
Abstract
Objective
The Veterans Health Administration established comprehensive women’s health clinics (CWHCs) to provide coordinated, high-quality primary care to women veterans. Intimate partner violence (IPV) is prevalent among women using these clinics. The Veterans Health Administration recommends screening women for IPV, yet screening uptake is low in CWHCs nationwide. We describe a multisite quality improvement initiative to enhance the adoption of IPV screening practices in the Veterans Health Administration’s CWHCs.
Methods
This quality improvement initiative, implemented in 2017-2018, included 4 steps in which we (1) conducted a baseline survey of screening practices at CWHCs throughout the United States; (2) selected and tailored evidence-based implementation strategies based on identified barriers and facilitators; (3) deployed multicomponent implementation support, targeting low-adopting facilities; and (4) conducted a follow-up survey to evaluate changes in IPV screening practices from baseline (winter 2017) to 1-year follow-up (winter 2018) using quantitative and qualitative analyses.
Results
Responders from 62 CWHC sites provided information on IPV screening practices and barriers; 42 low-adopting sites were targeted for implementation support. At follow-up, responders provided information on IPV screening practices, perceived usefulness of implementation support strategies, and continued barriers. Among sites that responded to both surveys (n = 47), the number of sites that implemented recommended screening practices increased by 66.7%, from 15 at baseline to 25 at follow-up (P = .02). Emergent themes reflected barriers and facilitators for IPV screening implementation.
Conclusions
Improvement in IPV screening practices in CWHCs is a pivotal step toward enhancing care for women. Yet, even with numerous implementation supports, barriers to adoption persist at many sites. Findings on modifiable barriers and unique facilitators can inform next steps for increasing screening uptake.
Keywords
Intimate partner violence (IPV), including physical, sexual, and psychological aggression against a current or past partner, 1 is a major public health concern. Women’s IPV experiences are associated with negative physical health outcomes (eg, cardiovascular and respiratory problems, chronic pain, reproductive health complications) and poor mental health outcomes (eg, posttraumatic stress, anxiety, depression, substance use, suicidality).2-6 Women veterans experience IPV at higher rates than non-veterans (33% vs 24%). 7
The Veterans Health Administration (VHA) is the largest integrated health care system in the United States. The use of VHA health care by women veterans has grown rapidly: the number of women primary care users nearly tripled from 2000 to 2015, from 159 810 users in 2000 to 439 791 users in 2015. 8 This expansion in use increases the VHA’s potential to reach more women veterans. As of 2015, approximately 2 million women veterans were residing in the United States or Puerto Rico. 9 Although the overall number of veterans is expected to decrease from 2015 to 2025, the women veteran population is expected to increase at a rate of approximately 18 000 women per year; women veterans will be the fastest-growing cohort in the veteran community, and an increasing portion of women veterans will be accessing VHA care. 9 Specifically, 425 982 women veterans used VHA outpatient services in 2015, compared with 155 430 women veterans in 2000, representing nearly a 3-fold increase in use. 8 As such, the VHA has a critical role to play in the prevention, identification, and treatment of key health problems, such as IPV, that affect women veterans. 10
Women veterans access VHA primary care through typical mixed-sex ambulatory care settings, as well as through comprehensive women’s health clinics (CWHCs), which provide interdisciplinary primary and specialty care in a dedicated space. At the time of this quality improvement evaluation, the VHA had 82 CWHCs. Rates of lifetime IPV among women veterans accessing CWHCs are as high as 74%. 11 Because CWHCs provide on-site interdisciplinary care (including mental health and social work), they are ideal settings for IPV screening programs. Screening women in these clinics is feasible and provides opportunities for education, referral, and intervention. 12 Women veterans perceive such practices as supportive, validating, and helpful, and they believe screening promotes readiness to disclose their experiences and access IPV-related services.13,14
Consistent with the US Preventive Services Task Force recommendation, 15 VHA’s IPV screening guidance, issued in 2013, advised medical providers to screen women of childbearing age annually. 16 However, uptake of IPV screening recommendations for women veterans has been inconsistent across the VHA, and not all medical centers have implemented routine IPV screening. Earlier research among VHA primary care providers reported barriers to IPV screening, including time constraints, lack of education and training, concerns about coordination of care after IPV disclosures, and lack of screening tools embedded into the electronic medical record. 17 Given the high prevalence of IPV among women veterans, VHA’s Office of Women’s Health Services (WHS) led an initiative to improve the adoption of IPV screening at CWHCs. We describe and evaluate the helpfulness of WHS’s quality improvement program for CWHCs and share lessons for implementation of similar screening programs in the VHA and other settings.
