
Abstract
Substantial literature has examined the effectiveness of intimate partner violence (IPV) interventions, and cognitive behavioral therapy (CBT) is noted as the second most common approach used in group interventions for partner violent men. However, as little research has examined how CBT principles are operationalized across program curricula, there is currently insufficient information from which to make recommendations for model CBT approaches in IPV interventions. In the current study, we review the literature to determine a set of core elements for comprehensive CBT interventions and use session-level curriculum data from 10 community-based programs to examine the presence of 14 components reflecting 4 CBT factors. Results suggest heterogeneity in the emphasis on CBT elements across programs, despite almost all managers listing CBT as a theoretical approach. Implications are discussed with a call for evaluators and meta-analysts to code for actual curriculum content as opposed to stated program labels.
Keywords
Introduction
Intimate partner violence (IPV) is a complex and multifaceted problem. The scope of IPV is far-reaching, and the deleterious consequences of partner violence have been discussed at length in the literature (Peterson et al., 2019; Trygged et al., 2014). IPV typically refers to any act of physical violence (e.g., punching, choking, slapping) or psychological abuse (e.g., manipulation, verbal assault, threatening) that occurs between current or former partners/spouses. IPV can also include sexual harm (e.g., coerced sex, sexual assault) and economic abuse (e.g., financial control/deprivation; World Health Organization [WHO], 2017). Although accurate estimation of the prevalence of IPV is difficult (official crime rates provide an incomplete view of IPV, reluctance of victims to report abuse; Walker & Bowen, 2019), IPV is reported as the leading type of violence experienced by women worldwide (WHO, 2017). Reports from Canada and the United States estimate that nearly one third of women will experience male-perpetrated IPV in their lifetime (Smith et al., 2018; Statistics Canada, 2018).
There is an urgent need to reduce and prevent partner abuse. Yet, meta-analytic research on IPV interventions for perpetrators of abuse is mixed; while a small number of programs have been shown to successfully reduce IPV perpetration, the majority has either small or negligible impacts on violent/abusive behavior (Arias et al., 2013; Babcock et al., 2004; Eckhardt et al., 2013). Importantly, moderator analyses suggest that some treatment-level factors (e.g., type of intervention, duration) may account for some of the mixed findings (Arias et al., 2013).
Notwithstanding their potential importance in moderating program success, the influence of treatment-level factors on IPV recidivism is considerably less studied compared with individual-level risk factors for IPV recidivism (e.g., Capaldi et al., 2012; Costa et al., 2015). For instance, a 2016 study of 238 domestic violence perpetrator programs in the United States and Canada found that the top two approaches used were overwhelmingly Power and Control (also known as the Duluth model; 1 35.6%), and cognitive behavioral therapy (CBT) (29.1%, Cannon et al., 2016). 2 Despite CBT being noted as one of the most common approaches to treatment (see also Hamilton et al., 2013, who found that 70% of European programs used CBT), little research has examined how CBT is specifically defined, operationalized, and implemented across varying IPV program curricula. As such, what is labeled as a CBT intervention varies dramatically across IPV programs, with no set standards as to what constitutes (or should constitute) this type of intervention approach (see Cannon et al., 2016; Eckhardt & Schram, 2009).
Without an in-depth understanding of how program curriculum content is implemented in practice, there is largely insufficient information from which to make conclusive recommendations for model cognitive behavioral IPV programs. The current study explores the literature on guidelines for CBT content in IPV interventions. In addition, the study examines the use of CBT approaches in the curriculum and program self-classification as CBT in 10 IPV intervention programs implemented in British Columbia, Canada.
What is CBT?
Broadly, CBT is conceptualized as a form of psychotherapy that focuses on the link between the thought processes, beliefs, attitudes, and values, which underlie how participants think (Clark, 2011). Maladaptive thinking patterns and failures of self-regulation are also common focal points of CBT-oriented interventions (J. S. Beck, 2011). Traditionally, CBT therapies involve the analysis of schematic models (e.g., underlying roots of core beliefs) and affective factors (e.g., situational contexts that activate maladaptive thoughts; Eckhardt & Massa, 2019).
CBT has undergone considerable evolution as a form of therapy. Specifically, the first wave of CBT therapies was founded on traditional behavioral principles such as positive and negative reinforcements (e.g., systematic desensitization, assertiveness training; Mitchell et al., 2018). The second wave incorporated practices focusing on altering cognitive processes (e.g., rational emotive behavior therapy [Ellis, 1957]; cognitive therapy [A. T. Beck, 1963]), while the third wave integrates elements of mindful awareness and value-based actions (e.g., acceptance and commitment therapy [Hayes & Smith, 2005]). Similarly, the CBT reach has evolved over time; while originally developed for treating internalizing problems such as anxiety, it has been extended and adapted to treat other areas such as anger, substance use, and psychiatric disorders (J. S. Beck, 2011). 3
As a result of the evolution and expansion of CBT, some have noted conceptual and definitional confusion toward what exactly constitutes CBT (Mitchell et al., 2018; Seeler et al., 2014) and what type of therapeutic approaches should be included under the CBT umbrella (Eckhardt & Schram, 2009). Despite this confusion, common elements across CBT interventions (i.e., basic principles of CBT) have been identified (see J. S. Beck, 2011; Mitchell et al., 2018; Seeler et al., 2014). For example, Mitchell and colleagues (2018) discuss eight hallmarks of CBT interventions. Specifically, CBT-oriented interventions should: (a) address both behaviors and cognitions; (b) target cognitions that immediately precede emotional upset and self-defeating behavior; (c) develop individualized treatment plans for each client; (d) be structured with a beginning, middle, and end; (e) be oriented toward skills building; (f) foster psychological flexibility; (g) be active and collaborative; and (h) incorporate homework.
Despite the popularity and widespread use of CBT in interventions for men who perpetrate IPV, the literature provides only general guidelines with respect to key factors and components that should be present for a given intervention to be classified as CBT. In general, CBT-oriented programs treat violence as learned behavior and focus on the link between thoughts and behavior, communication skills, how to be assertive without using violence, and how to manage anger (e.g., Babcock et al., 2004; 2016). In Babcock and colleagues’ (2016) sweeping review of the literature as background to a proposal for evidence-based IPV program standards, the authors note that CBT interventions tend to focus on restructuring distorted thoughts and managing anger arousal: Cognitive-behavioral interventions for reducing domestic violence assume that violent individuals endorse distorted thinking about self, partner, and the utility of violence in times of conflict (Banks et al., 2013; Wexler, 2000 . . . ) . . . . In addition, the role of anger arousal on the pathway to IPV is emphasized in CBT. Intimate partner violent men display increased trait anger, hostility, outward expression of anger, and inhibited anger control (Holtzworth-Munroe et al., 2000). Within this framework, maladaptive thinking patterns surrounding anger, which lead to more insulting and belligerent behavior in domestically violent men, are remedied through cognitive reappraisal and rehearsal techniques for managing anger (Eckhardt, 2007, pp. 361–362)
Similarly, in one of the most comprehensive summaries of CBT interventions for partner abusive men to date (Eckhardt & Schram, 2009), the authors outline four core conceptual factors associated with CBT interventions for perpetrators of abuse: (a) cognitive factors (i.e., addressing cognitive mechanisms that may lead to IPV; specifically the A-B-C model, which outlines the relationship between activating events, an individual’s belief system, and the ensuing emotional and behavioral consequences [see also Ellis, 1957]), (b) emotion regulation (i.e., understanding, labeling, and disrupting negative emotions that are expressed interpersonally), (c) interpersonal skills (i.e., strategies to improve relationship dysfunction and control abusive behaviors), and (d) a collaborative therapeutic alliance (i.e., facilitating a strong working relationship between therapist and client, whether on a one-on-one basis or in a group).
