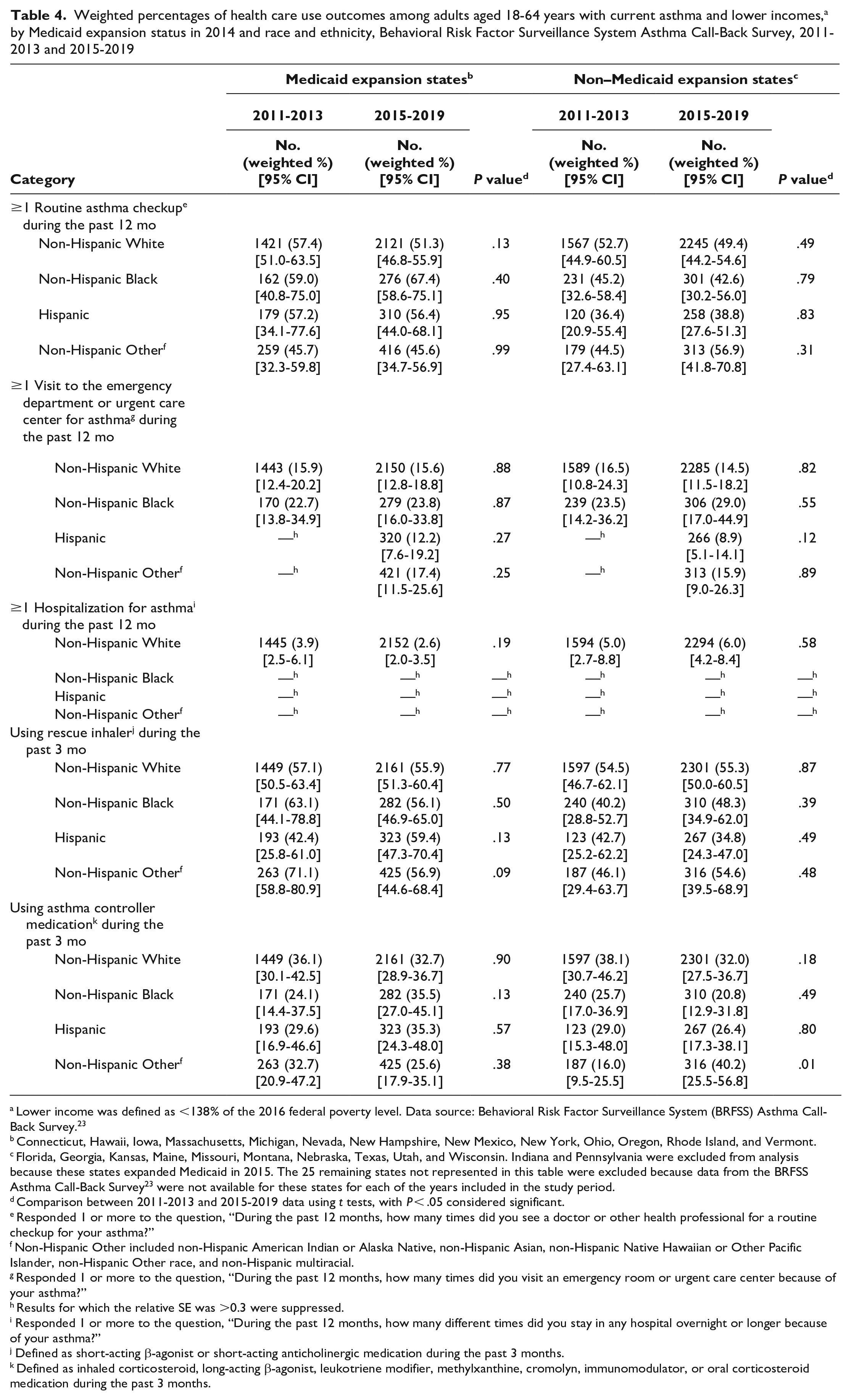
Lower income was defined as <138% of the 2016 federal poverty level. Data source: Behavioral Risk Factor Surveillance System (BRFSS) Asthma Call-Back Survey. 23
Connecticut, Hawaii, Iowa, Massachusetts, Michigan, Nevada, New Hampshire, New Mexico, New York, Ohio, Oregon, Rhode Island, and Vermont.
Florida, Georgia, Kansas, Maine, Missouri, Montana, Nebraska, Texas, Utah, and Wisconsin. Indiana and Pennsylvania were excluded from analysis because these states expanded Medicaid in 2015. The 25 remaining states not represented in this table were excluded because data from the BRFSS Asthma Call-Back Survey 23 were not available for these states for each of the years included in the study period.