Description and Purpose of the Program Being Evaluated
In 2013, the newly created VHA IPV Assistance Program 16 published guidelines recommending that women of reproductive age be screened at least annually with the 5-item E-HITS (Extended–Hurt, Insult, Threaten, Scream) instrument, the accuracy of which has been validated among women veterans. 18 Despite identification of IPV as an important national priority, research focusing on IPV among women VHA patients suggests low uptake of IPV screening as of 2016. 19 In an effort to achieve universal screening across the VHA, the WHS undertook a 4-step initiative in 2017 to enhance adoption and sustain implementation of IPV screening. The initial target for the initiative was CWHCs, because they serve a higher percentage of women veterans than sites with mixed-sex ambulatory care settings only.
Evaluation of this national initiative will enable dissemination of knowledge that may help spread and sustain IPV screening practices in the VHA and beyond. The goals of the evaluation were to (1) establish a baseline of IPV screening practices and identify barriers to screening at CWHCs nationwide; (2) select and tailor evidence-based implementation support strategies 20 based on these baseline data to bolster the spread of IPV screening at CWHCs, targeting clinics that had yet to adopt IPV screening practices into routine care; (3) deploy implementation support, including technical assistance and toolkit dissemination, to sites that had not yet implemented IPV screening; and (4) determine IPV screening practices after implementation support efforts, elucidating both facilitators of and barriers to screening. After deploying these strategies in CWHCs, we conducted a follow-up survey to assess uptake of IPV screening practices 1 year after the baseline survey.
Methods
Baseline Recruitment and Materials
During initial outreach to the 82 CWHC sites in VHA medical centers, we contacted key informants from 67 (81.7%) CWHCs (Figure). For the purposes of this study, we considered key informants to be women’s health medical directors and women veterans program managers. We could not reach 15 sites for several reasons, including vacancies in these key informant positions, having no available contact information for the key informant, and key informants on leave with no information about whom to contact in their absence. We used a modified 4-stage process 21 to recruit key informants from CWHCs. First, the deputy director of comprehensive women’s health (S.G.H.) sent an email to 72 identified contacts explaining the project and requesting completion of the baseline survey; a link to the survey was embedded in the email. Eight emails were returned because of delivery failures; of these sites, we were able to correct the email address or identify another point of contact at 3 sites, resulting in a 67-site final sample. Second, the project team sent a reminder email to the 67 sites requesting survey completion. Third, project team members contacted each nonresponding site via email to request survey completion. Fourth, project team members attempted to contact remaining nonresponding sites by telephone, leaving a maximum of 2 voicemail messages for the key informants if there was no answer. We completed stages 1 through 3 during 4 weeks and stage 4 during the following 2 weeks. We administered a brief baseline survey to each of the 67 sites in winter 2017. Survey instructions notified informants that their responses would inform future program planning. This project did not require institutional review board approval or a waiver because the information was not collected for research purposes but as part of a national quality improvement project overseen and directed by the third author (S.G.H.).
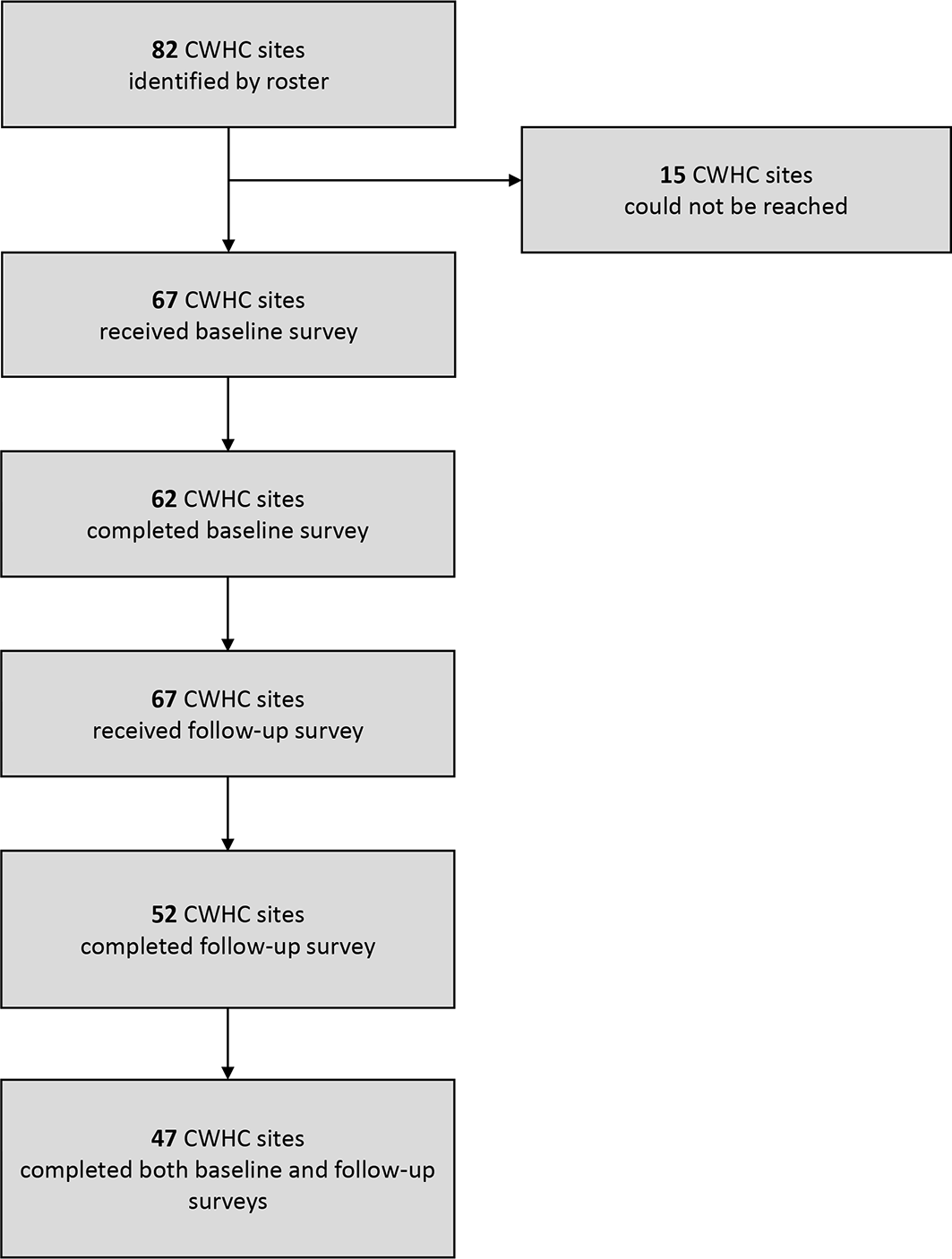