With respect to the specific curriculum content of a CBT intervention for male perpetrators of IPV, fewer guidelines exist regarding what should be taught. As reported by Babcock and colleagues (2016): The main components of this type of intervention include strategies that target thoughts, emotions, and behaviors and are conveyed through a mixture of psychoeducation, homework assignments, cognitive reframing, and self-esteem enhancement (Palmer et al., 1992). Interpersonal deficits are also targeted through a skills training approach . . . . (p. 362) [This type of] intervention would likely contain lectures that prioritize skills building related to deficits in areas such as communication strategies, anger management techniques, and relaxation training. Such interventions might require clients to complete logs and exercises intended to help them identify and challenge their pro-violent and irrational thoughts necessary for managing strong emotions (Eckhardt, 2007; Hamel, 2014; Wexler, 2013). More cutting-edge interventions incorporate into their lectures information about aggression and brain processes and devise homework assignments accordingly (e.g., Potter-Efron, 2014, 2015) (p. 375)
It is notable that Babcock et al.’s description makes use of the terms “would likely contain,” and “might require clients to,” and does not specify what it means in practice to “contain” or “prioritize” these program components. More specifically, if CBT interventions for perpetrators of partner violence are generally believed to consist of a core set of factors, it is unclear whether an IPV intervention should include all of these factors to be classified as a CBT approach—or whether one factor alone might suffice. In addition, with respect to the intensity of focus on each factor, it is unclear whether it is sufficient for programs to address related material/lectures (e.g., “communication strategies, anger management techniques, relaxation techniques” [Babcock et al., 2016, p. 375]) in a single program session or whether they should be addressed repeatedly throughout the curriculum to be considered a true CBT approach.
Classification of IPV Treatment Approaches
Some of the conceptual confusion regarding what constitutes an IPV intervention has been partially attributed to the (mis)labeling and classification of intervention treatment type (Babcock et al., 2004; Eckhardt & Schram, 2009). A number of socio-political factors may play a role in influencing how IPV intervention programs are defined and described. For example, as CBT is often viewed as more evidence-based than other approaches, describing one’s program as CBT may mean a greater chance for organizations that offer justice programs to receive funding. In addition, legislation in several U.S. states has exclusively restricted IPV interventions to the Duluth Model curriculum (Barner & Carney, 2011; Gondolf, 2010). Subsequently, there is considerable variation in the ways in which CBT interventions are operationalized and defined. As noted by Babcock and colleagues (2004): Some CBT groups are not strictly “cognitive” or “behavioral,” as they address emotional components of violence, such as empathy and jealousy (Dunford, 2000). Most modern cognitive–behavior groups also usually address perpetrator attitudes and values regarding women and the use of violence toward women. To the extent that CBT groups address patriarchal attitudes, and Duluth model groups address the learned and reinforced aspects of violence, any distinction between CBT and Duluth model groups becomes increasingly unclear. (p. 1026)
Nevertheless, when implementing their meta-analysis on IPV interventions, Babcock et al. (2004) classified programs as Duluth, CBT, or “other” (with one exception) based on primary evaluation reports. This approach to classifying treatment type is not uncommon, as primary evaluation studies (at least those published in academic journals) typically provide a limited description of program content and rarely present session-level details of program components, that is, the details of the program curricula are often ignored, and meta-analysts are left to rely on authors’ short descriptions of program approach and content, which may fail to present key information on treatment characteristics that would be of use in either appropriately classifying the treatment type or in structuring moderator analyses of treatment impact.
We contend that this approach to classification is problematic if we seek to understand the most-effective approaches for reducing partner abuse. While some programs might appear to use a prototypical CBT approach, it is likely that many interventions would perhaps be more accurately described as using a hybrid approach. For instance, in their discussion of CBT approaches in IPV interventions, Eckhardt and Schram (2009) noted that many “self-described CBT programs . . . have a focus on cognitive content, but spend little time on [core CBT components such as] cognitive process, emotion regulation, and/or relationship skills training” (p. 139). We highlight the authors’ use of the term “self-described CBT programs,” another problematic issue in the literature, which is a focus of the current study, that is, the possibility of independent evaluators relying on program staff descriptions of program content as a means to classify the treatment approach, as opposed to observing intervention sessions directly and/or conducting a detailed review of session-level curriculum materials.
Understanding the variation in how programs describe intervention components is more than a semantic inquiry; it may well be that a focus on anger in a CBT curriculum is important in terms of participant outcomes, but that effects are only realized if the curriculum includes a repeated, multilevel focus on understanding anger triggers and how to de-escalate emotions—as opposed to a 20-min discussion on a single day in a 12-week program. Yet, the results from the North American Domestic Violence Intervention Program Survey (Cannon et al., 2016) as well as the bulk of the summative evaluation research in this area (e.g., Babcock et al., 2004; Eckhardt et al., 2013; Feder & Wilson, 2005) suggest a dichotomous coding of yes/no to program characteristics such as “addresses anger and impulse skills” (assuming detailed descriptions of program characteristics are even presented, which they are often not). 4
Unfortunately, coding program content in this way is typical in the field; surveys across multiple programs often rely on program manager characterizations of program theoretical approach and content (e.g., Cannon et al., 2016; Hamilton et al., 2013; Price & Rosenbaum, 2009). Despite efforts to develop principles of effectiveness and evidence-based practices for IPV prevention and intervention, numerous gaps in knowledge remain with respect to how treatment approach and curriculum content characteristics affect participant outcomes (Babcock et al., 2016; Hamel, 2019). Importantly, in our review of the literature, we were unable to identify any definitions or existing standards with respect to a threshold of CBT emphasis for a program to be considered CBT. Put differently, while many programs may list CBT as a primary or secondary therapeutic approach, little exists in the way of principles or standards for meeting this definition.