Comparison between 2011-2013 and 2015-2019 data using t tests, with P < .05 considered significant.
Responded 1 or more to the question, “During the past 12 months, how many times did you see a doctor or other health professional for a routine checkup for your asthma?”
Non-Hispanic Other included non-Hispanic American Indian or Alaska Native, non-Hispanic Asian, non-Hispanic Native Hawaiian or Other Pacific Islander, non-Hispanic Other race, and non-Hispanic multiracial.
Responded 1 or more to the question, “During the past 12 months, how many times did you visit an emergency room or urgent care center because of your asthma?”
Results for which the relative SE was >0.3 were suppressed.
Responded 1 or more to the question, “During the past 12 months, how many different times did you stay in any hospital overnight or longer because of your asthma?”
Defined as short-acting β-agonist or short-acting anticholinergic medication during the past 3 months.
Defined as inhaled corticosteroid, long-acting β-agonist, leukotriene modifier, methylxanthine, cromolyn, immunomodulator, or oral corticosteroid medication during the past 3 months.
In our secondary analysis of health insurance coverage, we found no significant differences over time among racial and ethnic minority groups in either the expansion or nonexpansion group. However, among non-Hispanic White expansion group members, the prevalence of health insurance coverage increased significantly from 81.8% (95% CI, 76.9%-85.8%) in 2011-2013 to 94.4% (95% CI, 91.6%-96.3%) in 2015-2019 (P < .001).
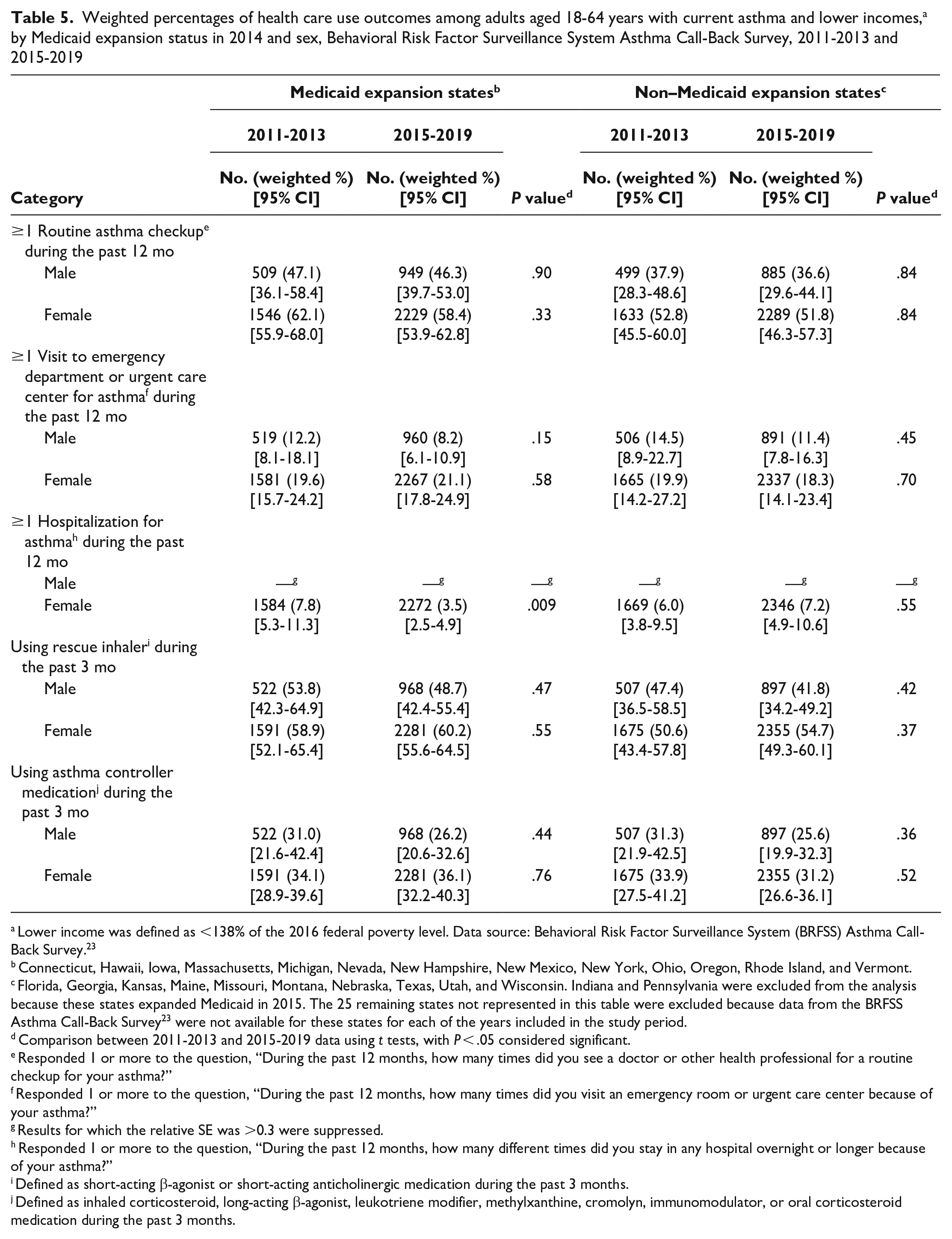
In a secondary analysis stratified by sex, we found a significantly smaller percentage of asthma-related hospitalizations among women in the expansion group after 2014 (2011-2013: 7.8% [95% CI, 5.3%-11.3%]; 2015-2019: 3.5% [95% CI, 2.5%-4.9%]; P = .009) but no significant differences among women in the nonexpansion group (Table 5). Among men in the nonexpansion group, we found no significant differences in asthma-related medical visits (routine, ED, or urgent care center) and asthma medication use. In the expansion group, the prevalence of health insurance coverage among women increased significantly from 2011-2013 (82.1%; 95% CI, 77.3%-86.0%) to 2015-2019 (94.5%; 95% CI, 92.0%-96.2%; P < .001). The prevalence of health insurance coverage among men in the expansion group also increased significantly from 2011-2013 (79.6%; 95% CI, 70.5%-86.5%) to 2015-2019 (91.0%; 95% CI, 86.4%-94.2%; P = .01). We found no significant changes in health insurance coverage among women and men in the nonexpansion group.