Respondents to a baseline survey and follow-up survey administered as part of an initiative conducted by the Veterans Health Administration’s Office of Women’s Health Services to enhance the adoption of screening practices for intimate partner violence into routine primary care for women veterans. The baseline survey was administered in winter 2017 and a follow-up survey 1 year later, in winter 2018, after the provision of implementation support. Abbreviation: CWHC, comprehensive women’s health clinic.
The baseline survey collected the following information from each CWHC site: current screening practices, the instrument used for screening, the discipline of health care providers who completed screenings, support services for women who disclose IPV, perceived barriers to IPV screening, the name of the CWHC site, and the role of the survey respondent at the CWHC. We created a list of potential barriers to IPV screening by synthesizing a list of barriers identified by VHA health care providers in previous research. 17 Respondents could write in additional barriers. The survey also included an open-ended format for supplying feedback about the initiative or sharing contextual details about IPV screening adoption at their site.
Implementation Support Strategies
Findings from the baseline data guided subsequent selection and use of implementation strategies to enhance adoption of IPV screening practices in CWHCs. We used the baseline survey to identify sites that had not implemented IPV screening consistent with recommendations 16 (ie, screening women of childbearing age and/or all women annually) or did not respond to the survey. Using this information, we developed a roster of 42 low-adopting sites to target for implementation support. We then used 4 evidence-based strategies to enhance adoption of IPV screening among low-adopting sites. These strategies included using 2 web-based, interactive training sessions facilitated by the WHS project team, an IPV screening toolkit, coaching calls, and an IPV screening grant.
The web-based, facilitated interactive training sessions consisted of a review of the baseline survey results and IPV screening expectations and offered information on implementation strategies developed to address the barriers identified in the survey. Facilitators encouraged discussion and sharing of experiences and successful practices among participants. The training session included time for sites to ask questions, which were answered by a subject matter expert from a CWHC with a high level of compliance with IPV screening recommendations. Project team members were available for follow-up questions via email and telephone meetings.
The IPV screening toolkit included the VHA-recommended IPV screening tool, examples of an IPV screening protocol and safety plan, a detailed description for embedding the screening tool into an electronic medical record system (including screen shots of the electronic medical record template), and other IPV educational materials (eg, patient handouts, health care provider education).
During coaching calls, the low-adopting sites had the opportunity to discuss and trouble-shoot local issues with project team members from WHS and staff members from CWHC sites that were successfully implementing IPV screening into routine care.
Together with VHA’s National IPV Assistance Program through the Office of Care Management and Social Work, we posted a call for proposals for a $3000 grant to support efforts to increase implementation of IPV screening. We invited the 42 low-adopting CWHCs to participate in all 4 implementation support activities. Technical assistance for all aspects of screening implementation occurred during 8 months. In total, 21 sites participated in the web-based training sessions, and many sites took advantage of the coaching calls and toolkits, although we did not record these data. Seven of 10 sites that applied for the grant received it.