The implications of the lack of classification guidelines and subsequent mislabeling of programs are not inconsequential, as (wrongful) claims concerning the effectiveness of a certain treatment type profoundly impede our ability to know what works and make inferences about evidence-based practices and model programs for preventing partner violence. If we strive to advance scientific progress and understand the most effective approaches for reducing partner abuse, determining which program characteristics are most associated with effective outcomes is imperative to developing guidelines for maximizing treatment efficacy. A critical task in developing model programs and informing evidence-based practices involves carefully examining the core components of CBT interventions, analyzing program managers’ self-descriptions of treatment approach, and comparing how programs are described to what they are actually implementing in practice (see also Eckhardt & Schram, 2009).
The Current Study
The current study explores the literature on CBT approaches in IPV interventions, and uses data derived from an evaluation of 10 community-based IPV intervention programs for perpetrators of violence that were implemented in 12 communities 5 across British Columbia, Canada in 2017–2018. These programs were part of a larger simultaneous evaluation of 12 IPV intervention programs operating throughout the province. The objectives of the study are to: (a) review the existing literature and propose a set of core elements for comprehensive CBT–IPV interventions, (b) examine 10 IPV program manager characterizations of their program’s theoretical approach, and (c) apply the set of CBT elements identified in Objective 1 to determine the presence of and intensity in which the elements are implemented across the 10 curricula and explore variation in program characterization versus actual program content.
Method
Data Collection and Analytic Approach
Objective 1
To develop a list of the core elements for a CBT-oriented intervention targeting abusive men, we conducted a thorough search of the existing literature in the field. We sought to identify a set of overarching factors for CBT interventions (e.g., emotion regulation), as well as a list of components comprising each of these factors (e.g., identification of anger triggers). The literature search was conducted by two independent reviewers, 6 primarily through the use of Google Scholar and PsycInfo using key terms “CBT,” “cognitive behavioral therapy,” “IPV,” “intimate partner violence,” and “batterer intervention.” Both reviewers continued their search until they felt they had reached a point of saturation in the literature. The reference lists of key articles in the field (e.g., Babcock et al., 2016; Cannon et al., 2016; Eckhardt & Schram, 2009) were also examined for the inclusion of any articles related to CBT interventions for IPV offenders.
Objectives 2 and 3
Data collection
To develop a thorough understanding of each of the 10 program frameworks and curricula, comprehensive program grant application materials were reviewed and data were extracted to an information sheet containing sections for theoretical approach, program structure, participant screening, curriculum content, and so forth. Each program manager was asked to verify the accuracy of the extracted information and edit the content as necessary. In addition, requests for specific missing data were made and managers were asked to send copies of any relevant program materials. 7 Forty-seven program components were systematically coded in a narrative format, including goals, approach/framework, processes and procedures, session-level curriculum content (i.e., outlines of content for each day of the program), delivery methods (e.g., use of discussion, role-play, video), intended participants (voluntary versus mandated to the program), sources of referral, risk assessments, anticipated outcomes (e.g., reduced psychological and physical violence; increased use of community resources), inclusion of partners/families, aftercare procedures (e.g., group and one-on-one sessions), and staffing/training.
Program manager classification of program approach
Each of the program manager characterizations of their program’s approach 8 was coded for mention of CBT. Managers were asked to (a) list their program’s primary theoretical approach as well as (b) any additional theoretical approaches and therapeutic techniques used in the program. Programs were coded dichotomously as 0/1 for listing CBT as the primary approach, and 0/1 for listing CBT as an additional approach/technique.
Systematic classification CBT curricular content
The curricula of the 10 programs in our sample were coded for each of the factors and components identified in Objective 1; specifically, to analyze the presence and emphasis of CBT curriculum content in each program, the session-level content of each program (i.e., the specific material covered in each week of each program) was coded in Microsoft Excel for any inclusion (yes/no) of the 14 CBT components listed in Table 1. Multiple rounds of coding were conducted by two reviewers (described earlier); all coding was completed independently. Specifically, in Round 1 of coding the first reviewer coded Programs 1 to 5, and the second reviewer coded Programs 6 to 10. In Round 2, the first reviewer verified the codes for Programs 6 to 10 while the second reviewer verified the codes for Programs 1 to 5. Whenever a disagreement in coding occurred, a suggestion for an alternate code was entered into the database and sent to the original coder for a response (i.e., either agree or disagree with the proposed change). This process was repeated until all discrepancies were resolved, and a final code was agreed upon by both reviewers.
Core Factors and Components for IPV–CBT Interventions
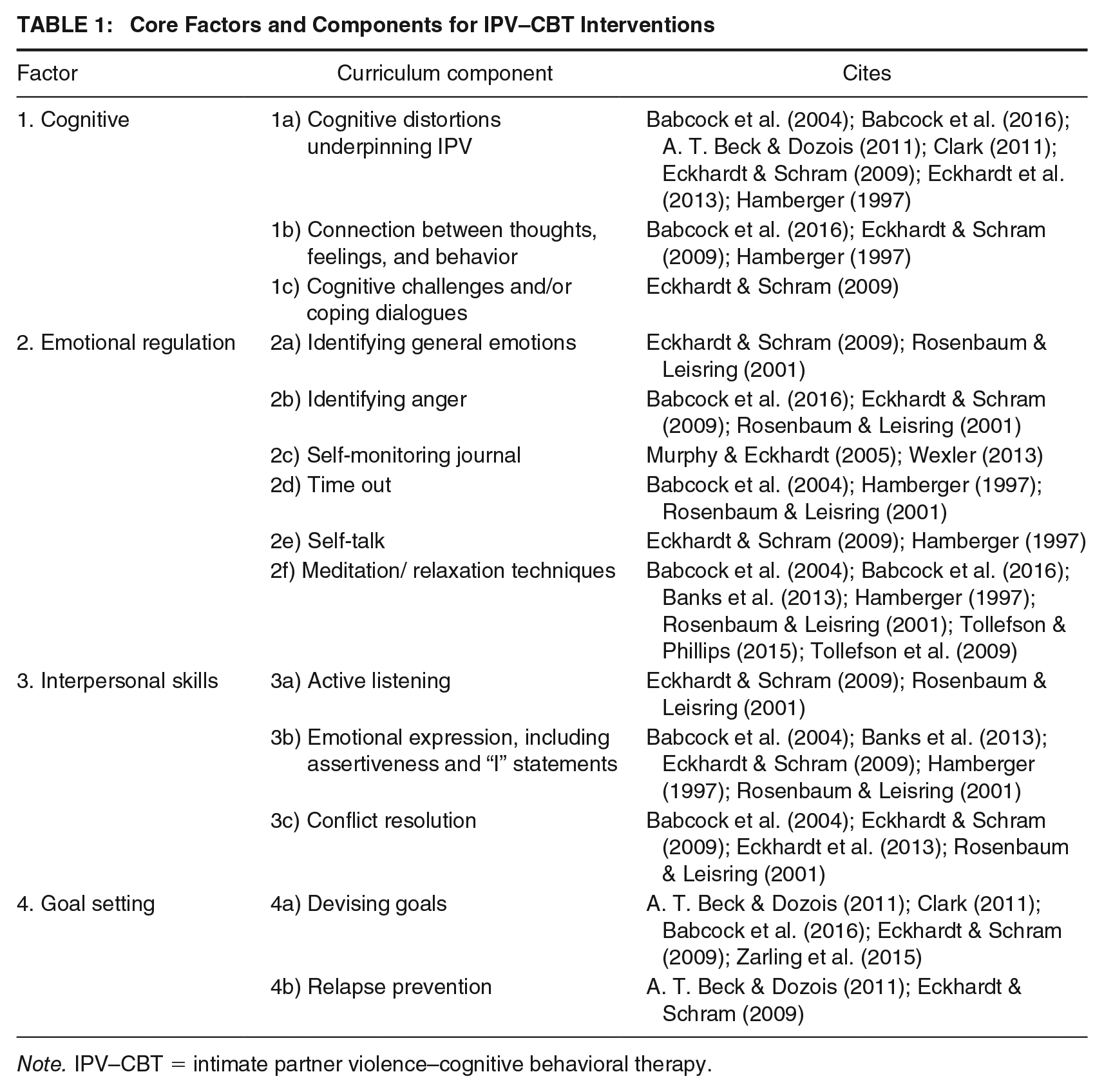
Note. IPV–CBT = intimate partner violence–cognitive behavioral therapy.