Weighted percentages of health care use outcomes among adults aged 18-64 years with current asthma and lower incomes, a by Medicaid expansion status in 2014 and sex, Behavioral Risk Factor Surveillance System Asthma Call-Back Survey, 2011-2013 and 2015-2019
Lower income was defined as <138% of the 2016 federal poverty level. Data source: Behavioral Risk Factor Surveillance System (BRFSS) Asthma Call-Back Survey. 23
Connecticut, Hawaii, Iowa, Massachusetts, Michigan, Nevada, New Hampshire, New Mexico, New York, Ohio, Oregon, Rhode Island, and Vermont.
Florida, Georgia, Kansas, Maine, Missouri, Montana, Nebraska, Texas, Utah, and Wisconsin. Indiana and Pennsylvania were excluded from the analysis because these states expanded Medicaid in 2015. The 25 remaining states not represented in this table were excluded because data from the BRFSS Asthma Call-Back Survey 23 were not available for these states for each of the years included in the study period.
Comparison between 2011-2013 and 2015-2019 data using t tests, with P < .05 considered significant.
Responded 1 or more to the question, “During the past 12 months, how many times did you see a doctor or other health professional for a routine checkup for your asthma?”
Responded 1 or more to the question, “During the past 12 months, how many times did you visit an emergency room or urgent care center because of your asthma?”
Results for which the relative SE was >0.3 were suppressed.
Responded 1 or more to the question, “During the past 12 months, how many different times did you stay in any hospital overnight or longer because of your asthma?”
Defined as short-acting β-agonist or short-acting anticholinergic medication during the past 3 months.
Defined as inhaled corticosteroid, long-acting β-agonist, leukotriene modifier, methylxanthine, cromolyn, immunomodulator, or oral corticosteroid medication during the past 3 months.
Discussion
Our findings suggest that other, unmeasured factors beyond health insurance coverage (eg, social determinants of health4,31 or access to state- or community-based asthma programs promoting asthma awareness or education32-35) might influence the use of asthma-related health care among people with lower incomes. These factors might explain why changes in the prevalence of health insurance coverage did not necessarily translate into improvements in the use of asthma-related health care; such factors might also explain the significant increase in the use of asthma controller medication among non-Hispanic Other respondents in the nonexpansion group despite a nonsignificant increase in health insurance coverage. Improved understanding of these factors and how to address them could augment the impact of expansion as a tool to advance health equity among people with asthma.