Follow-up Procedures and Materials
We conducted a follow-up survey 1 year after the baseline survey (in winter 2018) to (1) evaluate changes in IPV screening practices from baseline to follow-up, (2) identify barriers to screening implementation, and (3) assess whether high-adopting sites maintained IPV screening practices consistent with VHA recommendations. In winter 2018, we contacted key informants from the original sample of 67 CWHCs via email with an embedded link requesting completion of the follow-up survey.
The brief follow-up survey collected the same information assessed at baseline; it also asked questions about the usefulness of the implementation support strategies and requested additional feedback. The survey again included an option for an open-ended response for each item and an open-ended question asking responders to indicate anything else they would like to share about IPV screening implementation at their CWHC.
Data Analysis
We used univariate analyses to assess the rates of IPV screening adoption and instruments used at baseline. We used the McNemar χ2 test on matched data to compare baseline and follow-up survey responses. This test allowed us to determine significant differences in IPV screening practices before and after the provision of implementation support (with a P value of < .05 considered significant). Not all sites responded to both surveys; some sites were lost to follow-up, and some sites that responded at follow-up did not respond to the baseline survey; we included in χ2 analyses only sites with data on each variable at both time points. To analyze write-in responses, we conducted an inductive thematic content analysis 22 to identify barriers to IPV screening implementation reported at follow-up across CWHC sites.
Results
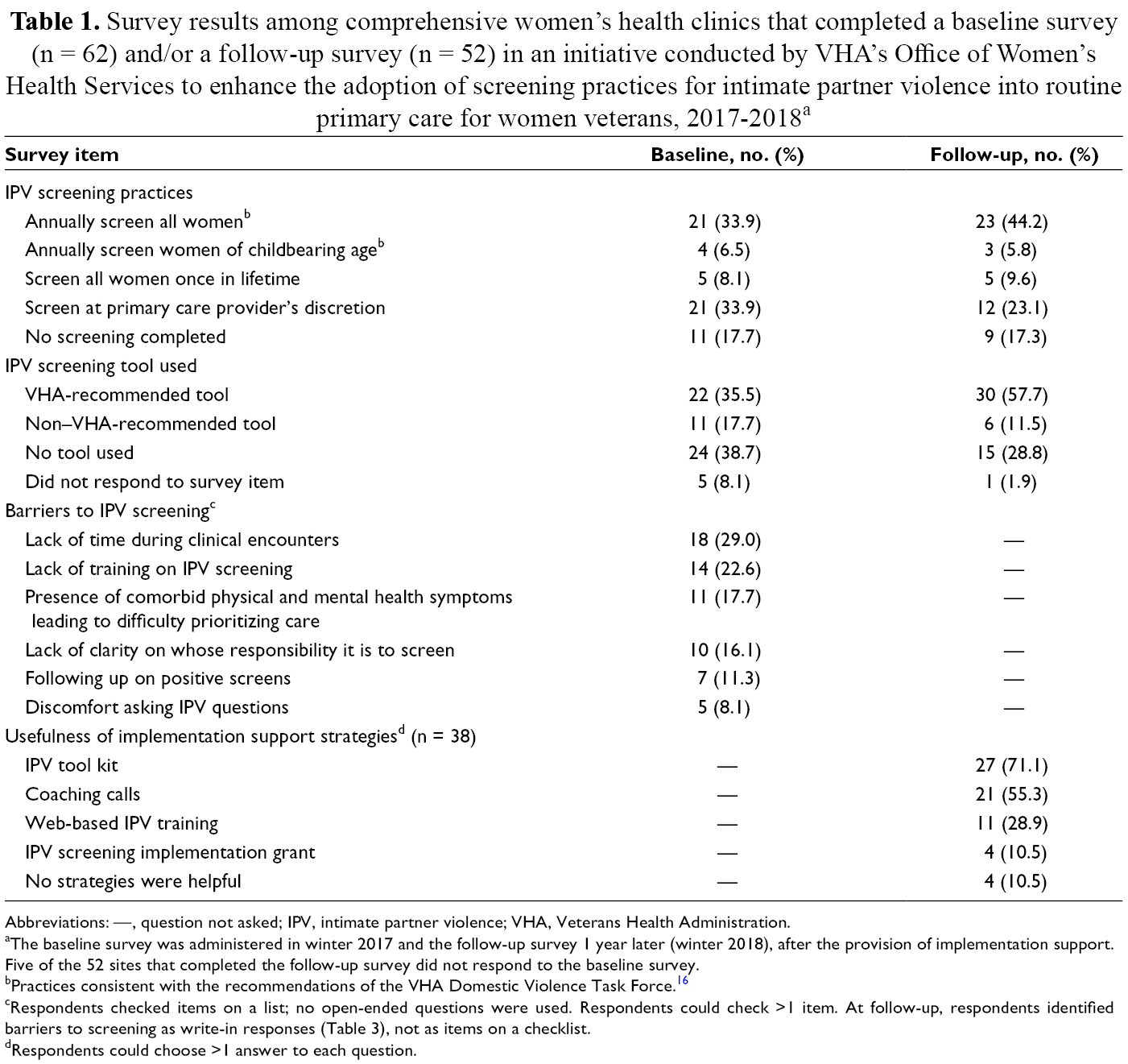
Of 67 VHA sites reached, 62 completed the baseline survey (92.5% participation rate). Of the 62 sites, 25 (40.3%) reported engaging in screening practices consistent with recommendations (ie, screening either all women or women of childbearing age annually); 37 (59.7%) reported screening women for IPV once in their lifetime, screening for IPV at the discretion of the primary care provider only, or not routinely screening patients for IPV. Twenty-two sites (35.5%) reported using VHA’s recommended tool. However, 35 sites (56.4%) reported either using a non–VHA-recommended tool or not using a screening tool at all; 5 sites did not respond to this survey item.