Curricular Content Scoring
To explore variation in the inclusion of the core CBT elements across all programs, we examined each program’s curricular content to construct (a) component scores, (b) factor scores, and (c) an overall CBT score. The procedures for the calculation of each score are described below. The consistency between curricular content scores and CBT classification was also explored by comparing each program manager’s self-classification (e.g., using CBT as a primary or secondary approach) and their associated CBT curricular scores.
Component Scores
First, for each of the 10 programs, every individual curriculum session was coded 0 = no/1 = yes for the presence of the 14 components identified in Objective 1. Next, to capture the intensity/emphasis of the component in the program, we counted the number of times each component was present across all sessions in each program—the number of sessions differed across the 10 programs—and computed the percentage of the total sessions in which the component was present. For example, if the cognitive distortion component was present in 4 out of 12 sessions for a given program, it was scored 33% on that component.
Factor scores
For each of the four CBT factors identified in Objective 1, the total number of sessions addressing any of the components comprising a given factor was summed, with a program scoring a maximum of 1 for each of its sessions. For example, if Session 9 of Program A addressed all three of the Cognitive Factor components identified in Objective 1 (see Table 1), Session 9 was scored 1 for “Cognitive Factor”; similarly, if Session 9 of Program B addressed only one of the three Cognitive Factor elements, it would also be scored 1 for the Cognitive Factor. The sum for all sessions was divided by the total number of sessions for each program, with the resulting score representing the proportion of all sessions that addressed at least one component from each factor (e.g., 2/15 = 13%). Each factor was scored independently, with a range from 0% to 100%.
Overall CBT score
To derive an overall assessment of a program’s focus on CBT in its curriculum, the following formula was implemented: Factors 1 to 3 were allocated an equal weighting of 30% each, and Factor 4 (goal-setting) was weighted at 10%. 9 Each of the factor scores was multiplied by their respective weight and summed, resulting in a total CBT score out of 100 for each program. 10
Findings
Objective 1: Core Elements of CBT Interventions for IPV
Based on the existing literature, we identified four key CBT factors relevant for IPV interventions, which include a total of 14 components. See Table 1, followed by a narrative description of each of the factors and components. The descriptions often include illustrative examples derived from modules from the 10 program curricula examined for Objective 2. We propose that this list of CBT elements be considered relevant to IPV interventions classified as having a cognitive behavioral approach.
Factor 1: Cognitive
The cognitive factor focuses on the mechanisms and information processing systems that promote and maintain abusive behavior, including the identification of cognitive distortions or irrational beliefs and the importance of questioning the validity of cognitions (A. T. Beck & Dozois, 2011; Eckhardt & Schram, 2009). Here, participants learn how their beliefs may be linked to their abusive behavior, and discover techniques to evaluate and change their distorted thoughts to eliminate the undesirable behavior (Babcock et al., 2004; A. T. Beck & Dozois, 2011; Eckhardt et al., 2013). This factor includes three components.
Cognitive distortions underpinning IPV
The first component focuses on participants’ unrealistic expectations, faulty attributions, irrational beliefs, and minimization/ denial of responsibility. In particular, participants are taught to identify their own cognitive distortions (or scripts/schemas; e.g., “a woman’s job is to please her man”), understand that defensive beliefs are self-protection devices that most people use to avoid painful thoughts, feelings or consequences, and learn how defenses stand in the way of responsibility and learning new behaviors (Eckhardt & Schram, 2009; Hamberger, 1997). Defensive behaviors may include, for example, attacking (e.g., going on the offensive; believing that “if you don’t get her she will get you”), blaming (e.g., shifting the responsibility for your actions onto your partner; “she asked for it”), and rationalizing (e.g., making up reasons to excuse your actions; “it was for her own good”; Program J Module 4; 11 Program C Module 3; see also Eckhardt & Schram, 2009, p. 146).
Connection between thoughts, feelings, and behavior
In this component, participants learn how to analyze the underlying beliefs that drive their problematic thinking, the effects of their belief systems on negative emotional/behavioral reactions, and how to reframe their thoughts (A. T. Beck & Dozois, 2011; Eckhardt & Schram, 2009). This may include reference to the ABC philosophy model, in which “A” = Activating events, “B” = Belief system, and “C” = emotional and behavioral Consequences. Participants are taught that if they can change the belief they can change the thoughts, change the way they feel, and ultimately change the way they act (Eckhardt & Schram, 2009). Example exercise (Program J Module 8): Participants think of a scenario that triggered their anger (A = “my partner went to a movie with our son and didn’t invite me”). Next, participants examine the underlying beliefs that triggered their response (B = “my family does not like me and does not want to spend time with me”). Then, participants analyze how the scenario made them feel (C = write down the associated feelings and rate their intensity from 1 to 100, then write down the accompanying behaviors or physical sensations experienced). Finally, participants learn to reframe the belief (B) by thinking of examples that show how this belief is not true (see also Eckhardt & Schram, 2009, p. 149).