Implementing expansion as a key component within a set of strategies could be more effective in reducing asthma disparities than relying on a single strategy. This possibility is supported by existing evidence indicating that clustered interventions and multisectoral collaboration may yield greater impacts in public health efforts to achieve health equity and reduce asthma-related morbidity and mortality than single interventions or single-sector activities.4,31 Thus, state, local, and territorial public health practitioners can use these findings to consider implementing efforts to reduce asthma morbidity while improving health equity. For example, combining expansion with complementary activities (eg, community health worker delivery of culturally competent education on asthma self-management and asthma trigger reduction, plus collaboration with community leaders to raise awareness of these services) could magnify public health impact.
Our results echo the results of prior studies while adding new insights. A study by Shi et al 17 that used national data found no decreases in asthma-related ED visits, hospitalizations, or outpatient visits after states could implement expansion starting in 2014. The use of asthma controller medication increased during this period; data on rescue inhaler medication and preventive controller medication were analyzed in aggregate, unlike the data in our study, in the study by Shi et al. 17 In addition, the study by Shi et al 17 did not account for whether individual states implemented expansion. These methodologic differences and distinct study populations might explain the differences between our study and previous analyses. Shi et al 17 presented race-stratified data, whereas we stratified data by race and ethnicity. A study by Hsu et al 15 compared data from 2012-2013 with data from 2015-2016 and found that expansion was associated with an increased prevalence of health insurance coverage among adults with asthma and lower incomes. However, relationships between expansion and cost barriers to asthma-related care were not significant. 15 The previously reported modest impact of expansion on reducing cost barriers to asthma-related care might explain our findings on expansion and use of asthma-related health care.
Beyond asthma, studies have generally found that expansion has reduced morbidity and mortality associated with certain health conditions (eg, cardiovascular disease, liver disease, some cancer types).14,36 Our dissimilar data on asthma-related health care use might be explained by study limitations or asthma-specific considerations (eg, asthma inhaler copayments or technique).4,15,32,35 Health insurance copayments for medical encounters (eg, ED or urgent care) could also affect asthma-related health care use. 37 The availability and accessibility of health care providers participating in Medicaid programs is another potential barrier to asthma-related health care use.14,38
Strengths and Limitations
This study had several limitations. First, the cross-sectional design precluded assessments of causality and there was an inability to assess Medicaid coverage, mitigated by including only people with lower incomes. Second, the survey design measured income level but did not examine other social determinants of health that could influence asthma-related health care use; as such, we could not determine how these factors influenced asthma-related health care use. Third, because data were self-reported, misclassification was possible. Fourth, nonresponse bias might have affected results; however, this possibility was reduced by using analytic sampling and weighting procedures. Fifth, the sample size precluded difference-in-differences analyses stratified by race, ethnicity, and sex. Also, sample size limited the study’s statistical power to detect weak-to-moderate differences between groups. Finally, our findings might not be generalizable to states outside our investigation.
This study also had several strengths, including its population-based study design, weighted statistical analyses to yield results representative of the populations in all 23 included states, difference-in-differences analyses to decrease the possible impact of unmeasured confounding, and multiple sensitivity analyses addressing various considerations. These results increase knowledge about expansion and asthma in general as well as the potential impact of expansion as a strategy to advance health equity for adults with asthma and lower incomes.
Conclusions
This investigation did not find strong relationships between Medicaid expansion and asthma-related health care use among adults with asthma and lower incomes from 23 states. Exploratory analyses stratified by race, ethnicity, and sex indicate some complex relationships between health insurance coverage and outcomes of asthma-related health care use. These findings increase knowledge about expansion as a strategy to advance health equity for adults with asthma and lower incomes. Also, these results highlight opportunities to learn more about factors beyond health insurance coverage (eg, social determinants of health) that might influence asthma-related health care use among people with lower incomes. With this knowledge, implementing expansion as a key component within a set of strategies could further reduce long-standing disparities in asthma. State, local, and territorial public health practitioners can use these findings when considering the implementation of efforts to reduce asthma-related morbidity and mortality while improving health equity.
Supplemental Material
sj-docx-1-phr-10.1177_00333549241228501 – Supplemental material for Medicaid Expansion and Health Care Use Among Adults With Asthma and Low Incomes: The Adult Asthma Call-Back Survey
Supplemental material, sj-docx-1-phr-10.1177_00333549241228501 for Medicaid Expansion and Health Care Use Among Adults With Asthma and Low Incomes: The Adult Asthma Call-Back Survey by Xiaoting Qin, Maria C. Mirabelli, W. Dana Flanders and Joy Hsu in Public Health Reports
Footnotes
Disclaimer
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online. The authors have provided these supplemental materials to give readers additional information about their work. These materials have not been edited or formatted by Public Health Reports’s scientific editors and, thus, may not conform to the guidelines of the AMA Manual of Style, 11th Edition.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.