The most commonly identified barrier to IPV screening adoption at baseline was lack of time during clinical encounters (29.0%; 18 sites) (Table 1). Three other major barriers were lack of training on IPV screening (22.6%; 14 sites), presence of comorbid physical and mental health symptoms leading to difficulty prioritizing care (17.7%; 11 sites), and lack of clarity on whose responsibility it is to screen (16.1%; 10 sites). Other barriers were being unclear about what to do or offer in response to disclosures (11.3%; 7 sites) and discomfort asking questions about IPV (8.1%; 5 sites).
Survey results among comprehensive women’s health clinics that completed a baseline survey (n = 62) and/or a follow-up survey (n = 52) in an initiative conducted by VHA’s Office of Women’s Health Services to enhance the adoption of screening practices for intimate partner violence into routine primary care for women veterans, 2017-2018 a
Abbreviations: —, question not asked; IPV, intimate partner violence; VHA, Veterans Health Administration.
aThe baseline survey was administered in winter 2017 and the follow-up survey 1 year later (winter 2018), after the provision of implementation support. Five of the 52 sites that completed the follow-up survey did not respond to the baseline survey.
bPractices consistent with the recommendations of the VHA Domestic Violence Task Force. 16
cRespondents checked items on a list; no open-ended questions were used. Respondents could check >1 item. At follow-up, respondents identified barriers to screening as write-in responses (Table 3), not as items on a checklist.
dRespondents could choose >1 answer to each question.
Follow-up Survey Results
Fifty-two of 67 sites completed the follow-up survey (77.6% participation rate). Of these sites, 26 (50.0%) reported screening either all women or women of childbearing age annually (Table 1). The other half of sites reported screening women for IPV once in their lifetime (5 sites), screening for IPV at the discretion of the primary care provider only (12 sites), or not routinely screening patients for IPV (9 sites). Thirty (57.7%) sites reported using VHA’s recommended screening tool, whereas 6 sites (11.5%) reported using a non–VHA-recommended tool and 15 sites (28.9%) reported not using a screening tool at all; 1 site did not respond to this survey item.