Cognitive challenges and/or coping dialogues
The focus of this component is on learning to identify, dispute, and replace faulty cognitions by constructing an alternate cognitive frame (e.g., of positive coping dialogues/scripts and alternate attitudes) that is rehearsed by the individual and used as an automatic response to conflict (Eckhardt & Schram, 2009). For example, this might include discussing cognitive distortions that affect decision-making (e.g., the belief that coercion and threats are the only way to get what they want), disputing distorted thoughts (e.g., listening to their partner’s needs might ultimately lead to a more peaceful solution that also meets their own needs), and developing a new coping script that is devoid of irrational beliefs (e.g., “it’s not realistic to think people will always act the way you want them to”; Eckhardt & Schram, 2009). The ultimate goal of this component is to help participants devise corrective alternate scripts that can be used in their day-to-day life (A. T. Beck & Dozois, 2011; Eckhardt & Schram, 2009; Hamberger, 1997).
Factor 2: Emotional Regulation
Factor 2 focuses on mechanisms for self-regulation. This factor incorporates the concept of emotional literacy (i.e., being able to identify feelings and give them verbal labels) to improve self-awareness. In addition, it includes techniques to de-escalate emotions that may lead to abusive and/or violent behavior (Babcock et al., 2016; A. T. Beck & Dozois, 2011; Eckhardt & Schram, 2009). Factor 2 includes six components:
Identifying general emotions
This component involves the identification and examination of a range of emotions such as stress, frustration, and shame. These emotions, if repressed/ignored, may funnel into the use of anger as a proxy for their outward expression and increase the risk of violence (Eckhardt & Schram, 2009; Rosenbaum & Leisring, 2001). Example activity: Introduce the “anger funnel” and build a discussion around how to become more aware of different emotions and feelings that may end up conveyed as anger (Program C Module 2).
Identifying anger
The focus of this component is on learning to identify anger as it arises; if participants can identify anger and become aware of its warning signs, they will be able to change direction and diffuse the emotion or take other actions to prevent violence (Rosenbaum & Leisring, 2001). Participants may learn, for example, that violence does not just “happen”; that they can manage anger appropriately by identifying its triggers (Babcock et al., 2016; Hamberger, 1997). Triggers can be external to the individual, for example, situational (e.g., waiting for someone who is late), smells (e.g., perfume, smoke), sounds (e.g., door slamming), or images (e.g., a movie, television), as well as internal to the individual including physical, behavioral, and psychological cues that indicate increased tension such as blurred vision, increased heart rate, and sweating (Program I Module 8).
Self-monitoring journal
Self-monitoring helps participants engage in a process of self-reflection and creating awareness around patterns of negative behavior. In this component, participants learn how to complete logs to reflect on triggering events, identify cues/warning signs, and record their reactions (A. T. Beck & Dozois, 2011; Eckhardt & Schram, 2009). Example activity: Rate anger on a scale from 1 to 10, describe the triggering event (what caused the anger), identify warning signs that anger was increasing, reflect on how they behaved/reacted when they were angry, and plan how they might respond differently next time.
Time-out
The purpose of a time out is to diffuse the tension during a conflict so that partners can communicate in a more constructive manner once their emotions have calmed. In this component, participants learn the steps involved in a time-out technique: (a) recognize that their anger is escalating, (b) use these cues to remove themselves from the situation and take a break to cool down, (c) use non-violence coping skills to de-escalate and think about the conflict/issues, and (d) return to the discussion at a better time when the intensity of their emotions has subsided (Hamberger, 1997; Rosenbaum & Leisring, 2001).
Self-talk
This component focuses on teaching participants that when anger arises, engaging in positive self-talk can be used as a strategy to guide their behavior by changing the way they feel, de-escalating their emotions, and helping them regain control (Eckhardt & Schram, 2009; Hamberger, 1997). Self-talk statements that participants may be taught include, for example, “I don’t need to prove myself in this situation, I can stay calm,” “My anger is a signal. Time to talk to myself and to relax” (Program J Module 4).
Meditation/relaxation techniques
The focus of this component is to provide participants with stress/anger-reducing techniques to help master emotional arousal. Such techniques include mindfulness practices, deep breathing, meditation, and body relaxation exercises that bring awareness to their thoughts, feelings, and surroundings (Eckhardt & Schram, 2009; Rosenbaum & Leisring, 2001).
Factor 3: Interpersonal Skills
Factor 3 focuses on the participant’s relationships and interactions with others and teaches skills geared toward creating and maintaining healthy relationships so that the use of controlling and abusive behaviors is minimized. This factor is largely centered around communication skills and incorporates the concepts of being a good listener, being assertive in a healthy way by articulating their needs, and using communication as an effective conflict resolution strategy (Eckhardt & Schram, 2009). Factor 3 includes three components:
Active listening
The focus of this component is to teach participants that part of being a good communicator is being a good listener. Specifically, participants are taught that behaving defensively and trying to win arguments hinder one’s ability to accurately process and understand what the other person is saying (Eckhardt & Schram, 2009). Instead, participants learn skills for engaged listening, moderating negative emotional reactions, and reflecting on what the speaker is saying (Rosenbaum & Leisring, 2001). Specific skills for active listening include, for example, maintaining eye contact, being attentive, listening for feelings, asking questions, avoiding the impulsive need to respond, and monitoring reactions that may convey disdain (Eckhardt & Schram, 2009; Rosenbaum & Leisring, 2001 Program J Module 7).
Emotional expression
In this component, the focus is on effective communication and self-expression. Here, participants learn respectful and constructive communication skills, what it is to be assertive, and how to be assertive in a non-aggressive manner. Skills and exercises may include, for example, non-violence assertiveness such as how to respectfully express one’s feelings, wants, or needs, learning to refuse requests from others, asking for help, using “I” statements (e.g., “When you take long phone calls during dinner, I get angry because I begin to think you don’t want to talk to me”), and admitting when they are wrong (Eckhardt & Schram, 2009; Rosenbaum & Leisring, 2001 Program H Module 13).
Conflict resolution
The third component of Factor 3 focuses on processes and skills involved in formulating calm and rational solutions to conflicts. Here, participants learn that conflict is not necessarily a bad thing; it has the purpose of clearing the air, signaling the need for change, and enabling the expression of deep feelings (Eckhardt & Schram, 2009; Rosenbaum & Leisring, 2001). Examples of guidelines to facilitate negotiation and conflict resolution include: sticking to the present (i.e., do not bring up mistakes from the past), demonstrating empathy (i.e., try to understand the other’s point of view), asking for clarification (i.e., do not assume or try to mind read), and resisting the urge to win or be right (Eckhardt & Schram, 2009; Program C Module 4; Program J Module 7).
Factor 4: Goal Setting
Factor 4 reflects the importance of devising relationship goals, family goals, and/or goals for personal growth as well as goals for the prevention of relapse/recurrence of violence. The factor includes two components, as follows:
Devising goals
The first component includes a discussion of the importance of setting goals to enable work toward change, the actual specification of personal and family relationship goals, and working toward achieving these goals (i.e., progress check-ins; A. T. Beck & Dozois, 2011; Clark, 2011). Example exercise: Identify one goal for each of the following areas: (a) personal, (b) career/work, and (c) relationships/family life, and fill out a SMART (Specific, Measurable, Achievable, Relevant, Timely; Drucker, 1954) goals worksheet (Program I Module 11).
Relapse prevention
The focus of this component is to help prevent individuals from returning to old patterns of problematic behavior either temporarily (e.g., using insulting comments during an argument) or permanently as the result of a complete relapse (e.g., consistent use of controlling and violent behaviors; Eckhardt & Schram, 2009). Specifically, this component involves working on maintaining goals, reviewing skills learned throughout the program that can be used to achieve these goals, and preventing the resurgence of abusive and violent behaviors (A. T. Beck & Dozois, 2011; Eckhardt & Schram, 2009). For example, participants complete a self-evaluation form and devise a strategy to handle setbacks, including writing their own progress report and discussing skills they have learned throughout the program, identifying areas in need of improvement, and specifying a relapse prevention plan (Program C Module 12).
Objective 2: Program Manager Classification of Program Theoretical Approaches
Table 2 presents the theoretical approaches used by program managers to describe their respective IPV intervention programs. In total, two managers listed CBT as their program’s primary theoretical approach, while seven managers listed CBT as an additional/secondary theoretical approach or therapeutic technique used in their program. 12 Table 2 also presents an overview of the four factor scores and total CBT score for the 10 programs in the sample. Overall, substantial variability across all metrics was observed with respect to the program characterizations as stated by program managers versus actual content of program curricula (i.e., scores for each core CBT factor as well as CBT content overall).
Factor Scores and Total CBT Score by Program
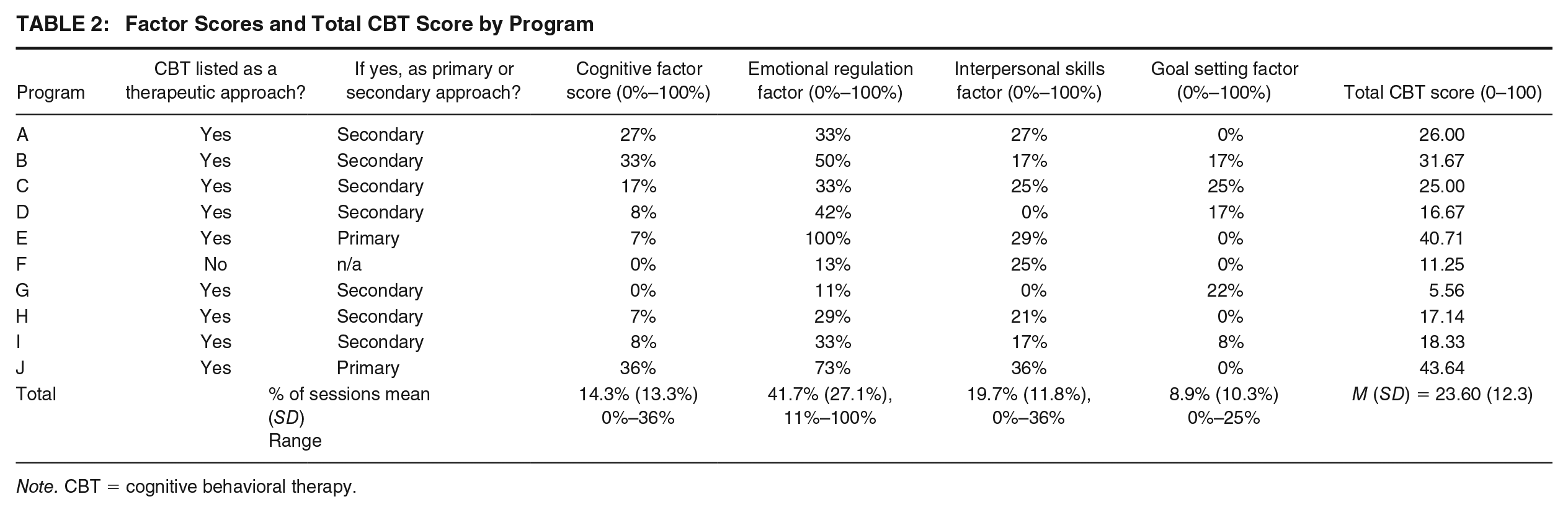
Note. CBT = cognitive behavioral therapy.
Objective 3: CBT Curricular Content in the 10 Intervention Programs
As shown in Table 2, program curricula varied substantially with respect to focus on CBT elements. The average total CBT score was 23.60 out of 100 (SD = 12.3) across all programs, with a range from 5.6 to 43.6. In terms of the four factors, findings suggest that there is very little consistency across the 10 programs in terms of which (if any) core CBT factors are included in the curricula as well as the intensity of focus throughout each intervention. For instance, as demonstrated in Table 2, there is substantial variability in the degree to which each program included components comprising the Emotional Regulation Factor. While Program E included a focus on emotional regulation in each of its 14 sessions (100%), Program G only included an emotional regulation component in 1 of its 9 sessions (11%). The overall mean for the Emotional Regulation Factor was 41.7%, suggesting that, on average, nearly 42% of a program’s sessions focused on at least one of the components in this factor. Similar variability is shown for the other three factors. For the Interpersonal Skills Factor, the inclusion of a related component ranged from 0% to 36%, and on average 19.7% of a program’s sessions focused on one of the three components related to this factor. In addition, an average of 14.3% of program sessions focused on the Cognitive Factor (range 0–36%), and program sessions averaged 8.9% (range = 0%–25%) for a focus on goal setting.