Change in Screening Practices
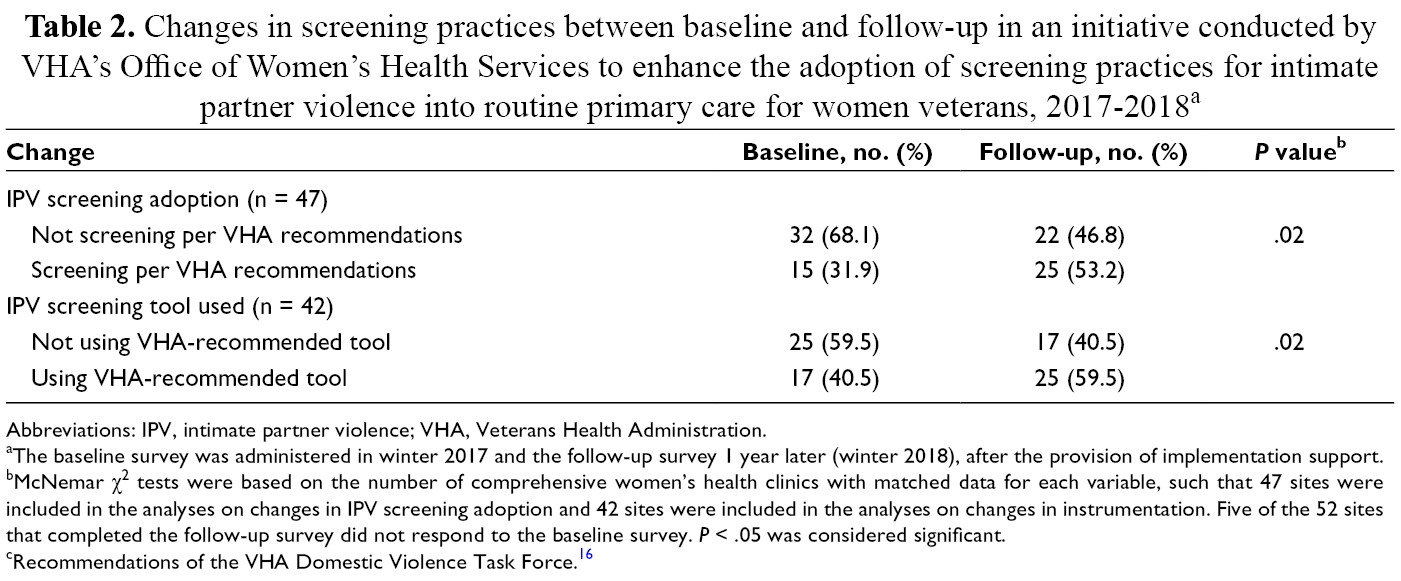
Although 52 sites completed the follow-up survey, 5 of these sites did not complete the baseline survey (Table 2). Of the 47 sites that responded to the question on IPV screening adoption in both surveys, the number of sites adopting routine IPV screening increased by 66.7% (from 15 to 25) from baseline to follow-up, a significant increase in screening adoption (P = .02). Although 13 new sites implemented IPV screening during the year, 3 sites discontinued screening. Twenty-six sites (55.3%) reported using VHA’s recommended screening tool in the follow-up survey. Of the 42 sites that responded to the question on the IPV screening tool used in both surveys, the number of sites that used the VHA-recommended tool increased significantly from 17 to 25 (P = .02) from baseline to follow-up. Nine sites began implementing the VHA-recommended tool during the study period, and 1 site discontinued its use.
Changes in screening practices between baseline and follow-up in an initiative conducted by VHA’s Office of Women’s Health Services to enhance the adoption of screening practices for intimate partner violence into routine primary care for women veterans, 2017-2018 a
Abbreviations: IPV, intimate partner violence; VHA, Veterans Health Administration.
aThe baseline survey was administered in winter 2017 and the follow-up survey 1 year later (winter 2018), after the provision of implementation support.
bMcNemar χ2 tests were based on the number of comprehensive women’s health clinics with matched data for each variable, such that 47 sites were included in the analyses on changes in IPV screening adoption and 42 sites were included in the analyses on changes in instrumentation. Five of the 52 sites that completed the follow-up survey did not respond to the baseline survey. P < .05 was considered significant.
cRecommendations of the VHA Domestic Violence Task Force. 16
Perceptions of the Usefulness of Implementation Support
Of the 38 sites that responded at follow-up to the survey item on the usefulness of implementation support efforts, 34 (89.5%) found at least 1 resource to be useful. Twenty-seven (71.1%) sites identified the IPV toolkit as the most useful resource. The next most useful resource was direct contact with subject matter experts and other peer CWHCs that had successfully implemented screening at their sites (55.3%, 21 sites). Eleven (28.9%) sites indicated that the interactive web-based training sessions were useful, and 4 (10.5%) sites indicated that receiving the IPV screening implementation grant was useful.