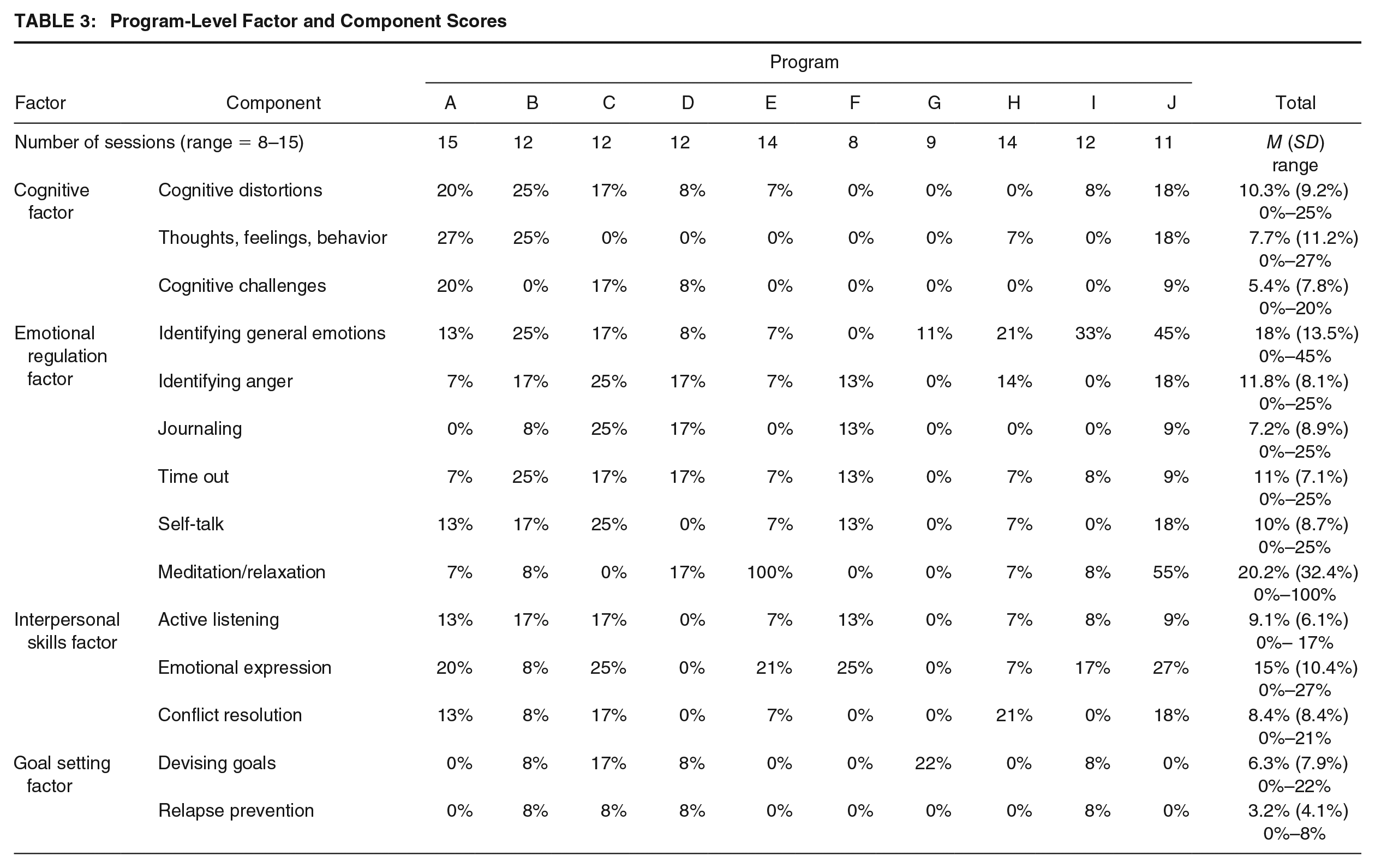
Next, Table 3 provides an examination of the variability across the 10 programs by summarizing the content of the programs with respect to the 14 CBT components. In general, the findings indicate instability in the ways in which programs included the core CBT components. For example, no single component is included in all 14 program curricula (i.e., at least one program scored 0% on each component). In addition, there is substantial variability across programs in the degree of emphasis assigned to each component; the highest average percentage of sessions was for meditation/relaxation techniques (20.2%; however, scores across programs ranged from 0% to 100%), followed by identifying general emotions (18%), emotional expression (15%), identifying anger (11.8%), and timeout (11%). Conversely, the lowest component rates were for relapse prevention (3.2%), cognitive challenges/coping dialogues (5.4%), devising goals (6.3%), and self-monitoring journals (7.2%).
Program-Level Factor and Component Scores
Discussion
Treatment-level factors related to IPV intervention success are largely unknown (Babcock et al., 2016). This gap in knowledge is directly related to the limited guidelines for classification of program approach to treatment, inconsistencies in the conceptualization and operationalization of curriculum content resulting in the mislabeling of IPV intervention treatment types, and limited descriptions of program content, which fail to present key information on treatment characteristics. In the current study, we focused on the widely used CBT approach to IPV intervention and sought to identify core components of an archetypal CBT framework and examine differences in component operationalization across 10 IPV programs. Based on a scoping review of the literature, we identified four core CBT factors, which include a total of 14 components, that we contend should be considered relevant to the consistent and accurate operationalization and classification of an intervention as CBT. While the results from the current study do not permit us to recommend any particular level of focus on these factors (e.g., at least three of four, and repeatedly throughout a curriculum), we argue that program developers, policymakers, and other decision-makers should consider this set of components when deciding whether a given program is, in fact, a CBT intervention.
Implications of the Disconnect Between Program Labeling and Content
In the current study, we also found that program manager descriptions of their program’s content (in a sample of 10 programs) generally did not match with the details of the curriculum assessment. Considering the lack of guidelines for classification and limited information concerning what should be included in a CBT intervention for men who perpetrate IPV, this is not surprising. However, the implications of mislabeling are worthy of discussion as these labels are commonly used to make inferences about best practices. For instance, if the label CBT is applied to a wide variety of treatment approaches, regardless of the specific curriculum content that is addressed in the program itself (i.e., the label CBT is used simply because the program includes some minimal content that addresses the connection between thoughts and behaviors), and the verification/comparison of program label to curriculum content is not possible (due to session-level details not being provided), readers are left with no choice but to accept the self-described label of an intervention as appropriate. When program labels are inconsistent with the actual content of the program, and it is unclear what treatment is actually being received in practice, our ability to make proper inferences about “what works” in an intervention is impeded. Put differently, if there is a tendency toward an over-application of the CBT label, with interventions being incorrectly labeled as CBT, claims concerning the effectiveness/ineffectiveness of programs labeled as CBT are likely to be biased (Eckhardt & Schram, 2009). Scientific progress is harmed in the face of conceptual and definitional confusion in primary studies, as treatment effects are easily under- or over-estimated and comparisons of the effectiveness of alternative approaches are apt to be misleading.
The problematic practice of over-applying the label of CBT and/or mislabeling interventions is exemplified in several systematic reviews and meta-analyses of IPV interventions. For example, in their systematic review of CBT interventions for men who physically abuse their female partner, Smedslund and colleagues (2011) included Duluth-oriented interventions “as they have many cognitive-behavioral components . . . [And] not to include this model would eliminate most batterer intervention programmes in the US” (p. 3). While the authors acknowledge that not everyone will agree with their categorization of Duluth-oriented programs as a type of cognitive behavioral intervention, we nonetheless contend that combining these distinct interventions (despite their clearly stated differences; e.g., see Babcock et al., 2016; Eckhardt et al., 2013; Rosenbaum & Leisring, 2001) and making claims about the (in)effectiveness of CBT for partner abusive men are problematic if we seek to understand the most effective approaches for reducing partner abuse. In a more recent systematic review of IPV interventions, Nesset et al. (2019) discuss the challenge of making claims about the effectiveness of CBT interventions as many programs combine multiple theoretical models and treatment modalities. Furthermore, they lament that “the elements of treatment should at least be described clearly [in primary studies] to make it possible to evaluate and compare treatment effects” (p. 10). Similar issues are observed in several other meta-analyses regarding a lack of clarity concerning the classification of treatment type (e.g., see Arias et al., 2013; Babcock et al., 2004).
Variation Among “CBT” IPV Interventions
In the current study, we also explored session-level program curricula to determine the extent to which the 14 program components reflecting four key CBT factors (identified in Objective 1) were presented in the curricula of 10 IPV interventions. Our findings indicate that programs self-described as using a CBT approach showed little consistency in terms of which (if any) core CBT factors were included. This variability is not unexpected, as programs in British Columbia are typically grassroots-developed and are not required to conform to any provincial standards.
Of greater interest is the variation in the use of CBT content across the curricula of the 10 programs. For example, for the two programs (E and J) in which managers described the program as primarily using a CBT approach, factor scores ranged from 0% to 100%. While these two programs were rated the highest across the sample for the total CBT score (43.64 and 40.71, respectively), a closer inspection of the curriculum components suggest a different picture. That is, while Program J had factor scores of 36% to 73% for all but the Goal-Setting factor (0%), Program E had scores of 7%, 29%, and 0% for the Cognitive, Interpersonal Skills, and Goal-Setting factors, respectively, but scored 100% on Emotional Regulation. The high score on Emotional Regulation was driven primarily by the program’s inclusion of a meditation session in each of the 14 curriculum sessions. Other than the regular inclusion of meditation practice, Program E did not represent a prototypical CBT approach and in practice looked vastly different than Program J. Overall, as a result of the demonstrated heterogeneity of operationalization and inclusion of CBT curriculum content across programs, it is clearly inadvisable to judge a CBT program by its label and to subsequently make assumptions about its content based on that label. We note that this conceptual confusion is likely not limited to CBT in the context of IPV and may also apply to CBT interventions in other clinical areas such as substance use, anger management, or risk reduction in community corrections.
Recommendations
Altogether, the findings herein present a concerning picture regarding the classification of interventions as CBT. Given the observed heterogeneity of treatment-related content across the 10 programs in the current study, there is evidence of uncertainty as to what, exactly, is meant by a “CBT intervention for men who perpetrate abuse.” Furthermore, there is even greater uncertainty regarding what a CBT intervention includes in terms of curriculum content. That is, a CBT label provides little indication of the actual content of the program. The incongruity between program label and program content highlights the need for clear classification guidelines and reporting protocols. Our recommendations for the field are as follows:
A move away from indiscriminate labeling through the development and adoption of clear guidelines with respect to key factors and components that should be present for a given intervention to be classified as cognitive behavioral therapy, as well as a threshold of CBT component emphasis for a program to be considered CBT.
To eliminate the problematic reliance of program staff self-classification of treatment type (which as demonstrated here and also discussed elsewhere [e.g., Eckhardt & Schram, 2009]) have often been shown to be misleading], a new standard for the reporting of session-level curriculum information in primary evaluations of IPV interventions is needed. Journal editors should request that evaluators include a detailed description of the curriculum content of the program that was studied. Without new protocols for reporting treatment-level information, IPV interventions will likely continue to be mislabeled, and the advancement of principles of effectiveness and evidence-based practices for IPV prevention and intervention will be difficult (if not impossible) to achieve.
As the dichotomous coding of presence/absence of curriculum content does not permit an assessment of curriculum component emphasis throughout the program, we encourage evaluators to not only code for the inclusion of specific curriculum content but to also report on the intensity of the included curriculum content (put differently, code for the emphasis the program puts on the component). Reporting the presence of and emphasis placed on each component will allow for a more in-depth understanding of the operationalization and implementation of the intervention, allowing meta-analysts to determine if there is a relationship between treatment-level variables and intervention effectiveness. In turn, this knowledge will guide the development of intervention and prevention efforts and subsequently allow for more conclusive claims toward what works in IPV interventions for men who perpetrate abuse.
Limitations
Although the current study brings further attention to a critical issue in the literature, several limitations should be considered. The first limitation is in respect to our review of the literature and the development of a list of the core elements for a CBT-oriented intervention targeting abusive men. Despite two experienced reviewers conducting a scoping review of the literature on CBT IPV interventions for male perpetrators of partner abuse, it is possible that some sources may have been missed which would have affected our proposed set of CBT factors and components. It is also possible that other reviewers of the literature might suggest additional or alternate components to include such as the style of program delivery, presence of homework, and so forth. Second, with respect to program manager classification of theoretical approaches, it is possible that managers may not have given due consideration to the description of their intervention’s approaches. The fact that some program managers listed up to 15 different approaches in a single program suggests that some programs may be better classified as a hybrid approach. It may also suggest that managers believed listing as many possible different theoretical approaches would be helpful in the quest to receive program funding or support, perhaps as a way to “tick a box” that appeals to a funder, and/or as a means to appear knowledgeable to evaluators about alternative treatment approaches.
In addition, because we were unable to directly observe program sessions, it is possible that the written materials provided for the process evaluation do not accurately reflect the complete curriculum session content, limiting our ability to accurately code for CBT-related components. Furthermore, challenges such as mental health disorders, addiction, and literacy issues may affect the implementation of CBT interventions for partner violent men (and serve as barriers to treatment effectiveness), and programs in practice may look different than they do on paper due to facilitators adjusting to clientele mix. Finally, there are certainly alternative ways to score programs for CBT elements. We do not argue that our approach is the singular method for CBT curriculum assessment, but rather we stress the need for practitioners and researchers alike to more systematically assess curriculum content when classifying IPV programming. Viewed in this light, the current study offers one such approach and illuminates the notable variation in programs classified as CBT interventions.
Conclusion
The inconsistent findings on effectiveness for IPV interventions have been attributed in part to heterogeneity across programs, indicating a clear need to examine factors that underlie treatment effectiveness. Existing research typically relies on program labels designated by program staff or reported on by program evaluators, but the conceptualization and operationalization of CBT vary widely across IPV programs. We argue for more concrete definitions of program elements and the widespread adoption of clear classification guidelines for interventions to be labeled as CBT. Further, given the inconsistencies between program labels and curriculum content, new protocols for reporting of treatment-level information are needed. Together, these shifts can increase our ability to establish evidence-based recommendations for the reduction and prevention of partner abuse and violence.
Footnotes
This project was funded in part by a grant from the BC Ministry of Public Safety and Solicitor General, Community Safety and Crime Prevention Branch.