Barriers to and Facilitators of IPV Screening Implementation
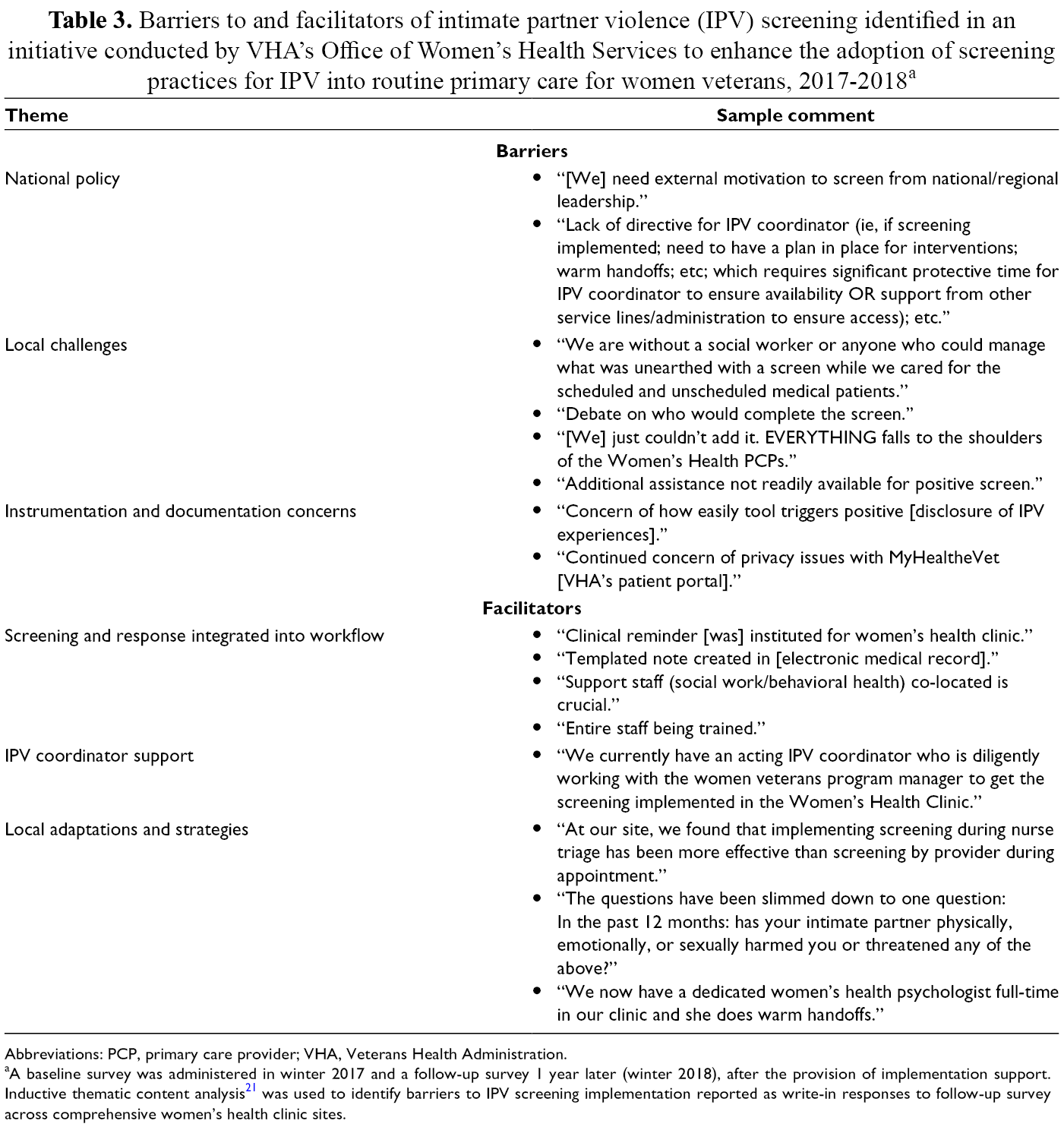
On the follow-up survey, 37 of 52 (71.2%) sites provided at least 1 open-ended response. Thematic analysis of these responses revealed dominant themes on barriers to and facilitators of IPV screening adoption (Table 3). Barriers included national policy (recommendations vs mandate or directive), especially related to the desire for support of leadership and a national IPV screening directive; local challenges, such as concerns about staffing, including burden to staff members; and instrumentation and documentation concerns, such as concerns about the sensitivity of the VHA-recommended screening tool (eg, the tool may overestimate the occurrence of IPV) and patient privacy. Facilitators included having IPV screening and response integrated into workflow through reminders and templated notes embedded into the electronic medical record; co-located IPV coordinator support; adequate training; and local adaptations and strategies used by sites, including changes to screening workflow and the screening process itself.
Barriers to and facilitators of intimate partner violence (IPV) screening identified in an initiative conducted by VHA’s Office of Women’s Health Services to enhance the adoption of screening practices for IPV into routine primary care for women veterans, 2017-2018 a
Abbreviations: PCP, primary care provider; VHA, Veterans Health Administration.
aA baseline survey was administered in winter 2017 and a follow-up survey 1 year later (winter 2018), after the provision of implementation support. Inductive thematic content analysis 21 was used to identify barriers to IPV screening implementation reported as write-in responses to follow-up survey across comprehensive women’s health clinic sites.
Lessons Learned
This national quality improvement project demonstrated the state of IPV screening practices in a sample of VHA CWHCs, changes in screening practices over time, and barriers to screening adoption at follow-up. At baseline, fewer than half of CWHCs in the sample engaged in IPV screening. Guided by findings from the baseline survey, the WHS project team provided education and technical assistance through web-based training sessions, dissemination of an IPV screening toolkit, coaching calls with WHS or peer sites, and grant opportunities to enhance uptake of IPV screening. At follow-up, most sites reported that various implementation support strategies recommended during the study period were useful. At follow-up, more than half of the sites reported IPV screening practices consistent with VHA’s recommendations.
Although improvement in screening practices is a pivotal step toward broader uptake of IPV screening, continued barriers to screening exist at many VHA sites. Survey respondents in our study reported IPV screening barriers similar to barriers identified in previous VHA research17,23 and in non-VHA health care settings.15,24-26 Our findings extend this literature by illustrating challenges identified by health care providers at CWHCs, clinics uniquely positioned to address women veterans’ health needs.
Survey respondents identified site-specific factors, such as uncertainty about which staff member is responsible for conducting IPV screening, staff concerns about the added workload screenings could generate, and inadequate training. Two sites that reported discontinuing IPV screening at follow-up indicated that they did so because staff turnover resulted in the need to retrain staff members in how to conduct screenings. Survey respondents also noted concerns about the VHA screening protocol; several sites indicated worry about the sensitivity of VHA’s recommended screening tool, and others noted documentation concerns. Many of the barriers noted are modifiable; thus, targeted, site-specific support may help to overcome them.
Lessons can be learned from the sites that reported successful screening implementation through such strategies as integrating IPV screening into clinic workflow, co-locating additional staff members to conduct screening, providing training on IPV screening to all staff members, and adapting screening procedures to fit the unique conditions at their site. These successful IPV screening strategies can help guide screening implementation at other low-adopting sites.
Although IPV screening adoption significantly increased at the CWHC sites during the time of implementation support, 9 of 52 sites had not adopted any IPV screening at follow-up. Thus, a continued need exists to enhance adoption rates of IPV screening if the VHA is to reach its goal of screening all women veterans annually. In addition, although this quality improvement project was conducted in CWHCs, not all VHA medical centers have such clinics. Most women veterans receive primary care from designated women’s health primary care providers in general primary care (mixed-sex) clinics. We believe that the barriers identified by the sites exclusively serving women veterans (CWHCs) likely extend to health care providers at other clinics, where screening uptake may be even lower. Expanding commitment to IPV screening among all VHA primary care sites is crucial and would optimize the quality of care for women veterans.
Many identified barriers to screening reflect systems-level factors, such as lack of institutional support and a national IPV screening directive. Supportive local leadership is essential in the successful implementation of any novel practice and can advocate for adequate staffing resources, protected time for IPV screening, and continued training for health care providers and women’s health teams. Low-adopting VHA sites indicated such a need for a national directive, which they may feel is essential to leverage and negotiate redistribution of resources for IPV screening. Without a formal mandate, sites not only lacked clarity about IPV screening procedures but also felt unempowered to advocate for additional resources and support for IPV screening.
Limitations
Our study had several limitations. First, although we observed significant differences in IPV screening practices between baseline and follow-up, we cannot, with certainty, attribute these differences to implementation efforts and support. Second, although we collected data on the perceived usefulness of the implementation strategies, we do not know the extent to which each strategy was used by sites and affected adoption. Third, this project reflects a programmatic evaluation that necessitated the identification of low-adopting sites to target for implementation support. As such, we did not collect data anonymously; therefore, the data may reflect a social desirability and/or nonresponse bias. Sites that had successfully implemented IPV screening may have been more interested in participating in our survey than sites that had not implemented IPV screening. We cannot ascertain the extent to which responses would have differed had the survey been administered anonymously. Future studies of IPV screening implementation should consider methods to preserve anonymity. Fourth, our findings may have been skewed by missing data from the 15 CWHC sites that could not be reached for the baseline survey and the sites lost to follow-up. Finally, we did not use a formal facilitated implementation approach; thus, we did not systematically track coaching calls and other such assistance contacts. Rather, we delivered technical assistance in an ad hoc fashion across sites. Future work will include a formal facilitated implementation.
Conclusion
Improving access to and quality of care for women veterans is a major VHA priority. Despite the prevalence of IPV among women veterans, IPV screening programs have had low levels of adoption across VHA primary care clinics. This multisite quality improvement initiative provided useful information about barriers, facilitators, and lessons learned for IPV screening implementation in VHA CWHCs. As the largest integrated health care system in the United States, the VHA has the opportunity to identify best practices for IPV screening that can serve as a national model. Addressing the modifiable barriers reported in our study can increase the success of future efforts to support IPV screening implementation throughout all of primary care in the VHA. Accordingly, early IPV detection and response will enhance women veterans’ quality of care and connection to needed resources while reducing health care costs and improving the health and well-being of women. In early 2019, the VHA published a directive mandating IPV screening 27 ; it will be important to monitor the uptake and sustainment of IPV screening in the VHA and evaluate whether this national policy affects IPV screening practices across VHA care settings.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.